Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Holonomic brain theory wikipedia , lookup
Apical dendrite wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Synaptogenesis wikipedia , lookup
Optogenetics wikipedia , lookup
Neuroanatomy wikipedia , lookup
Metastability in the brain wikipedia , lookup
Cortical cooling wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Time perception wikipedia , lookup
Development of the nervous system wikipedia , lookup
Human brain wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Microneurography wikipedia , lookup
Central pattern generator wikipedia , lookup
Environmental enrichment wikipedia , lookup
Neuroplasticity wikipedia , lookup
Aging brain wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuroeconomics wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Evoked potential wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Synaptic gating wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Muscle memory wikipedia , lookup
Embodied language processing wikipedia , lookup
Cerebral cortex wikipedia , lookup
Basal ganglia wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
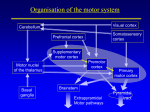
VMED 5171/NS28/GMS Central Control of Motor Function Student Preparation Textbook of Medical Physiology Guyton and Hall, Ch. 55, 56 Neuroscience Bear et al., Ch. 14 Overview • Cerebral (association) cortex - generates the impulse to act, the design and the planning of movement. • Basal ganglia and thalamus - provide the gross motor “programs.’ • Motor cortex, brain stem and spinal cord interact to maintain posture and movement execution. • Cerebellum - maintains equilibrium and smooth coordination of movement. Descending Motor Control • Higher centers are required for: – initiation of voluntary movement – regulation of the rate, forcefulness, and smoothness of movement • Descending tracts - control motor function • Ascending tracts - sensory function for planning and feedback. Hierarchy of Motor Control LEVEL FUNCTION STRUCTURES high strategy association areas of neocortex, basal ganglia middle tactics motor cortex, cerebellum low execution brain stem, spinal cord Example of the Role of Central Control of Motor Function How Does the Brain Communicate With the Motor Neurons of the Spinal Cord? Two Major Groups of Descending Pathways • Lateral pathways – involved in voluntary movement of the distal musculature; under direct cortical control. • Ventromedial pathways – involved in the control of posture and locomotion; under brain stem control. Descending Tracts In Spinal Cord Lateral pathways Ventromedial pathways Lateral Pathways: Corticospinal tract Rubrospinal tract Ventromedial Pathways: Vestibulospinal tract Tectospinal tract Ventromedial Pathways: Pontine (medial) reticulospinal tract Medullary (lateral) reticulospinal tract Summary of the major descending spinal tracts and their points of origin corticospinal tract reticulospinal tracts rubrospinal tract tectospinal, vestibulospinal tracts Central Motor Control Systems • Pyramidal system (corticospinal tract) [lateral pathways] • Extrapyramidal system (everything else: basal ganglia, cerebellum, brain stem) [ventromedial pathways] Cerebral Cortex • Primary motor cortex - discrete purposeful movements • Premotor area - patterns of movement • Supplemental motor area - bilateral movements, fixation movements Human area 4 = M1 = primary motor cortex Human area 6 = premotor area (PMA) and supplemental motor area (SMA) = premotor cortex Corticospinal Tract (Pyramidal Tract) • Arises from primary motor cortex (30%), premotor cortex and supplementary motor area (30%), and somatic sensory areas of cortex (40%). • Projects from cerebral cortex to spinal cord without interruption. • Synapses with: – motor neurons controlling distal muscles (alpha and gamma motor neurons) – interneurons controlling motor neurons Pathway of Pyramidal Axons • CST axons are grouped together and form the medullary pyramids. – CST also called the pyramidal tract • Most CST axons decussate at the junction between medulla and spinal cord. These axons form the lateral corticospinal tract. • Lateral CST innervates contralateral (to cortex) interneurons and motor neurons supplying distal limb muscles. Pathway of Pyramidal Axons • Some axons descend without decussation in ventral columns to form the medial (ventral) corticospinal tract. Most of these fibers cross to the opposite side of the cord in thoracic or cervical areas of cord. • Involved in control by supplementary motor area of bilateral postural movements and motor neurons supplying trunk and proximal limb muscles. Other CST Targets • Feedback signals from the cortex to inhibit adjacent motor cortex areas to “sharpen” the boundaries of excitatory output. • Fibers to caudate nucleus and putamen of BG. • Fibers to red nucleus – rubrospinal tract. • Fibers to the reticular substance and vestibular nuclei – reticulospinal and vestibulospinal tracts, reticulocerebellar and vestibulocerebellar tracts. Other CST Targets cont. • Fibers to the pontine nuclei – pontocerebellar tract. • Fibers to the inferior olivary nuclei – olivocerebellar tract. So, descending information in CST also results in activation of the basal ganglia, cerebellum, and brain stem. Inputs to Motor Cortex • Subcortical fibers from other cortical areas: somatosensory, frontal, auditory, visual. • Subcortical fibers from contralateral cortex through the corpus callosum. • Somatosensory fibers from thalamic ventrobasal complex. • Fibers from thalamic VL and ventroanterior nuclei – from cerebellum and basal ganglia. • Fibers from thalamic intralaminar nuclei – arousal. CST Lesions • Common causes of CST lesions include: – stroke – tumors – trauma • Upper motor neuron (UMN) disease • Lesions to motor cortex will affect limb muscles contralateral to lesion. Why? CST Lesions – Positive Signs • Abnormal responses to stimuli (hyperreflexia) or motor behaviors that emerge as a result of the lesion. • Primarily due to withdrawal of inhibitory influences or to interneuron connection defects. CST Lesions – Negative Signs • Loss of the function normally controlled by CST (paralysis), resulting in the inability to initiate fine voluntary movements, or a loss of fractionation (the inability to control individual muscles independently.) • Primarily due to a loss of connections of CST neurons onto alpha motor neurons. • Examples: hypotonia (decreased muscle tone), weakness, diminution of movement (paresis). CST Conclusion • Direct activation of alpha, gamma motor neurons and interneurons. • Background tonic signals to motor areas of cord. Brain Stem Motor Centers • Pontine reticular nuclei – excite antigravity muscles (muscles of the vertebral column and limb extensor muscles) – pontine reticulospinal tract. • Medullary reticular nuclei – inhibit antigravity muscles – medullary reticulospinal tract. Pontine & medullary systems balance each other. • Vestibular nuclei – supplement the excitatory function of the pontine system by integrating vestibular information – lateral and medial vestibulospinal tracts. Basal Ganglia and Cerebellum The basal ganglia and cerebellum are large collections of nuclei that modify movement on a minute-to-minute basis. The motor cortex sends information to both, and both structures send information back via the thalamus. Output of the cerebellum is excitatory and inhibitory, while the basal ganglia are inhibitory. The balance between these two systems allows for smooth, coordinated movement, and a disturbance in either system will show up as movement disorders. Basal Ganglia (Basal Nuclei) • Nuclei deep to the cerebrum • Important in posture and planning and coordination of motor action (via dopamine) • Loss of actions results in muscle tremors (Parkinson’s disease) • Striatum [caudate, putamen], globus pallidus, substantia nigra, subthalamic nucleus Basal Ganglia • Most afferents come from the cerebrum, most efferents go to the cerebrum • Connected to the motor area of the cortex and to the thalamus • No direct connection to alpha motor neurons Feedback loop from the cortex, to the basal ganglia, to the thalamus (VLo), to cortical area 6 (SMA) Putamen Pathway For Execution of Learned Patterns of Movement X Caudate Pathway For Cognitive Planning of Motor Patterns X Corpus Striatum (caudate nucleus and putamen) • Afferents - premotor and supplemental motor areas of cortex, somatosensory cortex, substantia nigra • Efferents - globus pallidus, eventually back to cortex • Gross movement initiation, visual limb placement Globus Pallidus • Afferents –from the striatum, subthalamus • Efferents – to substantia nigra, subthalamus, thalamus, RF • Motor relay, tonic background contractions Neurotransmitters • Dopamine (-): substantia nigra to caudate nucleus • ACh (+): from cortex to putamen and caudate • GABA (-): from caudate and putamen to globus pallidus and substantia nigra Neurotransmitters • Norepinephrine, serotonin, enkephalin, glutamate also serve as transmitters. Neurotransmitters Diseases • Parkinson’s disease (paralysis agitans) – widespread destruction of substantia nigra and or globus pallidus. Characterized by rigidity, tremor at rest, and akinesia. • Loss of dopamine secreting neurons in substantia nigra; excessive ACh activity in the striatum from cortex. • Treat by replacing dopamine (L-DOPA) and/or by blocking ACh from cortex. Diseases • Chorea (Huntington’s disease) – associated