Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Functional magnetic resonance imaging wikipedia , lookup
Intracranial pressure wikipedia , lookup
Neuroscience and intelligence wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Neurogenomics wikipedia , lookup
Human multitasking wikipedia , lookup
Limbic system wikipedia , lookup
Human brain wikipedia , lookup
Neuroinformatics wikipedia , lookup
Neurobiological effects of physical exercise wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Embodied cognitive science wikipedia , lookup
Blood–brain barrier wikipedia , lookup
Environmental enrichment wikipedia , lookup
Neuroanatomy wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Selfish brain theory wikipedia , lookup
Neurolinguistics wikipedia , lookup
Neuroeconomics wikipedia , lookup
Brain morphometry wikipedia , lookup
Neurotechnology wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Metastability in the brain wikipedia , lookup
Haemodynamic response wikipedia , lookup
Sports-related traumatic brain injury wikipedia , lookup
Brain Rules wikipedia , lookup
Neuroplasticity wikipedia , lookup
History of neuroimaging wikipedia , lookup
Neurophilosophy wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Alzheimer's disease wikipedia , lookup
Neuropsychology wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
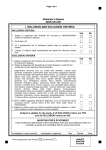
By Majid Fotuhi, MD, PhD ear of developing Alzheimer’s disease (AD), far more than the disease itself, has become an epidemic and a major source of concern for Baby Boomers in the US. Elderly beyond the age of 80 are the fastest growing segment of the population, and many of them who experience cognitive decline receive the diagnosis of AD. Their children, mostly Baby Boomers, now wonder if they are next. Common questions that they have may include: 1. My mother in her 80s has been just diagnosed with AD. When do you think I will get it? 2. What can I do to reduce my risk of developing AD? Is it possible? 3. I can never remember anyone’s name and sometimes feel embarrassed for not remembering even the names of people I have known for a long time. I have AD, right? 4. Ginkgo biloba, vitamin E, curcumin, and fish oil all seem to be good for warding off AD. Which one do you recommend? The concern for developing this dreadful disease is not limited to the lay population. Recently, a physician with a busy practice called me to request an earlier appointment. During our phone conversation, I learned that he is 50 years old and has been forgetting names and appointments. His family believes that he has developed AD. Meanwhile, he works full-time, publishes articles, and engages in many social and professional meetings and gatherings. I could hear from his trembling voice that he was truly concerned that he would soon develop AD. Among the more than 78 million Baby Boomers in the US, far fewer than one percent have been diagnosed with AD. Thus, more than 99 percent of this population does not have AD and F 34 logically should not worry about it. However, they do worry. Their concerns are real and must be addressed. A successful strategy to provide reassurance and to help Baby Boomers take steps to improve their brain health is easy. It requires educating them regarding causes of short-term memory problems in their current day-to-day life and making them appreciate their risk factors for developing dementia in their last decades of life. Common Cause of Poor Short-Term Memory Forgetting names and occasional appointments more likely occurs in Baby Boomers with multiple medical issues (e.g., obesity, heart failure, or chronic uncontrolled pain), depression, medication side effects, stressful lifestyle, long work hours, constant fatigue, and most commonly, lack of adequate sleep.1 Some of the common causes of poor sleep quality include insomnia, restless legs syndrome, frequent urination, obstructive sleep apnea (OSA), and anxiety. Many patients with OSA do not realize that their grogginess, lack of energy, and difficulty with concentration during the day stem from frequent hypoxia and awakenings that they experience during the night. Heart patients who have low cardiac ejection fraction also suffer from low levels of oxygen to their brains, and as a result, their cognitive abilities decline. Patients with untreated depression have difficulty paying attention and often report being extremely forgetful. Treating and optimizing medical issues produces a noticeable improvement in memory functions for our patients and improves their confidence that they do not have early signs of AD. Information overload may be yet another factor that hinders memory. Thanks to a surfeit of technological advances, from Practical Neurology March/April 2009 pagers, BlackBerries and text messaging to e-mails, websites, and podcasts, Baby Boomers are bombarded with loads of information in a constant stream. Somehow, their