Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Biochemistry of Alzheimer's disease wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Neurophilosophy wikipedia , lookup
Subventricular zone wikipedia , lookup
Central pattern generator wikipedia , lookup
Neuroeconomics wikipedia , lookup
Nervous system network models wikipedia , lookup
Embodied language processing wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Environmental enrichment wikipedia , lookup
Limbic system wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Selfish brain theory wikipedia , lookup
Intracranial pressure wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Brain Rules wikipedia , lookup
Blood–brain barrier wikipedia , lookup
Development of the nervous system wikipedia , lookup
Optogenetics wikipedia , lookup
Brain morphometry wikipedia , lookup
Neuropsychology wikipedia , lookup
Synaptic gating wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
History of neuroimaging wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Human brain wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Metastability in the brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Sports-related traumatic brain injury wikipedia , lookup
Channelrhodopsin wikipedia , lookup
Hypothalamus wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Aging brain wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuroanatomy wikipedia , lookup
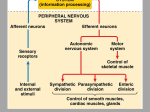
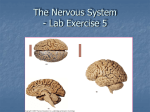
THE NERVOUS SYSTEM Divisions of the nervous system Protection of the Brain: The Cranial Meninges • Cranium is covered with protective membranes = meninges – Cranial meninges are continuous with spinal meninges – 3 layers: 1. outer, fibrous dura mater – forms sheets (falx) that separate the cerebrum and the cerebellum into the hemispheres and the cerebellum from the cerebrum – comprised of an outer endosteal layer and and inner meningeal layer 2. middle arachnoid mater – avascular layer -named for the spider-like struts (trabeculae) that connect the arachnoid to the underlying pia mater 3. inner, thin pia mater – vascular connective tissue -makes direct contact with brain tissue -cells of the pia mater are impermeable to the passage of many substances -this membrane is pierced by tiny capillaries that nourish the brain tissue – arise from the larger capillaries that travel within the dura mater •large spaces for the circulation of blood can be found between the two dural layers = sinuses e.g. superior sagittal sinus • also large veins run through the subarachnoid space e.g. cerebral veins -there are spaces between these membranes A. subarachnoid space: between the arachnoid and pia maters -for the circulation of CSF B. subdural space: between the arachnoid and the dura mater C. epidural space – between • Medical Application Pathology – – There are three types of hemorrhage involving the meninges Epidural bleeding is rapid because it is usually from arteries, which are high pressure. • • • • • • • – – A subarachnoid hemorrhage is acute bleeding under the arachnoid; it may occur spontaneously or as a result of trauma. A subdural hematoma is located in a separation of the arachnoid from the dura mater. • • • • Epidural bleeds from dural arteries can grow until they reach their peak size at six to eight hours post injury, spilling from 25 to 75 ml of blood into the epidural space the bleeding strips the dura from the inside of the skull, causing an intense headache. the bleeding is usually restricted to defined locations as its expansion stops at skull's sutures, where the dura mater is tightly attached to the skull. Bleeding into the epidural space in the spine may also cause epidural hematoma. These may arise spontaneously (e.g. during childbirth, or as a rare complication of anaesthesia (such as epidural anaesthesia) bleeding is likely to be venous. may present as pain, muscle weakness, or bladder and bowel dysfunction. estimates vary from 1 per 10,000 to 1 per 100,000 epidural anaesthetics subdural bleeding usually results from tears in veins that cross the subdural space. This bleeding often separates the dura and the arachnoid layers. Subdural hemorrhages may cause an increase in intracranial pressure (ICP), which can cause compression of and damage to delicate brain tissue. the blood may be aspirated surgically to remove the mass and reduce the pressure it puts on the brain – – The hematoma is neurosurgically evacuated through a burr or craniotomy. The diagnosis of epidural hematoma requires a patient to be cared for in a