Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Nervous system network models wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Neural oscillation wikipedia , lookup
Limbic system wikipedia , lookup
Perivascular space wikipedia , lookup
Time perception wikipedia , lookup
Biology of depression wikipedia , lookup
Neurogenomics wikipedia , lookup
Development of the nervous system wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Neuroplasticity wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Metastability in the brain wikipedia , lookup
Environmental enrichment wikipedia , lookup
Aging brain wikipedia , lookup
Central pattern generator wikipedia , lookup
Neuroeconomics wikipedia , lookup
Optogenetics wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Anatomy of the cerebellum wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Embodied language processing wikipedia , lookup
Muscle memory wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Synaptic gating wikipedia , lookup
Substantia nigra wikipedia , lookup
The BasalGanglia Consist of Fom Nuclei
The Striatum, the Input Nucleus to the Basal Ganglia Is
Heterogeneous in Both lts Anatomy and Function
The StriaturnProjectsto the Output Nuclei via Direct
and Indirect Pathways
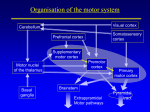
The BasalGanglia Are the Principal Subcortical Compone ts
of a Family of Parallel Circuits Linking the Thalamus
and Cerebral Cortex
The SkeletomotorCircuit EngagesSpecificPortions
of the CerebralCortex,BasalGanglia,and Thalamus
Single Cell RecordingStudiesProvide Direct Insight' to
the Role of the Motor Circuits
Studies of the Oculomotor Circuit Provided Importan
Insight Into How the SkeletomotorCircuit Operates
Same Movement Disorders Result From Imbalances
in the Direct and Indirect Pathwaysin the BasalGanglia
Overactivity in the Indirect PathwayIs a Major Factor
in ParkinsonianSigns
The Level of Dopamine in the Basal Ganglia Is Decrea ed
in Parkinson Disease
Underactivity in the Indirect PathwayIs a Major Facto
in Hyperkinetic Disorders
Huntington DiseaseIs a Heritable Hyperkinetic Disorder
The Gene for Huntington DiseaseHas BeenIdentified
Glutamate-lnduced Neuronal Cell DeathContributes
to Huntington Disease
The BasalGanglia Also Have a Role in Cognition, Mood,
and Nonmotor Behavior Function
An Overall View
r
r
E BASAL
GANGLIA
CONSIST
of fouT nuclei, portions
f which play a major role in normal voluntary
ovement. Unlike mostother components of the
motor ystem, however, they do not have direct input or
output connections with the spinal cord. These nuclei
receiv their primary input trom the cerebral cortex and
send t eir output to the brain stem and, via the thalamus, b ck to the prefrontal, prernotor, and motor cortices. he motor functions of the basal ganglia are
therefo mediated, in large part, by motor areasof the
frontal ortex.
C' 'cal observations fiTst suggested that the basal
gangli areinvolved in the control of movement and the
produc 'on of movement disorders. Postmortem E~xamination f patients with Parkinson disease,Huntington
disease and hemiballismus revealed pathological
change in these subcortical nuclei. Thesediseasel;have
three c aracteristic types of motor disturbances: (1)
tremor and other involuntary movements; (2) changes
in pos re and muscle tone; and (3) poverty and slownessof ovement without paralysis. Thus, disorders of
the bas I ganglia may result in either diminished movement ( s in Parkinson disease)or èxcessivemovement
(as in untington disease). In addition to these disorders 0 movement, damage to the basal ganglia is
associa d with complex neuropsychiatric cognitive and
behavi ral disturbances, reflecting the wider role of
these n clei in the diverse functions of the frontallobes.
Pri arily becauseof the prominence of movement
abno
lities associated with damage to the basal
ganglia they were believed to be major componentsof a
motor ystem, independent of the pyramidal (or
corticos inal) motor system, the "extrapyramidal" motor syst m. Thus, two different motor syndromes were
,
854
Part VI / Movement
i
~
~;,
.'
~
~
Jft"
Fi!
in
Ni
s~
m
distinguished: the pyramidal tract syndrome,characterized by spasticity and paralysis, and theextrapyramidal
syndrome,characterized by involuntary movements,
muscular rigidity, and immobility without paralysis.
Thereare severalreasonswhy this simple classification is no longer satisfactory. First, we now know that,
in addition to the basal ganglia and corticospinal
systems,other parts of the brain participate in voluntary
movement. Thus, disorders of the motor nuclei of the
brain stem, red nucleus, and cerebellum also result in
disturbances of movement. Second,the extrapyramidal
and pyramidal systems are not truly independent but
are extensively interconnected and cooperate in the
control of movement. Indeed, the motor actions of
the basal ganglia are mediated in large part through
the supplementary, prernotor, and motor cortices via the
pyramidal system.
Becausethey are so common, disorders of the basal
ganglia have always been important in clinical neurology. Parkinson diseasewas the first diseaseof the nervous system to be identified as a molecular disease
caused by a specific defect in transmitter metabolism.
Therefore, in addition to providing important informa-
tion about~ otor control, the study of diseased basal
ganglia ha provided a paradigm fOT studying the
relationshi of transmitters to disorders of mood, cogrtition, and nonmotor behavior, topics that wilt be
consideredin detail in Chapters 60 and 61. Theuse Di:a
variety of 1natomical, molecular, and neural imaging
techniquesras weIl as animal models of basal ganglia
~
as led
to
major
advances
in
understanding
diSOrders
the
orga
.ation
and
function
of
the
baBa!
tb
tiro
~
.:,
~
(I
::
v,
J\\.
bi
St
~':~ cl
ganglia.
These insi hts have, in turn, led to new pharmacologic
and neuro urgical approachesto treatment of diseases
of the baBa ganglia.
il
h
A
e
The Basa}Ganglia Consist of Four Nuclei
b
b
The basal,anglia consistof severalinterconnected subcortical nuflei with major projections to the cerebralcortex, thala~ us, and certain brain stem nuclei. They re-
a
ceive
majo
input
trom
the cerebral
cortex
and
thalamus
and send heir output back to the cortex (via the thalamus) and to the brain stem (Figure 43-1). Thus, the
basal gan lia are major components of large cortical-
Cc
n
g
t-
h
1;
,
"-f
""..,..4
~
;,
~
Chapter43 / The ~asalGanglia
855
m
\,,~
I:/:
Corpus
callosum
Lateral ventricle
Caudate nucleus
Thalamus
Putamen
Globus pallidus:
External segment
Internal segment
InternaIcapsule
I
Claustrum ~
-Subthalamic
nucleus
Amygdala -
-Substantia
Basal
ganglia
nigra
Figure 43-2 This coronal section shows the basal ga~glia
in relation to surrounding structures. (Adapted trom
Nieuwenhuys et al. 1981.)
I
subcortical reentrant circuits linking cortex and tata
mus.
The four principal nuclei of the basalganglia
(1 )
the striatum, (2) the globus pallidus (or pallid
), (3)
the substantia nigra (consisting of the pars reti ata
and pars compacta), and (4) the subthalamic nu leus
(Figure 43-2). The striatum consistsof three imp rtant
subdivisions: the caudatenucleus, the putamen, an the
ventral striatum (which includes the nucleus ac
bens). Except at its most anterior pole, the stria
is
divided into the caudate nucleus and putamen b the
internal capsule,a major collection of fibers that
between the neocortex and thalamus in both dire ons.