expectation is that they should remember details from these many different forms of communication and be able to keep up with them. Never in the history of our civilization have people been exposed to this degree of information on a daily basis. Our middle-aged busy patients need to adjust expectations in this regard. I sometimes suggest they limit checking e-mails (or playing with their BlackBerries or iPods) to once every three hours to reduce their flow of incoming data. They also would benefit from a five- to ten-minute relaxation break (e.g., meditation) during their hectic days. When Baby Boomer patients relate stories of forgetting names, I remind them that learning and remembering people’s names can be considered a skill, similar to dancing or learning a new language. Paying attention, persistence in memorizing a name at the first encounter, and repetition of a new name throughout the conversation are simple means of committing a name to memory. onset AD and late-onset AD. With early-onset presenile Alzheimer dementia (quite rare, affecting less than one percent of the Baby Boomer population), patients lose their cognitive abilities at a rapid rate.2 They cannot function at their jobs and, within one or two years, have difficulty maintaining their finances or even some of their routine activities of daily living. This form of dementia has a strong genetic component, and indeed, patients who have family members with early-onset AD are at significantly increased risk. In contrast, late-onset dementia (beyond age 65) has a lower genetic component.3 A person in his 70s has approximately a two percent risk of developing dementia. His risk may be doubled (to four percent) if he has parents who experienced dementia in their 80s. In other words, a patient has about a 96 percent chance of remaining cognitively healthy—if he has no other risk factors. Risk Factors for Cognitive Decline with Aging Heredity and AD Addressing medical, psychological, and lifestyle issues are the first steps toward helping Baby Boomers identify ways in which they can improve attention and memory. An equally important step is educating them regarding the difference between early- March/April 2009 A number of risk factors associated with lifestyle choices and cerebrovascular issues increase up to 16-fold the risk of developing cognitive impairment with aging.4,5 Thus, a Baby Boomer with obesity, diabetes, hypertension, smoking, sedentary lifestyle, high cholesterol, strokes, and chronic stress is far more likely to devel- Practical Neurology 35 AD Prevention op dementia than her neighbor who is otherwise well but has parents with AD. Chronic untreated hypertension can literally lead to smaller brains.6,7 Similarly, chronic OSA can cause 18 percent cortical atrophy in frontal lobes and even in the hippocampus, the brain region most essential for short-term memory.8,9 Uncontrolled diabetes is yet another condition associated with thinning of the cortex with age.10 These factors are extremely important, and Baby Boomers worried about AD can start their efforts toward improving brain health through addressing their risk factors.5,11 To help patients identify and recognize their risk and protective factors, I have developed a screening questionnaire (Table 1). Their particular score on this test provides an opportunity for me to talk to them about setting priorities on ways in which they can lower their chance of developing dementia in their 80s. Simple lifestyle changes during midlife have the potential to serve as “primary prevention” strategies for late-life dementia (Fig. 1). New Way of Thinking About Aging & Dementia In 1997, Snowdon, et al.’s pivotal study changed the way neuroscientists view the brain with aging and dementia.12 The Nun Study showed that many elderly women had large loads of AD tangles but no hint of cognitive impairment. The inconsistency between severity of Alzheimer neuropathology and degrees of dementia could be explained by the coexisting number and severity of strokes in the brain. The combination of Alzheimer pathology and vascular pathology—not either one of them alone— turned out to be the deciding factor for development of cognitive impairment in the majority of their elderly participants (Fig. 2). Findings from other research groups confirmed the results of the Nun study. For example, it was shown that presence of subcortical lacunar strokes can increase the risk of dementia five- to six-fold.13 Extent of plaques and tangles may be similar in elderly with dementia and those with no evidence of dementia, again supporting the notion that Alzheimer pathology by itself may not be sufficient for triggering symptoms of cognitive deterioration among elderly.14,15 The net conclusion of the recent literature in this field suggests that a substantial number of elderly can harbor high amounts of plaques and tangles in their brains and have no signs of dementia—if