facility with a neurosurgeon on call to decompress the hematoma if necessary and stop the bleed by ligating the injured vessel branches. subarachnoid hemorrhage Protection of the Brain: CSF – CSF: 80 to 150 mL of clear, colorless liquid • replaced completely up to three times per day • glucose, proteins, lactic acid, urea, ions • made by specialized cells in the lateral ventricles – choroid plexus – networks of capillaries in the walls of the ventricles – covered by ependymal cells (epithelial) cells) that filter the blood plasma and produce CSF by secreting it – these cells are capable of allowing passage of certain substances from the blood through them into the CSF – inhibit the passage of others • continually circulates – ventricles of the brain and central canal to subarachnoid space • functions: – 1. Chemical protection: provides an optimal chemical environment for neuronal signaling – 2. Mechanical protection: acts as a shock absorber, preventing direct physical contact between brain tissue and the bones of the cranium or vertebral canal – 3. Circulation: allows the exchange of nutrients and waste products between the blood and nervous tissue Flow of CSF -CSF forms in the choroid plexi of the lateral ventricles and flows into the 3 rd ventricle through the interventricular foramina -the 3rd ventricle adds to the CSF volume -the CSF then flows into the 4th ventricle via and cerebral aqueduct (passes through the midbrain) – contributes more volume -then enters the subarachnoid space via openings in the 4 th ventricle called apertures -also enters the central canal of the SC -circulation is driven by ciliary action and pressures provided by the blood and gravity – 10 mm Hg Circulation of the CSF •CSF is gradually reabsorbed into the blood through fingerlike projections into the dural venous sinuses = arachnoid granulations -absorbed at about 20ml/hr which equals its rate of formation •interfering with the drainage of CSF into the subarachnoid space can result in accumulation of CSF in the ventricles & CSF pressure rises = hydrocephalus (implantation of a shunt – lateral ventricle into the superior vena cava or abdomen) Blood-Brain Barrier (BBB) • • within the body the capillaries are sites of exchange between materials in the blood and the ECF – filtration of the blood plasma by capillary cells helps form the ECF most locations within the body, this exchange is very free – – – – • the capillary walls are formed of a single layer of cells = endothelium the cells are joined loosely and are connected by numerous gap junctions and pores between the cells this allows for an easy diffusion of many plasma components (except large plasma proteins) between the cells themselves so even small changes in blood plasma contents can dramatically effect the ECF composition however, in the brain, the capillary cells are careful as to what is filtered out of the blood – – – – – – – the cells of the endothelium are very tightly linked together the cells are joined by tight junctions to restrict the flow of materials among them and through them into the ECF surrounding the brain so materials must directly passage the cells themselves to contribute to the ECF so the passage of things like glucose, amino acids, ions are carried through the cells by carrier proteins But lipid-soluble materials and gases (oxygen) can cross easily through the PM of the endothelial cells so transport between the cells is Anatomically Prevented and transport through the cell is Physiologically Restricted = BBB role of astrocytes in the BBB: 1. signal the capillaries to “get tight” • 2. participate in the transport of some ions like K+ The blood supply to the brain • Arterial blood reaches brain via internal carotid, vertebral arteries • Venous blood leaves via internal jugular veins -transient ischemic attacks (TIA): no permanent neurologic damage -temporary cerebral dysfunction caused by impaired blood flow to the brain -dizziness, weakness, blurred vision, slurred speech, paralysis -persists from 5 to 50 minutes -caused by emboli (blood clots), atherosclerosis -cerebral vascular accident (CVA): stroke -affects 500,000 people per year -third leading cause of death -permanent cerebral dysfunction caused by impaired blood flow to the brain -sudden onset of symptoms -caused by cerebral hemorrhage (anuerysm), blood clot, atherosclerosis -treatment – rapid administration of clot-dissolving drugs (e.g. tPA) if stroke is caused by a clot Neuronal Organization Neural Organization: Pathways •A neural pathway is comprised of centers/cell bodies and tracts • Sensory pathway – Ascending – Information from sensory receptors to CNS • Motor pathway – – – – Descending Information from CNS to skeletal muscle or glands Direct pathways – cause precise, voluntary movements Indirect pathways – result in involuntary movement (from brain stem) Major Regions of the Brain Figure 15.1 Major Divisions of the Brain Major Regions of the Brain Major Regions and Landmarks • Cerebrum = largest portion -left and right cerebral hemispheres divided by the longitudinal fissure -connected by the corpus callosum -folded into ridges and grooves: grooves = sulci -sulci divide the cerebrum into lobes -ridges = gyri (gyrus) –Central sulcus •Frontal and parietal lobes Major Regions and Landmarks -outer layer of the cerebrum = cerebral cortex -area for specific processing of sensation, -area of voluntary movement, speech, all thought processes -motor and sensory areas e.g. primary visual, auditory & gustatory areas e.g. primary motor area (precentral gyrus): controls voluntary contractions -plus association areas for integration and analysis of incoming info & help in making of “decisions” The Cerebrum -cerebrum is comprised of: 1. white matter - neurons with long, myelinated axons -organized into tracts A. Association tracts: conduct impulses between gyri within a hemisphere B. Commisural tracts: connects gyri in one hemisphere to others in the other hemisphere 1. corpus callosum 2. anterior commisure 3. posterior commisure C. Projection tracts: tracts that connect cerebrum to the lower parts of the CNS (e.g. Thalamus, brainstem) 2. gray matter – outer edge of the cerebrum = cerebral cortex (2-4 mm thick = billions of neurons) -localized areas of gray matter called the basal ganglia Basal Ganglia -nuclei found deep within the cerebrum - links to the midbrain - receives input from the cortex & provides output to the motor areas of the cortex via the thalamus -integrates motor commands -regulates the initiation & termination of muscle mve. -also functions to anticipate body movements & controls subconscious contraction of skeletal muscle • • comprised of the: 1. striatum – – – • • • • caudate nucleus: activity occurs prior to eye movements putamen: precedes or anticipates body movements nucleus accumbens 2. globus pallidus: regulates muscle tone for movements 3. claustrum 4. substantia nigra: high concentration of dopanergic neurons 5. subthalmic nucleus Medical application: Basal Ganglia -damage to the basal ganglia: -results in uncontrollable, abnormal body movements -muscle rigidity may develop and tremors -Parkinson – neurons that extend from the substantia nigra to the caudate nucleus and putamen degenerate -loss of dopamine releasing neurons – increase in muscle tone and stiffness -Huntington - hereditary disorder -caudate nucleus and putamen degenerate with loss of neurons that release GABA or ACh -spasmatic muscle contractions and loss of mental status Integrative Functions and the Reticular Activating System • integrative function of the cerebrum – processing of sensory information (analysis and storage) and making a decision • • includes sleep and wakefulness, learning and memory, emotional responses wakefulness/sleep: role of the RAS – – – – – 24 hr cycle called circadian rhythm established by the hypothalamus and epithalamus transition between the states of sleep and wakefulness is controlled by the RAS portion of the cerebral cortex that is activated upon sleep arousal when active – transmission of signals to many areas of the cortex both directly and via the thalamus = general increase in cortical activity – arousal = awakening from sleep • stimulation of the RAS – by touch, pressure, pain, light • no input by olfactory receptors!! • stimulation of cholinergic neurons that release AcH – sleep = state of altered consciousness from which you can be arouse • • • • • • • exact function is still unknown two components: NREM and REM NREM – four stages REM – 3 to 5 episodes per 7 to 8 hour sleep period (10-20 minutes) regulated by many areas of the brain – hypothalamus, forebrain, medulla oblongata sleep inducer – adenosine – binds to receptors and inhibits the RAS (inhibits arousal) caffeine – binds to adenosine receptors and blocks their action – activity of the RAS is maintained Integrative Functions • learning and memory – learning = the ability to acquire new information • no completely satisfactory explanation – memory = the process by which information that is acquired through learning is stored and retrieved – role for long-term potentiation (LTP) – enhances transmission at the