All three subdivisions of the striatum have a co
on
embryological origin.
The striatum is the major recipient of inputs t the
basal ganglia from the cerebral cortex, thalamus, and
brain stem. lts neurons project to the globus pal idus
and substantianigra. Togetherthese two nuclei, w ose
cell bodies are morphologically similar, give rise t the
major output projections from the basal ganglia. The
globus pallidus lies medial to the putamen, just la eral
to the intemal capsule,and is divided into external and
internal segments. The intemal pallidal segment i related functionally to the pars reticulata of the subst tia
nigral which lies in the midbrain on the medial side of
the ifternal capsule. The cells of the internal pallidal
se ~
nt and pars reticulata use -y-aminobutyric acid
(GA A) as a neurotransmitter. Just as the caudate nucleus is separated fIom the putamen by the internal
caps~ e, the internal pallidal segment is separated fIom
the s bstantia nigra.
addition to its reticular portion, the substantia nigra al 0bas a compactzone (pars compacta).This zone is
a dis ct nucleus that lies dorsal to the pars reticulata althou someof its neuronslie within the pars reticulata.
The c lls of the pars compactaare dopaminergic and also
cont neuromelanin,a dark pigment derived fIom oxidized and polymerized dopamine. Neuromelanin,
whi accumulateswith agein large lysosomal granules
in cel bodies of dopaminergic neurons,accounl.. for the
dark ~iscoloration of tros structure. Dopaminergic cells
area$ O found in the ventral-tegmental
area, a medial extensi
of the pars compacta.
e subthalarnic nucleus is closely colmected
anato 'cally with both segmentsof the globus pallidus
and, e substantia nigra. It lies just below the thalamus
and a ove the anterior portion of the substantia nigra.
The utaminergic cells of tros nucleus are the only
excita~oryprojections of the basalganglia.
~
~
The striatum, the Input Nucleus to the Basal
Gan ia, Is Heterogeneous in Both lts Anatomy
and unction
AII ~reas of cortex send excitatory, glutaminergic projectiqns to specific portions of the striatum. The striaturn ~so receives excitatory inputs Eromthe intralaminar nuclei of the thalamus, dopaminergic pfl)jections
Dopamine
fro
the
raph
nuclei.
~
,
I
\
\
~
I
Direct
pathway
facilitates
movement
Indir ct
path ay
inhibi 5
mov ment
I
I
\
I
\
I
I
Î
\
\
I.
,
,
,
,
I
I
Pytamen
midbrain,
and
serotonergic
input
from
the
lthough the striatum appears homogeneous on
rou. e staining, it is anatomically and furu:tionally
high heterogeneous.It consists of two separate palts,
the '1atrix and striosomecompartments (the latter aIso
refer~d to as patches).Thesecompartments differ histoche~caIly Eromone another and Rave different receptors. ifhe striosome compartment receives its Dlajor input tom limbic cortex and projects primaril~{ to the
substbntia nigra pars compacta.
IthoUgh the striatum contains several disl:inct cell
type 90-95% of them are GABA-ergic mediuJm-spiny
proje tion neurons. Thesecells are both major targets of
corti
input and the sole source of output. They are
large y quiescent except during movement or in respo
to peripheral stimuli. In primates the mediumspiny neurons of the striatum cao be subdivided into
two roups. Those thai project to the external pallidal
segm nt express the neuropeptides enkephalin and
neu tensin; those thai project to the internal pallidal
segm nt or substantia nigra pars reticulata express
subst nce Pand dynorphin.
e striatum aIso contains two types of local inhibit ry interneurons: large cholinergic neurc'ns and
small r cells thai contain somatostatin,neuropeptide Y,
or ni ic oxide synthetase.Both classesof inhibitory interne roos have extensive axon collateraIs thai reduce
the ac 'vity of the striatal output neurons. AlthoUgh few
in nu~ber, they are responsibie for most of the tonic activity ~ the striatum.
Gord
The ~triatum Projects to the Output Nuclei via
Direct and Indirect Pathways
Figure 43-3 The anatomic connections of the oasal
ganglia-thalamocortical
circuitry, indicating the paralle direct and indirect pathways from the striatum to the bas I
ganglia output nuclei. Two types of dopamine receptors { 1
and D2) are located on different sets of output neurons in he
striatum that give rise to the direct and indirect pathways. nhibitory pathways are shown as gray arrows; excitatory p thways, as pink arrows. GPe = external segment of the glo us
pallidus; GPi = internal segment of the globus pallidus; S c =
substantia nigra pars compacta; STN = subthalamic nucle s.
The 0 output nuclei of the basal ganglia, the intemal
pallid I segment and the substantia nigra pars reticulata, t nically inhibit their target nuclei in the thalamus
and b ain stem. This inhibitory output is thought to be
modu ated by two parallel pathways that run fI~omthe
stria m to the two output nuclei: one direct and the
other. direct. The indirect pathway passesfust to the
exte al pallidal segmentand from there to the 5ubthalamic ucleus in a purely GABA-ergic pathway, and finally rom the subthalamic nucleus to the output nuclei
Chapter43 / The BasalGari!;lia
I
1
1f
I
i
i:
1
(
~
"
in an excitatory glutaminergic projection (Figu 43-3).
The projection trom the subthalamic nucleus is e only
excitatory intrinsic connection of the basal gan lia; all
others are GABA-ergic and inhibitory.
The neurons in the two output nuclei dis alge
tonically at high frequency. When phasic excitat ry inputs transiently activate the direct pathway fr
the
striatum to the pallidum, the tonically active n~urons
in the pallidum are briefly suppressed, thus Itrmitting the thalamus and ultimately the cortex [to be
activated. In contrast, phasic activation of the i direct
pathway transiently increases inhibition of the thalamus, as can be determined by considering the olarity of the connectionsbetween the striatum and e external pallidal segment, between the external se ment
and the subthalamic nucleus, and betweenthe sub alamic nucleus and the internal pallidal segment ( igure
43-3).
Thus, the direct pathway can provide positivefeedback and the indirect pathway negativefeedback the
J
circuit between the basal ganglia and the thal us.
5: \ These efferent pathways h~ve opposing effects 0 ~e
basal ganglia output nucleI and thus on the th aInlC
,
targets of thesenuclei. Activation of the direct pa war
disinhibits the thalamus, thereby increasing thaI 0..cortical
activity, whereas activation of the indirect ath;
war further inhibits thalamocortical neurons. A~ a re:
sult,
i
"
C
movement, whereas activation of the indirect pa war
inhibits movement.
The two striatal output pathways are affecte dif-
,
,,;
~
Motor
Limbif~ ~
/'
""'"
,
~\
)
~
~
/.
~
\'i~
J
:
Ot
c'.(.
Ocul~mator
\1
pretrorc
/'
~"
y
p'
~~
./
r
activation
of
the
direct
pathway
faci
\;
~
Figure 43-4 The frontallobe
targets of the basal gangliathalamocortical
circuits. ACA = anterior cingulate area;
DLPcl= dorsolateral prefrontal cortex; FEF = frontal e've field;
LOFcl= lateral orbitofrontal
cortex; MC = primary motor corcortex; PMC = premotor cor.
tex; ~ OFC = medial orbitofrontal
tex; S F = supplementary
eye field; SMA = supplementary
motor area.
tates
by thepars
dopaminergic
projection
trom the
".ferently
stantia nigra
compacta to
the striatum.