their brains are otherwise healthy. In fact, it is becoming increasingly difficult to justify diagnosing those 80 and older with AD, as plaques and tangles seem to be only part of a combination of culprits in late-life dementia.16 Neuroprotective Factors Exercise. Brain plasticity continues throughout life and is not limited to childhood. In a study by Kramer et al., retired elderly were invited to participate in a “walking” study.17,18 One group was randomly assigned to walk three times per week for six months. Another group performed stretching exercises, and a 36 third group continued with their routine lifestyle, which did not include significant physical activity. At the end of six months, MRIs of the brain were obtained and were compared to MRIs obtained at baseline. A three percent increase in cortical areas in frontal lobes was noted in the group that walked three times per week. Brain volume growth was accompanied by a 15 percent improvement in performance in cognitive tests. In short, a simple walking regimen resulted in actual expansion of cortical areas, comparable to being three years younger, after only six months of regular exercise. More recent evidence suggests that even hippocampus shows plasticity with physical exercise.17,18 One potential mediator for this increase in brain size appears to be brain-derived neurotrophic factor (BDNF).19,20 Blocking BDNF in comparable animal studies reduced the amount of brain plasticity with exercise. Brain stimulation. Intensive brain stimulation can expand the size of the cortex as well. May et al. in Germany obtained brain MRIs in a group of medical students before and after three months of intense studying in preparation for their national board exams.21 MRIs revealed a significant increase in brain volume in parietal lobes and hippocampus. Parietal lobe expansion remained significant but plateaued three months after students had completed their exams, when they were no longer working hard in memorizing long lists of medical terms. In contrast, hippocampal expansion continued during these three resting months. The surprising growth in hippocampus may be in part due to its unique ability for neurogenesis throughout adult life. These results clearly indicate that cognitive stimulation can modify the volume of cortex and hippocampus at both microscopic and macroscopic levels. Diet. Along with studies highlighting the importance of exercise and brain stimulation, numerous others have highlighted the critical role of diet in brain health.22,23 Inflammation is a key part of neurodegeneration with aging. Levels of inflammatory markers (such as C-reactive protein) tend to be higher in individuals with dementia compared to those without cognitive impairment.24 Nonsteroidal anti-inflammatory drugs (NSAIDs), especially ibuprofen, have been associated with some reduced risk of developing AD.25 Though these findings remain controversial, they support the important role of inflammation in brain aging. Findings from The Cache County Study revealed a significant reduction in risk of AD in individuals who consume high quantities of fruits and vegetables or those who take vitamin E or vitamin C supplements.26,27 We recently reported that the combination of NSAIDs and antioxidant vitamins (E and C) can lead to “better” cognitive performance in elderly.28 The elderly at high risk for developing AD gained a synergistic benefit from taking antioxidant vitamins and anti-inflammatory agents together. The Cache county results were based on data from approximately 5,000 participants who were monitored for eight years. Practical Neurology March/April 2009 Table 1. Baby Boomer Memory Quiz. A full-size PDF of this survey is avilable for download at practicalneurology.net. Look for this article under “Current Issue,” and see the last page. Our recent systematic literature review supports a strong neuroprotective role for omega-3 fatty acids in preventing cognitive impairment with aging.29 Those who consume two or three fish meals every week and/or take fish oil supplements consistently perform better than those who do not. These observations require further confirmation by longterm clinical trials; numerous studies have been in agreement that reducing inflammation in the brain through diet (rich in fruits, vegetables, and omega-3 fatty acids) may be a key step toward better brain health.30 Ten Steps Toward a Healthier Brain Late-life brain health depends to a large degree on lifestyle choices during midlife.1,31 Recognizing and addressing risk factors and neuroprotective strategies that impact brain volume have now gained more importance and provide support for recommending lifestyle changes that can potentially provide primary prevention for late-life dementia (Fig. 1). These recommendations can only be based on observational studies in large cohorts of participants monitored for several years or decades. Clinical trials to