Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuroplasticity wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Executive functions wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Embodied language processing wikipedia , lookup
Cortical cooling wikipedia , lookup
Biology of depression wikipedia , lookup
Human brain wikipedia , lookup
Environmental enrichment wikipedia , lookup
Neuroesthetics wikipedia , lookup
Nonsynaptic plasticity wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Nervous system network models wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Biological neuron model wikipedia , lookup
Spike-and-wave wikipedia , lookup
Neuroeconomics wikipedia , lookup
Aging brain wikipedia , lookup
Long-term depression wikipedia , lookup
Signal transduction wikipedia , lookup
NMDA receptor wikipedia , lookup
Synaptogenesis wikipedia , lookup
End-plate potential wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Chemical synapse wikipedia , lookup
Neurotransmitter wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
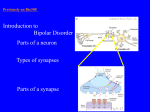
Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat *Please note that this lecture and the upcoming two lectures are not present in the book. Hence, these notes are your primary resource. This lecture is basically about the cerebral cortex and higher intellectual functions, neurotransmitters and the fast neurotransmitter glutamate. The Cerebral Cortex and Higher Intellectual Functions: The cerebral cortex is the outermost layer of the brain which consists of FIVE lobes: 12345- Frontal Parietal Temporal Occipital Insula (A hidden lobe found deep behind the parietal and frontal lobes) Each lobe of the cortex has a function. The frontal lobe, for instance, has the prefrontal cortex (will be discussed further later on) which is responsible for the personality of the individual, his thinking abilities and behavior. The occipital lobe is divided into several functional visual areas and is therefore responsible for the vision. Giving each lobe a certain function is quite challenging so the cortex of the brain was divided into three types according to their function. These three are: 1) Primary cortex 2) Secondary cortex 3) Association cortex 1|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat 1) Primary cortex - It’s the site that first receives the information as an impulse. This impulse is in the form of an action potential. If there is an action potential then the primary area receives information if not then there is no information received and hence no sensation. e.g. primary visual cortex in the occipital lobe enables you to see , primary somatosensory (postcentral gyrus- colored blue in the slides), primary motor (precentral gyrus- refer to slides), primary gustatory (to taste) and so on… 2) Secondary cortex - It’s responsible for the processing of the information received by the primary cortex. In other words, it helps in understanding the sensation received. - The primary visual area 17 enables you to see but the secondary areas 18 and 19 help you understand what you’re seeing. - Together, the primary and secondary cortex, receive and process the sensation. For example, you can smell food and know the source of the smell- does it smell good or not? 3) Association cortex - It’s a large part and forms most of the cortex and each area has a particular function. (Almost all areas are association except 17,18,19, 1,2,3,4,… which are primary and secondary areas) - It’s responsible for the higher order processing. 2|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat - Your primary and secondary areas help you see, smell and hear. But it’s the association area that connects the sensations together. For example, someone speaking to you in Arabic, you hear (auditory) that he’s speaking in Arabic and so you respond to him (speech) in the same language. Another examples are Broca’s area and Wernicke’s area (responsible for the language). - Most common association areas in the brain are the prefrontal and parietal areas that link more than one sense to produce higher complex information. - Prefrontal cortex refers to the anterior part of the frontal lobe. It contains areas (9,10,11). As mentioned earlier in the first page, the functions of the prefrontal cortex are thinking, determining the personality, behavior, intentions… Consequences of damage of any of the areas: Primary cortex damage: No sensation. e.g. damage to visual primary area blindness damage to primary auditory area deafness damage to somatosensory area no touch or pain sensation Secondary cortex damage: There is sensation but no understanding of it. e.g. One can hear a sound but doesn’t understand what it is. One can smell something but can’t tell if it’s pleasant or unpleasant? *** What happens when the primary motor area is damaged? What happens when the secondary motor area is damaged? In the motor areas, unlike the sensory, the processing happens BEFORE the action. The primary area is responsible for the simple movements. The secondary is responsible for the processing and more skillful 3|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat moves. So, when the primary area (Area 4) is damaged it causes paralysis. On the other