Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Emotion perception wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Sleep paralysis wikipedia , lookup
Sleep medicine wikipedia , lookup
Lateralization of brain function wikipedia , lookup
Synaptic gating wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Human brain wikipedia , lookup
Aging brain wikipedia , lookup
Sleep and memory wikipedia , lookup
Rapid eye movement sleep wikipedia , lookup
Neuroplasticity wikipedia , lookup
Sensory substitution wikipedia , lookup
Emotional lateralization wikipedia , lookup
Nervous system network models wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Metastability in the brain wikipedia , lookup
Proprioception wikipedia , lookup
Effects of sleep deprivation on cognitive performance wikipedia , lookup
Start School Later movement wikipedia , lookup
Dual consciousness wikipedia , lookup
Brain Rules wikipedia , lookup
Sensory cue wikipedia , lookup
Neuroscience in space wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Non-24-hour sleep–wake disorder wikipedia , lookup
Neuroesthetics wikipedia , lookup
Neuroanatomy wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Embodied cognitive science wikipedia , lookup
Time perception wikipedia , lookup
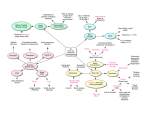
UNIT 3 PSYCHOLOGY Acknowledgements: Some information referred to in these course notes comes from the new Psychology textbook: VCE UNITS 3 & 4 by authors Grivas Down and Carter (1999) Macmillan, Victoria. Page references in the course notes indicate where information can be located in the textbook referred to above. 2 UNIT 3 SUMMARY BIOLOGICAL BASES OF BEHAVIOUR The Nervous System Nervous System Central NS brain spinal cord Peripheral NS Somatic NS Sympathetic NS Autonomic NS Parasympathetic NS What is the human nervous system made of? The neuron or nerve cell. Neurons are tiny individual cells, whereas nerves are large bundles of neuron fibres. Neurons are specialised to carry information from place-to-place and to integrate (bring together meaningfully) information from a variety of places in the nervous system. Information passes from neuron to neuron in the form of electrochemical impulses (or energy) – the language of the nervous system. There are three main types of neurons in the nervous system: Sensory or afferent neurons carry information from the sense organs to the CNS. Interneurons connect neurons with other neurons, and integrate the activities of sensory and motor neurons. They are found only in the CNS. Motor or efferent neurons carry away from the CNS to a targetted muscle, organ or gland in the body. The structure of a neuron Dendrites carry information (impulses) in from other neurons. The soma contains the cell nucleus and maintains the cell. Incoming information is collected and combined in the soma until sufficient to send a nerve impulse along the axon. The axon is a long thin fibre that carries information away from the soma toward other neurons. An axon terminal is the area where one neuron communicates with another. A synaptic knob (terminal button) is found on each axon terminal (and contains sacs called synaptic vesicles which hold special chemicals called neurotransmitters) Nerve impulses are electrochemical signals that transport information rapidly throughout the nervous system. A synapse is the tiny area or gap where neurons meet, without touching. 3 The cerebral cortex is only one part of the brain. Why study it in particular? Because the cerebral cortex is responsible for many of our higher-order information processing activities such as the ability to use language, think, plan and solve problems. Not surprising then, the cerebral cortex in humans is larger than in our pets like dogs and cats who have relatively small cortices – frogs and fish none at all. The brain is divided into 2 halves or hemispheres. The cerebral cortex is the convoluted outer covering of the two hemispheres. It is approx. 2mm thick. Each hemisphere contains 4 lobes: FRONTAL TEMPORAL OCCIPITAL PARIETAL We have come to understand its working through studies with intact brains (using localised sedation, EEG, MRI, PET, CAT scan) and people with split brains and brain damage. Frontal lobes contains the primary motor cortex responsible for initiating movement. also associated with the way we express our personalities - see (Phineas Gage p50) contains Broca’s area which involves production of clear and fluent speech (once again usually left hemisphere only). Broca’s aphasia is characterised by impaired production of language and speech sounds. Person speaks meaningfully but without fluency. Temporal lobes contain the primary auditory cortex (like specialised areas in the motor and somatosensory cortex it has particular areas which respond to sounds of different frequencies – guitar note received in different place than recorder.) are also important in memory – especially our ability to remember faces. also responsible for holding memories of our personal experiences like birthdays, holidays, accidents etc. contains Wernicke’s area (but in the left hemisphere only) which is important in interpreting and understanding sound – especially of spoken language – also important for locating the right word in