Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lateralization of brain function wikipedia , lookup
Neural engineering wikipedia , lookup
National Institute of Neurological Disorders and Stroke wikipedia , lookup
Neurolinguistics wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
History of anthropometry wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Neurogenomics wikipedia , lookup
Neurophilosophy wikipedia , lookup
Behavioral epigenetics wikipedia , lookup
Causes of transsexuality wikipedia , lookup
Selfish brain theory wikipedia , lookup
Neuroscience and intelligence wikipedia , lookup
Human brain wikipedia , lookup
History of neuroimaging wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Cortical cooling wikipedia , lookup
Haemodynamic response wikipedia , lookup
Biology of depression wikipedia , lookup
Neuroeconomics wikipedia , lookup
Metastability in the brain wikipedia , lookup
Intracranial pressure wikipedia , lookup
Neuropsychology wikipedia , lookup
Impact of health on intelligence wikipedia , lookup
Sports-related traumatic brain injury wikipedia , lookup
Neuroanatomy wikipedia , lookup
Neuroplasticity wikipedia , lookup
Brain morphometry wikipedia , lookup
The Effect of Ischemia on Biogenic Amine
Concentrations in the Central Nervous System
JUSTIN A. ZIVIN, M.D.,
P H . D . , AND JOAN STASHAK,
M.S.
SUMMARY A rabbit spinal cord ischemia model was used to study the effects of focal ischemia on the
tissue concentrations of serotonin, 5-hydroxyindole acetic acid, and norepinephrine. Ischemia induced by
abdominal aorta occlusion caused both serotonin and norepinephrine concentrations to decline in the most
ischemic areas of the spinal cord by 55 minutes. In marginally perfused adjacent areas, serotonin concentrations transiently declined at 14 and 20 min. after the onset of ischemia and then returned to normal. The
minimum was reached at the same time when previous studies showed damage had become irreversible in
more ischemic regions. Concentrations of 5-hydroxyindole acetic acid did not change at any time and
norepinephrine declined only in the most ischemic areas after damage was irreversible. Thus, permanent
serotonin and norepinephrine decreases occur only in areas destined to be destroyed by infarction, but the
serotonin returns to normal in marginal tissue that remains viable. These studies suggest that serotonin
may be involved in the early stages of irreversible changes during central nervous system ischemia.
Stroke, Vol 14, No 4, 1983
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
DURING CENTRAL NERVOUS SYSTEM ISCHEMIA, there is abrupt loss of neurological function.
Since function can be severely compromised while
morphological changes are not immediately apparent,
some physical or biochemical phenomenon must be
responsible for the dysfunction. Because biogenic
amines are both neurotransmitters and have potent vasoactive properties, for many years there has been considerable speculation about their influences on the development of injury to the CNS. 1 Many experimental
stroke models exist,2"4 and many studies have been
conducted in which biogenic amine concentrations
have been measured during and after CNS ischemia.
When focal CNS ischemia has been investigated by
such methods, the results are subject to criticism because the distribution of damage is not reliably reproducible in any of the currently known cerebral stroke
models. Since the brain is so complex morphologically
and neurotransmitter concentrations differ substantially from region to region, comparatively small differences in lesion distribution might produce major
differences in the results of biochemical studies.
Furthermore, as no gross morphological marker is evident at the early time periods (when the damage is not
yet irreversible), sampling from larger areas of brain
may include normal or partially ischemic tissue. Consequently, the biochemical measurements may represent an average value from tissues in which very diverse changes are occurring.
To overcome many of these deficits, a rabbit model
of spinal cord infarction has been developed.5 The
prime advantages of this model for biochemical purposes are that the lesion is highly reproducible in its
distribution and the anatomy of the spinal cord is considerably simpler than that of the brain. Both features
facilitate analysis of the results of such studies.6 Serotonin (5HT) and norepinephrine (NE) are present in
substantial concentrations in spinal cord7 (dopamine
From the Department of Neurology, University of Massachusetts
Medical Center, Worcester, Massachusetts.