hand, when the secondary area is damaged simple movements (voluntary- writing, pushing, pulling…) remain while skilled and complex moves are lost since they require planning and processing. The secondary area (Area 6) is called the premotor area because processing happens before (pre-) the motor action. Area 6 receives the information and then 4. Damage to the secondary sensory cortex is called Agnosia. Damage to the secondary motor cortex is called Apraxia. Association Area Damage loss of higher complex abilities ** Damage to the prefrontal cortex (Recall: the functions of the prefrontal cortex are personality determination, behavior, higher functions…etc) In the 1860s, a railroad construction worker had an accident where a large iron rod was driven into his head destroying his prefrontal cortex. Since the respiratory and cardiovascular centers are in the medulla and the pain, sensory and motor areas are behind the prefrontal cortex; he survived and didn’t lose any of his senses or motion. However, his personality and behavior changed severely as a result of his injury. Note: The subcortical is responsible for one’s emotion but what controls the emotion is mainly the prefrontal cortex. An example to get a better understanding of this is when you feel angry-- it’s the subcortical’s job. However, whether you respond to this feeling of 4|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat anger by hitting someone or not, for example, is controlled by your personality which is the prefrontal cortex’s role. Therefore, damage to the prefrontal cortex causes lack of foresight (no predicting), frequent stubbornness, inattentive and moody behavior, lack of ambitions, sense of responsibility and sense propriety(rude) and finally less creativity and inability to plan for the future. Synapses and Neurotransmitters • We know that the brain consists of neurons in which an action potential is transmitted. These neurons intercommunicate by synapses. A synapse is a specialized site of contact, and transmission of information between a neuron and an effector cell. • There are two types of synapses: Chemical and Electrical. The main synapses present in the brain are chemical synapses. Chemical Synapses: One neuron releases neurotransmitter molecules into a small space (the synaptic cleft) that is adjacent to another neuron. Steps: The process begins with a wave of electrochemical excitation called an action potential travelling along the membrane of the presynaptic cell, until it reaches the synapse. Calcium ion channels open allowing the entry of calcium ions into the presynaptic neuron. This high concentration of Ca-ions causes the release of neurotransmitters by 5|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat exocytosis via synaptic vesicles which bind to their chemical receptors and transmits its effect on the postsynaptic neuron. Finally, the neurotransmitter is either reabsorbed by the presynaptic cell, and then repackaged for future release, or else it is broken down metabolically by enzymes. Synapses depend greatly on the postsynaptic neuron’s receptors rather than on the type of neurotransmitters. The type of receptors determines the effect of the released neurotransmitter. There are two types of receptors (both are ligand-gated, ligand receptors and neurotransmitter binding):1- Ionotropic Receptors (Ion channel receptors) They open ion channels. - Opening Na+ or Ca++ channels causes depolarization (influx of ions) and hence EXCITATION. It approaches and overcomes the threshold causing an action potential. - Opening K+ or Cl- channels causes hyperpolarization (outflow of ions) and hence INHIBITION. It becomes more negative becoming distant from the threshold value. 2- Metatropic Receptors (Second messenger receptors) - Can open specific ion channels (If Na+ excitation, if K+ inhibition), Activates cAMP or cGMP, Activation of one or more intracellular enzymes, Activation of gene transcription. - Once the neurotransmitter binds to the receptor it either activates an excitatory G protein which increases cAMP production or an inhibitory G protein which decrease the production of cAMP. 6|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat - Other second messenger such as PLC. Differences Between Ionotropic and Metatropic Receptors Ionotropic Metatropic Faster Slower Lasts longer Signal Amplification is possible Special to certain DNA to allow transcription and synthesis of the coded protein. Drugs and the Synapse As pharmacy students, it’s very important to learn the effects of drugs on synaptic transmission. As said before, the post synaptic effect depends mainly on the type of receptors present on the post synaptic neuron. Therefore, drugs either work as AGONISTS, ANTAGONISTS or ALLOSTERIC MODULATORS. Agonist: a chemical that binds to a receptor and activates the receptor to produce a biological response (activation). They mimic (copy) the effect of the neurotransmitter. * The neurotransmitter is the most potent (effective) agonist. Antagonist: drugs that block the effects of neurotransmitters (no activation). (It does not oppose the receptor’s action, it just block the receptor) When both are present, the activation and effect are less. E.g. we have 20 receptors, 20 agonists and antagonists with the same binding power. 