memory to express ourselves clearly when we speak or write. Wernicke’s aphasia is the term given to patients with damage to the area causing them to string together a fluent series of words which are largely meaningless. Comprehension of speech is affected as well. Occipital lobes contains the primary visual cortex, the final destination of information from receptors (sensory neurons) in the eyes. secondary and association areas of the visual cortex merge with association areas of the parietal and temporal lobes. Parietal lobes contains the primary somatosensory cortex which receives and understands messages from receptor neurons in skin about touch, pressure, temperature, pain and muscle movement and information about the position of the body in space. monitors our position about head and body positions, and transfers the information to areas controlling movement. neglect syndrome results from (usually) damage to the right parietal lobe (so that subjects "neglect" the left side of their world). Note: There are also association areas in each cortical lobe. They enable higher-order brain functions like speech, and the ability to make decisions and solve problems because they bring together information from the primary cortical areas and other relevant areas of the brain. EVEN SIMPLE BEHAVIOURS REQUIRE INTERACTION BETWEEN CORTICAL LOBES. 4 Hemispheric specialisation It is important to note that sensory (or motor) pathways between the CNS and PNS are contralaterally organised, that is, movement (or sensation) on the right side of the body occurs in response (or is received in) the relevant area of the left hemisphere, and visa-versa. The corpus callosum …is the main bridge linking both hemispheres. It consists of a large number of axon fibres allowing left and right hemispheres to communicate by sharing information. Damage to the corpus callosum has taught us much about what each hemisphere is specialised for. In addition to this we have gained information on hemispheric specialisation through research on people with intact brains and those with brain damage (injury, surgery, disease). What happens when the corpus callosum is severed? In order to relieve symptoms of severe epilepsy, Roger Sperry severed the corpus callosum of some patients, effectively allowing him to isolate the functions of both hemispheres and study them. Referred to as split-brain surgery, the procedure allowed Sperry to test both hemispheres separately because information processed in the right visual field is processed in the left hemisphere, and information processed in the left visual field is processed in the right hemisphere. When Sperry presented words very briefly to patient’s right visual fields and asked them to describe what they saw, they could. But, if it was presented to their left visual fields instead, patients were unable to name or describe the object. But, by using the left hand the same patients could select the object out from others hidden behind a screen with the left-hand (controlled by the right hemisphere). So, even though visual information reaching the right hemisphere was seen and understood, it could not be verbalised because the information in the r/h could not cross the corpus callosum to the left hemisphere, which does have the ability to use language, and therefore name and describe the object. How are the cognitive and behavioural functions of the left and right cerebral hemispheres different? Left hemisphere VERBAL/ANALYTICAL lANGUAGE-reading -writing -speech ANALYSIS-calculation -time-sense -rhythm MOVEMENT/SENSATION in Right body Right hemisphere NON-VERBAL SPATIAL-puzzles -recognising faces, patterns, melodies CREATIVITY-visualisation -fantasy -recognition, expression of emotion MOVEMENT/SENSATION in Left body The Spinal Cord This structure begins from the base of the brain, and continues down the spine to the lower back. It is made of tracts (a thick bunch of nerves), which allow two-way communication. The main functions of the spinal cord: To carry sensory information from the PNS to the brain To carry motor information from the brain to muscles, organs and glands in the PNS Note: a third and most important function of the spinal cord is a spinal reflex which is an automatic and adaptive response occurring when an interneuron inside the spinal cord allows a connection between a sensory and motor neuron independently of the brain. Eg., After stepping on a thorn a sensory neuron connects with an interneuron inside the spinal cord which in its turn activates a motor neuron which releases neurotransmitter chemicals into effector cells in foot muscles, causing the foot to contract. 