Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cognitive neuroscience wikipedia , lookup
Electrophysiology wikipedia , lookup
Multielectrode array wikipedia , lookup
Axon guidance wikipedia , lookup
Aging brain wikipedia , lookup
Nervous system network models wikipedia , lookup
Environmental enrichment wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Neurotransmitter wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neuroregeneration wikipedia , lookup
Nonsynaptic plasticity wikipedia , lookup
Subventricular zone wikipedia , lookup
Neuroplasticity wikipedia , lookup
Adult neurogenesis wikipedia , lookup
Development of the nervous system wikipedia , lookup
Metastability in the brain wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Apical dendrite wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Chemical synapse wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Synaptogenesis wikipedia , lookup
Optogenetics wikipedia , lookup
Limbic system wikipedia , lookup
Synaptic gating wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuroanatomy wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Hippocampus wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Channelrhodopsin wikipedia , lookup
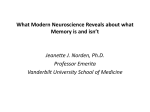
Pharmacological Reports Copyright © 2013 2013, 65, 555565 by Institute of Pharmacology ISSN 1734-1140 Polish Academy of Sciences Review Hippocampus, hippocampal sclerosis and epilepsy Krzysztof Sendrowski, Wojciech Sobaniec Department of Pediatric Neurology and Rehabilitation of the Medical University of Bia³ystok, J. Waszyngtona 17, PL 15-274 Bia³ystok, Poland Correspondence: Krzysztof Sendrowski, e-mail: [email protected] Abstract: Hippocampal sclerosis (HS) is considered one of the major pathogenic factors of drug-resistant temporal lobe epilepsy. HS is characterized by selective loss of pyramidal neurons – especially of sectors CA1 and CA3 of the hippocampus – pathological proliferation of interneuron networks, and severe glia reaction. These changes occur in the course of long-term and complex epileptogenesis. The authors, on the basis of a review of the literature and own experience, present the pathomechanisms leading to hippocampal sclerosis and epileptogenesis, including various morphological and functional elements of this structure of the brain and pharmacological possibilities of preventing these processes. Key words: hippocampus, hippocampal sclerosis, epilepsy, epileptogenesis Pathophysiology of epilepsy Epilepsy is one of the most common neurological diseases and affects about 1% of the population [7]. An epileptic seizure is the result of functional disorders of the brain and is formed as a result of abnormal, excessive bioelectrical discharge in the nerve cells [21]. This disorder can theoretically occur in every population of neurons, but it is often observed in the immediate vicinity of organic brain damage, such as a scar or a tumor. A group of changed, overly excitable nerve cells is called an epileptic focus. The cause of an epileptic seizure is a sudden imbalance between excitatory and inhibitory processes in the neural network [34]. Physiologically, at the cellular and synaptic level, the transmembrane currents and neurotransmitters provide such a balance. Homeostasis is main- tained by the balancing effects of excitatory and inhibitory neurotransmitters and currents: sodium and calcium with chloride and potassium. Ionic conductivity systems and neurotransmitters are closely related because the reaction of neurotransmitters to specific receptors on the cell membrane of neurons causes movement of ions in both directions: from the interior of the neuron to the extracellular space and vice versa. An essential element generating and conditioning nervous system activity is the action potential. It is created as a result of fast intracellular sodium current. This leads to a sudden depolarization of the cell membrane of the neuron and its propagation along the axon, and neurotransmitter release from the presynaptic ending into the synaptic cleft. There, the neurotransmitter connects with receptors of the postsynaptic membrane. Pharmacological Reports, 2013, 65, 555565 555 Depending on the type of neurotransmitter released (excitatory or inhibitory), an action potential is triggered in subsequent neurons (the spread of stimulus) or conduction is blocked when the inhibitory neurotransmitter is released. The effect of the inhibitory neurotransmitter action on ionotropic receptors is hyperpolarization of the neuronal membrane and the release of inhibitory postsynaptic potential (IPSP), and excitatory neurotransmitter - its depolarization and release of excitatory postsynaptic potential (EPSP). The ability to generate action potential by a nerve cell is determined by whether it is “reached” by more EPSP or IPSP from neurons. A well-developed network of connections between inhibitory and excitatory neurons ensures physiological homeostasis in the brain. In pathologic conditions, both intrinsic factors (channelopathies) and extrinsic factors (extracellular environment changes, activity of astrocytes, remodeling of synaptic endings) may contribute to excessive excitability of nerve cells and ultimately lead to epileptic seizure. Long-term imbalance of excitation/inhibition, initiated by various pathological factors, starts the process of epileptogenesis leading to the formation of an active epileptic focus. The condition for the occurrence of an epileptic seizure is excessive bioelectric activity of a group of neurons as well as hypersynchronization of this activity in the cerebral cortex [4]. The gap junctions – formed by directly adjacent cell membranes of neighboring neurons and astrocytes – are an extremely important ultrastructural basis of hypersynchronization of discharges. The transmission of interneuronal information through gap junctions is much faster than transmission through synapses [98]. Another important factor in conditioning hypersynchronization of excitatory discharges is the reorganization of the cortical microarchitecture occurring over time. Epileptogenesis The process of epileptogenesis is usually explained in the literature by the two-hit hypothesis. The term epileptogenesis commonly refers to a period of time from the first hit, such as trauma or stroke, to the occurrence of the first epileptic seizure. It is a chronic process, in which a series of biochemical and structural changes take place in the nerve tissue. Experimental and clinical studies have shown that nerve tis556 Pharmacological Reports, 2013, 65, 555565 sue in experimental animals and in patients with epilepsy, although it does not always show structural changes, differs at the molecular level of normal tissue [63]. During this period, the following processes take