confirm how mid-life lifestyle changes may reduce risk of late-life dementia are unlikely to be conducted, due to challenges in monitoring large numbers of participants over decades and having adequate control (placebo) groups. In The Memory Cure: How to Protect Your Brain against Memory Loss and Alzheimer, I highlight (based on my review of more than 2,000 papers in the field) 10 steps I recommend to my Baby Boomer “worried well” patients.1 1. Take control of your blood pressure. High blood pressure is the silent killer for the brain. Individuals who have higher blood pressure throughout midlife are two or three times more likely to develop cognitive impairment in their 80s.5 Some studies suggest that chronic hypertension actually causes brain atrophy.6,7 Controlling high blood pressure can reduce the risk of developing dementia significantly.32 A recent study showed that people taking antihypertensive medications had a lower load of amyloid plaques March/April 2009 than those who did not have hypertension, suggesting that these medications may alter the neuropathology in AD.33 One out of four Americans has high blood pressure; more than three-quarters of these patients do not treat their hypertension successfully. Given the increased risk of coronary artery disease, maintaining a healthy blood pressure should be a top priority for all of our patients, regardless of whether they are concerned about their heart health or their brain longevity. Simple steps to lower blood pressure without medications include reducing the amount of salt in the diet, walking daily, and reducing stress as much as possible. However, for those with serious hypertension (systolic blood pres- Practical Neurology 37 AD Prevention Figure 1. Several observational studies have provided support for the concept that lifestyle changes during midlife can serve as strategies for the primary prevention of dementia. Fig.1&2: Fotuhi M. The Memory Cure: How to Protect your Brain against Memory Loss and Alzheimer's Disease. New York: McGraw Hill, 2003, with permission. sure >160), medications are often necessary. Our middle-aged patients interested in keeping their brains young must take their hypertension (mild or severe) seriously. 2. Lower your cholesterol. Hypercholesterolemia accelerates risk of coronary artery disease and cerebrovascular disease.34,35 Cholesterol-lowering medications, perhaps in ways beyond lowering cholesterol, have been shown to reduce the risk of strokes. As strokes, small or large, are strong players in determining brain health, lowering cholesterol should be a priority for healthier brain.36 For those with only mild hypercholesterolemia, a change in diet may be sufficient. A special attempt should be made to increase HDL, as low HDL may be as detrimental as high LDL. Statins have been associated, with mixed and unconvincing results, with lower risk of AD. Clearly, if a patient has high cholesterol, he or she needs treatment. The current literature does not support prescribing statins to otherwise healthy individuals with normal cholesterol for the sole purpose of warding off AD.35 3. Homocysteine, vitamin B12, and folate. Absorption of vitamin B12 from gastrointestinal mucosa diminishes with age. Incidence of low B12 and high homocysteine increases with each decade of life.37,38 Those with significant B12 deficiency have significant cortical atrophy and cognitive impairment.39 B12 supplements improve concentration and attention; patients often report “increased energy” when their B12 levels are replenished. Folate supplementation diminishes risk of dementia.40,41 Surprisingly, several studies have shown that B12 treatment does not necessarily produce the same effect.42 Low levels of B12 may be associated with other biochemical abnormalities (e.g., low folate or B6) that contribute to developing dementia. While researchers continue to explore the details of the link between low B12 and risk of dementia, it is prudent for our patients to have normal B12 levels. I often recommend maintaining B12 levels within 500–1000 pg/lit. 4. Eat a diet rich in antioxidants and fish. In addition to 38 high levels of vitamins E and C, fruits and vegetables contain essential vitamins and Suppminerals.43 lementing rat diet with blueberries has been shown to increase cognitive function and “exploring behavior.” Aged animals that receive additional blueberries perform similar to young counterparts.44 Fish consumption has also been shown to improve cognitive performance and, in some studies, shows benefit in reducing the risk of dementia.29 Thus, we can recommend to all my patients (without any hesitation) eating a heart-healthy diet that contains four to five pieces of fruits and vegetables per day and two to three servings of fish every week. Due to financial and practical issues, no clinical trial can ever be performed (in a double-blinded placebo control fashion) to establish the