hippocampus after a period of high-frequency stimulation – role for glutamate = binds NMDA glutamate receptors on post-synaptic neurons • different categories of memory – 1. immediate: ability to recall ongoing experiences, provides perspective to the present time so we know where we are and what we are doing – 2. short-term: temporary ability to recall information - seconds to minutes old » e.g. look up a phone number and then dial it a few seconds later » hippocampus, mamillary bodies of the hypothalamus and the anterior and medial nuclei of the thalamus – 3. long-term: transfer of short-term into a more permanent type » last from days to years » e.g. use the telephone number enough – stored permanently » role for the basal ganglia, cerebral cortex and cerebellum • http://www.nlm.nih.gov/medlineplus/memory.html • http://en.wikipedia.org/wiki/Anterograde_amnesia • http://en.wikipedia.org/wiki/Retrograde_amnesia Major Regions and Landmarks • Diencephalon – includes the hypothalamus, thalamus, epithalamus and subthalamus – thalamus: 80% of the diencephalon • paired oval masses of gray matter organized into nuclei, interspersed with white matter • joined by the intermediate mass (gray matter) in about 70% of brains • major relay station for most sensory impulses from the SC, brain stem • crude perception of pain, heat and pressure (refined in cerebrum) • transmits motor information from cerebellum to the cerebrum • relays nerve impulses to and from different areas of the cerebrum • seven major groups of nuclei !!! •hypothalamus -Emotions, autonomic functions, hormone production -mamillary bodies – serve as relay stations for reflexes related to eating -supraoptic and preoptic nuclei that in hormone secretion (ADH) and body temp -major functions: 1. control of the ANS – integrates signals from the ANS (regulated smooth and cardiac muscle contraction) major regulator of visceral activities (heart rate, food movements, contraction of bladder) 2. produces hormones & connects with pituitary to regulate its activity 3. regulates emotional and behavioral patterns – rage, aggression, pain and pleasure + sexual arousal 4. regulates eating & drinking – hypothalamus contains a thirst center which responds to a rise in osmotic pressure in the ECF (dehydration) 5. controls body temperature – monitors temp of blood flowing through the hypothalamus •epithalamus – consists of the pineal gland and habenular nuclei -pineal gland – part of the endocrine system -secretes the hormone melatonin -increased secretion in dark -promote sleepiness and helps set the circadian rhythms of the body (awake/sleep period) •subthalamus – works with the cerebrum and cerebellum to control body movements -majority is made of the subthamic nuclei -sends efferent connections to the caudate nucleus and putamen, to the medial and lateral nuclei of the thalamus and to the red nucleus and substantia nigra of the midbrain -also receives afferent connections from the substantia nigra Major Regions and Landmarks BRAIN STEM • Medulla oblongata – – – – – – – continuation of the SC that forms the inferior part of the brain stem relays sensory information and controls automatic motor functions where the SC and MO meet - 90% of the axons from the right side of the SC cross over to the left side of the MO and vice versa = decussation white matter contains sensory/ascending and motor/descending tracts some of the white matter form bulges called pyramids – white tracts that connect the cerebrum to the SC contains several nuclei also that regulate autonomic functions - reflex centers for regulating heartbeat and BP (cardiovascular center), respiration (respiratory center), plus vomiting, coughing, sneezing, hiccuping and swallowing nuclei in the posterior part are associated with sensations of touch, proprioception, pressure and vibration -associated with 5 pairs of cranial nerves VIII IX X XI XII -other nuclei 1. inferior olivary: part of the olive -relay impulses from proprioceptors to the cerebellum – joint and muscle position 2. gracile: ascending sensory tracts from SC synapse here -relayed to the thalamus by postsynaptic neurons 3. cuneate: ascending sensory tracts from SC synapse here -relayed to the thalamus by postsynaptic neurons -injury to the medulla: hard blow to the back of the head or upper neck can be fatal -damages the medullary rhythmicity area of the respiratory center (disrupts pattern of breathing) -non-fatal injury: paralysis and loss of sensation, irregular breathing and heart rate Major Regions and Landmarks BRAIN STEM • Pons = “bridge” - e.g. connects