S subiatal
~
I~~~
~
~
857
neurons that project directly to the two output n clei
have Dl dopamine receptors that facilitate trans .ssion, while those that project in the indirect pa
y
have D2 receptors that reduce transmission.
Although their synaptic actions are different, the
dopaminergic inputs to the two pathways lead t the
same effect-reducing inhibition of the thalamocor .cal
neurons and thus facilitating movements initiate in
the cortex. We can now seehow depletion óf dopa ne
in the striatum, asoccurs in Parkinson disease,maf eaJ
to impaired movement. Without the dopaminergi action in the striatum, activity in the output nucle. in~
creases.This increased output in turn increases. .bition of the thalamocortical neurons that othe .se
facilitate initiation of movement. Dopamine gic
synapsesare also found in the pallidum, the sub
amic nucleus, and the substantianigra. Dopaminergi action at thesesites, and in the cortex, could further odulate the actions of the direct and indirect path ars
trom the striatum.
The ~asal Ganglia Are the Principal
SubQOrticalComponents of a Family of
Para~lelCircuits Linking the Thalamus
and tere bral Cortex
The bfsal ganglia were traditionally thought to function
only ~ voluntary movement. Indeed, fOTsome time it
W= s b lieved that the basal ganglia sent their entire output to the motor cortex via the thalamus and thus act as
a
I through which movement is initiated by different C~ .cal areas. It is now widely accepted, however,
that
ough
their
interaction
with
the
cerebral
cortex
the ba al ganglia also contribute to a variety of behaviors 0 er than voluntary movement, including skeletomotor'loculomotor, cognitive, and even emotional functions. I
Seyeral observations point to diversity of function.
First, c~rtain experimental and disease-relatedlesionsof
adverse
emotional
and
cognithe bt 1 ganglia produce
live
e
erts.
This
was
fiTst
recognized
in
patient:s
with
Hun. gton. disease. Patients with Par~on
diseas.e
also h ve dlsturbances of affect, behavlor, and cogmtion.
cond, the basal ganglia have extensive and
'\
858
Part VI / Movement
highly organized connections with virtually the enti
putamen. Gijventhe highly topographic connectionsbecerebral cortex, as weIl as the hippocampus and amyg
tween th s~aturn and the pallidurn and between the
dala. Finally, a wide range of motor and nonmotor be
pallidum n~ the subthalarnicnucleus, it is unlikely that
haviors have been correlated with activity in individua
there is s gztificant convergence between neighboring
basalganglia neuronsin experimental animals and wi
circuits. ere is, however, sorne anatornical evidence
metabolic activity in the basalganglia as geenby imag
that the .~its convergeto sornedegreein the substaning studies in humans.
tia nigra r$ reticulata.
The basal ganglia may be viewed as the principa
subcortical components of a family of circuits linkin
the thalamus and cerebral cortex. These circuits ar
The Skel to~otor Circuit Engages Specific Portions
largely segregated, bath structurally and functionally.
Each circuit originates in a specific area of the
of the Cer bral Cortex, Basal Ganglia, and Thalamus
cerebral cortex and engages different portions of the
Since mo e~ent disorders are prominent in diseai,es
basal ganglia and thalamus. The thalamic output of
of the bas I ganglia, it is appropriate here to focus on
each circuit is directed back to the portions of the frontal
the skelet motor circuit. In primates the skeletomolobe from which the circuit originates. Thus, the skeletotor circuit ri~ates in the cerebral cortex in precentral
motor circuit begins and ends in the precentral motor
motor fie ds and postcentral somatosensory areas
fields (the premotor cortex, the supplementary motor
and projec s ~argelyto the putamen. The putamen is
area,and the motor cortex); the oculomotorcircuit, in the
thus an im ortant site for integration of movement refrontal and supplementary ere fields; the prefrontal
lated and s~nsory feedback information related to
circuits, in the dorsolateral prefrontal and lateral ormovement. ]he putamen receives topographic probitofrontal cortices;and the limbic circuit, in the anterior
jections fr
the primary motor cortex and premotor
cingulate area and medial orbitofrontal cortex (Figure
areas, incl dmg the arcuate premotor area and the
43-4). Each area of the neocortex projects to a discrete
supplemen ary motor area. Somatosensoryareas 3a, 1,
region of the striatum and does so in a highly topo2, and 5 pr jeft in an overlapping manner to the motor
graphic manner. Association areas project to the cauportions 0 !he putamen. Topographically organized
date and rostral putameI\; sensorimotor areas project
projections from each cortical area result in a somatoto most of the central and caudal putamen; and limbic
topic orga 'z~tion of movement-related neurons in
areas project to the ventral striatum and olfactory
the putam. The leg is represented in a dorsolateral
tubercle.
zone, the 0 of~cial region in a ventromedial zone, and
The concept of segregated basal gangliathe arm in zpne between the two (Figure 43-5). Each
thalamocortical circuits is a valuable anatomic and
of these rep &entationsextends along virtually the 'enphysiologic framework tor understanding not only the
tire
rostroc uqal axis of the putamen. Recentanatomidiverse movement disorders associatedwith basalgancal and ph iqlogical data indicate that the skeletomoglia dysfunction but also the many-faceted neurologic
tor circuit is further subdivided into severiu
and psychiatric disturbances resulting from basal ganindependen ~ubcircuits, each centered on a specific
glia disorders. Structural convergence and functional
precentral otor field.
integration occur within, rather than between, the five'
Output e~ronsin the putamen project topograpmidentified basal ganglia-thalamocortical circuits. For excally to the a,doventral portions of bath segmentsof
ample, the skeletomotor circuit has subcircuits centered
the pallidu $nd to the caudolateral portions of the
on different precentral motor fields, with separate sosubstantia gr~ pars reticulata. In turn, the motor pormatotopic pathways tor control of leg, arm, and orofations of the' temal pallidal segmentand substantia rucial movements.
gra pars reti u~atasend topographic projections to speWithin each of these subunits there may even be .
cific thalami n~clei, including three ventral nuclei-the
discrete pathways responsible tor different aspects of
ventrallater I nucleus (pars oralis) and the lateral venmotor processing. Injection of transsynaptically transtral anterior nQclei(pars parvocellularis and pars magported herpes simplex virus that is transmitted in the
nocellularis ~nd the centromedian nucleus (see Figretrograde direction into the primary motor cortex,
ure 18-4fOTt e iorganizationof the thalamic nuclei). The
supplementary motor area, and lateral premotor area
skeletomoto circuit is then closed by projections from
results in labeling of distinct populations of output neuthe ventraIl tetal and ventral ant.erior(pars magnocelrons in the internal pallidal segment(see Figure 5-9 tor
lularis) nucl i to the supplementary motor area, from
technique). Virus transported in the anterograde directhe
lateré\l tItal anterior (pars parvocellularis) and the
tion was labeled in distinctly separate regions of the
ventrallater I J!iucleito the premotor cortex, and frolll
I
"
i:i
j,
~
ti
c
e
c.
c.
F
s
r
11
f
f
{i;h
;;,~
"
I
lî
The
;anglia
:hapter4:
the ventrallateral and centromedian nuclei to the pre
centra! motor fields.