5 Note: When the spinal cord is severed the somatic nervous system (enabling voluntary movement) is prevented from passing messages to the CNS. Nerves damaged in the spinal cord don’t recover, with a person losing voluntary movement below the point of the severed area permanently. Paraplegics lose voluntary muscle movement in the legs – though reflexes in their legs still function. It happens when the spinal cord is severed above where spinal nerves project to the legs. Quadriplegics lose movement in both legs and arms as the spinal cord is cut above the spinal nerves controlling both arms and legs. The role of the somatic nervous system in the control of skeletal muscles (also called skeletal nervous system) The main functions of the somatic nervous system involve: carrying information via a network of neurons extending from the sensory receptors to the CNS. the control of voluntary movement associated with skeletal muscles. there are two types of muscles in our bodies: skeletal muscles (or striated/striped) and smooth muscles. The somatic nervous system is involved in the control of skeletal muscles, most of which connect to bones in our bodies. (Note: in contrast to the somatic nervous system, the ANS controls the function of most smooth body muscles.) because the somatic nervous system controls these skeletal muscles, it controls movement of obvious and less obvious kinds, ranging from moving legs in order to walk, to altering facial expression, eye movements and speech. remember: skeletal muscles are inactive unless they receive messages from motor neurons. nerves in the somatic nervous system do not activate non-skeletal muscles such as the stomach, intestines and heart. The Autonomic Nervous System The autonomic nervous system involves the network of neurons connecting the CNS with the internal muscles, organs and glands of the body (p79). Autonomous, independent and automatic, the ANS functions independently of the brain to keep vital organs in our bodies functioning (heart, stomach, kidneys, liver, sweat glands etc.). Whether we are awake or asleep, alert or comatose, the ANS modifies the activity of visceral (smooth) muscles, organs and glands. The ANS is different from the somatic nervous system because the somatic nervous system initiates or causes movement or change (in skeletal muscles), whereas the ANS modifies and changes the activities of muscles, organs and glands to meet whatever demands face the body at the time. While most changes in the body caused by the ANS are not under our conscious control, some can be controlled sometimes. Furthermore, a technique called biofeedback (meaning feedback provided by a particular device on some biological function in the body) is learned by some people, with some success, to control blood pressure, asthma, migraine headaches and other physiological responses causing illness. The ANS is divided into two further divisions: the sympathetic and parasympathetic divisions of the ANS. Most visceral (smooth) muscles, organs and glands receive messages from two different sets of neurons which produce quite opposite effects, that is, some pathways in the ANS speed up the heart beat, for example, while others have the opposite reaction and slow it down. So both systems act on the same targets throughout the body (blood vessels, sweat glands, stomach etc.) but with opposing effects on them. The sympathetic branch of the ANS prepares the body for emergency action in a threatening situation or one requiring vigorous physical activity by arousing some bodily systems and inhibiting others in ways that increase our chances of surviving the emergency. Sugar is released for energy, the heart beats faster, we breathe faster, digestion is temporarily inhibited etc. (p85) The parasympathetic division of the ANS generally reverses arousal, calming and relaxing the body. It restores homeostasis (a balanced body state). Heartbeat is slowed, pupils return to normal size, blood pressure drops, and so forth. This division of the ANS helps build up and conserve energy, and is usually dominant. The parasympathetic system also reacts more slowly than the sympathetic division, taking 20 to 30 minutes for the effects to disappear (thought to be due to the hormone adrenalin which remains in the bloodstream for some time after.) 6 Sudden death can occur when the parasympathetic branch of the ANS overreacts by slowing physiological functions too much, bringing them to a halt - termed parasympathetic rebound. So in brief, in our emergency situation the somatic system controls muscles necessary for running away and waving to others for help. The sympathetic branch of the ANS raises blood pressure, quickens our heartbeat and breathing rate, and makes us sweat. It marshals internal body systems and processes in ways that help our bodies to deal with the emergency. When the danger has passed the parasympathetic division of the ANS restores balance (homeostasis) once again. Fight-flight response The fight-flight response is an automatic and adaptive response of the body caused by activation of the sympathetic branch of the ANS. It leads to a state of physiological arousal mobilising the body to deal with the threat by confrontation (fight) or flight. Note: It’s best to think of the fight-flight response in relation to the body’s reaction to short-term stressors. General Adaptation Syndrome The GAS consists of three stages: the alarm stage, the resistance stage and exhaustion stage. The alarm stage occurs in two phases after we first notice the emergency (yes, that’s definitely a shark behind us in the water!) (i In the shock phase of the alarm stage the ability of our body to deal with this stressor drops below its normal level. We might barely be able to support ourselves and go limp at the knees. Suffering from the shock of the situation, our blood pressure drops, body tempertaure