place: a process of pathological “learning” of the neurons, pathological reorganization of neural activity, but also the reorganization of the nerve tissue microstructure. According to the latest research, three basic phases can be distinguished in the process of epileptogenesis: acute brain damage (initial insult), latent period with “maturation” of the epileptic focus, and actual epilepsy, where a process called secondary epileptogenesis takes place [77]. The most important etiological factors include severe craniocerebral trauma, where the risk of post-traumatic epilepsy depending on the severity of the injury ranges from 2% to as much as 25% [63]. High risk factors also include: stroke, epileptic state, recurrent and prolonged febrile convulsions, cerebral thrombosis and neuroinfections. Therefore, the neurobiologic basis of epileptogenesis was analyzed in experimental models of such damages [43]. Epileptic focus formation is often explained by the kindling model [68], defined as a progressive increase in neuronal response to rarely used and weak stimulation of a small area in the brain. A stimulus of a subliminal intensity after a certain time causes epileptic discharges at the place of stimulation. If the stimulus is repeated, a process of progressive change begins: first the stimulation causes local, short epileptic discharge, after consecutive stimulation the discharges last longer, spread to larger areas of the brain, and eventually clinical epileptic seizures are observed. This process is dynamic. The interval between successive attacks becomes shorter in untreated patients. Moreover, the primary focus can produce a secondary or mirror focus [53]. The consequence of the socalled initial insult initiating epileptogenesis is immediate and gradually progressive processes of varying course over time. Immediate response involves neuronal activation with intracellular calcium ion accumulation and further stages of excitotoxicity, starting the system of secondary messengers, activation of gene expression and protein synthesis. In the following days, at the site of injury, inflammatory processes take place and mediators of inflammation, glial and endothelial cell responses are activated. At a later stage of epileptogenesis, growth processes occur: the sprouting of new axons, synaptogenesis and angiogenesis. The consequence of these Hippocampus and epilepsy Krzysztof Sendrowski and Wojciech Sobaniec processes is the reorganization of nerve tissue microarchitecture [3]. This is usually a clinically silent period. Sometimes these changes are sufficient for the clinical manifestation of epilepsy, sometimes a second hit is necessary. It may not only be an external factor, such as craniocerebral trauma, but also a “sufficient” level of damage to nerve tissue as a result of the processes of apoptosis and neuronal necrosis and gene expression occurring since the initial insult [67, 77]. The hippocampus and epilepsy Anatomy of hippocampus The hippocampus is an essential part of the archeocortex. In mammals, it is three-layered structure located on the medial surface of the temporal lobe in the back of each cerebral hemisphere. The name hippocampus is derived from Greek and means sea horse, which it resembles in shape. In the literature, it is often referred to as Ammon’s horn (cornu Ammonis), which is derived from the distinctive image of an Egyptian god. The hippocampus is an important part of the limbic system, which plays vital role in the behavioral, emotional and memory processes. The structure of the archeocortex is much simpler than of the neocortex. Histologically, we can divide the hippocampal cortex into four sectors: CA1 – CA4, which vary in size and the amount of nerve cells. The CA1 field contains small pyramidal cells, the small CA2 field is made up of small pyramidal cells, the CA3 field forms a broad, loose band of pyramidal neurons. The CA4 field, also referred to as a hilar region, is formed by loosely structured pyramidal cells, which are surrounded by a U-shaped dark seam of gray matter (dentate gyrus). Individual fields of the hippocampus show differences in the structure and arrangement of nerve connections. Most of the afferent fiber reach the hippocampus through the tractus perforans. They form synapses with the dendrites of pyramidal cells. Some afferent fibers switch in the granular cell layer, whose axons are called mossy fibers, and form synapses with pyramidal cells. In the hippocampus, mossy fibers are only present in the CA3 and CA4 fields. Axons of pyramidal cells form afferent pathways. The main afferent pathways of the hippocampus lead to the corpora mamilaria to the front nuclei of the thalamus and to the hypothalamus. The main hippocampus afferent pathways originate in the enthorinal cortex (EC), the other run from the amygdala and various parts of the neocortex. The EC has connections to other areas of the cerebral cortex. The main output pathway of EC axons project densely to the granule cells in the dentate gyrus; apical dendrites of CA3 get a less dense projection, and the apical dendrites of CA1 get a sparse projection. Thus, the perforant pathway establishes the EC as the main “interface” between the hippocampus and other parts of the cerebral cortex. The dentate granule cell axons (mossy fibers) pass on the information from the EC on thorny spines that exit from the proximal apical dendrite of the CA3 pyramidal cells. Then, the CA3 axons loop up into the region where the apical dendrites are located, extend all the way back into the deep layers of the EC - the Shaffer collaterals completing the reciprocal circuit. Field CA1 also sends axons back to the EC, but these are more sparse than the CA3 projection. Within the hippocampus, the flow of information from the EC is largely unidirectional, with signals propagating through a series of tightly packed cell layers, first to the dentate gyrus, then to the CA3 layer, to the CA1 layer, and next out of the hippocampus to the EC, mainly due to collateralization of the CA3 axons [1]. The hippocampus is an important structure in the pathophysiology of convulsions and epilepsy. Because of its relatively simple histological construction, it is often used in experimental and clinical studies of this disease. The hippocampal cortex contains two major groups of neurons: principal neurons and interneurons. Most principal neurons form excitatory synapses on the cell bodies of other neurons in the remote areas of the brain, whereas interneurons usually form inhibitory synapses on principal neurons and other interneurons. Therefore, they modulate the excitatory effect of the principal neurons and prevent excessive excitation of the neuronal network, thereby preventing the generation of convulsions. With respect to the above anatomy of the