Basa]
859
;MA
\
Single Cell Recording Studies Provide Direct
Insight into the Role of the Motor Circuits
The contribution of the basalganglia to move ent
can be assessedmost directly by studying the activi of
neurons within the skeletomotor circuit of behaving rimates, especially activity in the intemal segmentof the
pallidum, the principal output nucleus, The onse of
rapid, stimulus-triggered limb movementsis procee ed
fust by changesin neuronal firing in the motor cir its
of the cortex and only later in the basal ganglia, Thi sequential firing suggests that a serial processing oc rs
within the basal ganglia-thalamocortical circuits d
that much of the activity within these circuits is initia ed
at the corticallevel.
During the executionof a specific motor act, su as
wrist flexion or extension, the normally high late of
spontaneousdischarge in movement-related neuro in
the intemal pallidal segment becomes even higher in
the majority of cells, but in Borneit decreases.Neur ns
that exhibit phasic decreasesin discharge maf pla a
crucial role in movement by disinhibiting the ventrol teral thalamus and thereby gating or facilitating co 'cally initiated movements (via excitatory thalamoco .cal connections). Populations of neurons that sh w
phasic increases in discharge would have the op 0site effect, further inhibiting thalamocortical n rons and thus suppressing antagonistic or competi g
movements.
Little is known about how movement-related si nals from the direct and indirect pathways are in grated in the intemal pallidal segmentto control ba
ganglia output. One possibility, of course,is that si
s
associatedwith a particular voluntary movement are irected over both pathways to the same population f
pallidal neurons. With this arrangement, the inpu
fIom the indirect pathway might assist in braking r
possibly smoothing the movement, while th~se in
direct pathway simultaneously facilitate the moveme t.
This reciprocal regulation would be consistent with e
basal ganglia's apparent role in scalingthe amplitude r
velocity of movement. Alternatively, the direct and ind rect inputs associatedwith a particular movement coul
be directed to separatesetsof neurons in the output n clei of the basàlganglia. In this configuration, the skel tomotor circuit might play a dual role in modula .
voluntary movements by both reinforcing the selecte
pattem (via the direct pathway) and suppressingpote tially conflicting patterns (via the indirect pathway .
This dual role could result in focusin~the neural activi
Figure 43-5 The somatotopic
organization
of the basal
ganglia-thalamocortical
motor circuit is illustrated
in these
mesial and lateral views of a monkey brain, as weil as the
basal garilglia and thalamus.
The motor circuit is dividèd into
a "face" epresentation
(blue), "arm" representation
(dark
green). a d 'Ileg" representation
(light green). Arrows
SI-IOW
subcircuit
within the port ion of the motor circuit concerned
with the rm, CM = centromedian
nucleus of the thalamus;
GPe = e er[1al segment of the globus pallidus; GPi = internal
segment
f the globus pallidus; MC = primary motor cortex;
PMC = P frontal motor cortex; SMA = supplementary
motor
area; STN = 'subthalamic nucleus; VApc = parvocellular
portion of th ventral anterior nucleus of the thalamus; VLo = pars
oralis of t e ventrolateral
nucleus
of the thalamus.
thai med'ates each volunt~ movement in a war similar to the ï4ïbitory surround described for various sensory syst ms.
Neuron activit;y within the skeletemotor circuit has
beenex .ed in monkeys performing a variet;y of motor tasks At all stages of th~ circuit (cortical, striatal,
and palli at) the activit;y of substantial proportions of
mov~me t-trelatedneurons depends upon the direction
of limb ovement, independent of the pattem of mus-
"
860
Part VI / Movement
Chapter 43 / The Basal Gangllia
'\
~,.
;i
~
.
:
,
..Ic.
~
"
cle activity. These directional cells comprise 30- 0% of
the movement-related neurons in the supplem ntary
motor area,motor cortex, putamen, and pallidum. All of
these neurons are arranged somatotopically. In e motor cortical, but not in the basal ganglia many ovement-related cells have been found whose firin does
depend on the pattern of muscle activity. In train d primates,the activity in arm-related neurons of the' ernal
pallidal segment also is clearly correlated with mplitude and velodty.
Studies combining behavioral training and s' glecell recording indicate that the skeletomotor circui is involved not only in the execution but also in the p epartion for movement. In the precentral motor 'elds,
including the premotor cortex, supplementary otor
area, and motor cortex, striking changes in dis alge
late occur in Borneneurons aftel the presentatio of a
cue that spedfies the direction of limb movement to be
executedlater. Thesechangesin activity persist un' the
movement-triggering stimulus is presented. The thus
representa neural correlateof one of the preparato aspects of motor control referred to as "motor set" ( hapter 38).
Directionally selective activity before mov ment
also occurs within the putamen and the interna segment of the pallidum. Individual neurons within ese
structures tend to exhibit eitherpreparatory (set-re ated)
or movement-related responses,suggesting tha the
preparation and executionof motor action are me iated
by separatesubchannelsin the skeletomotor dr it. In
the internal segmentof the pallidum subpopulati ns of
neurons that receive input fIom the suppleme tary
motor area tend to exhibit set-like preparato responses. However, neurons receiving inputs fro the
motor cortex tend to exhibit phasic, movement-re ated
responses. These different response patterns
er
support the idea that the skeletomotor circuit is omposed of distinct subcircuits that connect to diff rent
precentral motor fields (motor cortex, suppleme tary
Figure 43-6 (Opposite) The basal ganglia-thalamocort
cal
circuitry under normal conditions and in Parkinson dis ase,
hemiballism, and chorea. Inhibitory connections are sho n as
gray and black arrows; excitatory connections, as pink a d
red. Degeneration of the nigrostriatal dopamine pathway i
Parkinson disease leads to differential changes in activity i the
two striatopallidal projections. indicated by changes in the darkness of the connecting arrows (darker arrows indicate increased neuronal activity and lighter arrows, decreased a tivity). Basal ganglia output to the thalamus is increased in
Parkinson disease and decreases in ballism and chorea. G e =
external segment of the globus pallidus; Gpi = internal se ment of the globus pallidus; SNc = substantia nigra pars ompacta; STN = subthalamic nucleus.
861
mot r rrea, and arcuate premotor area). These subcircuit ~ay have distinctive roles in motor contral and in
the atf'ogenesisof specific motor signs and s)rmptoms
that c(;ur in Parkinson diseaseand other diseasesof the
basa g{mglia.
Stu ies of the Oculomotor Circuit Provided
Imp riant Insight Into How the Skeletomotor
Circ .i~Operates
The c4Iomotor circuit is involved in the control of saccadi
e movements. It originates in the frontal and
suF le entary motor ere fields and projects to the
bod 0 the caudale nucleus. The caudale ntLcleusin
turn
jects via the direct and indirect pathways to the
later I portions of the substantia nigra pars rE!ticulata,
whi projects back to the frontal ere fields as v"ell as to
the s perior colliculus. Inhibition of tonic activity in the
Bubsantia nigra pars reticulata disinhibits output neurons' R e deep layers of the superior colliculu.s whose
~
acti
ty is associated
with
saccades.
Inactivation
of neu-
rons in the pars reticulata results in involuntary saccade t the contralateral side. These observati'Dnsprovide the critical clue that the skeletomoto:r circuit
mig similarly disinhibit thalamocortical neurons phasicall during movement, thus facilitating the intended
mov ment.