drops, and muscle tone is lost. ii In the countershock stage the sympathetic division of the ANS is activated, and the body’s ability to resist/cope and grapple with the stressor increases (instead of sinking beneath the waves we’ll make a run/swim for it, and probably make record time…..for a while at least). This happens because the pituitary gland release hormones which make the adrenal glands increase production and release of the hormones adrenalin and noradrenalin.) In the resistance stage we have more resistance to/and ability to handle the original stressor, but our ability to ward off and cope with new stressors, decreases. In other words by this stage we are vulnerable to a host of other stressors, of either a physical or psychological nature. If the stress continues we may reach the exhaustion stage. This is extreme. The body's resources are exhausted, and stress hormones depleted. Unless relieved it can result in a psychosomatic disease, loss of health etc. This stress can also interrupt the body's immune system. (Note: it’s best to distinguish GAS (at least all three stages of the syndrome) from the fight-flight response as a reaction to longer-term, prolonged stress. Of course activation of the sympathetic division of the ANS is involved in both reactions, which are not mutually exclusive.) Arousal and Stress The term arousal is a reference to the overall state of alertness and activation of the individual. (p85) Stress occurs anytime we must adjust or adapt to the environment. Ordinary life is filled with never-ending adjustments we need to make. Even happy events like births, marriages, throwing a party and falling in love cause stress. Some events are more likely to act as stressors (things which cause us stress) than others eg. unpredictable work and pressure (work sped up, bigger workload unexpectedly). In general, people feel more stress in situations over which they have little or no control, or don’t have the skills to cope with the demands they are facing. Where emotional shocks are intense or repeated, unpredictable, uncontrollable and linked to pressure, stress is magnified and damage is likely to result. (p101) Appraising Stressors. Stress depends on how we perceive a situation. Thus, changing our thoughts and attitudes to stressors can sometimes help us cope with them. Psychosomatic illnesses (including some forms of heart disease, stomach ulcers, migraines, asthma and endless others illnesses) are not imagined (unlike hypochondria). At least in part they can be caused by or exacerbated by stress. Whilst there is no cause and effect, there is a strong correlation between stress and physical illness. 7 The polygraph (literally many graphs - usually 4 measures) It is misnamed when sometimes mistakenly referred to as a "lie-detector". It usually measures changes in heart rate, blood pressure, breathing rate, and the galvanic skin response (GSR is a measure of the electrical conductivity of the skin). However, it is important to note that it actually measures the general level of arousal. It can't tell the difference between lying, fear, guilt or excitement or numerous other emotions which may appear similar in terms of physiological reactions. Even when done properly, the polygraph may be inaccurate. Those who think: exciting thoughts upsetting thoughts use self-inflicted pain tranquilising drugs and people who lie without anxiety can fool the test. It can also cause an innocent man to be labelled as a guilty one, if sufficiently aroused by the situation. It is important to note the difference between baseline or control questions and relevant questions when the polygraph is administered (p89) VISUAL PERCEPTION To feel, smell, see, hear or know we are leaning over or standing in an upright position involves both sensory and perceptual activity. We have 7 different perceptual systems (including the kinesthetic and vestibular systems). The perceptual system studied in detail in VCE Psychology is the visual perception system which is defined as the complete network of physiological structures involved in vision: the eyes, photoreceptors, optic or neural pathway and visual cortex. We are surrounded by external physical energy sources. Generally receptor neurons (sensory neurons) only respond to one type of physical energy - the ears respond to mechanical energy in the form of sound waves; smell to chemical energy; and in vision the rods and cones (collectively called photoreceptors) respond to electromagnetic radiation or light energy. Finding meaning in external stimuli involves two interactive and interdependent types of processing: visual sensation and visual perception. It is important to note the differences between both types of processing, though in reality they are impossible to separate, given they are both critical parts of the whole visual system. Comparison of differences between visual sensation and perception Visual Sensation …is passive because it involves only neurological (neuron-based) detection and processing of light energy by the photoreceptors …the stimulus has no meaning …visual sensation from the same stimuli will not usually vary (except for those with damage to eye, optic pathway, or areas of the visual cortex) Visual Perception … is