with degeneration of striatum. Irregular pattern of involuntary movement of muscle groups (chorea = dance). Progresses to rigidity and dementia, death. • Unopposed DA release by substantia nigra. • Results from loss of GABA containing neurons and therefore the loss of inhibitory input to globus pallidus. Diseases • Ballism – violent flailing movements. • Caused by destruction of subthalamic nuclei or its connections. • Hemi-ballism – unilateral. • Athetosis – writhing movements of hand, arm, neck, or face. • Caused by lesions in the globus pallidus. Diseases • Black walnut toxicosis in horses – produces laminitis and liquefactive necrosis of the substantia nigra and globus pallidus. Can result from as little as 5% in shavings used as bedding. Treated by removing bedding. • Yellow star thistle poisoning in horses (nigropallidal encephalomalacia) – necrosis of substantia nigra and globus pallidus. No tx. Cerebellum (Little Brain) The cerebellum contributes to smooth coordination of motor activity. With a huge sensory input, the cerebellum rapidly processes information on instantaneous body position and makes corrective adjustments of planned motor activity. The cerebellum operates through numerous reciprocal connections which “follow-up” motor activity in a servomechanism fashion. Sensory Homunculi of the CBL Cerebellar Function • In voluntary movement – corrects motor irregularities – compares motor “central” intentions to “peripheral performance” – controls ballistic movements • In posture and equilibrium – cooperation with spinal cord, cortex and reticular formation • Primarily inhibitory function Cerebellar Inputs and Outputs • The cerebellum operates in 3’s: – there are 3 routes in and out of the cerebellum – there are 3 main inputs – there are 3 main outputs from 3 deep nuclei. • The 3 routes are the peduncles, or “stalks” the rostral, middle and caudal cerebellar peduncles. Cerebellar Inputs and Outputs • The 3 inputs are: – mossy fibers from the spinocerebellar pathways and – mossy fibers from the pons, carrying information from the contralateral cortex – climbing fibers from the inferior olive Cerebellar Afferent Pathways mossy fibers climbing fibers Cerebellar Inputs and Outputs • The 3 deep nuclei are: – (1) fastigial - concerned with balance; sends information mainly to the vestibular and reticular nuclei – (2) dentate and (3) interposed - both concerned with voluntary movement; send axons mainly to the thalamus and red nucleus • All 3 receive inputs from sensory afferent tracts and from the cerebellar cortex. Cerebellar Efferent Pathways • To medullary and pontine regions of the brain stem – posture and equilibrium • To thalamus (VL & VA), to cortex, to thalamus (midline), to basal ganglia, red nucleus, & reticular formation – coordination between agonists and antagonists • To thalamus (VL & VA) to cortex – coordination of sequential motor actions Cerebellar Circuits Cerebellar Circuits • Inputs to the cerebellar cortex (mossy and climbing fibers) excite the deep nuclei cells as they enter. • The output of the CBL cortex (Purkinje cell axons) inhibits the deep nuclei cells. • Climbing fibers excite Purkinje cell dendrites. • Mossy fibers excite granule cells, whose axons (parallel fibers) excite Purkinje cell dendrites. • Deep nuclei cells and Purkinje cells fire tonically. Cerebellar Circuits Feedback loop from the cortex, to the cerebellum, to the thalamus (VLc), to cortical area 4 (PMA) Diseases • Cerebellar lesions – intention tremor. • Hereditary cerebellar degeneration (abiotrophy): Kerry blue terrier, rough-coated collie, Gordon setter, Arabian horses, Holstein-Friesian cattle, Yorkshire swine – loss of Purkinje cells. • Cerebellar hypoplasia – perinatal infection by feline parvovirus – kills granule cells, P-cells. Decortication Lesion (A) • Hypermetria • Spasticity/hyperreflexia • Hemiparesis Decerebration Lesion (B) • • • • • Lose cortex, thalamus Leaves subthalamus Hyperactive reticular formation Extensor rigidity Hyperexcited gamma and alpha motor neurons • Unopposed vestibular facilitation • Flexor hypertonus Cerebellar Lesion • • • • • Hypotonia Ataxia Nystagmus Intention tremor Dysmetrias Over-Simplified Summary • Motor cortex – initiation of movements • Brain stem centers – balance of excitation and inhibition of antigravity muscles; integration of vestibular information • Basal ganglia – posture and planning and coordination of motor action • Cerebellum – equilibrium; coordination of motor action based on sensory information and feedback Hierarchy of Motor Control LEVEL FUNCTION STRUCTURES high strategy association areas of neocortex, basal ganglia middle tactics motor cortex, cerebellum low execution brain stem, spinal cord