association between diet during midlife and risk of latelife dementia. However, available data from observational studies remain fairly convincing, especially for the Mediterranean diet. For Baby Boomers interested in taking supplements instead of eating fruits, vegetables, or fish, I recommend vitamin E, vitamin C, curcumin, and long-chain omega-3 fatty acids such as DHA and EPA. Curcumin, a natural NSAID with no significant side effects, can reduce amyloid accumulation and aggregation.45,46 Plans are now underway to start a clinical trial for this combination (MemoGuard) to establish its exact effectiveness in enhancing cognitive function and reducing risk of dementia in patients with mild cognitive impairment. Gingko biloba has been studied extensively during the past 10 years; double-blinded clinical trials have failed to show any convincing results for recommending it for either prevention or treatment of dementia.47,48 In general, some supplements may have a potential role for improving brain health. However, they are not “magic bullets” for preventing dementia. They may help cognitive function, but only in the setting of other heart-healthy lifestyle choices. Drinking one glass of wine with dinner might have modest neuroprotective effects, as well.49 However, the strength for such recommendation is minimal compared to other factors, such as controlling blood pressure. Excessive alcohol consumption itself can cause brain atrophy. 5. Protect your brain. Head trauma has been associated with cognitive impairment late in life.50,51 Shrinkage of hippocampus has been documented in veterans with severe head trauma and Figure 2. Multiple small subcortical strokes or large cortical strokes contribute to a higher risk of “vascular” dementia (upper pictures). Plaques and tangles in the hippocampus and cortex increase the risk of Alzheimer-type dementia (lower picture). Either of these factors, strokes or AD, by themselves may not trigger significant cognitive impairment in elderly (silent dementia). However, their combination causes manifestation of dementia symptoms more readily—and at an earlier age. Practical Neurology March/April 2009 coma in the battlefield.52 Traumatic brain injury (e.g., in boxers) increases the amyloid load in the brain, thus suggesting a potential mechanism for late-life dementia.53,54 Trauma to the brain may also tear white matter bundles between the cortical and subcortical areas.55 It may even affect the hemodynamics of blood flow in the brain. Most patients are aware of the negative impact of head trauma, but a reiteration about the importance of wearing seatbelts and helmets is prudent. 6. Sharpen your senses. Lack of sleep, medication side effects, and difficulties with vision or hearing can impair the acquisition of new information. If information is not firmly registered in the brain, it cannot be retrieved later. I often highlight the importance of adequate sleep and maintaining “fresh senses,” for better memory acquisition both in the short term and in the long term. OSA, quite common in the US, has a direct link to short-term memory loss as well as dementia.56,57 Patients often feel tired and groggy in the morning and complain of not being able to pay attention. Given the critical importance of sleep apnea in causing memory loss, I always carefully obtain history regarding sleep issues, snoring, and “dozing off” in meetings or at traffic lights. Interestingly, most patients do not realize that their daytime hypersomnolence may indeed be related to their snoring at night and to their obesity. Educating patients about this connection often helps awaken them to the importance of hypoxia associated with their sleeping pattern. OSA is also associated with hypercoagulability, hypertension, and increased risk of myocardial infarction.58 In addition to improving memory and lowering risk of brain atrophy with age, treating sleep apnea can be lifesaving. Some Baby Boomers may sleep only four hours per night, lead busy social and personal lives, and manage multiple large projects simultaneously. They may receive phone calls, e-mails, and pages 12 to 14 hours per day. If they are concerned about forgetting names and appointments, they need to consider reducing working hours and pay more attention to their sleep. 