active because it involves brain-based processing of information …the stimulus is given meaning (in the final stage referred to as interpretation) …visual perception can vary because it uses mental processes, and is guided by our past experience, and motivational and emotional states at the time. Sometimes one person interprets the same sensory information in different ways, and sometimes people have a different perception of a stimulus at the same time. 8 The interactive processes in visual sensation and perception collectively involve six continuous and sequential stages of processing: sensation: reception ............................................................................................................................... transduction ............................................................................................................................... transmission ............................................................................................................................... perception: selection ............................................................................................................................... organisation ............................................................................................................................... interpretation ............................................................................................................................... Thresholds (p117) The absolute threshold is minimum stimulus intensity needed for detection of the presence of that stimulus, at least 50% of the time (with no other stimulus present). The differential threshold (or just noticeable difference) measures how much an already detectable stimulus must change in intensity before the difference can be detected, at least 50% of the time. Weber's Law states the amount of change needed to produce a just difference noticeable is a constant proportion of the original stimulus intensity. The process of sight The path of light moves: through cornea, through pupil (surrounded by iris), through lens, through vitreous humour, to retina (containing the photoreceptors: rods and cones), to optic nerve (which crosses at the optic chiasm) , to final destination in the occipital lobes of the cerebral cortex. The role of parts of the eye The CORNEA is a transparent convex shaped covering which protects the eye, and focuses the light onto the retina at back of the eye. The IRIS is the coloured ring of muscle that expands or contracts to alter the size of the pupil, thereby determining how much light will enter the eye. The PUPIL is the opening that admits light to the eye. It dilates or contracts as necessary. The LENS is the major focussing mechanism of the eye. the ciliary muscles adjust its shape when the viewing distance changes: elongating to focus on distant objects, and bulging to focus on objects nearby. At the RETINA the rods and cones receive and absorb light, and process it for transmission as neural messages (in the form of electrochemical energy) to the visual cortex for further processing, and the final stage of perception, interpretation.(p124) Diagram of the Eye 9 Rods and Cones RODS CONES Do not provide clear detail in the object viewed – low visual acuity Function best in dim light, and 500 times more sensitive to light than cones Found mainly in the periphery of the retina (none in fovea) Adapt to the dark relatively slowly (maximum sensitivity occurring after 30 mins) Only 1 type of rod receptor – rods respond best to blue light, but report only on level of brightness not colour, and are unresponsive to red light). Give clear, sharp, definition of object viewed – high visual acuity Only operate in brighter light conditions Found mainly in the centre of the retina (fovea is area which provides best visual acuity) Adapt to the dark quickly (maximum sensitivity gained after 7-8 mins) 3 different types of cones – they provide information by responding to short (blue), medium (green), or long wavelengths of light, (red). Dark Adaptation The term dark adaptation is used to refer to the changes that take place as the photoreceptors in the eyes adjust to light of lower levels of intensity. It happens when the eyes move to rod vision. Maximum sensitivity is reached between 30-45 minutes for the rods. Dark adaptation allows us to see in light conditions too weak to stimulate the less sensitive cones. Note: Therefore the threshold for rods is much lower than it is for cones. Organisation of Visual Sensations into Visual Perceptions The principles of visual perception fall into three main categories: the constancies, the depth principles (or cues), and the Gestalt grouping principles. PERCEPTUAL CONSTANCIES Size constancy - perceived size of an object remains the same even though size of image cast on the retina changes. Shape constancy – perceived shape of an object is unaltered by changes in the shape of its retinal image. Brightness constancy - perceived brightness level of an object stays the same under changing conditions of light. The exception is where objects emit their own light eg. a fire, light on the alarm clock etc. Orientation constancy – the perceived orientation of objects remains stable even though the retinal