$
SO
Movement Disorders Result
Fro Imbalances in the Direct and Indirect
Path ars in the Basal Ganglia
Cons d~rable progresshas been made in understanding
the ecranisms underlying the major movement disorders f the basalganglia. Hypokineticdisorders(of which
Parki Bon disease is the best-known example) are
char ~rized by impaired initiation of mclvement
(akin ia~ and by a reduced amplitude and vel.ocity of
vol tatY movement (bradykinesia).They are usually
acco p,nied by muscular rigidity (increasedresistance
to pa sive displacement)and tremor.
yperkinetic disorders(exemplified by HUIltington
disea e and hemiballismus) are characterized by excessive °tor activity, the symptoms of which are involuntary ovements (dyskinesias)and decreased muscle
tone h otonia).The involuntary movements may take
Bever I forms-slow, writhing movements of the extremi Oe (athetosis); jerky, random movements of the
limb
d orofacial structures (chorea); violent, largeampl tu e, proximal limb movements (ballism), and
more s~stained abnormal postures and Blower movement 'fith underlying cocontraction of agorrist and
~
'\
862
Part VI / Movement
antagonist muscles (dystonia). Various types of inv 1untary movements often occur in combination d
Borneappear to have a common underlying cause. e
best example is the similarity between chorea and b 1lism, which may simply be distal (chorea) or proxi al
(bailism) forms of the same underlying disorder.
In recent years the development of primate mod Is
of both hypo- and hyperkinetic disorders, induced y
systemic or local administration of selective neuroto Ïns, has made it possible to study Borneof the path physiologic mechanismsunderlying this diverse gym tomatology. Both extremes of the movement disord r
spectrum can now be explained asspecificdisturbanc s
within the basal ganglia-thalamocortical motor circu t.
Normal motor behaviors depend on a critical balan e
between the direct and indirect pathways fIom e
striatum to the pallidum. In the simplest of terms, ove activity in the indirect pathway relative to the dire t
pathway results in hypokinetic disorders, such s
Parkinson disease; underactivity in the indirect pa war results in choreaand ballism (Figure43-6).
Overactivity in the Indirect Pathway Is a Major
Factor in Parkinsonian Signs
Parkinson disease,fust described by JamesParkinson.
1817,is one of the most common movement disorder,
affecting up to one million people in the United State
alone. It is also one of the most studied and bestunde
stood. Parkinson's descriptionstill captures the chara
teristic posture and movements of the patients with thi
disease:
...involuntary
power,
propensity
in parts
tremulous motion, with lessenedmuscula
not in action
to bend
the
tronk
and
even
forwards,
when
supported,
and
to
pass
with
f
trom
walking to a running pace,the sensesand intellects being un
injured.
The cardinal symptoms of the diseaseinclude a pauci
of spontaneous movement, akinesia, bradykinesia, in
creased muscle tone (rigidity), and a characteristi
tremor (4-5 per second) at rest. A shuffling grot as wel
as flexed posture and impaired balance are also promi
nent. The appearanceof the typical patient with Parkin
son diseaseis instantly recognizable and unforgettable
tremor, mask-like facial expression,flexed posture, an
paucity and slownessof movement.
Parkinson diseaseis the firstexample of a brain dis
order resulting from a deficiency of a single neurotrans
mitter. In the mid 1950sArvid Carlson showed thai 80%
of the brain's dopamine is in the basal ganglia. Next
Oleh Horynekiewicz found thai the brains of patient
with P 'kipson disease are deficient in dopaminle, in
the stri tuPt, most severely in the putamen. In the
early I 60~ Parkinson disease was shown to result
largely 0 the degenerationof dopaminergic nelLrons
in the su s antia nigra pars compacta.Walter BrikIrlayer
and Ho
ekiewicz found that intravenous administration f L-dihydroxyphenylalanine (L-OOPA), the
precurs
f dopamine, provided a dramatic, although
brief, re e sal of symptoms. The subsequent demonstration y George Cotzias that gradual increases in
oral a ..tration of L-OOPAcould provide signifiicant
and con' ous benefit began the modem era of pharmacolo c therapy. Even with the development of
newer a d more effective antiparkinsonian drugs, the
benefits f drug therapy usually begin to wane after
about fi
ears; and troublesome side effects develop
in the fo
pf motor responsefluctuations and dru:?;related dys .esias.
Rese rch in Parkinson diseasewas recently revitalized by iIi am Langston'
s discovery
that
drug
addicts
exposed
t
the
meperidine
derivative
l-meth;rl-4-
phenyl-l , ,6-tetrahydropyridine (MPTP) develop a
profoun Parkinsonian state.This observation led to intenseinv stigation of the role of exogenoustoxins in the
pathoge Sf of Parkinson diseaseand to the development of n nhuman primate animal model for experimental s y. Primarily on the basis of studies in
MPTP- at d primates, a working model of the pathophysiolo ~ f Parkinson disease has been developed.
Accordin t this model, loss of dopaminergic Ïnlput
trom the u stantia nigra pars compactato the striatum
leads to .ased
activity in the indirect pathway and
decrease a tivity in the direct pathway (see Fig;ure
43-6) bec u of the different actions of dopamine on
the two a wars (via Dl and 02 receptors, respectively). B th of these changeslead to increased acti'vity
in the in
al pallidal segment, which results in increased'
bition of thalamocortical and rnidbrain
tegmental n urons and thus the hypokinetic features of
the disea .i
Expe' 'nts with MPTP-treated monkeys have
shown si ..cant changesin neuronal activity along the
indirect p war. For example, rnicroelectrode recording studi
ave shown that tonic activity is decreased
in the ex e al pallidal segment but increased in the
subthala ic ucleus and intemal pallidal segment.'[he
changes' t cic discharge in the pallidum (and the abnormal m t r signs) are reversed by systernic admi]:listration of
dopamine receptor agonist apomorphïne.
The exces i e activity in the indirect pathway at the
~ubthal ic In~cleusapp~ars t~ be .an im~ortant.fa~tor
m the pro uttion of parkinsoman slgns,smce leslonmg
of the sub halamic nucleus, which reducesthe excessive
~
}~
Chapter43 / The BasalGan.~lia
863
Parkinson disease + surgical therapies
STN lesion
~~:::::--
~
/
/'
/
I
)-
Putamen
Put~men
J
7
Spinel
cord
ease.
of theof subthalamic
nucleus (Ieh)
or internal
Figure Lesions
43-7 Sites
surgical intervention
in parkinson
f
egis-
ment of the globus pallidus (right) effectively reduce parki sonjan signs and dyskinesias by respectively normalizing or
excitatory drive on the intemal pallidal se~ent,
markedly ameliorates parkinsonian signs in MfTptreated monkeys. Selectiveinactivation of the sensoimotor portion of either the subthalamic nucleus or th internal pallidal segment is sufficient to ameliorat the
cardinal parkinsonian motor signs (akinesia, tIe or,
'and rigidity) in MPTP-treated animals (Figure 4 -7).
Surgicallesions of the posterior (sensorimotor) po .on
of the intemal pallidal segment (pallidotomy) in patients with advanced, medically intractabie case of
Parkinson disease is also highly effective in rever ing
parkinsonian signs. Pallidotomy has undergone revival in recentyears as an effective treatment of pati fitS
with advanced disease whose symptoms are po rly
controlled by medication alone and who experi nce
drug-induced motor complications (as will be fu er
discussedlater).