7. Exercise. Physical activity is the best medicine for preventing memory loss, both in the short- and long-term.17,18 Improved blood flow to the brain with exercise is associated with generation of new blood vessels. The brain is a vascular organ that receives 20 percent of the blood from the heart (considering that it accounts for two percent of body weight, it receives 10 times its share of cardiac output). Better vascular health for the brain is important for thinking clearly, making better decisions, and remembering more. Exercise also improves HDL-to-LDL ratio, reduces stress, lowers risk of heart attacks, and enhances mood. Baby Boomers often complain of “lack of time” for regular exercise. If they indeed are serious about improving their memory and cognitive health, they need to be serious about engaging in regular physical activity. They can start with as little as 15 minutes of walking per day and gradually increase it to 45 minutes per day. 8. Jog your brain. Increased brain stimulation is linked to March/April 2009 lower risk of AD.59 “Use it or lose it” applies to the brain as much as to muscles. Neurons can grow new synapses with brain stimulation. I tell patients about the MRI study in which brain stimulation in medical students led to substantial increase in brain volume; it is a vivid example of active brain plasticity in adulthood. Almost all Baby Boomers have heard of benefits associated with doing crossword puzzles, trying new hobbies such as dancing, or engaging in a game of chess.31 I encourage them to take on hobbies that they enjoy. This approach ensures that they continue with their hobby and adhere to their plans for regular brain workout. Baby Boomers with challenging careers (e.g., engineers, doctors, executives, architects) acquire plenty of brain exercise at work and should not worry about which new brain-stimulating software to play on their iPod or Nintendo DS. These individuals may benefit more from Tai chi, yoga, or other programs that combine thinking and concentration with relaxation. 9. Socialize. Several studies reveal the importance of socialization for better brain health and lower stroke risk.60–62 Middle-aged individuals with isolated lifestyles are more prone to cognitive decline with aging and dementia.63 Reduced risk of dementia in individuals who enjoy participating in social activities, volunteering, or spending time with friends has been well documented. Though understanding the neurobiology of better brain health due to mingling with others is in its infancy, it is reasonable (based on observational studies) to recommend participation in social activities. Joining dance groups may be an excellent strategy to exercise, engage the brain, and socialize—all at the same time. 10. Beware of depression. Patients who tend to be lonely and avoid joining social groups may have signs and symptoms of depression. Such individuals need further evaluation. Depression may be associated with a smaller hippocampus; some studies suggest that this presumed atrophy can be reversed with antidepressants.64–66 Animal studies support the notion that stress and anxiety may lead to neuronal injury in hippocampus. More studies are now underway to study the link between depression and dementia, but clearly patients who have major depression need to be treated promptly. Excessive worrying for memory loss and AD at a young age may represent signs of untreated major depression. Stress and anxiety increase stroke risk.67 I remind patients of the importance of relaxation—and that laughter is the best medicine. I encourage them to smile more often. Many Baby Boomers are consumed with so many personal and professional commitments they forget to laugh. They need to be reminded of the importance of taking it easy and enjoying life as much as possible. Improving Brain Fitness For Baby Boomers, memory loss should not be considered synonymous with early signs of AD. Late-life dementia is a result of multiple “hits” to the brain, from a variety of risk factors such as hypertension, obesity, chronic stress, head trauma, OSA, and poor Practical Neurology 39 AD Prevention diet. Baby Boomers must realize that they have many opportunities for improving their brain fitness and actually increase the size of their cortex and hippocampus. Instead of worrying about AD, they need to establish a strategy to improve blood pressure, sleep, and medical issues. We must remind them that exercise, challenging brain activities, heart-healthy diet, and laughing more often 1. Fotuhi M. The Memory Cure: How to Protect your Brain against Memory Loss and Alzheimer's Disease. New York: McGraw Hill, 2003. 2. Cummings JL. Alzheimer's disease. N Engl J Med 2004;351(1):56–67. 3. Green RC, et al. Risk of dementia among white and African American relatives of patients with Alzheimer disease. JAMA 2002;287(3):329–36. 4. Xu W, Qiu C, Gatz M, Pedersen NL, Johansson B, Fratiglioni L. Mid- and late-life diabetes in relation to the risk of dementia: a population-based twin study. Diabetes 2009;58(1):71–7. 5. Kivipelto M, Ngandu T, Laatikainen T, Winblad B, Soininen H, Tuomilehto J. Risk score for the prediction of dementia risk in 20 years among middle aged people: a longitudinal, populationbased study. Lancet Neurol 2006;5(9):735–41. 6. Gianaros PJ, Greer PJ, et al. Higher blood pressure predicts lower regional grey matter volume: Consequences on short-term information processing. Neuroimage 2006;31(2):754–65. 7. Wiseman RM, Saxby BK, et al. Hippocampal atrophy, whole brain volume, and white matter lesions in older hypertensive subjects. Neurology 2004;63(10):1892–7. 