hippocampus, the pyramidal neurons are the principal cells. In field CA3, their function is modulated by projections of the granule cells of the dentate gyrus, mossy fibers, synapses of the perforant pathway from the EC, and collaterals from CA3 interneurons. The function of the CA1 sector pyramidal neurons is modulated by the perforant pathway synapses from the EC and Schaffer collaterals of CA3 (Fig. 1). Pharmacological Reports, 2013, 65, 555565 557 Fig. 1. Circulation of nerve impulses between the separates hippocampal structures. Details in the text Temporal lobe epilepsy and hippocampal sclerosis (HS) Temporal lobe epilepsy (TLE) is the most common form of epilepsy in adults [104]. TLE patients have focal seizures, some of which with secondary generalization. In most of these patients, the epileptic focus is located in the medial temporal lobe structures, such as the hippocampus, amygdala and parahippocampal gyrus. Pharmacological treatment of epilepsy often does not provide satisfactory control of seizures. Drug resistance applies to 25–30% of TLE patients. In such cases, the treatment of choice is neurosurgery (anterior temporal lobectomy) [33]. HS is an anatomic basis of medial temporal lobe epilepsy (MTLE), common in experimental models of convulsions and epilepsy as well as in patients with drug-resistant epilepsy [11]. In changed hippocampal nerve tissue, significant histological changes (reorganization of the hippocampus microarchitecture) and functional changes occur. In histological examinations, HS is characterized by degeneration and selective loss of pyramidal neurons, pathological proliferation of interneuron networks, and severe glia reaction [82, 94]. In classical HS, pyramidal cell loss is observed in CA1 and CA3 and around the end-folium, while the cells of sector CA2 are spared. In other less common subtypes of HS, loss of pyramidal neurons occurs in all fields of the hippocampus (total hippocampal sclerosis), or only around the end-folium (end-folium hippocampal sclerosis) [93]. In an experimental model of TLE, Sloviter demonstrated irreversible damage of dentate hilar mossy cells that provide excitatory inputs onto inhibitory interneurons. In contrast, most dentate gyrus inhibitory GABA-basket cells were preserved [87]. On this basis, the author proposed the “dormant basket cell hypothesis”, which explained TLE with impaired inhibi558 Pharmacological Reports, 2013, 65, 555565 tion by “latent (dormant)” GABA interneurons of bioelectrical activity of the principal neurons. The “latency” of these interneurons is due to the lack of their physiological stimulation by damaged hilar mossy cells [88]. In addition to neuronal degeneration and gliosis, the so called mossy fiber sprouting and the dentate gyrus granule cell dispersion are also characteristic of HS [14]. They constitute a histological basis of functional reorganization of the hippocampus manifested by excessive excitation in the abovementioned excitatory reciprocal circuit of nerve impulses EC – dentate gyrus – CA3 – CA1 – EC. Mossy fibers are axons of dentate gyrus granule cells, which physiologically connect with the neurons of the endfolium and hippocampal CA3 sector. If in the process of HS sector CA3 neurons and end-folium neurons are lost, their feedback projection to granule cells will also be lost. The consequence of such deinnervation will be the projection of these axons to neighboring mossy fibers (sprouting). Sprouting will cause reciprocal synaptic stimulation, which may explain the excessive excitability of dentate gyrus neurons observed in temporal lobe epilepsy [91]. Experimental studies have shown that the imbalance of excitation/inhibition between the dentate gyrus and the hippocampus due to the production of even a small number of excitatory collaterals is responsible for persistent neuronal hyperexcitability [21]. The effect of these changes is excessive neuronal excitation stimulating the processes of neuronal epileptogenesis and excitotoxicity. Another histological change in HS is the dispersion of dentate gyrus granule cells. Under physiological conditions, the granular layer cross section has 4–5 cells, whereas in more than 40% of HS the width of the granular layer increases and dispersion of cells may be over 10. Since many of the cells are spindleshaped, resembling migrating embryonic neurons, in the pathogenesis of these changes we take into account the active process of neurogenesis in the subgranular layer. The possibility of neurogenesis in the adult hippocampus has been confirmed in animal models [13, 38] and in humans [35], including in patients with epilepsy [28, 71]. A clinical diagnosis of hippocampal sclerosis (HS) associated with drugresistant temporal lobe epilepsy is based on radiological examination. High-resolution magnetic resonance imaging has the greatest practical importance [18], in particular MR volumetry [19]. Preoperative diagnostics utilize comprehensive exams involving neuroimaging and electrophysiological techniques [48, 70]. Hippocampus and epilepsy Krzysztof Sendrowski and Wojciech Sobaniec Molecular studies in recent years have added additional information on the pathogenesis of TLE and HS. Processes such as synaptic plasticity and glial reaction play an extremely important role. The most important pathogenic factor in synaptic plasticity is the reorganization of the structure and function of neuronal membrane receptors. This applies to both ionotropic and metabotropic receptors [10, 69]. Synaptic plasticity is considered to be an important pathophysiological factor of posttraumatic epilepsy, among others [97]. A patient after severe craniocerebral trauma suffers from a decline in bioelectrical activity in the first phase, which is associated with damage or death of a certain population of neurons. Due to the dynamic process of synaptic plasticity, which may occur in an uncontrolled manner at times, a development of seizure activity takes place in this area [44]. In studies conducted on organotypic cultures of the hippocampus, long-term blocking of the electrical activity of neurons with calcium blockers, tetrodotoxin and NMDA receptor inhibitors, resulted in excessive excitation of neurons. This effect was induced by synaptic plasticity [6]. On the other hand, recurring seizures also induce synaptic plasticity in the brain, which in time further increases the intensity of seizures. It has been shown for example that ictal epileptiform discharges induced by hyperkalemia of the hippocampus culture environment ignited the synaptic plasticity process, which resulted in excessive excitability of the nerve cells leading to progressive epileptogenesis [65]. In an experimental HS model induced by brain injury, changes in the expression of structural proteins of subunits of GABAA receptor