I
elimin~ting abnormal and excessive output from the internal
Segment. GPe = external segment of the globlJS palpallida
lidus;
Pi = internal segment of the globus pallidus; STN =
~
subth
Imic nucleus;
SNc = substantia
nigra pars compacta.
~us the hypokinetic features of Parkinson disease
appea~to result from increased(inhibitory) output from
the in,emal pallidal segmentas a result of increased (excitatoI\Y)drive from the subthalamic nucleus. j\.ccordingly ~esia and bradykinesia are no longer vie~wedas
negatiwesignsthat reflect loss of basal ganglia function,
but ra er aspositive signs that, like rigidity and tremor,
result from excessiveand abnormal activity irt intact
stru re~. This abnormal motor activity can be reverse by reducing or abolishing the pathological
outpu .
Inladdition to the increasein tonic output of the intemal pal1idal segmentin MPTP-treated monkeys, phasic ac~vity also changes.Thesechangesin the paitternof
discharge in basalganglia output are likely to be E!qually
as imftortant as the changes in the rate of dis(Darge.
Indee~, recent data suggest that tremor may be due to
"
864
Part VI / Movement
increased
synchronization
of oscillatory
dif spatial
within the basal
ganglia nuclei.
Differences in
arge
temporal patterns and discharge may accountfo differences in clirtical features among the various yperkinetic disorders.
The Level of Dopamine in the Basal Ganglia I
Decreased in Parkinson Disease
Measurements of dopamine in the striatum
d the
metabolic activity of individual basal ganglia n clei in
patients with Parkinson diseaseare consistent .th the
pathophysiologic model proposed. Uptake of do amine
in the putamen of thesepatients is greatly reduce , as assessedearlier by direct biochemical assaysand
re recently by uptake of the precursor18F-DOPAmeasred by
positron emission tomography (PET) (see Chap r 19).
Imaging of patients with Parkinson diseasehas hown
less synaptic activity (as measured by activated blood
flow in the contralateral putamen,the anterior cin late,
the supplementary motor area,and the dorsolate I prefrontal cortex) both when the patients were mo ing a
joystick and when they were resting. Administra. on of
dopamine agonists increasedthe blood flow to t e supplementary motor and anterior cingulate areas uring
ptovement tests. Surgical destruction of the palli urn in
patients with Parkinson diseasehas been show to restore activity in the supplementary motor and pr motor
areas during this same movement task. Thes neuroimaging studies lend strong additional support to the
importance of the pallidöthalamocortical portion of the
motor circuit in normal movementand the produ .onof
akinesiaand bradykinesia.
Underactivity in the Indirect Pathway Is a Maj r
Factor in Hyperkinetic Disorders
Involuntary movements in patients with basal g glia
disorders maf result either from clear-cut lesi ns of
these nuclei or from imbalancesin neurotransmitt r systems. Apart trom parkinsonism, the basal ganglia disorder for which the neuropathology is least in dubt is
hemiballism. In humans, lesions (usually due to small
strokes)restricted to the subthalamic nucleus maf result
in involuntary, of ten violent, movements df th contralaterallimbs (called "ballism" becauseof the s perfirial resemblanceof the movements to throwing). In addition to the involuntary movements of the pr ximal
limbs, involuntary movements of more distallim s maf
occur in an irregular (choreic) or more con. uous
writhing farm.
Experimentallesions of the subthalamic nuc us in
monkeys show that dyskinesias result only w en le-
sio f e made selectively in the nucleus, leaving intact
the a .acent projections from the intemal paUidal segme t 0 the thalamus. More recent studies combining
sel .e lesioning, microelectrode recording, and functio alltmaging provide new insights into the pathoph Si$ OGYof ballism and the hyperkinetic disorders in
gen r .The output of the intemal paIlidal segment is
red ce in hemiballism, as expected if the projection
fro the subthalamic nucleus is excitatory. E>:perimental esions of the subthalamic nucleus in morlkeys signifi antly reduce the tonic discharge of neurc,nsin the
inte al paIlidal segment and decreasethe phasic respo ses of these neurons to limb displacement. Thus
he .b Ilism maf result trom disinhibition of the thalamu d e to reduction in the tonic (and perhaps phasic)
ou u trom the intemal pallidal segment. Reduced inhibi 0 input from the intemal paIlidal segment might
pe .thalamocortical neurons to respond in an exagger te manner to cortical or other inputs, or it might
incr ase the tendency of these neurons to discharge
spo taneousl~ leading to involuntary movements. Altem ~ .elf,
a changed
discharge
pattem
(ral:her
than
low
rate
per
se)
maf
play
a
significant
fale.
Consis-
tent. th this idea, pallidotomy relieves hemibaIlism
and 0 er farms of dyskinesia, as weIl as parkinsonian
.!
SI
.!
Hu~tington Disease Is a Heritable
HYferkinetic Disorder
The other hyperkinetic disorder most often associated
wi d sfunction of the basal ganglia is Huntinlgton disease
.s disease affects men and women with equal
freq e cr, about 5-10 per 100,000.It is characb~rizedby
five fe tules: heritability, chorea, behavioral or psychiatri
isturbances, cognitive impairment (dementia),
and e th 15 or 20years aftel onset. In most patients the
ons t f the diseaseoccurs in the third to fifth decadeof
life. 4ny people have alreadyhad children by the time
the is~aseis diagnosed.
The Gpe for Huntington Disease Has
Bee I~entified
i
H tlt1gton diseaseis one of the first complex human
diso rdtrs to be traced to a single gene,which l",as identifie ~ mapping genetic polymorphisms (seeBox3-3).
The diseaseis a highly penetrant, autosomal dominant
diso der with a gene defect on chromosom'~4. This
gen encodesa large protein, huntingtin, the fLmction of
whi ras yet to be determined (Chapter3). Thleprotein
n
atly is located in the cytoplasm. As we have geen
by
indiinhi-
the
inhibi-
rE!duced,
and
early
the
hemibal-
striatal
pallidal
resembie
in
ex-
be
disease:
maf
of
replacement
closely
neuron.~.
internal
segment.
the
of
Huntington
in
in
could
resultiIlgfuncgeen
the
these
pathophysiology
dopamine
Huntington
in
dyskinesias
The
of
which
in
in
pallidal
loss
advanced
the
in
those
that,
nucleuE:
The
neurons
is
the
to
in
of
mechanism
movements
movements
rise
aresuit,
give
As
lost.
pallidum
these
internal
with
the
firing
inhibition
induced
chorea
of
that
to
pathology
characterized
the
is
brain,
common
A
the
disease
in
choreiform
that
dyskinetic
the
external
symptoms
subthalamic
neurons.
of
the
nucleus
the
of
akinesia
to
disease.
effect
side
Parkinson
a
dyskinesias,
increase
thus
reduce
project
associated
and
resembie
choreiform
disease,
!:he
the
rigidity
and
'1ar
de-
overac-
ex-
to
neurons
and
The
by
segment.
nucleus
neurons
leading
striatal
the
segment,
of
pallidal
subthalamic
pallidal
pallidal
inhibition
external
external
the
external
the
of
of
the
to
in
ons
a
denot
pa-
in
ther-
of
expression
upreg-
course
gene
receptor
the
or
does
inter-
pathway
thE~
to
L-DOPA
input
direct
dopaminergic
segment
Uris
of
in
would
segment
nucleus
inactivation
pallidal
lesions.