10 agonists will bind to 10 receptors and the same for the other 10 antagonists. So, a lower effect is produced (in this case half the effect). 7|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat Potency (efficacy): The efficacy of the drug is its tendency to activate the receptor. E.g. antagonists display no efficacy (potency) to activate the receptors they bind. Neurotransmitters have a high potency (efficacy) that’s why they are most potent agonists. Affinity: A drug has an affinity for a particular type of receptor if it binds to that receptor. This affinity varies from strong to weak. Allosteric Modulation: a substance which indirectly influences (modulates) the effects of a chemical (neurotransmitter, drug, agonist…) on a specific receptor. As you can see in the picture the presence of alcohol (ethanol) increased the effect of the neurotransmitter GABA by increasing the size of the passage way (allowing the entrance of more Cl- ions) and makes it last for a longer period of time. The allosteric modulator binds to a site different than that of the neurotransmitter increasing the effect (whether it’s excitatory or inhibitory). When making the drug it’s important to know the following about the neurotransmitter: - Rate limiting step Clearance and inactivation Location and pathway (which part of the brain it will affect?) Dysfunction and CNS pathology The synthesized drug will work by doing one or more of the following to the neurotransmitter: - Increasing the synthesis 8|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat - Causing vesicles to leak Increasing release Decreasing uptake Blocking the breakdown into inactive chemical Directly stimulating or blocking postsynaptic receptors Neurotransmitters: - Are chemicals found in the human’s cells that transmit signals across a synapse from a presynaptic neuron to a postsynaptic neuron. - There are many ways to classify neurotransmitters. - We will classify them as fast and slow neurotransmitters. Fast are those that have ion channels mainly as their receptors and slow are the ones that have mainly metatropic receptors. Metatropic receptors involve second messengers which are called ‘modulators’ since they alter protein synthesis. - Glutamate (L-glutamic acid) is an example of a fast neurotransmitter that we shall discuss shortly. Glutamate: - Fast neurotransmitter Main excitatory neurotransmitter in the mammalian CNS. 95% of excitatory synapses in the brain are glutamatergic Precursor for the neurotransmitter GABA which is the major inhibitory neurotransmitter - Its enzymatic pathway (refer to slides) shows that glutamate is made from the amino acid glutamine and that glutamate is the precursor for the production of GABA. - Glutamate receptors may be ionotropic (majority) or metatropic (minority) 9|Page Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat Ionotropic Receptors of Glutamate: There are three types: 1- NMDA receptor 2- AMPA receptor 3- KAINATE receptor All three are channels for Na+ and Ca++ ions (excitatory) and are present of the postsynaptic neuron. However, NMDA allows the passage of calcium ions more than sodium ions. AMPA allows the passage of sodium ions more than calcium ions. KAINATE receptors, on the other hand, are the only ones that are present on the presynaptic neuron. The reason is to self-regulate the neurotransmitter realease. In most cases, presynaptic receptors (not KAINATE and Glutamate’s case) allow the binding of the neurotransmitter when its concentration increases in the synaptic cleft. Consequently, it prevents the release more of the neurotransmitter. It gives it a break-like period. In the case of KAINATE receptors on the presynaptic neuron and glutamate, the KAINATE allows the entry of Ca++ ions into the PREsynaptic neuron. As we know, the entry of Calcium ions into the PREsynaptic neuron releases more of the neurotransmitter. Termination of signal: Glutamate neurotransmitter’s effect is terminated (ended) by glial cells (mainly astrocytes) which convert it back to its precursor, the amino 10 | P a g e Physiology 2 - Sheet #6 - Dr.Loai Al-Zgoul - Done by: Yara Zreiqat acid glutamine. Glutamine is then transferred to the presynaptic neuron which uses it again to synthesize glutamate and so on. Glutamate and CNS disorders: Stroke Ischemia: is a restriction in blood supply to tissues, causing a shortage of oxygen and glucose supply to the cells which in turn stops the production of ATP. Glial cells have transporters which use ATP to reuptake the glutamate. When there is no ATP, glutamate molecules accumulate in the synaptic cleft which continue binding to the receptors (NMDA and AMPA receptors) and allowing the entry of Na+ and mainly Ca++ ions causing excitation. This is known as excitotoxicity. This leads to the death (apoptosis) of that area of the brain. There is a certain drug that is given in the early 20-30 minutes to decrease defect neurons in stroke patients. This drug blocks the receptors (NMDA and AMPA) so it’s NMDA and AMPA antagonist. However, it blocks mainly NMDA receptors since they allow the entry of Ca++ ions more than AMPA. Calcium ions are a main cause of apoptosis so that’s why this drug is mainly a NMDA antagonists. 11 | P a g e