have been shown [37]. Both in animal models of epilepsy as well as surgically resected hippocampal tissue from TLE patients, the authors reported a reduced density of ionotropic GABAA receptors associated with a loss of GABAergic inhibitory neurons and a compensatory reorganization of the structure of the receptor’s subunits in the retained nerve cells [90]. Lasoñ et al. also demonstrated a change in the expression of membrane receptors of hippocampal nerve cells for excitatory amino acid receptors, among others, in the chemical kindling model [60] and the pilocarpine and kainic acid-induced seizure model [61]. Mathern et al. also confirmed the reorganization of NMDA receptor expression in TLE patients [74]. Since the 1990s, scientists have focused on the role of metabotropic glutamate receptors (mGluRs) in the process of epileptogenic synaptic plasticity. It turned out that the activa- tion of the mGluR with its chemical agonist ACPD (1-amino-1,3-dicarboxycyclopentane) caused long lasting and synchronous epileptogenic discharges in the neural network of the hippocampal CA3 sector [92]. Subsequent studies have shown that activation of mGluR receptors induces a depolarization-activated, voltage-dependent cationic current, which is responsible for lowering the threshold of excitability of hippocampal neurons and persistent ictal discharges generated in these cells [10, 25]. Role of glia in the pathogenesis of HS and epilepsy Most studies on the patophysiology of temporal lobe epilepsy (TLE) focus on the structure and function of neurons, because of their ability to generate discharges. However, it should be noted that in addition to damage to and loss of neurons, HS is constantly accompanied by glial reaction. It occurs regardless of the experimental epilepsy model. Astrogliosis occurs in over 90% of the surgically resected hippocampus of patients with TLE [95]. Until recently, glia was only considered “brain glue” for neurons. It turned out, however, that glia, and particularly astroglia, plays important functions in the process of neurotransmission [103]. Astrocyte cell membranes have the same receptors as neurons, although their expression is different [52, 101]. For example, the density of potassium channels on the astrocyte cell membrane is much higher than the density of sodium channels, which prevents the generation of action potentials by glia. A very important role is played by Kir4.1 potassium channels belonging to the family of inwardly rectifying K+ (Kir) channels. They cooperate with aquaporin-4 (AQP4) channels, which are unique to astrocytes. The coordinated action of these channels is crucial for the maintenance of water and ion homeostasis in the brain [8, 76, 102], and their dysfunction was implicated in the pathogenesis of epilepsy [45]. The astrocytal network, in contrast with neurons, mainly communicates through gap junctions. These connections allow for rapid uptake of potassium ions and glutamate by astrocytes, which prevents their harmful accumulation in the extracellular space. Glial cells by means of specific excitatory amino acid transporters (EAAT) capture excess excitatory neurotransmitters from the synaptic cleft, thus preventing excitotoxicity processes [96]. Astrocyte cell membranes for neurotransmitters have numerous receptors whose activation leads to excessive intracelPharmacological Reports, 2013, 65, 555565 559 lular Ca2+ accumulation, which can spread to adjacent astrocytes in the form of a “calcium wave”. This process involves the release of neuroactive substances called “gliotransmitters” from active astrocytes [81], which act back on the synapse to regulate the presynaptic function and modulate postsynaptic response [105]. Increased gliotransmitter release, including glutamate, in typical gliosis areas may play a significant role (for HS) in pathological hypersynchronia of neuronal firing [2]. In pathologically changed nervous tissue encountered, for example, in HS, glial cells are actively involved in epileptogenesis. Binder and Steinhäuser found that astrocytes in the HS focuses have a unique structure and function [12]. Bordey and Spencer showed significantly increased activity of excitatory sodium currents through the cell membrane of hippocampal astrocytes in patients with HS [17]. On the surface of astrocytes analyzed in the hippocampal tissue of patients with HS, severe expression of genes encoding proteins involved in the release of glutamate was also demonstrated [62]. Other authors have also described significant abnormalities in potassium channels and the function of potassium channel complexes with the aquaporin channel in HS. Kivi et al. demonstrated decreased expression of potassium channels in pathological hippocampal tissue, compared with normal tissue [54]. Recent studies also indicate that mutations in the KCNJ10 gene encoding the Kir4.1 potassium channel are associated with the varying clinical morphology of epileptic seizures [42]. In the hippocampus of patients with TLE associated with HS, a loss of perivascular Kir4.1 channels has been demonstrated [41]. Failure of the sclerotic hippocampus to buffer excess potassium ions in the extracellular space, impaired function of the transporters for excitatory amino acid and glutamine synthetase activity – an enzyme that converts glutamate to glutamine – contribute to increased neuronal hyperexcitation, neurotoxicity, and the spread of convulsive activity [31]. HS: cause or effect of epilepsy? Despite the well-studied histological and ultrastructural basis of HS, its pathophysiology remains unclear. Whether HS is a primary cause of focal epilepsy or maybe the result of repeated epileptic seizures is still an unanswered question [47]. 560 Pharmacological Reports, 2013, 65, 555565 In generally accepted theory and aforementioned epileptogenesis two-hit hypothesis, the initial insult of even a small area of nerve tissue of the brain caused by various etiological factors leads to a stretched over time sequence of histological and biochemical changes in the area of damage, a so-called maturation of the epileptic focus. Subsequent even small second hits activate the focus and cause epilepsy. In relation to this theory, the main factors that initiate HS and epileptogenesis are severe head trauma, perinatal trauma, history of early childhood status epilepticus or prolonged or recurrent febrile seizures [73]. The latter is the most frequently cited cause of HS [23]. In experimental febrile convulsions, severe pathological lesions were observed in preparations of rat brain, especially within the hippocampus [46]. In an experimental model of febrile seizures conducted at our institution, we have shown that recurrent hyperthermic seizures cause loss of more than a half of the pyramidal neurons in CA1 and CA3 sectors of the