direct
the
from
in
individuals
altered
result
early
normal
and
probably
disease
in
of
inhibitory
of
excessive
internal
surgical
after
pallidal
subthalamic
the
neurons
by
on
by
geen
internal
the
the
in
that
drive
administration
Since
increased
striatal
compounded
of
Parkinson
supersensitivity,
symptoms
ith
~yskinesias
idum.
resulting
tion
be
excitatory
nucleus
to
from
activity
output
similar
e
in
n
su~thalamic
th
pal
th
~
apr,
tients
produ
nal
and
stimul
would
crease~
the
manne
lower
crease
tive
r
inhibition
inhibition
oject
p
dopaminergic
S
~
I1harmacologically
for
are
g-induced
t
would
that
are
e
of
ss
1
the
neurons
and
both
striatum.
neurons
Huntington
of
the
preferentially
discharge
in
are
neurons
subthalamic
inactivation
I
of
excessive
of
p,thway
Striatal
disease
underlie
in
loss
Ü10Ugh
to
earliest
pr~ad
wide
see
is
appe*s
Hun$gton
hemil1allism.
rect
bitionl
causïrtg
tion
tional
expl'
stages
lism.
disea
neuro
This
segm
chore~
therap~
these
cessivd
reduce~
that
cessiv
part
865
Intersignificant
drug.
a
the
be
of
to
appears
administration
L-DOPA
of
prolonged
dosing
by;
Uiation
caused
parent.
In researchaimed at determining why the CA repeatsin the fust exon causeddisease,the first exon m
the mutant human huntingtin protein was express d in
mice where it was found to be sufficient to causea rogressive neurological phenotype. In these mice, the
exon formed multiple intranuclear inclusions mad up
of the huntingtin protein. A similar accumulatio of
huntingtin protein has now been found in the nucl i of
brain cells trom patients with Huntington disease.
A Drosophilamodel of Huntington diseasehas
n
developed by expressingan amino terminal fragme t of
the human huntingtin protein containing 2, 75,and 120
repeating glutamine residues. By expressing this agment in photoreceptor neurons of the compound ey of
the fly the polyglutamine-expanded huntingtin ind ed
neuronal degeneration much as it does in human eurong. The age on the onset and severity of the ne nal
degenerationagain correlated with the length of th repeat, and the nuclear localization of huntingtin a ain
presagedneuronal degeneration.
Finally, a cellular model of Huntington disease as
been created by transfecting the mutant Huntingt n's
gene into cultured striatal neurons. Here the gene induced neurodegeneration by an apoptotic mechani m,
consistentwith the idea that the Huntington protein cts
in the nucleus to induce apoptosis..Blocking nuclear 10calization of the mutant huntingtin suppressesits abi ity
to form intranuclear inclusions and to induce apopt is.
However, this apoptotic death did not correlate with e
formation of intranuclear inclusions. Full length h tingtin forms inclusions very rarely, raising the possib' ity
that intranuclear inclusions may not play a causalrol in
mutant huntingtin's induced death.1n fact, expos
of
transfected striatal neurons to conditions that s ppressed the formation of inclusions resulted in an increasein huntingin-induced death. These findings s ggeststhat mutant huntingtin may act within the nucl us
to induce neurodegeneration, but that the intranucl ar
inclusions themselves may reflect a defensemechan m
designed to protect against the death induced by h ntingtin rather than reflecting a mechanismof cell dea .
mittent
in Chapter 3, the first exon of the genecontained re eats
of the trinucleotide sequenceCAG, which encode the
amino acid glutamine. Whereas normal subjects ave
less than 40 CAG repeatsin the fust exon, patients ith
Huntington diseasehave more than 40 repeats. ose
that have between 70and 100repeatsdevelop Hun' gton disease as juveniles. Once expanded beyon 40
copies, the
repeats become unstable and
tend to increase from generation to generation, a henomenon which accountsfor genetic "anticipation, the
earlier onset of the diseasein the offspring than' the
$
Chapter43 / '!he BasalGanglia
factor' the emergence
of drug-induceddyskinesias.~
Glutamate-Induced Neuronal Cell Death
Contributes to Huntington Disease
Gluta~ at' is the principal excitatory transmitter in the
central n~rvous system. It excites virtually all c:entral
neuro and is present in nerve terminals at high concentra 'on (10-3 M). In normal synaptic transmission
the extracellular glutamate riBes transiently, and this
I
~
866
Part VI / Movement
rise is restricted to the synaptic cleft. In contrast, ustained and diffuse increasesin extracellular glut ate
kill neurons. This mechanism of cell death occurs primarily by the persistent action of glutamate on th Nmethyl-D-aspartate (NMDA) type of glutamate re eptors and the resulting excessiveinflux of Ca2+(Cha ter
12). ExcessCa2+ has several damaging conseque ces
that lead to cytotoxicity and death. First, it can acti ate
calcium-dependent proteases (calpains). Second, 2+
activates phospholipase A2, which liberates arachid nic
acid, leading to the production of eicosanoids, s bstancesthat produce inflammation and tree radicals at
causetissue damage.
Toxic changesproduced by glutamate, called gl tamateexcitotoxicity,are thoUght to causecell damage d
death after acutebrain injury such as stroke or exces ve
convulsions. In addition, excitotoxicity may contrib te
to chronic degenerative diseasesof the brain, such as
Huntington disease.It has been shown that injectio of
NMDA agonists into the rat striatum reproduces e
pattern of neuronal cellioss characteristic of Hun. gton disease.Thus, it is possible that the altered gene on
chromosome 4 produces an abnormality that leads to
excessive activation of NMDA receptors or release of
glutamate.
The Basal Ganglia Have a Role in Cognition,
Mood, and Nonmotor Behavior
~
Some circuits in the basal ganglia are involved in n motor aspectsof behavior. Thesecircuits originate in e
prefrontal and limbic regions of the cortex and enga e
specific areasof the striatum, pallidum, and substan °a
nigra.
I
The dorsolateralprefrontalcircuit originates in Bro mann's areas 9 and 10 and projects to the head of e
caudate nucleus, which then projects directly and in irectly to the dorsomedial portion of the internal palli 1
segmentand the rostral substantia nigra pars reticula .
Projections from these regions terminate in 1he ventr 1
~terior and medial dorsal thalamic nuclei, which
turn project back upon the dorsolateral prefrontal are.
The dorsolateral prefrontal circuit has been implicat d
broadly in so-called "executive functions" (Chapter1 ).
Theseinclude cognitive tasks such as organizing beha ioral responsesand using verbal skills in problem sol ingoDamage to the dorsolateral prefrontal cortex or su cortical portions of the circuit is associated with a
variety of behavioral abnormalities related to theseco nitive functions.
The lateral orbitofrontal circuit arises in the later 1
prefrontal cortex and projects to the ventromedial ca -
date ucleus. The pathway trom the caudate nucleus
follow that of the dorsolateral circuit (throUgh the intemal allidal segmentand substantia nigra pars reticuIata d thence to the thalamus) and returns to the orbitofr tal cortex. The lateral orbitofrontal cortex
appea s to play a major role in mediating empathetic
and sOfially appropriate responses.Damage to this area
is assopated with irritability, emotionallability, failure
to respbnd to social cues,and lack of empathy. A tleuroPSYchif triC disorder thought to be associatedwith disturban es in the lateral orbitofrontal cortex and circuit is
obsessi e-compulsive disorder (Chapter 61).