image may be of a different level of orientation. (p157) The Gestalt Grouping Principles There are a numerous Gestalt grouping principles. The following four are specified in the study design for psychology. Figure-ground organisation; where we distinguish “figure” from ground (background) Nearness or Proximity; where stimuli that are near each other tend to be grouped together, different to stimuli further away Similarity; where stimuli, similar in size, shape, colour or texture tend to be grouped together. Closure; our strong tendency to mentally complete an incomplete figure so it is perceived as a meaningful form (p135) 10 Depth Perception Internal primary cues Monocular depth cues accommodation External secondary cues interposition linear perspective texture gradient relative size height in the visual field Binocular depth cues retinal disparity convergence Depth perception is the ability to see three-dimensional space and accurately judge distance. Visual cliff provides evidence that depth perception is partly learned and partly innate (~ 4 months in humans) Adults perceive depth cues which can be monocular cues (one eye) and binocular (only operate when two eyes are used) Primary (muscular) cues (from within eye or body) accommodation (monocular cue) involves the focusing of the lens and is usually effective for distances less than 4 ft. The ciliary muscles holding the lens inform the brain and distance is assessed. convergence (binocular cue) occurs where depth is assessed when the eyes converge. Again muscular movements inform brain of distance/depth. retinal disparity (binocular cue) occurs when the eyes, which are 6-7cm apart present separate images of the world to the brain which merges them into a three dimensional perception. Greater disparity occurs at closer ranges. Secondary (pictorial) Depth cues (all monocular) relative size: more distant object is smaller. overlap or interposition: one object partially blocks another- obscured object perceived as more distant. texture gradient: changes in texture - the closer they are (finer texture), the further away. linear perspective: apparent convergence of parallel lines...a cue to distance. height in the visual field: objects closer to the horizon are perceived as further away. FACTORS THAT AFFECT PERCEPTION Psychological Factors Bottom-Up processing: analyses information starting with small units and builds upward. Top-Down processing: uses pre-existing knowledge to rapidly organise features into a meaningful visual stimulus. Perception is also affected by attention, prior experience, cultural factors, the suggestions of others, motives, emotions and many other more personalised factors which combine to form expectancy or perceptual set. These factors can operate over the short and longer term so they may not affect our visual perception the same way each time. Context can have a tremendous impact on our interpretation of a stimulus. For example, think about the figure 13. In a maths class, it will probably be perceived as a number, but on a packet of Rice 13iscuits it might be perceived differently. Physiological Factors Alcohol is a depressant and slows functioning in the body. It can affect perception because processing in the brain takes longer. This means the response to visual information is slower. The TAC has made 11 this point effectively in some advertisements where drivers who take longer to respond injure themselves or others. Alcohol can affect visual perception: the pupils dilate allowing too much light into the eye; perception of colour and distance is affected; vision narrows significantly so the driver is less able to utilise peripheral vision; and night vision is poorer. A condition termed Lazy Eye or Amblyopia develops due to excessive drinking over long time periods, where there is failure for one eye or both to line up with the visual object. In old age it is relatively normal for people to experience some changes or problems with their vision. Night vision, colour perception and recovering from glare at night are common problems. It becomes noticeably difficult to read small print, the words are hard to distinguish and blurred. The lens also loses its ability to focus readily, so viewing objects at various distances becomes difficult. Age-related Macular Degeneration is a disease causing damage to the cones situated in the fovea at the retina. (p171) Diabetes affects many parts of the body. It affects the eyes by reducing nourishment of the retina, due to weakening/swelling of blood vessels, causing diabetic retinopathy or overgrowth of blood vessels on the retinal surface, causing proliferative retinopathy. (p174) FALLIBILITY OF PERCEPTION An illusion occurs when we form a mistaken perception of a sensory stimulus. There are numerous visual illusions. The Moon illusion occurs in the natural world, and others such as the Ames illusion are created deliberately to fool us. The Moon Illusion: the apparent distance of the moon is greater when it is near the horizon than when it is overhead, because of size-distance cues making horizon seem further away. (p184) Muller-Lyer Illusion: experience with straight lines makes us see the arrow-headed line as shorter (and closer) than the line with inverted arrowheads (which appears further away). (p179) Ponzo Illusion (p182) Ames’ Room (p183) STATES OF CONSCIOUSNESS CONSCIOUSNESS Consciousness consists of all the thoughts, sensations, perceptions, memories and feelings that we are aware of at a given instant. William James described it by using the metaphor of a flowing stream that is continuous and ever-changing. CHARACTERISTICS OF NORMAL WAKING CONSCIOUSNESS We spend the most time in waking consciousness, which is organised, clear, meaningful and perceived as our reality, with a familiar sense of time and place. It is probably located in the cortex (frontal lobe), and also other areas throughout the brain. Controlled processes involve information processing, utilising mental alertness, awareness and focussed attention. Automatic processes require less concentration and therefore a lower level of consciousness. Attention involves focussing on certain stimuli and ignoring others. Attention may be selective- narrowlyfocussed awareness, or divided- distributed awareness to deal with several stimuli simultaneously. Daydreaming results when attention shifts voluntarily from external stimuli to internal events, thoughts and feelings. May occur when external stimulation is minimal. Purpose? Planning, problem-solving, creativity. Memory is utilised in normal waking consciousness, actively storing and retrieving information. 12 Content and time limitations operate in normal waking consciousness, so that its content is limited, organised and logical. ALTERED STATES OF CONSCIOUSNESS (ASC) An altered state of consciousness is defined as a distinct change in the quality and pattern of mental activity. There are shifts in perceptions, emotions, memory, time-sense, thinking, feelings of self-control and suggestibility. Altered states of consciousness can be caused by sensory overload, monotonous stimulation, unusual physical conditions, sensory deprivation, meditation and hypnosis. Some ASCs occur naturally eg. sleep and dreaming; and others are deliberately induced eg. meditation and hypnosis. An altered state of consciousness may be characterised by: self control changes - normal inhibitions may be lost, and people may be more open to loss of sense of self – not knowing where a person ends and external environment begins people become either more or less sensitive to external stimuli sense of time is disturbed – perceived as either slower or faster people tend to structure and analyse their thoughts less than usual emotional feelings change – with people being either more or less, or inappropriately emotional Unconscious people are totally unresponsive to the outside world, and their brains show almost zero electric activity. States of consciousness related to fatigue, delirium, hypnosis, drugs and ecstasy differ markedly from “normal” awareness. All people experience altered states such as sleep, dreaming and daydreaming. The measurement of certain physiological responses can indicate different states of consciousness: electrical activity of the brain heart rate body temperature galvanic skin response (GSR), (but physiological patterns of activity (alone) may be inconclusive in detecting whether a person is experiencing an ASC eg. daydreaming, meditation and hypnosis may appear similar physiologically.) A Description of Pain as an Altered State of Consciousness It is important to note that pain can occur in normal waking consciousness as well as during ASCs. Pain: an unpleasant sensory and emotional experience associated with tissue damage. (p205) It serves an adaptive function It isn’t triggered by a single stimulus like vision is, for example. It varies, and can be experienced at different levels. Note: psychological factors like one’s culture, motivation, and personality play a role in the way people experience pain. Meditation attempts to alter one’s state of consciousness/awareness by deeply relaxing both the mind and body. It involves focusing (concentrating) on one thing to the exclusion of everything else. Awareness of internal and external stimuli falls (so that awareness of pain may be decreased). It has not been reported as universally effective in pain management, though it is often used and recommended for use in palliative care. Hypnosis is a technique employed to induce an ASC where a person feels deeply relaxed, is in a sleep-like state and open to suggestion. (p207) (Both meditation and hypnosis have been used with varying levels of success to treat pain e.g. dentists may use hypnosis for patients as an alternative to anaesthetics; for childbirth and burns patients. Perhaps the selective attention involved (that is, the focus of attention is on another specific point, and not the pain) in both hypnosis and meditation explains why these ASCs bring some people relief from pain.) 13 SLEEP Webb (1975) considers sleep an innate biological rhythm, which can be delayed, but not ignored. A microsleep is a brief shift in brain activity (whilst seemingly awake) to patterns normally recorded in sleep. Sleep Deprivation: the effects vary according to age and personality. After 2-3 days: little impairment on complex tasks, but a decline in ability to concentrate, remain vigilant and follow simple routine. Hence low-level, boring, self-motivated tasks suffer. Great