hippocampus, but in contrast with HS, without accompanying gliosis [85]. In the same experiment, in electron microscopic tests, we also found significant ultrastructural abnormalities in the blood-brain barrier in the hippocampal cortex [66]. Reports on patients with epilepsy are ambiguous, even though the vast majority of them indicate an increased risk of epilepsy in children with febrile seizures [9, 100], and brain MR examinations show pathological lesions in the hippocampus of children with a history of prolonged febrile seizures, particularly focal [83, 99]. In a study analyzing a large group of 572 patients with TLE, Mathern et al. demonstrated that in most cases the occurence of TLE and HS was preceded by an initial precipitating injury. In the young, the dispersion of granule cells and sprouting of axons dominated in the pathology of hippocampus, which would rather suggest a developmental basis of HS [72]. An interesting issue in some patients with drug resistant TLE is a so-called “dual pathology”. It is based on the coexistence of HS (usually mild) and abnormal epileptogenic changes situated beyond the hippocampus [64]. This problem affects 5–30% of patients with drug resistant TLE [24]. A known example of clinical “dual pathology” is the coexistence of severe HS and cortical heterotopia, which in this case could also indicate the “congenital” evolving nature of HS. Over 100 years ago, Gowers postulated that “seizures beget seizures” [39]. According to this theory, is HS and corresponding TLE not the result of repeated Hippocampus and epilepsy Krzysztof Sendrowski and Wojciech Sobaniec subclinical discharges or prolonged epilepsy or status epilepticus? In experimental studies, histopathological changes similar to HS were observed in the kindling model [20, 22] and experimental kainic or pilocarpine acidinduced status epilepticus [27]. Interestingly, injection of kainic acid into immature rats did not produce substantial loss of hippocampal pyramidal cells or mossy fiber sprouting in contrast with the changes caused by the substance in adult rats [89]. A similar insensitivity to damage to the hippocampus in immature animals was observed in the kindling model [40]. These facts may explain the low sensitivity to excitotoxicity associated with immaturity of excitatory amino acid receptors and kainic acid in the brain of young animals and active neurogenesis [80]. However, more recent studies indicate that in the model of kainate seizures in the hippocampus of immature animals, a synaptic reorganization of sector CA3 and the subiculum occurs [29]. This leads to an increase in impulse conduction in sections CA3-CA1, activation of subsequent micro sections of the hippocampus, and the effect of hypersynchronization of bioelectrical activity of neurons necessary for the onset of epilepsy in the future [56]. Studies on the temporal lobe specimens of patients who died as a result of status epilepticus showed a significant loss of pyramidal neurons at sectors CA1 and CA3 and hippocampus hilus, therefore, the changes are similar to those of classical HS [30]. Damage to the hippocampus has also been reported in the MR of patients with frequent seizures in the course of cryptogenic, drug resistant TLE [49, 50]. Taking into account the above data, the answer to the question whether HS is the result or the cause of drug-resistant epilepsy should be that both concepts are true and supported by numerous scientific literature. It seems that, in the pathogenesis of HS, innate predisposing factors to such pathology as well as repetitive, uncontrolled seizures are equally important. HS and antiepileptic drugs HS is characterized by three pathological histological changes: loss of neurons, glial reaction (gliosis), and remodeling of neuronal networks especially interneurons (sprouting). Therefore, it is interesting to question whether and how antiepileptic drugs (AEDs) may prevent HS. AED mechanisms of action are mainly based on their effects on ion channels (sodium and calcium), excitatory and inhibitory amino acid receptors, inhibition of GABA metabolism and synaptic transmission [58]. All of these elements lead to the inhibition theory of excessive excitatory neurotransmission, resulting in so-called excitotoxicity and associated neuronal death. Since the major pathological changes of hippocampal nerve cells are found in sectors CA1 and CA3, characterized by the highest expression of the receptors of glutamic and kainic acid [26], the loss of these neurons occurs most likely in the mechanism of aponecrosis induced by excitotoxicity processes [75]. These neurons, especially those located around the hippocampal hilus, are fast-spiking inhibitory cells. Their loss disrupts the balance of excitation/inhibition, which enables uncontrolled discharge of excitatory neurons. In experimental studies, performed at our institution, effective neuroprotective AED activity was demonstrated in cultures of hippocampal neurons [84, 86]. Clinical experience suggests, however, that pharmacological treatment of epilepsy in many patients with TLE associated with HS is ineffective. The treatment of choice is neurosurgery (anterior temporal lobectomy), after which recurrent seizures are rare and AEDs can be safely discontinued [78]. The available AEDs can indeed prevent damage to neurons by inhibiting excitotoxicity processes, but their impact on other elements of HS, i.e., the sprouting of axons and glial reaction, is small. We can therefore conclude that AEDs inhibit pathological neuronal discharge, i.e., act as an anticonvulsant, but they do not prevent epileptogenesis. Recent experimental studies performed on immature rats genetically predisposed to epilepsy, however, have shown the potential antiepileptogenic effect of levetiracetam and ethosuximide [79]. Although promising antiepileptogenic effects of various chemicals e.g., immunosuppressants, antiinflammatory drugs, neurotrophins and erythropoietin were observed in several preclinical studies (for review, see [55]), these compounds have not found practical use as antiepileptogenic agents yet. Eid et al. indicate a key role in the pathogenesis of HS not only of glutamate and the excitotoxicity trail, but also glia [32]. Recent studies have shown that the characteristic (for HS) astrogliosis is associated with overexpression of adenosine kinase, which enhances spontaneous bioelectric activity of neurons. The hardened tissue also showed reduced hippocampal expression of adenosine A1 receptors, which play an impor- Pharmacological Reports, 2013, 65, 555565 561 tant role in inhibitory neurotransmission [15]. The possibilities to modulate gene expression of astrocyte membrane receptors, especially potassium channels, and effect on adenosine kinase may be interesting in the search for AEDs with new