8. Macey PM, et al. Brain morphology associated with obstructive sleep apnea. Am J Respir Crit Care Med 2002;166(10):1382–7. 9. Minoguchi K, Yokoe T, Tazaki T, et al. Silent brain infarction and platelet activation in obstructive sleep apnea. Am J Respir Crit Care Med 2007;175(6):612–7. 10. Last D, Alsop DC, Abduljalil AM, et al. Global and regional effects of type 2 diabetes on brain tissue volumes and cerebral vasoreactivity. Diabetes Care 2007;30(5):1193–9. 11. Kivipelto M, Ngandu T, Fratiglioni L, et al. Obesity and vascular risk factors at midlife and the risk of dementia and Alzheimer disease. Arch Neurol 2005;62(10):1556–60. 12. Snowdon DA, Greiner LH, Mortimer JA, Riley KP, Greiner PA, Markesbery WR. Brain infarction and the clinical expression of Alzheimer disease. The Nun Study. JAMA 1997;277(10):813–7. 13. Schneider JA, Boyle PA, Arvanitakis Z, Bienias JL, Bennett DA. Subcortical infarcts, Alzheimer's disease pathology, and memory function in older persons. Ann Neurol 2007;62(1):59–66. 14. Erten-Lyons D, Woltjer RL, Dodge H, et al. Factors associated with resistance to dementia despite high Alzheimer disease pathology. Neurology 2009;72(4):354–60. 15. Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007;69(24):2197–204. 16. Abbott A. Neuroscience: The plaque plan. Nature 2008;456(7219):161–4. 17. Colcombe SJ, Erickson KI, Scalf PE, et al. Aerobic exercise training increases brain volume in aging humans. J Gerontol A Biol Sci Med Sci 2006;61(11):1166–70. 18. Erickson KI, Prakash RS, Voss MW, et al. Aerobic fitness is associated with hippocampal volume in elderly humans. Hippocampus 2009. 40 19. Cotman CW, Berchtold NC, Christie LA. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci 2007;30(9):464–72. 20. Neeper SA, Gomez-Pinilla F, et al. Physical activity increases mRNA for brain-derived neurotrophic factor and nerve growth factor in rat brain. Brain Res 1996;726(1–2):49–56. 21. Draganski B, Gaser C, Kempermann G, et al. Temporal and spatial dynamics of brain structure changes during extensive learning. J Neurosci 2006;26(23):6314–7. 22. Morris MC, Evans DA, Bienias JL, et al. Dietary fats and the risk of incident Alzheimer disease. Arch Neurol 2003;60(2):194–200. 23. Morris MC, Evans DA, Bienias JL, et al. Dietary intake of antioxidant nutrients and the risk of incident Alzheimer disease in a biracial community study. JAMA 2002;287(24):3230–7. 24. Engelhart MJ, Geerlings MI, Meijer J, et al. Inflammatory proteins in plasma and the risk of dementia: the rotterdam study. Arch Neurol 2004;61(5):668–72. 25. Szekely CA, Thorne JE, Zandi PP, et al. Nonsteroidal anti-inflammatory drugs for the prevention of Alzheimer's disease: a systematic review. Neuroepidemiology 2004;23(4):159–69. 26. Wengreen HJ, Munger RG, Corcoran CD, et al. Antioxidant intake and cognitive function of elderly men and women: the Cache County Study. J Nutr Health Aging 2007;11(3):230–7. 27. Zandi PP, Anthony JC, Khachaturian AS, et al. Reduced risk of Alzheimer disease in users of antioxidant vitamin supplements: the Cache County Study. Arch Neurol 2004;61(1):82–8. 28. Fotuhi M, Zandi PP, Hayden KM, et al. Better cognitive performance in elderly taking antioxidant vitamins E and C supplements in combination with nonsteroidal anti-inflammatory drugs: the Cache County Study. Alzheimers Dement 2008;4(3):223–7. 29. Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009;5(3):140–52. 30. Cole GM, Lim GP, Yang F, et al. Prevention of Alzheimer's disease: Omega-3 fatty acid and phenolic anti-oxidant interventions. Neurobiol Aging 2005;26 Suppl 1:133–6. 31. Fotuhi M, Times TNY. The New York Times Crosswords to Keep Your Brain Young: The 6-Step Age-defying Program. New York: St. Martin's Griffin, 2008. 32. Peters R, Beckett N, Forette F, et al. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG): a doubleblind, placebo controlled trial. Lancet Neurol 2008;7(8):683–9. 33. Hoffman LB, Schmeidler J, Lesser GT, et al. Less Alzheimer disease neuropathology in medicated hypertensive than nonhypertensive persons. Neurology 2009. 34. Kivipelto M, Solomon A. Cholesterol as a risk (reducing stress) are important for better memory and healthier brain—in both the short term and the long term. PN Majid Fotuhi, MD, PhD, is the Director of the Center for Memory and Brain Health at The Sandra and Malcolm Berman Brain & Spine Institute at LifeBridge Health, Sinai Hospital of Baltimore, and is an Assistant Professor of Neurology at Johns Hopkins University School of Medicine. factor for Alzheimer's disease—epidemiological evidence. Acta Neurol Scand Suppl 2006;185:50–7. 35. Kivipelto M, Solomon A, Blennow K, Olsson AG, Winblad B. The new cholesterol controversy— a little bit of history repeating? Acta Neurol Scand Suppl 2006;185:1–2. 36. Seshadri S, Wolf PA, Beiser A, et al. Stroke risk profile, brain volume, and cognitive function: the Framingham Offspring Study. Neurology 2004;63(9):1591–9. 