brain stem to the cerebrum via bundles of axons - superior to the medulla and anterior to the cerebellum – consists of nuclei (cell bodies in gray matter) and tracts – somatic and visceral motor responses • Pontine nuclei – control voluntary movements that originate in the cerebral cortex and are relayed through the pons into the cerebellum • Pneumotaxic area – controls breathing (with medulla) • Apneustic area – controls breathing (with medulla) Major Regions and Landmarks BRAIN STEM • Midbrain (Mesencephalon) – relay station between the cerebrum and the spinal cord – extends from the pons to the diencephalon – sends motor tracts to the SC, medulla and pons & conducts sensory tracts to the thalamus – anterior portion contains a pair of white tracts = cerebral peduncles • conduct impulses from the cerebrum to the SC, pons and medulla – posterior portion = tectum • white matter tracts = cerebellar peduncles • four round elevations = colliculi • reflex centers for visual activities (tracking, scanning) pupillary reflex, shape of the lens • reflexes that mediate movements of the eyes, head and neck - the startle reflex • relays impulses from hearing receptors to the thalamus -generates involuntary somatic motor responses •release of dopamine from substantia nigra (nuclei) - loss of these neurons = Parkinsons •red nuclei forms synapses with cerebellum to coordinate muscle movements Major Regions and Landmarks • Cerebellum – – divided into hemisphere with lobes - like the cerebrum • anterior and posterior lobes involuntary motor activities • evaluates and coordinates motor activities initiated by the cerebrum and corrects problems by sending info back to the cerebrum • regulate posture & balance – – – – has a superficial layer of gray matter called the cerebellar cortex - like the brain deep to the gray matter are tracts of white matter = arbor vitae also has nuclei = cerebellar nuclei (origin of neurons that connect the cerebellum to the brain and SC) connected to the brain stem by three cerebellar peduncles • • • inferior – sensory information from the inner ear and body proprioceptors middle – carry commands for voluntary movements that originated into the cortex into the cerebellum for coordination superior – connects to the red nuclei and the nuclei of the thalamus Medical application: Ataxia • damage to the cerebellum • blindfolded people cannot find the tip of their nose • also changed speech patterns due to incoordinate speech muscles • abnormal walking or balance • alcohol overdose also suppresses the activity of the cerebellum The Limbic System • • • • • • corpus called the emotional brain callosum group of structures that surround the brain cingulate gyrus stem anterior thalmic nuclei hypothalmic nuclei involved in olfaction and memory fornix emotion – anger, fear, happiness… – associated with specific responses – behavioral patterns basic behavioral patterns – -preparing for attack, laughing, crying, blushing – also includes sexual behaviors for the continuation of the species – connects with the hypothalamus to regulate these behaviors olfactory tract main components: mamillary body – 1. limbic lobe: rim of cerebral cortex on the medial surface of amygdala each hemisphere – includes the parahippocampal gyrus hippocampus hippocampus (memory) – 2. dentate gyrus – 3. amygdala: stimulation - rage – 4. olfactory bulbs – 5. septal nuclei – 6. mammillary bodies of the hypothalamus Medical Application: Alzheimer’s Disease -loss or reasoning, memory -11% of population over 65 (4 million people) -unknown cause – thought to be genetic factors + environmental & lifestyle -neuronal plasma membranes contain a protein = amyloid precursor protein (APP) abundant in presynaptic axon terminals -cleavage of APP yields a secreted product = sAPPa that is secreted by the presynaptic terminals normally -if APP is cleaved at the wrong site – beta-amyloid -two forms of beta-amyloid are possible based on cleavage site – the longer form (Ab40) is harmless -but the form Ab42 – 10% of the cleaved b-amyloid – aggregates to form plaques and is neurotoxic -underlying causes for Ab plaque formation remain unknown -about 15% of cases appear to have a genetic link – familial Alzheimer’s -mutations in 3 genes: prenisilin-1, -2 and APP lead to early onset forms (less the 15% of all cases) – prenisilins cleave APP -mutations in these genes can shift the balance of b-amyloid to the harmful form, -so can age -also mutations in gene coding for apolipoprotein E (ApoE) a protein that helps transport cholesterol in the blood -may account