mechanisms of action [16]. With regard to the mechanisms of action of AEDs and structural and functional abnormalities occurring in HS, there is a very interesting new issue in epigenetics, i.e., the possibility of AEDs modulating the gene structure of nerve tissue cells [5]. This occurs through the neuronal plasticity discussed previously [59]. Commonly used to treat epilepsy valproic acid has the ability to inhibit histone deacetylase, an enzyme crucial for the regulation of histone acetylation, chromatin remodeling and gene expression [57]. The intensification by valproic acid of acetylation of histones H3 and H4 and the associated change transcription of genes [36] can attenuate excitotoxicity processes and thus degeneration and neuronal death [51]. In summary, the hippocampus fulfills an extremely important role in the pathogenesis of epilepsy and convulsions. The majority of patients with drug resistant TLE have a characteristic pathology of the brain structure – HS, characterized by loss of pyramidal neurons, severe glial reaction and remodeling of neuronal networks. Studies on the pathogenesis of HS, supported by numerous literature on the subject, do not provide a clear answer to the question whether HS is a cause or consequence of repeated seizures. We believe that both concepts are true and should be treated as of equal importance. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. References: 1. Amaral D, Lavenex P: “Chapter 3. Hippocampal Neuroanatomy”. In: The Hippocampus Book. Eds. Andersen P, Morris R, Amaral D, Bliss T, O’Keefe J, Oxford University Press, New York, 2006. 2. Angulo MC, Kozlov AS, Charpak S, Audinat E: Glutamate released from glial cells synchronizes neuronal activity in the hippocampus. J Neurosci, 2004, 24, 6920–6927. 3. Arellano JI, Munoz A, Ballesteros-Yanez I, Sola RG, DeFelipe J: Histopathology and reorganization of chandelier cells in the human epileptic sclerotic hippocampus. Brain, 2004, 127, 45–64. 4. Avoli M, Louvel J, Pumain R, Köhling R: Cellular and molecular mechanisms of epilepsy in the human brain. Prog Neurobiol, 2007, 77, 166–200. 5. Baer-Dubowska W, Majchrzak-Celiñska A, Cichocki M. Pharmacoepigenetics: a new approach to predicting indi- 562 Pharmacological Reports, 2013, 65, 555565 19. 20. 21. 22. 23. vidual drug responses and targeting new drugs. Pharmacol Rep, 2011, 2, 293–304. Bausch SB, He S, Petrova Y, Wang XM, McNamara JO: Plasticity of both excitatory and inhibitory synapses is associated with seizures induced by removal of chronic blockade of activity in cultured hippocampus. J Neurophysiol, 2006, 96, 2151–2167. Bell GS, Sander JW: The epidemiology of epilepsy: the size of the problem. Seizures, 2001, 10, 306–314. Benfenati V, Caprini M, Dovizio M, Mylonakou MN, Ferroni S, Ottersen OP, Amiry-Moghaddam M: An aquaporin-4/transient receptorpotential vanilloid 4 (AQP4/TRPV4) complex is essential for cell-volume control in astrocytes. Proc Natl Acad Sci USA, 2011, 108, 2563–2568. Berg AT, Shinnar S, Levy SR, Testa FM: Childhoodonset epilepsy with and without preceding febrile seizures. Neurology, 1999, 53, 1742–1748. Bianchi R, Chuang S-C, Zhao W, Young SR, Wong RKS: Cellular plasticity for group I mGluR-mediated epileptogenesis. J Neurosci, 2009, 29, 3497–3507. Bidziñski J: Hippocampus – anatomical substrate of temporal lobe epilepsy. Epileptologia, 2007, 15, 149–161. Binder DK, Steinhäuser C: Functional changes in astroglial cells in epilepsy. Glia, 2006, 54, 358–368. Bizon JL, Gallagher M: Production of new cells in the rat dentate gyrus over the lifespan: relation to cognitive decline. Eur J Neurosci, 2003, 18, 215–219. Blümcke I, Thom M, Wiestler OD: Ammon’s horn sclerosis: a maldevelopmental disorder associated with temporal lobe epilepsy. Brain Pathol, 2002, 12, 199–211. Boison D: Adenosine dysfunction in epilepsy. Glia, 2012, 60, 1234–1243. Boison D: The adenosine kinase hypothesis of epileptogenesis. Prog Neurobiol, 2008, 84, 249–262. Bordey A, Spencer DD: Distinct electrophysiological alterations in dentate gyrus versus CA1 glial cells from epileptic humans with temporal lobe sclerosis. Epilepsy Res, 2004, 59, 107–122. Bronen RA, Cheung G, Charles JT, Kim JH, Spencer DD, Spencer SS, Sze G, McCarthy G: Imaging findings in hippocampal sclerosis: correlation with pathology. Am J Neuroradiol, 1991, 12, 933–940. Casino GD, Jack CR Jr, Parisi JE, Sharbrough FW, Hirschorn KA, Meyer FB, Marsh WR, O’Brien PC: Magnetic resonance imaging-based volume studies in temporal lobe epilepsy: pathological correlations. Ann Neurol, 1991, 30, 31–36. Cavazos JE, Das I, Sutula TP: Neuronal loss induced in limbic pathways by kindling: evidence for induction of hippocampal sclerosis by repeated brief seizures. J Neurosci, 1994, 14, 3106–3121. Cavazos JE, Sanchez R: Pathophysiology of seizures and epilepsy. Neurol Dis Ther, 2004, 64, 5–20. Cavazos JE, Sutula TP: Progressive neuronal loss induced by kindling: a possible mechanism for mossy fiber synaptic reorganization and hippocampal sclerosis. Brain Res, 1990, 527, 1–6. Cendes F, Andermann F, Dubeau F, Gloor P, Evans A, Jones-Gotman M, Olivier A et al.: Early childhood febrile convulsions, atrophy and sclerosis of mesial struc- Hippocampus and epilepsy Krzysztof Sendrowski and Wojciech Sobaniec 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. tures, and temporal lobe epilepsy: an MRI volumetric study. Neurology, 1993, 43, 1083–1087. Cendes F, Cook MJ, Watson C, Andermann F, Fish DR, Shorvon SD, Bergin P et al.: Frequency and characteristics of dual pathology in patients with lesional epilepsy. Neurology, 1995, 45, 2058–2064. Chuang S-C, Bianchi R, Wong RKS: Group I mGluR activation turns on a voltage-gated inward current in hippocampal pyramidal cells. J Neurophysiol, 2000, 83, 2844–2853. Cotman CW, Monaghan DT: Anatomical organization of excitatory amino acid receptors and their properties. In: Excitatory Amino Acids in Epilepsy. Eds. Schwarz R, Ben-Ari Y, Plenum Press, New York, 1986, 237–252. Covolan R, Ribeiro LT, Longo BM, Mello LE: Cell damage and neurogenesis in the dentate granule cell layer of adult rats after pilocarpine- or kainite-induced status epilepticus. Hippocampus, 2000, 10, 169–180. Crespel A, Rigau V, Coubes P, Rousset MC, de Bock F, Okano H, Baldy-Moulinier M et al.: Increased number of neural progenitors in human temporal lobe epilepsy. Neurobiol. Dis, 2005, 19, 436–450. Cross DJ, Cavazos JE: Synaptic reorganization in subiculum and CA3 after early-life status epilepticus in the kainic acid rat model. Epilepsy Res, 2007, 73, 156–165. DeGiorgio CM, Tomiyasu U, Gott PS, Treimann DM: Hippocampal pyramidal cell loss in human status epilepticus. Epilepsia, 1992, 33, 23–27. Eid T, Thomas MJ, Spencer DD, Runden-Pran E, Lai JC, Malthankar GV, Kim JH et al.: Loss of glutamine synthetase in the human