37. Seshadri S, Beiser A, Selhub J, et al. Plasma homocysteine as a risk factor for dementia and Alzheimer's disease. N Engl J Med 2002;346(7):476–83. 38. Clarke R. Homocysteine, B vitamins, and the risk of dementia. Am J Clin Nutr 2007;85(2):329–30. 39. Vogiatzoglou A, et al. Vitamin B12 status and rate of brain volume loss in community-dwelling elderly. Neurology 2008;71(11):826–32. 40. Nilsson K, Gustafson L, Hultberg B. Improvement of cognitive functions after cobalamin/folate supplementation in elderly patients with dementia and elevated plasma homocysteine. Int J Geriatr Psychiatry 2001;16(6):609–14. 41. Luchsinger JA, Tang MX, Miller J, Green R, Mayeux R. Relation of higher folate intake to lower risk of Alzheimer disease in the elderly. Arch Neurol 2007;64(1):86–92. 42. Clarke R. Homocysteine-lowering vitamin B supplements do not improve cognitive performance in healthy older adults after two years. Evid Based Ment Health 2007;10(1):27. 43. Galli RL, Shukitt-Hale B, Youdim KA, Joseph JA. Fruit polyphenolics and brain aging: nutritional interventions targeting age-related neuronal and behavioral deficits. Ann N Y Acad Sci 2002;959:128–32. 44. Shukitt-Hale B, Carey AN, Jenkins D, Rabin BM, Joseph JA. Beneficial effects of fruit extracts on neuronal function and behavior in a rodent model of accelerated aging. Neurobiol Aging 2007;28(8):1187–94. 45. Yang X, Thomas DP, Zhang X, et al. Curcumin inhibits platelet-derived growth factor-stimulated vascular smooth muscle cell function and injury-induced neointima formation. Arterioscler Thromb Vasc Biol 2006;26(1):85–90. 46. Yang F, Lim GP, Begum AN, et al. Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo. J Biol Chem 2005;280(7):5892–901. 47. DeKosky ST, et al. Ginkgo biloba for prevention of dementia: a randomized controlled trial. JAMA 2008;300(19):2253–62. 48. DeKosky ST, Furberg CD. Turning over a new leaf: Ginkgo biloba in prevention of dementia? Neurology 2008;70(19 Pt 2):1730–1. 49. Ruitenberg A, van Swieten JC, Witteman JC, et al. Alcohol consumption and risk of dementia: the Rotterdam Study. Lancet 2002;359(9303):281–6. 50. Mehta KM, Ott A, Kalmijn S, et al. Head trauma and risk of dementia and Alzheimer's disease: The Rotterdam Study. Neurology Practical Neurology 1999;53(9):1959–62. 51. Plassman BL, Havlik RJ, Steffens DC, et al. Documented head injury in early adulthood and risk of Alzheimer's disease and other dementias. Neurology 2000;55(8):1158–66. 52. Bremner JD, Randall P, Scott TM, et al. MRIbased measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152(7):973–81. 53. McKenzie JE, Gentleman SM, et al. Increased numbers of beta APP-immunoreactive neurones in the entorhinal cortex after head injury. Neuroreport 1994;6(1):161–4. 54. Roberts GW, Gentleman SM, et al. Beta amyloid protein deposition in the brain after severe head injury: implications for the pathogenesis of Alzheimer's disease. J Neurol Neurosurg Psychiatry 1994;57(4):419–25. 55. Salmond CH, Menon DK, Chatfield DA, et al. Diffusion tensor imaging in chronic head injury survivors: correlations with learning and memory indices. Neuroimage 2006;29(1):117–24. 56. Findley LJ, Barth JT, et al. Cognitive impairment in patients with obstructive sleep apnea and associated hypoxemia. Chest 1986;90(5):686–90. 57. Ancoli-Israel S, Klauber MR, Butters N, Parker L, Kripke DF. Dementia in institutionalized elderly: relation to sleep apnea. J Am Geriatr Soc 1991;39(3):258–63. 58. Yaggi HK, Concato J, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005;353(19):2034–41. 59. Wilson RS, Bennett DA, et al. Cognitive activity and incident AD in a population-based sample of older persons. Neurology 2002;59(12):1910–4. 60. Fratiglioni L, Paillard-Borg S, Winblad B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol 2004;3(6):343–53. 61. Glymour MM, Weuve J, et al. Social ties and cognitive recovery after stroke: does social integration promote cognitive resilience? Neuroepidemiology 2008;31(1):10–20. 62. Ertel KA, Glymour MM, Berkman LF. Effects of social integration on preserving memory function in a nationally representative US elderly population. Am J Public Health 2008;98(7):1215–20. 63. Wang HX, Karp A, Herlitz A, et al. Personality and lifestyle in relation to dementia incidence. Neurology 2009;72(3):253–9. 64. Videbech P, Ravnkilde B. Hippocampal volume and depression: a meta-analysis of MRI studies. Am J Psychiatry 2004;161(11):1957–66. 65. Sheline YI, Gado MH, Kraemer HC. Untreated depression and hippocampal volume loss. Am J Psychiatry 2003;160(8):1516–8. 66. Santarelli L, Saxe M, Gross C, et al. Requirement of hippocampal neurogenesis for the behavioral effects of antidepressants. Science 2003;301(5634):805–9. 67. Tsutsumi A, Kayaba K, et al. Prospective study on occupational stress and risk of stroke. Arch Intern Med 2009;169(1):56–61. March/April 2009