Address correspondence to: Justin A. Zivin, M.D., Ph.D., Department of Neurology, University of Massachusetts Medical Center, 55
Lake Avenue North, Worcester, Massachusetts 01605.
Received May 28, 1982; revision accepted January 20, 1983.
and epinephrine are nearly absent). Therefore, it
seemed reasonable to investigate the changes that occur in 5HT and NE as a function of the duration of CNS
ischemia. In turn, if it could be demonstrated that
changes in these biogenic amines are correlated with at
least some aspects of CNS infarction, and since many
drugs are known to alter the actions and concentrations
of these biogenic amines, then it might be possible to
develop rational pharmacological strategies to ameliorate the damage produced by CNS ischemia.
Materials and Methods
Forty male New Zealand albino rabbits weighing 2
to 3 kg were fed rabbit chow and water ad lib until the
time of surgery. As described in detail previously,6 a
snare ligature was placed around the abdominal aorta
of each rabbit just caudal to the more caudal renal
artery and the free end of the snare was accessible
outside the rabbit. The animals were allowed to recover from surgery to confirm that motor and sensory
functions were normal. The snare ligature was then
pulled tight to occlude the aorta. Although the animals
were fully conscious, none evidenced any discomfort
when the aorta was so occluded. Complete paraplegia
and anesthesia in the hind quarters ensued in all rabbits
within 2 min of the onset of occlusion.
Previous studies6 indicated that in the rabbit spinal
cord ischemia model irreversible neurological damage
begins at approximately 9 min of ischemia, causes
irreversible damage in half of the animals at 20 min,
produces complete irreversible paraplegia at 33 min in
half the animals, and causes complete paraplegia in
essentially all rabbits by 55 min. Therefore, biochemical studies were performed at 5 min of ischemia to
determine if any neurochemical changes occurred before permanent damage was present and at 14, 20, 33
and 55 minutes to span the time periods of interest as
the clinical damage became progressively more irreversible. At these predetermined times the rabbits received an intravenous bolus of 100 mg of pentobarbital
which caused cardiac arrest within 15 sec. The spinal
column from the costovertebral angle to the upper sacral vertebrae was removed en bloc and the spinal cord
was rapidly pushed out of the spinal canal as described
BIOGENIC AMINE CHANGES DURING ISCHEMIA/Zmn and Stashak
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
previously.7 The middle of the lumbar enlargement
was identified and the cord was divided into 3 sections:
1. the midlumbar and caudal segment; 2. 1.5 cm of
cord above the midlumbar enlargement which included the upper lumbar cord; 3. the next more rostal 1 cm
of cord which included the low thoracic structures. The
levels were chosen because previous studies8 had indicated that when infarction was present (documented
histologically one week after the occlusion), the low
lumbar region was always involved, the upper lumbar
region was variably affected, and the low thoracic level
never showed signs of morphological damage. In initial studies, pieces of the cervical spinal cord were
similarly processed to serve as another control. The
spinal cord pieces were then rapidly frozen in blocks of
saline ice as described previously.7 The entire procedure, from the time of pentobarbital injection to embedding the cord segments in ice required less than 5
min. The blocks were then cut transversely in a cryostat to produce 500 ju,m thick sections which were
affixed to glass slides. Morphology was checked
grossly to establish that the spinal cord levels had been
correctly identified.
Seven consecutive sections were taken from the center of each block. From 6 sections, 500 ^im diameter
samples (punches) of gray matter were removed as
described previously;7 these came from: 1. anterior
horn; 2. lateral gray matter (between the anterior and
posterior horn); 3. posterior horn. From the seventh
section, the white matter was obtained by dissection
with an iris knife as described previously.9 These particular areas were chosen because our prior histological studies8 had indicated that the anterior horn in the
low lumbar region was more susceptible to infarction
than the posterior horn, and that an intermediate lateral
gray matter region existed that was variably affected.