epileptogenic hippocampus: Possible mechanism for raised extracellular glutamate in mesial temporal lobe epilepsy. Lancet, 2004, 363, 28–37. Eid T, Williamson A, Lee TS, Petroff OA, de Lanerolle NC: Glutamate and astrocytes-key players in human mesial temporal lobe epilepsy? Epilepsia, 2008, 49 Suppl 2, 42–52. Engel J Jr: Mesial temporal lobe epilepsy: what have we learned? Neuroscientist, 2001, 7, 340–352. Engelborghs S, D’Hooge R, De Deyn PP: Pathophysiology of epilepsy. Acta Neurol Belg, 2000, 100, 201–213. Eriksson PS, Perfilieva E, Bjork-Eriksson T, Alborn A-M, Nordborg C, Peterson DA, Gage FH: Neurogenesis in the adult human hippocampus. Nat Med, 1998, 4, 1313–1317. Fukuchi M, Nii T, Ishimaru N, Minamino A, Hara D, Takasaki I, Tabuchi A, Tsuda M: Valproic acid induces up- or down-regulation of gene expression responsible for the neuronal excitation and inhibition in rat cortical neurons through its epigenetic actions. Neurosci Res, 2009, 65, 35–43. Gibson CJ, Meyer RC, Hamm RJ: Traumatic brain injury and the effects of diazepam, diltiazem, and MK-801 on GABA-A receptor subunit expression in rat hippocampus. J Biomed Sci, 2010, 17, 38. Gould E, Tanapat P, McEwen BS, Flugge G, Fuchs E: Proliferation of granule cell precursors in the dentate gyrus of adult monkeys is diminished by stress. Proc Natl Acad Sci USA, 1998, 95, 3168–3171. 39. Gowers WR: Epilepsy and Other Chronic Convulsive Diseases: Their Causes, symptoms and Treatment. Churchill, London, 1901. 40. Haas KZ, Sperber EF, Opanashuk LA, Stanton PK, Moshé SL: Resistance of immature hippocampus to morphologic and physiologic alterations following status epilepticus or kindling. Hippocampus, 2001, 11, 615–625. 41. Heuser K, Eid T, Lauritzen F, Thoren AE, Vindedal GF, Taubøll E, Gjerstad L et al.: Loss of perivascular Kir4.1 potassium channels in the sclerotic hippocampus of patients with mesial temporal lobe epilepsy. J Neuropathol Exp Neurol, 2012, 71, 814–825. 42. Heuser K, Nagelhus EA, Taubøll E, Indahl U, Berg PR, Lien S, Nakken S et al.: Variants of the genes encoding AQP4 and Kir4.1 are associated with subgroups of patients with temporal lobe epilepsy. Epilepsy Res, 2010, 88, 55–64. 43. Holtkamp M, Meierkord H: Anticonvulsant, antiepileptogenic, and antiictogenic pharmacostrategies. Cell Mol Life Sci, 2007, 64, 2023–2041. 44. Houweling AR, Bazhenov M, Timofeev I, Steriade M, Sejnowski TJ: Homeostatic synaptic plasticity can explain post-traumatic epileptogenesis in chronically isolated neocortex. Cereb Cortex, 2005, 15, 834–845. 45. Jabs R, Seifert G, Steinhäuser C: Astrocytic function and its alteration in the epileptic brain. Epilepsia, 2008, 49, Suppl 2, 3–12. 46. Jiang W, Duong TM, de Lanerolle NC: The neuropathology of hyperthermic seizures in the rat. Epilepsia, 1999, 40, 5–19. 47. Johns P, Thom M: Epilepsy and hippocampal sclerosis: cause or effect? ACNR, 2008, 8, 16–18. 48. Kabay SC, Gumustas OG, Dirican AC, Ozden H, Guven G, Keskinkilic C, Dincer A, Baybas S: Proton magnetic resonance spectroscopy and cognitive functions in temporal lobe epilepsy patients with hippocampal sclerosis and magnetic resonance imaging negative patients. Epileptologia, 2010, 18, 61–71. 49. Kalviainen R, Salmenpera T: Do recurrent seizures cause neuronal damage? A series of studies with MRI volumetry in adults with partial epilepsy. Prog Brain Res, 2002, 135, 279–95. 50. Kalviainen R, Salmenpera T, Partanen K, Vainio P, Riekkinen P, Pitkänen A: Recurrent seizures may cause hippocampal damage in temporal lobe epilepsy. Neurology, 1998, 50, 1377–1382. 51. Kanai H, Sawa A, Chen RW, Leeds P, Chuang DM: Valproic acid inhibits histone deacetylase activity and suppresses excitotoxicity-induced GAPDH nuclear accumulation and apoptotic death in neurons. Pharmacogenomics J, 2004, 4, 336–344. 52. Kettenmann H, Steinhäuser C: Receptors for neurotransmitters and hormones. In: Neuroglia 2nd edn. Eds. Kettenmann H, Ransom BR, Oxford University Press, Oxford, 2005, 131–145. 53. Khalilov I, Holmes GL, Yehezkel BA: In vitro formation of a secondary epileptogenic mirror focus by interhippocampal propagation of seizures. Nat Neurosci, 2003, 6, 1079–1085. 54. Kivi A, Lehmann TN, Kovacs R, Eilers A, Jauch R, Meencke HJ, von Deimling A et al.: Effects of barium Pharmacological Reports, 2013, 65, 555565 563 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 564 on stimulus-induced rises of [K+]o in human epileptic non-sclerotic and sclerotic hippocampal area CA1. Eur J Neurosci, 2000, 12, 2039–2048. Kobow K, Auvin S, Jensen F, Loscher W, Mody I, Potschka H, Prince D et al.: Finding a better drug for epilepsy: antiepileptogenesis targets. Epilepsia, 2012, 11, 1868–1876. Koh S, Storey TW, Santos TC, Mian AY, Cole AJ: Early-life seizures in rats increase susceptibility to seizure induced brain injury in adulthood. Neurology, 1999, 53, 915–921. Langley B, Gensert JM, Beal MF, Ratan RR: Remodeling chromatin and stress resistance in the central nervous system : histone deacetylase inhibitors as novel and broadly effective neuroprotective agents. Curr Drug Targets CNS Neurol Disord, 2005, 4, 41–50. Lasoñ W, Dudra-Jastrzêbska M, Rejdak K, Czuczwar SJ. Basic mechanisms of antiepileptic drugs and their pharmacokinetic/pharmacodynamic interactions: an update. Pharmacol Rep, 2011, 2, 271–292. Lasoñ W, Jantas D: The role of epigenetics in pathomechanisms and epilepsy treatment. Epileptologia, 2009, 17, 113–122. Lasoñ W, Turchan J, Przew³ocka B, Labuz D, Machelska H, Przew³ocki R: Effects of pentylenetetrazol kindling on glutamate receptor genes expression in the rat hippocampus. Brain Res, 1998, 785, 355–358. Lasoñ W, Turchan J, Przew³ocki R, Machelska H, Labuz D, Przew³ocka B: Effects of pilocarpine and kainateinduced seizures on N-methyl-D-aspartate receptor gene expression in the rat hippocampus. Neuroscience, 1997, 78, 997–1004. Lee TS, Mane S, Eid T, Zhao H, Lin A, Guan Z, Kim JH et al.: Gene expression in temporal lobe epilepsy is consistent with increased release of glutamate by astrocytes. Mol Med, 2007, 13, 1–13. Leœkiewicz M, Lasoñ W: The neurochemical mechanisms of temporal lobe epilepsy: an update (Polish). Przegl Lek, 2007, 64, 960–964. Levesque MF, Nakasato N, Vinters HW, Babb TL: Surgical treatment of limbic epilepsy associated with extrahippocampal lesions: the problem of dual pathology. J Neurosurg, 1991, 75, 364–370. Lopantsev V, Both M, Draguhn A: Rapid plasticity at inhibitory and excitatory synapses in the hippocampus induced by ictal epileptiform discharges. Eur J Neurosci, 2009, 29, 1153–1164. £otowska JM, Sobaniec-£otowska ME, Sendrowski K, Sobaniec W, Artemowicz B: Ultrastructure of the bloodbrain barrier of the gyrus hippocampal cortex in an experimental model of febrile seizures and with the use of a new generation antiepileptic drug – topiramate. Folia Neuropathol, 2008, 46, 57–68. £ukasiuk K, D¹browski M, Adach A, Pitkänen A: Epileptogenesis-related genes revisited. Prog Brain Res, 2006, 158, 223–241. Majkowski J: Kindling: clinical relevance for epileptogenicity in humans. Adv Neurol, 1999, 81, 105–113. Malenka RC, Nicoll RA: NMDA-receptor-dependent synaptic plasticity: multiple forms and mechanisms. Trends Neurosci, 1993, 16, 521–527. Pharmacological Reports, 2013, 65, 555565 70. Martinez M, Santamaria J, Mercader JM, Catafau A, Cardenal C, Lomena F: Correlation of MRI hippocampal volume analysis, video/EEG monitoring and inter- and postictal single emission tomography in refractory focal epilepsy. Neuroradiology, 1994, 36, 11–16. 