Thf anterior cingulate circuit arises in the aruerior
cingul~te gyrus and projects to theventral striatum. The
ventrail striatum also receives "limbic" input from the
hippocbpus, amygdala, and entorhinal cortice:;. The
proje~ns of the ventral striatum are directed to the
ventr~I_landrostromedial pallidum and the rostrodorsal
subst~ti~ nigra pars reticulata. From therethe pathway
continu~s to neurons in the paramedian portion of the
medial dorsal nucleus of the thalamus, which irl turn
project ack upon the anterior cingulate cortex. Tlle anterior c' gulate circuit appearsto play an importarrt role
in moti ated behavior, and it maf convey reinforcing
stimuli 0 diffuse areas of the basal ganglia and cortex
via inp tsthrough the ventral tegmental areasand the
substan 'a,nigra pars compacta.These inputs may play
a major role in procedurallearning (see Chapter 62).
Damag tö the anterior cingulate region bilaterally can
by
cause ~ etic mutism, a condition characterized
profoun
ilnpairment
of movement
initiation.
.
In n~ral, the disorders associated with dysfunction of ~e prefrontal cortex and corticobasal gangliathalamo~orticalcircuits involve action rather than of perception br sensation.These disturbances are associated
both wi either intensified action (impulsivity) anclflattened a 'on (apathy). Obsessive-compulsivebehavior
can be ie~ed as a form of hyperactivity. The disturbances rnood associatedwith circuit dysfunctio:tl are
believed to span the extremes of mania and depression.
Both do amine and serotonin,two biogenic arnine~,that
modulat neuronal activity within the circuits, are important depression(Chapter61).
The e observations suggest that the neural mechanisms d~rlying complex behavioral disorders might
be analo~ous to the dysfunctions of the motor circuits
describe~ in this chapter. Thus, schizophrenia might be
viewed as a "Parkinson disease of thought." By this
~
analogy,
!
ordered
chizOPhreniC
odulation
symptoms
of
prefrontal
would
circuits.
arise
Other
from
discogni-
tive and motional symptoms maf sirnilarly be equivalents of otor disturbances such as tremor, dyskinesia,
and rigi ity.
Chapter43 / The BasalGanglia
An Overall View
8)
I
'.
867
selec~edReadings
In 1949Linus Pauling revolutionized medical
ing
by coining the term "molecular disease." He an rus
collaborators observed the altered electrophoretic mobility of hemoglobin 5 and reasonedthat sickle cell anemia, a diseaseknown to be genetic, could be expl ined
by a mutation of a gene for aspecific protein. A d ade
later Vernon Ingram showed that tros alteratio in
chargeoccurs in the amino acid sequenceof hemog obin
5, where a glutamic acid residue is replaced by a v line.
This change from a single negatively charged resid e in
normal hemoglobin to a neutral one explains the al red
molecular properties of hemoglobin 5, and thesein turn
account for the intermolecular differences and d sordered cell stacking observed in sickled red cells. Th s, a
single molecular changeis fundamental to underst ding the patient's pathology, symptoms, and progno is.
While the explanation foTother diseasesmay n t be
as simple, it is a fundamental principle of modem edicine that every disorder has a molecular basis.Rese rch
in Parkinson diseaseand myasthenia gravis fiTst ade
the medical community realize that particular co ponents of chemical synapsescan be specific target foT
disease.In myasthenia gravis the molecular target i the
acetylcholine receptor. In the disorders of the basal anglia same components of the synthesis, packagin or
tumover of dopamine and serotonin are altered. The
causes of the pathological alterations of these oci,
whether genetic, infectious, toxic, or degenerative, are
not yet known. Although we have identified the m ant
gene for Huntington disease,as yet we have no dea
about the function of the protein that the wild-type ene
encodes.It is clear that rational treatment for diseas s of
transmitter metabolism requires a good understan ing
of synaptic transmission in the affected pathways.
Mahlon R. DeL~ng
Albin~RL. 1995. The pathophysiology of chorea/ballism and
pa kill\sonism. Parkinsonism and Related Disorders
1: 11.
Broo DJ. 1995.The fale of the basal ganglia in motor contro~: contributions trom PET. J Neurol Sci 128:1-13.
Ches~let MF, Delfs JM. 1996.Basal ganglia and movement
dis rqers: an update. Trends Neurosci 19:417-42~~.
Gray .el AM. 1995.Building action repertoires: memory and
lea .g functions of the basal ganglia. Curr apin Neurobio 5:733-741.
Wi
artn T, DeLong MR. 1996.Functional and pathological
~o~els of the basal ganglia. Curr apin Neurobiol
6.7.$1-758.
~
Refer~nces
Alb
'
RIL, Young AB, Penner JB. 1989. The functional
omy of basal ganglia disorders. Trends Neurosci
12: 66L375.
AleX*
EïI GE, Crutcher
MD, DeLong
MR.
1990. Basal gangli
thalamocortical
circuits:
parallel
substrates
for
motor,
ocu omotor, 'prefrontal' and 'limbic' functions. Prog
Br
Res 85:119-146.
Baron MS, Vitek JL, Bakay RAE, Green J, Kaneoke Y,
Ha~himoto T, Turner RS, Woodard JL, Cole SA,
Mc1!Jonald WM, DeLong MR. 1996. Treatment of advan~ed Parkinson' s disease by GPi pallidotomy~ 1 year
pildt-study results. Ann Neurol40:355--366.
Bergm n H, Wichmann T, DeLong MR. 1990.Reversal of expe. ental parkinsonism by lesions of the subthalamic
nu eus. Science249:1436-1438.
Gash M, Zhang Z, Ovadia A, Cass WA, Yi A, ~irnmerman
L, usSel1D, Martin D, Lapchak PA, Collins F, Hoffer BJ,
Ger ardt GA. 1996. Functional recovery in parkinsonian
mo eys treated with GDNF. Nature 380:252-255,
Gerfen CR. 1995. Dopamine receptor function in the basal
gan lia. Clin NeuropharmacoI18:S162-S177.
Hikos aiO, Matsumara M, Kojima J, Gardiner TW. 1993.
Rol~ of basal ganglia in initiation and suppression of saccad* ere movements. In: N Mano, I Hamada, M DeLong
(ed .). ({ole ofthe Cerebellumand BasalGanglia in Voluntary
Mement. Amsterdam: Elsevier.
Hoove J~, Strick PL. 1993.Multiple output channels in the
ba I ganglia. Science259:819-821.
Kordo el! JH, et al. 1995. Neuropathological evidence of
gra survival and striatal reinnervation after the transpl tat!ion of fetal mesencephalic tissue in a patient with
Par 'nson's disease.N Engl JMed 332:1118-1124.
Marsd m, Obeso JA. 1994.The functions of the basal ganglia anP the paradox of sterotaxic surgery in Parkinson' s
di ase.Brain 117:877-897.
Nieuw nhuys R, Voogd J, van Huijzen C. 1981. TheHuman
Cenral Nervous System:'A Synopsisand Atlas. 2nd ed.
Ber 'n: Springer.