Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Convolutional neural network wikipedia , lookup
End-plate potential wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Neurotransmitter wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Neural coding wikipedia , lookup
Haemodynamic response wikipedia , lookup
Optogenetics wikipedia , lookup
Biological neuron model wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Development of the nervous system wikipedia , lookup
Types of artificial neural networks wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Chemical synapse wikipedia , lookup
Central pattern generator wikipedia , lookup
Axon guidance wikipedia , lookup
Nervous system network models wikipedia , lookup
Synaptogenesis wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Channelrhodopsin wikipedia , lookup
Neuroanatomy wikipedia , lookup
Microneurography wikipedia , lookup
Synaptic gating wikipedia , lookup
Syncope (medicine) wikipedia , lookup
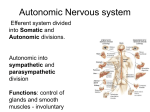
Autonomic Nervous System Anatomy & Physiology Diseases & Evaluation 2014 John Kincaid MD Origin of Concepts • In the 2nd century A.D. Galen concluded that nerves were tubes which distributed “animal spirits” throughout the body • The coordination of body functions by these tubes and spirits was “sympathy” • 1700’s: Winslow used the term Sympathetic for the chain of nerves running parallel to the spinal cord • Late 1800’s & early 1900’s: Langley & Gaskell defined the “Visceral” nervous system to consist of Sympathetic, Parasympathetic & Enteric components • Langley’s concept was an Efferent system only • Langley suggested Autonomic as a substitute for visceral or vegetative Autonomic: auto = self nomos = law Langley” 3 Autonomic Divisions: •Sympathetic •Parasympathetic •Enteric •The Sympathetic division was the “Thoraco-Lumbar” •The Parasympathetic division was the “Cranio-Sacral” •The Enteric division was intrinsic to the GI system Rhoades 2nd ed Fig 6-4 Sympathetic action is done by a two neuron chain: •Preganglionic neuron (1st order) & Postganglionic neuron (2nd order) •Preganglionic neurons arise from the intermediolateral column of the spinal cord between T1 & L3 •Postganglionic neurons arise from the paravertebral or prevertebral ganglia in the abdomen Low 1st ed Fig 1-1 •Preganglionic sympathetic axons exit a spinal nerve to a sympathetic ganglia via a “white ramus” •Synapse with postganglionic neurons may occur at that or higher/lower spinal levels •Most postganglionic neurons rejoin the spinal nerve via the “gray ramus” to cutaneous, vascular & muscle targets in the trunk & limbs •Preganglionic axons to intra-abdominal structures go through paravertebral ganglia to prevetebral ganglia •Sympathetic function tends to “diverge” •One preganglionic neuron may synapse with up to 100 postganglionic neurons Parasympathetic action also uses a two neuron chain •Preganglionic neurons arise from brainstem nuclei & the sacral spinal cord •Postganlionic neurons arise in ganglia located on or in the target structures •Parasympathetic action tend to be less divergent than sympathetic Low 1st ed Fig 1-3 Anatomical Issues How do sympathetic axons get from Th1 to the eye OR from L3 to the bottom of the foot? Where are the parasympathetic ganglia for the heart ,lungs, intestines, and bladder? What is the parasympathetic role in cutaneous functions? How do sympathetic axons get to the heart & lungs? Cardiac Autonomic Pathways Cardiac sympathetic output via “cardiac nerves” • Superior, middle & inferior cervical ganglia • Upper 3 thoracic levels Haines, 2nd ed Autonomic Neurotransmitters •Acetylcholine is the transmitter at preganglionic synapses in both systems •The receptor is similar to the neuromuscular junction synapse: directly gated channel which responds to the agonist nicotine •The postganglionic parasympathetic transmitter also is acetylcholine •The receptors are indirectly gated and respond to the agonist muscarine Rhoades 2nd ed Fig 6-2 The neurotransmitter at postganglionic SYMPATHETIC synapses is norepinephrine ( with one exception ) •The receptor is an indirectly gated G protein linked type •There are 2 general subtypes of postganglionic norepinephrine synapses: alpha & beta •These two synapses use different 2nd messenger systems & respond to different agonists ADD Stuff •The exception to norepinephrine is the sweat glands whose postganglionic neurons release acetylcholine Adrenal Medulla • • • • • The adrenal medulla is the “macro” nerve terminal of the sympathetic system Preganglionic axons pass through the paravertebral ganglia to terminate directly on the chromaffin cells of the adrenal medulla These cells release neurotransmitters directly into the circulation The output is 80% epinephrine The effect of vascular delivery lasts 5x longer than by release from postsynaptic nerves nd Non-adrenergic Non-cholinergic Neurons (NANC) • Some autonomic neurons release Nitric Oxide (NO) instead of norepinephrine or acetylcholine • NO releasing parasympathetic neurons innervate the corpus cavernosa of the penis • Nitric oxide release stimulates production of cyclic GMP & vasodilatation in the corpus • Phosphodisterase type 5 breaks downs GMP • Sildenafil or CIAlis inhibits this enzyme & enhances local vascular “performance” • Neuropeptides & autonomic fx Autonomic Functions Effector Pupil Sweat glands Blood vessels Skin Muscle Heart rate Bronchioles Parasymp Symp Constrict None Dilate Secrete None (face) None Decrease Constrict Constrict* Constrict* Increase Dilate Autonomic Functions Effector GI tract wall muscles Glands Urinary system Detrusor Sphincter Genitalia Parasymp Symp Contract Secrete Relax Inhibit Contract Relax Relax Contract Engorge Contract Gastrointestinal Control • The Enteric nervous system in walls of GI tract can function semiindependently • Effects: motility, secretion & blood flow • Autonomic action can influence these activities • Efferent and afferent components ( 90% of vagal axons are sensory) Vago-vagal reflexes Low, Clinical Autonomic Disorders 3rd ed Gastrointestinal Control • Parasympathetic GI input is mostly above the small intestine & below the transverse colon • Sympathetic input is more widespread • Parasympathetic action increases motility & secretion • Sympathetic action inhibits motility & secretion increases local blood Barfing flow Low, Clinical Autonomic Disorders 3rd ed Bladder Control • Parasympathetic input via Pelvic Splanchnic nerves Bladder wall (detrusor) Internal Sphincter • Sympathetic input via Hypogastric Nerves • Somatic input via Pudendal Nerve Voluntary sphincter • Afferent components Autonomic Nerves Wilson-Pauwels 1997 Fig CS 4-1 Bladder Control Pontine Micturaton Center Bladder Filling • Sympathetic action inhibits bladder wall contraction & enhances internal sphincter contraction Bladder Emptying • Sympathetic output is inhibited • Sensory input is allowed to activate parasympathetic mediated contraction of the detrusor & relaxation of internal sphincter • Pudendal somatic activity to the voluntary sphincter is inhibited • Disease effects Mathias & Bannister Central Autonomic Network • Cortical areas: Insular, anterior cingulate, prefrontal • The amygdala & lateral hypothalamus are the conduits for emotion related input • The suprachiasmatic & medial hypothalamic nuclei regulate circadian & homeostatic functions Mathias & Bannister 4th ed Thermoregulation Hypothalamic zones • Medial preoptic nuclei: warm sensing neurons which initiate heat dissipation • Dorsomedial & posterior nuclei: cold sensing neurons which initiate shivering and metabolic heat production • Both project to medullary raphe region Haines Fundamental Neuroscienc 30-6 Central Autonomic Network • The periaqueductal gray matter receives efferent input from the hypothalamus • Afferent input is via the Nucleus Tractus Solitarius (NTS) • The ventral-lateral medulla is the origin of efferent parasympathetic & sympathetic activity • The intermediolateral cell column of the spinal cord is the efferent pathway for sympathetic activity Central Autonomic Network Afferent input via: • Nucleus of the Solitary Tract (NTS) via Facial, glossopharyngeal & vagal axons from: taste buds on tongue baroreceptors (carotid & aortic sinuses) chemoreceptors ( carotid body), pulmonary and cardiac stretch receptors • Spinal cord from: visceral, • Low Clinical Autonomic Disorders 3rd ed thermo, ergo & nociceptic receptors Afferent data passes via spinal nerves & spinothalamic tract to thalamus & to insular cortex Efferent Actions • Ventrolateral Medulla is efferent path for: vasomotor tone (S) cardiac regulation (P &S) respiratory drive (Som) GI regulation (P & S) • Ventral medullary raphe is sympathetic pathway to sweat gland (sudomotor) & vasomotor control to the skin Low, Clinical Autonomic Disorders 3rd ed Blood Pressure & Cardiac Control • Ventral lateral medulla regulates blood pressure & heart rate responses to orthostatic, exercise & emotional challenges • Baroreceptor (BR) reflex is the main pathway for this control • Transmitters: Glutamate & Gaba Fig 4.3 Low, Clinical Autonomic Disorders 3rd ed Blood Pressure & Cardiac Control BRs are mechanosensitive endings in carotid & aortic sinuses • Continous discharge pattern which ↑ in systole & ↓ in diastole • Sustained ↑ in BP ↑ BR discharge rate which then Inhibits output of RVLM to spinal sympathetic neurons & Enhances vagal (nucleus ambiguus) output to the heart Blood Pressure & Cardiac Control BR reflex allows us to stand up without fainting • Upright posture shifts ~500 ml of blood to the lower body • ↓ venous return & ↓ cardiac output unloads BRs • ↓ vagal & ↑ sympathetic output via BR reflex maintains BP & cardiac output • In first 15-30 sec post standing BP is supported by ↓ vagal output resulting in ↑ heart rate • At 1-2 minutes post standing sympathetic output ↑ to maintain pressure Mechanism of Syncope Normals have 20 mm or less drop in systolic BP after 2 minutes of standing Autonomic Dysfunction • Ocular: Impaired adjustment to lighting levels • Secretomotor: Dry Eyes or Mouth • Orthostatic: Dizziness, weakness, exercise intolerance & syncope when upright • Enteric: Bloating, early satiety, nausea, constipation, diarrhea • Urological: Impaired emptying, incontinence Autonomic Dysfunction • • • • Sexual: Erectile & ejaculatory dysfunction Sudomotor: Deficient or excess sweat output Vasomotor: Skin color & temperature dysfx Endocrine: Hypoglycemic unawareness Autonomic Dysfunction Primary Diseases • Multi-system atrophy (Shy Drager) • Pure Autonomic Failure ( Idiopathic orthostatic hypotension) • POTS (Postural Orthostatic Tachycardia Syndrome) • Primary hyperhydrosis Secondary Conditions • • • • • • Diabetic Neuropathy Amyloidosis Acute Pandysautonomia ( GBS variant) Lambert Eaton Syndrome Hypohydrosis ( Ross syndrome) Neuro-cardiogenic Syncope Autonomic Dysfunction Postural Orthostatic Tachycardia Syndrome (POTS) • Heart rate ↑ > 30 bpm or to > 120 bpm within 10 minutes of standing • Orthostatic BP Δ within normal range • Orthostatic intolerance symptoms • Female / Male 5:1 most pts 20-40 yrs • ? Post-viral etiology in some Autonomic Dysfunction POTS • • • • • • Possible pathologic mechanisms Excessive sympathetic tone Excessive venous pooling (limb denerv) β receptor supersensitivity α receptor hyposensitivity Altered parasympath / sympath balance Brain stem dysregulation Autonomic Evaluation Pupillary responses to light & dark Tear & Salivary output BP maintenance during standing for 2-3 minutes / Check BP & HR Early responses (Parasympathetic withdrawl) ↑ HR Later Response (Sympathetic increase) • As blood pools in legs cardiac return ↓ • Sympathetic response constricts capacitance blood vessels, ↑ HR & leg muscle contraction • Response max @ ~ 2 minutes • BP should ↓ < 20 mm systolic ( < 10 mm diastolic) • HR should ↑ > 10-20 Tilt table testing eliminates leg muscle contraction component of orthostatic response Autonomic Testing Evaluation of the Orthostatic Response • In normals HR ↑ by ~ 15 sec and then ↓ by ~ 30 sec after standing • 30 : 15 ratio: Longest to Shortest RR interval in 1st 30 beats after standing < ~1.15 is abnormal This component of the orthostatic response is vagally mediated: reduction in parasympathetic output to the heart with resulting ↑ HR Autonomic Testing Valsalva Maneuvre Mathias & Bannister 4th ed Fig 21.6 • Abrupt sustained ↑ intra thoracic pressure: 40 mmHg blow for 15 sec while sitting • Immediate HR ↓ at onset & gradual ↑ until pressure released & then reflex bradycardia occurs • Valsalva ratio is HR @1 / HR @ 2 • Nl > ~ 1.3 • Cardiovagal (parasympathetic) test Cardiovascular – Valsalva Maneuver 280 120 Wolfgang Singer Mayo Rochester 240 80 Heart rate 40 160 0 Systolic BP 120 -40 Diastolic BP 80 -80 40 -120 0 10 20 30 40 50 60 70 80 Parasympathetic and Sympathetic components Time (sec) 90 100 110 HR (bpm) BP (mmHg) 200 Autonomic Evaluation Hear rate Δ with respiration Mathias & Bannister 4th ed Fig • In normal respiration HR ↑ during Inspiration & ↓ during Expiration • Normal “sinus arrythmia” • Do 10 cycles of 6/minute respiration while assessing HR • I:E Normal Δ 10-15 BPM • Cardiovagal (parasympathetic) test Autonomic Evaluation Sudomotor (Sweat) function • Temperature sensing • Hypothalamic control • Sympathetic (cholinergic) output • Sweat production Evaluate by: • Heating whole body & assess sweating pattern TST (thermoregulatory sweat test) OR Low ,Clinical Autonomic Disorders 2nd ed Ch19, Fig 3 Autonomic Evaluation •Locally applied stimului: Quantitative Sudomotor Axon Test: QSART Low, Clinical Autonomic Disorders 2nd Methodology • Ach locally iontophoresed into the skin • Sweat glands activated • Sweat out put ed Ch 15, Fig 3 measured Autonomic Evaluation QSART Patterns RSD & Neuropathic pain Low, Clinical Autonomic Disorders 2nd ed Ch 15 Fig 4 Fig 3 Autonomic Evaluation • What we are currently doing @ IU Health