71. Marucci G, Giulioni M, Rubboli G, Paradisi M, Fernández M, Del Vecchio G, Pozzati E: Neurogenesis in temporal lobe epilepsy: Relationship between histological findings and changes in dentate gyrus proliferative properties. Clin Neurol Neurosurg, 2013, 115, 187-191. 72. Mathern GW, Adelson PD, Cahan LD, Leite JP: Hippocampal neuron damage in human epilepsy: Meyer’s hypothesis revisited. Prog Brain Res, 2002, 135, 237–251. 73. Mathern GW, Babb TL, Armstrong DL: Hippocampal sclerosis. In: Epilepsy: A Comprehensive Textbook. Eds. Engel JJ, Pedley TA, Lippincot-Raven, Philadelphia, 1997, 133–155. 74. Mathern GW, Pretorius JK, Mendoza D, Leite JP, Chimelli L, Born DE, Fried I et al.: Hippocampal Nmethyl-D-aspartate receptor subunit mRNA levels in temporal lobe epilepsy patients. Ann Neurol, 1999, 46, 343–358. 75. Meldrum BS: Excitotoxicity and selective neuronal loss in epilepsy. Brain Pathol, 2008, 3, 405–412. 76. Nielsen S, Nagelhus EA, Amiry-Moghaddam M, Bourque C, Agre P, Ottersen OP: Specialized membrane domains for water transport in glial cells: high-resolution immunogold cytochemistry of aquaporin-4 in rat brain. J Neurosci, 1997, 17, 171–180. 77. Pitkanen A, £ukasiuk K: Mechanisms of epileptogenesis and potential treatment targets. Lancet Neurol, 2011, 10, 173–186. 78. Rathore C, Panda S, Sarma PS, Radhakrishnan K: How safe is it to withdraw antiepileptic drugs following successful surgery for mesial temporal lobe epilepsy? Epilepsia, 2011, 52, 627–635. 79. Russo E, Citraro R, Scicchitano F, De Fazio S, Di Paola ED, Constanti A, De Sarro G: Comparison of the antiepileptogenic effects of an early long-term treatment with ethosuximide or levetiracetam in a genetic animal model of absence epilepsy. Epilepsia, 2010, 51, 1560–1569. 80. Sankar R, Shin D, Liu H, Katsumori H, Wasterlain CG: Granule cell neurogenesis after status epilepticus in the immature rat brain. Epilepsia, 2000, 41, S53–S56. 81. Scemes E, Giaume C: Astrocyte calcium waves: what they are and what they do. Glia, 2006, 54, 716–725. 82. Schiffer D, Cordera S, Tereni A: Neuropathological findings in surgical specimens of temporal lobe epilepsy. Crit Rev Neurosurg, 1994, 4, 339–350. 83. Scott RC, King MD, Gadian DG, Neville BG, Connelly A: Hippocampal abnormalities after prolonged febrile convulsion: a longitudinal MRI study. Brain, 2003, 126, 2551–2557. 84. Sendrowski K, Boækowski L, Sobaniec W, I³endo E, Jaworowska B, Œmigielska-Kuzia J: Levetiracetam protects hippocampal neurons in culture against hypoxiainduced injury. Folia Histochem Cytobiol, 2011, 49, 148–152. 85. Sendrowski K, Sobaniec W, Sobaniec-£otowska ME, Artemowicz B: Topiramate as a neuroprotectant in the Hippocampus and epilepsy Krzysztof Sendrowski and Wojciech Sobaniec 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. experimental model of febrile seizures. Adv Med Sci, 2007, 52, Suppl 1, 161–165. Sendrowski K, Œmigielska-Kuzia J, Sobaniec P, I³endo E, Artemowicz B: Survival of cultured hippocampal neurons upon hypoxia: neuroprotective effect of gabapentin. Child Neurol, 2011, 41, 25–28. Sloviter RS: Decreased hippocampal inhibition and a selective loss of interneurons in experimental epilepsy. Science, 1987, 235, 73–76. Sloviter RS: Permanently altered hippocampal structure, excitability, and inhibition after experimental status epilepticus in the rat: the dormant basket cell hypothesis and its possible relevance to temporal lobe epilepsy. Hippocampus, 1991, 1, 41–66. Sperber EF, Haas KZ, Stanton PK, Moshé SL: Resistance of the immature hippocampus to seizure-induced synaptic reorganization. Brain Res Dev Brain Res, 1991, 60, 88–93. Sperk G, Wieselthaler-Hoelzl A, Drexel M: Altered GABAA Receptor Subunit Composition in Temporal Lobe Epilepsy. Encyclopedia of Basic Epilepsy Research. Elsevier, London, 2009, 1351–1356. Sutula TP, He XX, Cavazos J, Scott G: Synaptic reorganization in the hippocampus induced by abnormal functional activity. Science, 1998, 239, 1147–1150. Taylor GW, Merlin LR, Wong RKS: Synchronized oscillations in hippocampal CA3 neurons induced by metabotropic glutamate receptor activation. J Neurosci, 1995, 15, 8039–8052. Thom M: Recent advances in the neuropathology of focal lesions in epilepsy. Expert Rev Neurother, 2004, 4, 973–984. Thom M: Hippocampal sclerosis: progress since Sommer. Brain Pathol, 2009, 19, 565–572. Thom M, Sisodiya SM, Beckett A, Martinian L, Lin WR, Harkness W, Mitchell TN et al.: Cytoarchitectural 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. abnormalities in hippocampal sclerosis. J Neuropathol Exp Neurol, 2002, 61, 510–519. Tian GF, Azmi H, Takano T, Xu Q, Peng W, Lin J, Oberheim M et al.: An astrocytic basis of epilepsy. Nat Med, 2005, 11, 973–981. Timofeev I, Bazhenov M, Avramescu S, Nita DA: Posttraumatic epilepsy: the roles of synaptic plasticity. Neuroscientist, 2010, 16, 19–27. Traub RD, Michelson-Law H, Bibbig AE, Buhl EH, Whittington MA: Gap junctions, fast oscillations and the initiation of seizures. Adv Exp Med Biol, 2004, 548, 110–122. Van Landingham KE, Heinz ER, Cavazos JE, Lewis DV: MRI evidence of hippocampal injury after prolonged, focal febrile convulsions. Ann Neurol, 1998, 43, 413–426. Verity CM, Golding J: Risk of epilepsy after febrile convulsions: a national cohort study. Br Med J, 1991, 303, 1373–1376. Verkhratsky A, Steinhäuser C: Ion channels in glial cells. Brain Res Rev, 2000, 32, 380–412. Verkman AS: More than just water channels: unexpected cellular roles of aquaporins. J Cell Sci, 2005, 118, 3225–3232. Volterra A, Meldolesi J: Astrocytes, from brain glue to communication elements: the revolution continues. Nat Rev Neurosci, 2005, 6, 626–640. Williamson PD, Engel J Jr: Complex partial seizures. In: Epilepsy: A Comprehensive Textbook. Eds. Engel J Jr, Pedley TA, Lippincott-Raven Publishers, Philadelphia, 1997, 557–566. Zhang J, Wang H, Ye C, Ge W, Chen Y, Jiang Z, Wu CP et al.: ATP released by astrocytes mediates glutamatergic activity dependent heterosynaptic suppression. Neuron, 2003, 40, 971–982. Received: November 8, 2012; in the revised form: March 10, 2013; accepted: March 13, 2013. Pharmacological Reports, 2013, 65, 555565 565