sleep loss: can cause sleep-deprivation psychosis, suffering hallucinations, delusions, and disorientation. Rhythms of sleep are so steady that they continue for many days even with external cues removed. However, the normal 24-hr cycle (night and day cues) will eventually shift to a natural 25-hour cycle with the absence of time cues. The hypothalamus, reticular formation and a "sleep centre" in the brainstem actively produce sleep. During sleep, the brain changes its pattern of activity, not the amount. Changes in sleep patterns can be measured using an electroencephalograph (EEG). Eye movements are measured using electrooculograph, and muscle tension with an electromyograph. In addition special sleep laboratories are attached to hospitals so people suffering from a variety of sleep disorders and can be studied and helped. A polygraph is often used in sleep laboratories. It may measure for example, heart beat, brainwave activity, body temperature, or eye movements etc. BRAIN WAVE PATTERNS When awake - small, fast beta waves Just before sleep (very relaxed)- larger, slower waves called alpha waves. Hypnagogic images - occur just before you fall asleep. May be vivid and surprising, but rarely mistaken for real objects. Linked to increase in theta waves. STAGE 1 -enter light sleep and heart rate slows, breathing irregular, and muscles relax. Hypnic jerk is a reflex muscle contraction. Muscle spasms in the leg may also occur - called myoclonus. This stage contains small amplitude, high frequency irregular waves called theta waves, with some alpha waves. Persons woken in this stage may or may not feel they have been sleeping. STAGE 2 -sleep deepens and short bursts of activity called sleep spindles begin to occur with a lowering of body temperature. Sleep spindles mark the boundary of sleep with the majority of people reporting that they were asleep when woken in this stage. STAGE 3 -a new large and slow brain wave called delta, begin to appear with deeper sleep. STAGE 4 -deep sleep. Brain waves almost pure delta. After spending time in stage 4, the sleeper travels back through the stages to stage 1. REM & NREM REM is dream sleep. NREM (stages 2,3,4) are dream free 90% of the time. Dreams reported in REM sleep are more defined, longer and clearer. The first period of stage 1 sleep is “REM- and dream-free”. REM sleep is a time of high emotion; the heartbeat is irregular and breathing variable. However during REM sleep the body becomes atonic to prevent acting out the dreams. NREM sleep helps us recover from fatigue and is increased after exercise or physical exertion. REM sleep increases with more daytime stress and with increased learning. WHY DO WE SLEEP? Restorative Theory suggests sleep functions to promote growth and maintenance of the body. Stage 4 promotes growth and repair; REM sleep promotes brain growth and repair and memory maintenance and consolidation. 14 Survival Theory of sleep developed because our ancestors were more likely to survive if hidden (from predators) and inactive at night. Sleep is not essential, but simply wastes time and conserves energy. REM sleep paralysis prevents “straying”. Problems with survival theories: we are more vulnerable when sleeping. Sleep disorders Narcolepsy –victims have sudden, irresistible sleep attacks. It often occurs with cataplexy (temporary paralysis of muscles) as victim falls directly into REM sleep. Insomnia -trouble getting to sleep, frequent night-time waking, waking too early, poor quality sleep etc. Insomnia can be temporary or chronic (over 3 weeks). Hypersomnia involves excessive sleepiness, or sleep for excessive periods of time– sometimes caused by insomnia. Sleep Apnea -breathing stops for 20sec-2min, and sleeper wakes, gulps air and then goes back to sleep. (p235) Sleep phenomena Nightmares -simply bad dreams, during REM sleep. They are brief, but remembered. daytime anxieties. Night Terrors (stage 4) -total panic, may hallucinate dream images, may wake in sweat, unusual to remember terror. Body not immobilised, so may sit up and scream. Sleepwalking -occurs in NREM 3 and 4. Sleeptalking- also usually during Stages 3 and 4 NREM. Little connection to Types of dreams Daydreaming occurs when the focus of our attention is shifted from external events to internal thoughts and feelings. More likely to occur when we are still or alone, waiting to sleep, travelling or feeling bored. Different from night dreams because there is little eye movement and high levels of alpha brain waves. The content is jumbled, and even less organised than many night dreams. Believed by some to have definite functions. Perhaps they allow us to solve problems; rehearse and explore alternative ways of doing things; and help us to stay ‘alert’ when stimulation is low. (p245) Nightdreams occur mostly during periods of REM sleep. We usually dream about 2 hours per night, spending increasing time in REM sleep as the night progresses. Exactly why we need REM sleep is unclear, though people deprived of it experience REM rebound when their sleep isn’t disturbed. (p242) Lucid dreaming - LA BERGE -dreamer wakes within dream and can consciously direct it. They know they are dreaming, but still think and act within dream. People can learn to be lucid dreamers.