for 85% of the cases – late-onset Alzheimers -mutated genes for apoE = apoE4 – may increase risk of development -may predispose you to Ab plaque formation, or may hasten the onset - ????? Medical Application: Alzheimer’s Disease • • • • • • -brain abnormalities: 1. loss of ACh releasing neurons from the nucleus basalis (below the globus pallidus) 2. beta-amyloid plaques 3. neurofibrillary tangles -plaque – central core of b-amyloid, surrounded by degenerating nerve endings – the plaques attract microglia – inflammatory reaction against the plaque, including the secretion of toxic chemicals that harm “bystander” neurons • • -tangles – bundles of abnormal filaments that accumulate in the cell bodies of the affected neurons – probably form in response to the formation of Ab plaques – bind to the neurons and alter the proper formation of the neurons cytoskeleton – production of tangles • the Ab plaques are also thought to lead to excessive influx of Ca ions which kills the cells – hippocampal neurons (long-term memory) seem to be vulnerable • • -treatments: drugs that inhibit acetylcholinesterase improve alertness by increasing Ach signaling in the brain e.g. Donepezil – only ones currently approved (Aricept) – may improve the symptoms – they don’t slow the degeneration http://en.wikipedia.org/wiki/Alzheimer#Acetylcholinesterase_inhibitors I - Olfactory II - Optic III - Oculomotor IV-Trochlear V - Trigeminal VI - Abducens VII - Facial VIII - Acoustic IX - Glossopharyngeal X - Vagus XI - Accessory XII - Hypoglossal -cranial nerves – 12 pairs -considered part of the peripheral nervous system (PNS) -olfactory & optic contain only sensory axons = sensory nerves -remaining are either motor or mixed nerves – both motor and sensory axons “some say my mother bought my brother some bad beer, my my” Spinal Cord • length in adults = 16 to 18 inches • Cervical and lumbar enlargements – cervical = C4 to T1, nerves to and from upper limbs – lumbar = T9 to T12, nerves to and from lower limbs • Tapers to conus medullaris • filium terminale arises from the CM - extension of the pia mater that anchors the SC to the coccyx • 31 segments each with – Dorsal root ganglia • Sensory neuron cell bodies – Pair of dorsal roots – Pair of ventral roots Spinal Meninges • Specialized membranes • Provide physical stability and shock absorption • Three layers – Dura mater = dense irregular CT • continuous with the brain’s DM • above it is the epidural space – Arachnoid = continuous with brain • above it is the subdural space • below is the subarachnoid space • avascular – Pia mater = connective tissue • collagen and elastin bundles • well vascularized • The Pia Mater – Innermost meningeal layer – Bound firmly to underlying tissue – Denticulate ligaments bind pia mater to the arachnoid -spinal tap: under local anesthetic -long needle is inserted into the subarachnoid space and CSF is withdrawn or antibiotics or anesthetics are given -given between L3 & L4 or L4 & L5 Histology of the Spinal Cord • Central gray matter – Contains cell bodies of neurons and glial cells + unmyelinated axons – Gray matter projections are horns • Peripheral white matter – Myelinated and unmyelinated axons – Tracts or columns Organization of Gray Matter • Posterior gray horns – Somatic and visceral sensory nuclei • Anterior gray horns – Somatic motor control • Lateral gray horns – Visceral motor neurons • Gray commissures – Axons of interneurons crossing cordated and unmyelinated axons Organization of White Matter • Six columns (funiculi) – Anterior, lateral and posterior white columns – Contain tracts • Ascending tracts relay information from spinal cord to brain • Descending tracts carry information in the opposite direction • Spinothalamic tract – • Posterior columns – • pain, temperature, deep pressure & crude touch proprioception, discriminative touch, two-point discrimination, pressure and vibration Direct pathways (corticospinal & corticobulbar) – – – precise, voluntary movements corticobulbar: cerebral cortex to brain stem and out via cranial nerves to muscles of head and neck corticospinal: also called the pyramidal tracts (lateral and anterior) • • cerebral cortex to spinal cord and out to voluntary muscles (synapses with lower motor neurons in the ventral gray horn) Indirect pathways (rubrospinal, vestibulospinal) – – programming automatic movements, posture & muscle tone, equilibrium & coordination of visual reflexes rubrospinal: alternate route for voluntary movements of arms and legs • – red nucleus of midbrain through the lateral column vestibulospinal: