Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epigenetics of human development wikipedia , lookup
Molecular Inversion Probe wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Deoxyribozyme wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Oncogenomics wikipedia , lookup
Metagenomics wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Epigenomics wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gel electrophoresis of nucleic acids wikipedia , lookup
Gene expression programming wikipedia , lookup
Gene desert wikipedia , lookup
Genetic engineering wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Gene nomenclature wikipedia , lookup
Point mutation wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Genome evolution wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Gene expression profiling wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Copy-number variation wikipedia , lookup
Genome editing wikipedia , lookup
Genome (book) wikipedia , lookup
Gene therapy wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
History of genetic engineering wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
SNP genotyping wikipedia , lookup
Microsatellite wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Bisulfite sequencing wikipedia , lookup
Helitron (biology) wikipedia , lookup
Designer baby wikipedia , lookup
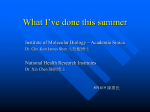
Clinical Chemistry 52:12 2203–2210 (2006) Molecular Diagnostics and Genetics Quantitative Assay of Deletion or Duplication Genotype by Capillary Electrophoresis System: Application in Prader–Willi Syndrome and Duchenne Muscular Dystrophy Chia-Cheng Hung,1† Chih-Ping Chen,2, 3† Shuan-Pei Lin,3, 4 Shu-Chin Chien,5 Chien-Nan Lee,6 Wen-Fang Cheng,6 Wu-Shiun Hsieh,7 Ming S. Liu,8 Yi-Ning Su,9, 10* and Win-Li Lin1 Background: Deletions and duplications involving large DNA segments result in underexpression or overexpression, depending on the changes in allele dose, and are known to cause many common disorders. Detection of allele dose variations in the human genome is increasingly important in medical genetic diagnosis. Methods: We used multiplex quantitative PCR coupled with capillary electrophoresis for accurate allele dose determination. In cases of Prader–Willi syndrome (PWS), a total of 24 patients with PWS, as well as 205 control individuals from the general population, were analyzed by use of multiplex quantitative PCR to amplify the FGFR2 gene, the KRIT1 gene, and the SNRPN gene simultaneously. In cases of Duchenne muscular dystrophy (DMD), we optimized the multiplex quantitative PCR to amplify 38 exons to analyze the DMD gene for rapid diagnosis of 12 DMD-affected males, 12 obligate carriers from families, and 50 unaffected female controls. 1 Institute of Biomedical Engineering, College of Medicine and College of Engineering, and 9 Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan. 2 Department of Obstetrics and Gynecology, 3 Department of Medical Research, and 4 Department of Pediatrics, Mackay Memorial Hospital, Taipei, Taiwan. 5 Departments of Medical Genetics and Obstetrics and Gynecology, China Medical University Hospital, Taichung, Taiwan. Departments of 6 Obstetrics and Gynecology, 7 Pediatrics, and 10 Medical Genetics, National Taiwan University Hospital, Taipei, Taiwan. 8 Institute eGene, Inc., Irvine, CA. † These authors contributed equally to this study. *Address correspondence to this author at: Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan. Fax 886-2-23813690; e-mail: [email protected]. Received March 31, 2006; accepted September 19, 2006. Previously published online at DOI: 10.1373/clinchem.2006.071118 Results: We were able to unambiguously diagnose the deletion genotype in PWS patients and identify all deletion or duplication genotypes and carrier status in DMDaffected cases with 100% sensitivity and specificity. Conclusions: This report describes a novel single assay that can rapidly quantify allele dose to provide accurate clinical genetic diagnosis. This technique offers a valuable alternative for the rapid detection of genomic deletions or duplications and decreases costs because it does not require expensive fluorescent reagents. © 2006 American Association for Clinical Chemistry Deletions and duplications involving large DNA segments are known to cause many common disorders. They lead to underexpression or overexpression, depending on changes in allele dose (1 ). Detection of allele dose variations in the human genome is increasingly important in medical genetic diagnosis. Prader–Willi syndrome (PWS)11 is a complex developmental and neurobehavioral disorder, with an overall incidence of 1 in 10 000 newborns (2 ). This severe neurobehavioral disease has been reported to be caused by loss of function of paternal-derived genes from chromosome 15, especially a related SNRPN 12 gene on chromo- 11 Nonstandard abbreviations: PWS, Prader–Willi syndrome; DMD, Duchenne muscular dystrophy; FISH, fluorescence in situ hybridization; MLPA, multiplex ligation-dependent probe amplification; HDA, high-performance DNA analysis. 12 Human genes: SNRPN, small nuclear ribonucleoprotein polypeptide N; DMD, dystrophin (muscular dystrophy, Duchenne and Becker types); FGFR2, fibroblast growth factor receptor 2 (bacteria-expressed kinase, keratinocyte growth factor receptor, craniofacial dysostosis 1, Crouzon syndrome, Pfeiffer syndrome, Jackson-Weiss syndrome); KRIT1, KRIT1, ankyrin repeat containing. 2203 2204 Hung et al.: Quantitative Assay of Deletion or Duplication Genotype some 15q11.2– q13 (3, 4 ). Approximately 70% of PWS cases are associated with a de novo paternally derived deletion, ⬃25% with maternal uniparental disomy 15, and the rest with deletions or epimutations in the imprinting center or from chromosome 15q translocations (5–7 ). Duchenne muscular dystrophy (DMD), one of the most common lethal genetic disorders in children, affects 1 in 3500 newborn males (8 ) and is inherited in an X-linked recessive pattern, resulting from variations in the DMD gene on Xp21.1. The DMD gene, consisting of 79 exons and spanning a region of 2.4 million bp of genomic DNA, is the largest known human gene (9, 10 ). Approximately 55%– 65% of DMD cases are associated with large intragenic deletions or duplication, ⬃5%–10% with duplications of large segments (11 ), and the remaining cases with point variations, small deletions, or insertions (12 ). Approximately 1⁄3 of cases arise from de novo variations without family history, and 2⁄3 are inherited from female carriers (13 ). Detection and identification of female carriers and noncarriers are important for genetic counseling. In general, the hybridization-based techniques, including fluorescence in situ hybridization (FISH) (14, 15 ) and Southern blotting (11, 16 ), are the most common approaches for the detection of gene deletions, but these are time-consuming and labor-intensive and cannot be used with high-throughput strategies. Moreover, Southern blotting requires relatively large amounts of genomic DNA. Multiplex amplifiable probe hybridization (17, 18 ) and multiplex ligation-dependent probe amplification (MLPA) (19 –21 ) are rapid techniques involving preparation of only 2 reactions and are efficient primary methods to diagnose deletion and duplication genotypes. These assays rely on detection of fluorescence, however, and require relatively expensive reagent sets. Multiplex quantitative PCR is a new approach for the detection of gene deletions, duplications, and rearrangements (22 ). In recent years, several new techniques have been developed for the quantitative assay of PCR products, including fluorescence-based strategies (23–27 ), microchip electrophoresis (28 –31 ), denaturing HPLC (32, 33 ), capillary electrophoresis (34, 35 ), and mass spectrometry (36 ). Capillary electrophoresis is a simple, high-performance, reliable, high-resolution, timesaving, and low labor-intensive technique that has shown promise as a sensitive and specific tool for the separation of biomolecules and the detection of variations in DNA (37– 40 ). We present a new method for high-throughput PWS deletion analysis and DMD deletion/duplication determination by multiplex quantitative PCR coupled with a high-performance DNA analysis (HDA) system that uses capillary electrophoresis for accurate determination of allele dose. This method allows transmission of 524 nm excitation light superbright light-emitting diodes based on indium gallium nitride material technology (41 ). Materials and Methods patient samples DNA samples from all PWS patients, DMD patients, family members, and unaffected individuals were obtained from National Taiwan University Hospital. A total of 229 DNA samples were analyzed in the PWS deletion study, including specimens from 24 patients with a diagnosis of PWS and 205 unaffected individuals from the general population. A total of 74 DNA samples were analyzed in the DMD deletion/duplication study, including 12 patients with a diagnosis of DMD, 12 obligate carriers from families, and 50 unaffected females from the general population. Genomic DNA was collected from peripheral whole blood with a Chemagic DNA Blood Kit (Chemagen), according to the manufacturer’s instructions. This study was approved by the Ethics Committee of the Department of Medical Genetics, National Taiwan University. multiplex quantitative pcr for pws deletion study Multiplex quantitative PCR was used to amplify the FGFR2, KRIT1, and SNRPN genes (FGFR2 forward, CAC AAT CAT TCC TGT GTC GT; FGFR2 reverse, AGC AGT CAA CCA AGA AAA GG; KRIT1 forward, TTC GAA TGG CTA CTT CTA CCT G; KRIT1 reverse, AAA ACG TCT TTT AAA TCA GAG C; SNRPN forward, CTT TGT ACT CCT CCA GCA AC; SNRPN reverse, TAC AGG AAT GAA AGG CAT TA). The KRIT1 and FGFR2 genes were used as internal controls for determining the relative allele dose of the SNRPN gene. All multiplex quantitative PCR amplifications were designed in a total volume of 25 L containing the following: 100 ng of genomic DNA; 0.04 M each primer of the FGFR2 gene; 0.08 M each primer of the KRIT1 gene; 0.2 M each primer of the SNRPN gene; 200 M dNTPs; 0.5 units of AmpliTaq Gold enzyme (PE Applied Biosystems); 2.5 L of GeneAmp 10⫻ buffer II (10 mmol/L Tris-HCl, pH 8.3, 50 mmol/L KCl), in 2 mmol/L MgCl2 as provided by the manufacturer. Amplification was performed in an MBS thermocycler (ThermoHybaid). PCR amplification was performed with an initial denaturation step at 95°C for 10 min, followed by 25 cycles consisting of denaturation at 94°C for 30 s, annealing at 53°C for 45 s, extension at 72°C for 45 s, and then a final extension step at 72°C for 10 min. multiplex quantitative pcr for dmd deletion/ duplication study Multiplex quantitative PCR of the DMD gene was performed with primers as designed in previous studies (42– 44 ). Eight sets of multiplex PCRs were used to optimize the system and allow the amplification of 38 exons. The primers are listed in Table 1 in the Data Supplement that accompanies the online version of this article at http://www.clinchem.org/content/vol52/ issue12. Each multiplex PCR for the DNA fragments was performed in a total volume of 50 L containing the Clinical Chemistry 52, No. 12, 2006 following: 200 ng of genomic DNA; 0.04 to 0.4 mol/L each primer; 200 mol/L dNTPs; 1 unit of AmpliTaq Gold enzyme (PE Applied Biosystems); and 5 L of GeneAmp 10⫻ buffer II (10 mmol/L Tris-HCl, pH 8.3, 50 mmol/L KCl) in 2 mmol/L MgCl2 as provided by the manufacturer. PCR amplification was performed on an MBS thermocycler (ThermoHybaid) with 95°C for 10 min followed by 24 cycles of 94°C for 1 min, melting temperature for 1 min, 72°C for 3 min, and final extension at 72°C for 10 min. hda capillary electrophoresis system For rapid DNA separation and detection we used an HDA capillary electrophoresis system with CK-5000 disposable cartridge (eGene) (41 ). The gel-matrix in the gel cartridge consists of proprietary linear polymer with ethidium bromide dye. The system was used according to the manufacturer’s operation manual: 2 L of unpurified multiplex quantitative PCR products were directly diluted 10-fold with 18 L of deionized H2O. The samples were placed in the instrument sample tray and were automatically injected into the capillary channel and subjected to electrophoresis by selecting the OM900.mtd method from BioCalculator software. The sample injection voltage was 5 kV with sample injection time of 20 s followed by separation voltage of 3 kV and separation time of 900 s. The system can simultaneously analyze 12 PCRs in 10 min. determination of total snrpn gene copy number The specific multiplex quantification PCR was analyzed by the HDA capillary electrophoresis system. The quantification of DNA fragments was based on the integrated peak area automatically determined by BioCalculator software. Total SNRPN gene copy numbers were calculated by adjusting the relative known doses of the FGFR2 and KRIT1 genes. We used the following equation to calculate the copy number of the SNRPN gene in the unknown samples (U) compared with the control samples (C): 2205 Results multiplex quantitative pcr We performed multiplex quantitative PCR amplification with a total of 229 DNA samples to identify the PWS genotype with the SNRPN gene segment and the control FGFR2 and KRIT1 gene segments. For the DMD deletion/ duplication study, the technique was also used to detect common exon deletions and duplications in the DMD gene. Thirty-eight DNA fragments were assigned to 8 sets of multiplex quantitative PCRs according to their sizes. Annealing temperature, template concentration, primer concentrations, and number of cycles were optimized for different genes/amplicons. We tested the relationship between the number of PCR cycles and the amount of PCR product to determine the linearity of the PCR (45 ). Up to 25 cycles, PCR is in the exponential phase (46, 47 ). Therefore, we standardized the number of PCR cycles in our multiplex quantitative PCR to 25 cycles. capillary electrophoresis for pws deletion study The PCR products had different fragment sizes: FGFR2, 251 bp; KRIT1, 326 bp; and SNRPN, 448 bp. The diluted crude PCR products were injected directly into the capillary channel on the HDA system. The results of analysis of amplification by the HDA system of FGFR2, KRIT1, and SNRPN gene segments in several samples from PWS patients with deletions, PWS patients without deletions, and unaffected individuals are shown in Fig. 1. Deletions in the PWS patients were further confirmed by FISH studies with SNRPN probes (see Fig. 1 in the online Data Supplement). Diagnostic results obtained in PWS patients with deletion by the HDA capillary electrophoresis system were comparable to those obtained with FISH technology. quantification of snrpn genes The 3 continuous peaks shown in Fig. 1 represent the FGFR2, KRIT1, and SNRPN genes, respectively. Total copy numbers of the SNRPN gene calculated from the Peak area of SNRPN (U)/[Peak area of FGFR2 (U)] ⫻2 Peak area of SNRPN (C)/[Peak area of FGFR2 (C)] or Peak area of SNRPN (U)/[Peak area of KRIT1 (U)] ⫻2. Peak area of SNRPN (C)/[Peak area of KRIT1 (C)] determination of dmd gene copy number In the DMD deletion/duplication study, we used BioCalculator software to measure the areas of the different peaks from each exon. To identify carrier status in females on the basis of findings of large deletions or duplications in the allele dose analysis, we determined the copy number of specific test exons in the unknown samples as described in our previous report (33 ). Fig. 1. Separation of FGFR2, KRIT1, and SNRPN amplified DNA fragments by capillary electrophoresis on the HDA system in PWS with deletion (A), PWS without deletion (B), and unaffected individuals (C). ●, FGFR2 gene; », KRIT1 gene; ✻, SNRPN gene. 2206 Hung et al.: Quantitative Assay of Deletion or Duplication Genotype Fig. 2. Total copy numbers of SNRPN gene determined by multiplex quantitative PCR with HDA capillary electrophoresis system assay. (A), measured for the KRIT1 gene. (B), measured for the FGFR2 gene. results of multiplex quantitative PCR for the reference gene (KRIT1) in 24 PWS patients and 205 unaffected individuals from the general population are graphically displayed in Fig. 2A. The results of calculation of the copy numbers with FGFR2 as the control gene are shown in Fig. 2B. Comparison of results revealed patients had similar copy numbers for these genes. The SNRPN gene copy number in samples from PWS patients with deletions was virtually identical to the expected value of 1, and the nondeletional samples and those from unaffected populations were close to a copy number of 2. Statistical analysis revealed that deletion type could be distinguished from nondeletion type with an uncertainty of P ⬍0.0001 (Table 1). To test the validity and reproducibility of our system for dose determination of the SNRPN gene, we analyzed patient samples repeatedly at least 3 times, and the results were all demonstrated to be reproducible. capillary electrophoresis for dmd deletion/ duplication study After amplification of the DMD gene, we analyzed the multiplex PCR products with both gel electrophoresis and the HDA capillary electrophoresis system for the detection of different exons of the DMD gene (Fig. 3A). The corresponding signals in the HDA capillary electrophoresis system were compared with bands separated by gel electrophoresis and stained with ethidium bromide (Fig. 3B). The lower sensitivity of ultraviolet gel-based detection led to differences between band intensities on gel and values obtained with the HDA method. The results of multiplex quantitative PCR coupled with HDA capillary electrophoresis system analysis in affected males, carriers, and unaffected individuals are shown in Fig. 4. The results were analyzed by use of the ratios of deleted and undeleted exons. The absence of corresponding signals in the affected cases compared with unaffected controls (Fig. 4B) indicates the deleted exons in the DMD patient. The decreased amplification in the corresponding signals for deleted exons in a DMD carrier are shown in Fig. 4C, and increased amplification in the corresponding signals in a DMD patient with duplicated exons and a carrier are shown in Fig. 4, D and E. Every sample was analyzed at least 3 times, and the results were reproducible. quantification of dystropin genes The copy numbers of the DMD gene as determined by multiplex quantitative PCR and HDA capillary electrophoresis system analysis in deleted carriers, nondeleted carriers, and unaffected females expressed in test exon: reference exon ratios are shown in Fig. 2 in the online Data Supplement. Use of this analytical tool with the measured copy numbers allowed unambiguous differentiation between deleted and undeleted exons, enabling successful identification of unaffected females and deleted carriers. Moreover, we successfully determined that 1 of the DMD patients had duplication of exons 13–17 and another had duplication of exons 50 –58. There was no diagnostic value within the indeterminate interval, even for females with unknown status (see Table 2 in the online Data Supplement). quantitative real-time pcr We used a quantitative real-time PCR assay to verify the status of the deleted carriers and nondeleted carriers identified by the multiplex quantitative PCR with HDA capillary electrophoresis system analysis (48 ). Results of allele dose analysis for exons 6 and 51 according to their deletion rates in the DMD patients are shown in Fig. 3 in the online Data Supplement. When the DNA sample was from a carrier of a deletion including exon 6 or 51, the signal corresponding to the deleted exon was approximately half that of an unaffected female [1.12 (0.18) for exon 6 and 1.15 (0.20) for exon 51]. The findings of the quantitative real-time PCR-based assay were compatible with those of multiplex quantitative PCR and HDA capillary electrophoresis system allele dose analysis for both deleted carriers and nondeleted carriers. These findings demonstrated that this multiplex quantitative PCR technique can reliably detect DMD-affected males and female carriers. Table 1. Copy numbers of the SNRPN gene calculated by the HDA capillary electrophoresis system. Samples Expected gene copy number Measured copy number by KRIT1 gene, mean (SD) Measured copy number by FGFR2 gene, mean (SD) Unaffected individuals (n ⫽ 205) PWS patients without deletions (n ⫽ 12) PWS patients with deletions (n ⫽ 12) 2 2 1 2.009 (0.134) 2.028 (0.154) 1.023 (0.139) 1.992 (0.137) 2.080 (0.089) 1.046 (0.089) Clinical Chemistry 52, No. 12, 2006 2207 Fig. 3. Exons of DMD gene detected by 8 different multiplex quantitative PCR sets. (A), detection by HDA capillary electrophoresis system. (B), detection by gel electrophoresis. The DNA fragments were separated by 1.5% agarose gel staining with ethidium bromide. Discussion HDA is a high-throughput, multichannel, and microcapillary electrophoresis method that provides a simple, rapid, and reliable alternative to genetic quantification. This method allowed the precise and efficient identification of trisomic and disomic animals (49 ). In designing the multiplex PCR used in the present study, we chose to amplify the diagnostic SNRPN gene as the largest product rather than as a size between the 2 internal standard genes. Variations in the quality of the extracted DNA can have major effects on amplification efficiency, with the largest effects seen in the larger products in a multiplex reaction. However, our previous multiplex quantitative genotype analysis studies with HPLC instruments showed that competitive PCR allowed the accurate determination of allele dose variations (32, 33, 50, 51 ). PWS is a complex genetic disorder characterized by small hands and feet, short stature, poor sucking, feeding difficulties, hypotonia, hypogonadism, hyperphagia, early childhood obesity, and a chromosome 15q11– q13 deletion in the majority of cases. The current diagnostic approach when the syndrome is suspected is methylation testing and FISH with the SNRPN and control probes from chromosome 15. Methylation PCR is accurate in 99% of PWS patients, and 70% of PWS patients have the chromosome 15q11– q13 deletion confirmed with FISH analysis and methylation PCR. In cases of FISH results indicating the wild-type gene but continued suspicion of PWS, analysis of DNA obtained from parents and the affected individual should be performed to detect possible maternal disomy 15 and/or an imprinting defect. In this report, we describe an alternative molecular method that uses 2208 Hung et al.: Quantitative Assay of Deletion or Duplication Genotype Fig. 4. The results of multiplex quantitative PCR coupled with HDA capillary electrophoresis system analysis in affected males, carriers, and unaffected individuals (A), unaffected individual; (B), deleted DMD-affected male; (C), the carrier individual with deleted exon 51; (D), duplicated DMD-affected male; (E), the carrier individual with duplicated exon 51. capillary electrophoresis based quantitative assay for determining the deletion status. This assay is less expensive and less time-consuming than FISH analysis, but for identifying the typical deletion seen in PWS patients it is as accurate as chromosome testing and the SNRPN probe. The results obtained with this multiplex PCR/HDA system are compared with findings by other methods to diagnose PWS in Table 2. To calculate the total SNRPN allele dose, we used 2 autosomal genes outside of chromosome 15 (KRIT1 and FGFR2) as controls with a copy number of 2 in relation to the SNRPN probe, which would have a copy number of only 1 in a PWS patient with a paternally derived deletion. DMD is the most common lethal neuromuscular genetic disorder in males. Affected patients usually present with proximal muscle weakness and pseudohypertrophy at an early age, invariably become wheelchair bound, and eventually die prematurely. Effective treatment has not been found, and current management strategies consist of identifying DMD carriers so that early interventions can be carried out. Because DMD follows an X-linked inheritance pattern, female relatives of DMD patients are at risk of being carriers. To institute early interventions such as genetic counseling and prenatal diagnosis, a fast and cost-effective test that can accurately identify at-risk car- riers is crucial. In the past, increased serum creatine kinase was used to identify asymptomatic carriers (52 ). Under many circumstances, however, creatine kinase values may be within the reference interval in approximately 1⁄3 of female carriers. Therefore, carrier detection by DNA analysis is still the most accurate technique. To detect the DMD gene deletion/duplication in affected males and carriers in an efficient way, we devised an HDA capillary electrophoresis system for quantitative PCR-based assay. The strategy is based on quantitative multiplex PCR of the deleted/duplicated and undeleted/ unduplicated exons of the patient and the obligate carrier in the family. In patients with DMD, the deleted/ duplicated exons can be easily identified by direct visual inspection of the absence/increase of the corresponding peak. For carrier detection, the carrier status can be confirmed by calculating the alteration in the allele dose by use of the deleted/duplicated to undeleted/unduplicated exon ratio. In the present study, the value of the peak area for PCR amplification from each exon was divided by that of the reference exon, and the ratios of the unknown samples were compared with the control samples to determine the copy number of each exon. When the value of the copy number from the sample was higher than 1.5, the result was classified as unaffected. Con- Table 2. Various causes of PWS and comparison of results obtained with different diagnostic methods. Percentages 60%–70% 25%–30% ⬍5% ⬍5% Causes of PWS Deletion in paternally derived PWS region Maternal uniparental disomy 15 (UPD) Chromosome translocation breaking within the PWS critical region Imprinting defect with variation Multiplex PCR MLPA Methylation PCR FISH analysis Sequence analysis Yes No No Yes Yes No Yes Yes No Yes No Yes No No No No No No No Yes 2209 Clinical Chemistry 52, No. 12, 2006 versely, if the value was ⬍1.5, the result was classified as deleted carrier. No overlap was observed between the values obtained for single and double copy number. This novel multiplex quantitative PCR method for deletion or duplication analysis was easier and faster than traditional diagnostic approaches. In addition, the HDA system based on capillary electrophoresis was suitable for analyzing large numbers of samples and accommodated high sample throughput. Furthermore, the diluted crude PCR products are directly and automatically injected into the capillary channel without the need for further purification or denaturation. This is not a turn-key system, however, and users must be trained to accurately interpret the results. This analytic method can efficiently analyze 12 PCR products simultaneously in 10 min. For DMD diagnosis, the approximately $32 per patient cost of 2 different probe mixes of MLPA reagent sets is a significant decrease compared with preexisting techniques. The MLPA process requires the use of an expensive fluorescent-based sequencer/DNA analyzer such as an ABI 3730/ABI 3100, whereas the proposed process uses a much less expensive eGENE HDA capillary electrophoresis system. The cost of a single multiplex assay is about $2.50, and it costs approximately $20 per patient to perform 8 sets of multiplex PCR coupled with use of the HDA capillary electrophoresis system. Compared with quantification assay labeled with fluorescent dye, our method is a simple, inexpensive, and in-house protocol with a reliable quantification method well suited for measuring gene copy numbers. In conclusion, we report a powerful, rapid, and extremely reliable quantitative PCR assay and demonstrate its clinical application for the detection of deletion or duplication genotypes. This assay can be used for quantification of the SNRPN gene copy numbers in deletion/nondeletion types of PWS, as well as for identification of deletion/ duplication genotype in affected male and female carriers for diagnosis of DMD. This study showed that the sensitivity and specificity of this multiplex quantitative PCR coupled with HDA capillary electrophoresis analysis are consistent with those of conventional FISH and real-time PCR analysis. This attractive alternative method is a promising tool for the detection of disorders involving deletions and duplications, such as PWS, Angelman syndrome, and DiGeorge syndrome. We are very grateful to all the families who participated in this research. We acknowledge Dr. Su-Ming Hsu for English language editing and Dr. Fon-Jou Hsieh for expert assistance. This work was supported by the National Science Council of Taiwan (NSC 93-2314-B-002-174; NSC 94-3114-P-002-002-Y5). References 1. Lynch M. Genomics. Gene duplication and evolution. Science 2002;297:945–7. 2. Cassidy SB. Prader-Willi syndrome. Curr Probl Pediatr 1984;14:1– 55. 3. Buiting K, Gross S, Lich C, Gillessen-Kaesbach G, el-Maarri O, Horsthemke B. Epimutations in Prader-Willi and Angelman syndromes: a molecular study of 136 patients with an imprinting defect. Am J Hum Genet 2003;72:571–7. 4. Nicholls RD, Knepper JL. Genome organization, function, and imprinting in Prader-Willi and Angelman syndromes. Annu Rev Genomics Hum Genet 2001;2:153–75. 5. Cassidy SB. Prader-Willi syndrome. J Med Genet 1997;34:917– 23. 6. Mann MR, Bartolomei MS. Towards a molecular understanding of Prader-Willi and Angelman syndromes. Hum Mol Genet 1999;8: 1867–73. 7. Bittel DC, Butler MG. Prader-Willi syndrome: clinical genetics, cytogenetics and molecular biology. Expert Rev Mol Med 2005;7: 1–20. 8. Emery AE. Population frequencies of inherited neuromuscular diseases—a world survey. Neuromuscul Disord 1991;1:19 –29. 9. Bebchuk KG, Bulman DE, D’Souza VN, Worton RG, Ray PN. Genomic organization of exons 22 to 25 of the dystrophin gene. Hum Mol Genet 1993;2:593– 4. 10. Roberts RG, Coffey AJ, Bobrow M, Bentley DR. Exon structure of the human dystrophin gene. Genomics 1993;16:536 – 8. 11. Hu XY, Ray PN, Murphy EG, Thompson MW, Worton RG. Duplicational mutation at the Duchenne muscular dystrophy locus: its frequency, distribution, origin, and phenotypegenotype correlation. Am J Hum Genet 1990;46:682–95. 12. Muntoni F, Torelli S, Ferlini A. Dystrophin and mutations: one gene, several proteins, multiple phenotypes. Lancet Neurol 2003; 2:731– 40. 13. Prior TW, Bridgeman SJ. Experience and strategy for the molecular testing of Duchenne muscular dystrophy. J Mol Diagn 2005;7: 317–26. 14. Kuwano A, Mutirangura A, Dittrich B, Buiting K, Horsthemke B, Saitoh S, et al. Molecular dissection of the Prader-Willi/Angelman syndrome region (15q11–13) by YAC cloning and FISH analysis. Hum Mol Genet 1992;1:417–25. 15. Voskova-Goldman A, Peier A, Caskey CT, Richards CS, Shaffer LG. DMD-specific FISH probes are diagnostically useful in the detection of female carriers of DMD gene deletions. Neurology 1997; 48:1633– 8. 16. Gillessen-Kaesbach G, Robinson W, Lohmann D, Kaya-Westerloh S, Passarge E, Horsthemke B. Genotype-phenotype correlation in a series of 167 deletion and non-deletion patients with PraderWilli syndrome. Hum Genet 1995;96:638 – 43. 17. Patsalis PC, Kousoulidou L, Sismani C, Mannik K, Kurg A. MAPH: from gels to microarrays. Eur J Med Genet 2005;48:241–9. 18. White S, Kalf M, Liu Q, Villerius M, Engelsma D, Kriek M, et al. Comprehensive detection of genomic duplications and deletions in the DMD gene, by use of multiplex amplifiable probe hybridization. Am J Hum Genet 2002;71:365–74. 19. Gatta V, Scarciolla O, Gaspari AR, Palka C, De Angelis MV, Di Muzio A, et al. Identification of deletions and duplications of the DMD gene in affected males and carrier females by multiple ligation probe amplification (MLPA). Hum Genet 2005;117:92– 8. 20. Procter M, Chou LS, Tang W, Jama M, Mao R. Molecular diagnosis of Prader-Willi and Angelman syndromes by methylation-specific melting analysis and methylation-specific multiplex ligation-dependent probe amplification. Clin Chem 2006;52:1276 – 83. 2210 Hung et al.: Quantitative Assay of Deletion or Duplication Genotype 21. Shao H, Lip V, Wu BL. Effectiveness of multiplex ligation-dependent probe amplification assay used for detecting deletion of Prader-Willi syndrome. Beijing Da Xue Xue Bao 2005;37:64 –7. 22. Markoulatos P, Siafakas N, Moncany M. Multiplex polymerase chain reaction: a practical approach. J Clin Lab Anal 2002;16:47– 51. 23. Sanchez JL, Storch GA. Multiplex, quantitative, real-time PCR assay for cytomegalovirus and human DNA. J Clin Microbiol 2002;40:2381– 6. 24. Sellner LN, Taylor GR. MLPA and MAPH: new techniques for detection of gene deletions. Hum Mutat 2004;23:413–9. 25. Lehr HP, Reimann M, Brandenburg A, Sulz G, Klapproth H. Real-time detection of nucleic acid interactions by total internal reflection fluorescence. Anal Chem 2003;75:2414 –20. 26. Matsubara Y, Kerman K, Kobayashi M, Yamamura S, Morita Y, Takamura Y, et al. On-chip nanoliter-volume multiplex TaqMan polymerase chain reaction from a single copy based on counting fluorescence released microchambers. Anal Chem 2004;76: 6434 –9. 27. Haslett JN, Sanoudou D, Kho AT, Han M, Bennett RR, Kohane IS, et al. Gene expression profiling of Duchenne muscular dystrophy skeletal muscle. Neurogenetics 2003;4:163–71. 28. Hataoka Y, Zhang L, Mori Y, Tomita N, Notomi T, Baba Y. Analysis of specific gene by integration of isothermal amplification and electrophoresis on poly(methyl methacrylate) microchips. Anal Chem 2004;76:3689 –93. 29. Sanders JC, Breadmore MC, Kwok YC, Horsman KM, Landers JP. Hydroxypropyl cellulose as an adsorptive coating sieving matrix for DNA separations: artificial neural network optimization for microchip analysis. Anal Chem 2003;75:986 –94. 30. Tian H, Brody LC, Fan S, Huang Z, Landers JP. Capillary and microchip electrophoresis for rapid detection of known mutations by combining allele-specific DNA amplification with heteroduplex analysis. Clin Chem 2001;47:173– 85. 31. Landers JP. Molecular diagnostics on electrophoretic microchips. Anal Chem 2003;75:2919 –27. 32. Hung CC, Lee CN, Chen CP, Jong YJ, Chen CA, Cheng WF, et al. Quantification of relative gene dosage by single-base extension and high-performance liquid chromatography: application to the SMN1/SMN2 gene. Anal Chem 2005;77:6960 – 8. 33. Hung CC, Su YN, Lin CY, Yang CC, Lee WT, Chien SC, et al. Denaturing HPLC coupled with multiplex PCR for rapid detection of large deletions in Duchenne muscular dystrophy carriers. Clin Chem 2005;51:1252– 6. 34. Telatar M, Grody WW, Emmanouilides C. Detection of bcl-2/IgH rearrangements by quantitative-competitive PCR and capillary electrophoresis. Mol Diagn 2001;6:161– 8. 35. Zabzdyr JL, Lillard SJ. A qualitative look at multiplex gene expression of single cells using capillary electrophoresis. Electrophoresis 2005;26:137– 45. 36. Ng ES, Yang F, Kameyama A, Palcic MM, Hindsgaul O, Schriemer DC. High-throughput screening for enzyme inhibitors using frontal affinity chromatography with liquid chromatography and mass spectrometry. Anal Chem 2005;77:6125–33. 37. Bjorheim J, Ekstrom PO. Review of denaturant capillary electrophoresis in DNA variation analysis. Electrophoresis 2005;26: 2520 –30. 38. Issaq HJ, Chan KC. Separation and detection of amino acids and their enantiomers by capillary electrophoresis: a review. Electrophoresis 1995;16:467– 80. 39. Tian H, Brody LC, Mao D, Landers JP. Effective capillary electrophoresis-based heteroduplex analysis through optimization of surface coating and polymer networks. Anal Chem 2000;72: 5483–92. 40. Lorieau J, Shoemaker GK, Palcic MM. Quantitative nanopipettor for miniaturized chemical and biochemical reaction sampling. Anal Chem 2003;75:6351– 4. 41. Liu MS, Amirkhanian VD. DNA fragment analysis by an affordable multiple-channel capillary electrophoresis system. Electrophoresis 2003;24:93–5. 42. Beggs AH, Koenig M, Boyce FM, Kunkel LM. Detection of 98% of DMD/BMD gene deletions by polymerase chain reaction. Hum Genet 1990;86:45– 8. 43. Chamberlain JS, Gibbs RA, Ranier JE, Nguyen PN, Caskey CT. Deletion screening of the Duchenne muscular dystrophy locus via multiplex DNA amplification. Nucleic Acids Res 1988;16:11141– 56. 44. Bennett RR, den Dunnen J, O’Brien KF, Darras BT, Kunkel LM. Detection of mutations in the dystrophin gene via automated DHPLC screening and direct sequencing. BMC Genet 2001;2:17. 45. Cha RS, Thilly WG. Specificity, efficiency, and fidelity of PCR. PCR Methods Appl 1993;3:S18 –29. 46. Abbs S, Bobrow M. Analysis of quantitative PCR for the diagnosis of deletion and duplication carriers in the dystrophin gene. J Med Genet 1992;29:191– 6. 47. Lubin MB, Elashoff JD, Wang SJ, Rotter JI, Toyoda H. Precise gene dosage determination by polymerase chain reaction: theory, methodology, and statistical approach. Mol Cell Probes 1991;5: 307–17. 48. Joncourt F, Neuhaus B, Jostarndt-Foegen K, Kleinle S, Steiner B, Gallati S. Rapid identification of female carriers of DMD/BMD by quantitative real-time PCR. Hum Mutat 2004;23:385–91. 49. Ramakrishna N, Meeker C, Li S, Jenkins EC, Currie JR, Flory M, et al. Polymerase chain reaction method to identify Down syndrome model segmentally trisomic mice. Anal Biochem 2005;340: 213–9. 50. Lin CY, Su YN, Lee CN, Hung CC, Cheng WF, Lin WL, et al. A rapid and reliable detection system for the analysis of PMP22 gene dosage by MP/DHPLC assay. J Hum Genet 2006;51:227–35. 51. Su YN, Hung CC, Li H, Lee CN, Cheng WF, Tsao PN, et al. Quantitative analysis of SMN1 and SMN2 genes based on DHPLC: a highly efficient and reliable carrier-screening test. Hum Mutat 2005;25:460 –7. 52. Hood D, Van Lente F, Estes M. Serum enzyme alterations in chronic muscle disease. A biopsy-based diagnostic assessment. Am J Clin Pathol 1991;95:402–7.