In contrast, the white matter was always spared by as
much as 1 hr of ischemia. All tissue samples were then
placed in small polyethylene tubes containing 100 ix\
of ice cold 0.1 M perchloric acid and 57 nM 5-hydroxytryptophan. The tubes were closed and immediately
spun in a small centrifuge to submerse all tissue in the
cold acid. The tubes were then placed in the cup horn
of a Branson Sonifier 200 and sonicated at full power
for 15 to 30 sec (preliminary studies showed no loss of
5HT or NE after 2 minutes of such treatment). A five
/JL\ aliquot was removed for protein determination;10 the
remainder was spun at 5000 X g in a refrigerated
centrifuge, the supernate was removed, aliquotted for
5HT and NE assays, and frozen at - 80°C. All assays
were performed within one week. Serotonin and 5hydroxyindoleacetic acid (5HIAA) were measured by
high pressure liquid chromatography with electrochemical detection;" 5-hydroxytryptophan was used
as an internal standard. Norepinephrine was measured
by a radioenzymatic procedure. n These methods are of
sufficient sensitivity so that NE, 5HT, and 5HIAA
could all be measured on aliquots of each sample. For
measurement of 5HT and 5HIAA, tissue sample pools
were repeatedly checked throughout each day to ensure that results were reproducible. For 5HT the coeffi-
557
cient of variation for such determinations averaged
2.15%, for 5HIAA the coefficient of variation averaged 3.10%.
The experimental protocol consisted of comparing
groups of 4 ischemic animals and 4 control animals in
which a snare ligature was placed but not pulled tight.
Only one period of ischemia was studied during each
experiment so that the related experimental and control
animals were exposed to the same uncontrolled variables. Biochemical assays were conducted simultaneously on the corresponding experimental and control
animal tissues. Thus, comparison of results of experimental and related control values is more precise than
that between different durations of ischemia. As a consequence, the data analysis methods emphasized comparison of the ratio of the experimental results of a
given duration of ischemia with the related controls.
Concentrations of the biogenic amines are normalized in terms of protein concentration in the homogenate. Results were analyzed by a three-factor analysis
of variance (case I). 13 The differences among cell
means were determined by the Newman-Keuls procedures13 and results demonstrable at the 5% confidence
level {p < 0.05) were considered significant. With a
complex factorial design, an occasional result may be
lost (in this study, fewer than 1%). Such data were
handled by standard methods and the degrees of freedom were appropriately reduced.14
Results
All animals in which the snare ligature was tightened developed complete paraplegia and anesthesia in
the hind quarters within 2 minutes. In preliminary experiments, attempts were made to delineate the extent
of the ischemic region by injection of carbon black.
Although this procedure clearly showed lack of perfusion in the musculature of the lower abdomen, hind
legs, and sacral regions, there was not usually a definite delineation of the carbon black at any level of the
spinal cord (DeGirolami and Zivin, unpublished observations). Thus, although the lower lumbar and sacral segments of the spinal cord were unquestionably
ischemic, as shown by the abrupt onset of functional
deficits and necrotic changes that ultimately appear,5' 6-8 the blood flow is not completely absent in
these areas. As a consequence, it was not possible to
dissect the spinal cord on the basis of unequivocal
knowledge of the precise locus of the blood flow
changes, and therefore the division was made on the
basis of anatomical landmarks (as indicated in the Materials and Methods Section).
Preliminary experiments also indicated that the
blood pressure in the thoracic aorta did not change
from normal while the abdominal aorta was occluded,
but the pressure in the femoral arteries dropped to
undetectable levels (Roizen and Zivin, unpublished
observations).
Serotonin
The average 5HT concentrations in control rabbits at
low thoracic and lumbar levels were: posterior gray
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
matter, 5.65 ± 0.25 ng/mgprotein (mean ± s.e.,n =
60); lateral gray matter, 12.67 ± 0.57; anterior gray
matter, 13.46 ± 0.59; and white matter, 5.28 ± 0.36.
Table 1 summarizes the results seen in ischemia; the
table gives the ratios of experimental to control values
at the three spinal cord levels and in the four areas as a
function of duration of ischemia. Asterisks indicate
values that are significantly different from unity. It
seemed possible that further significant effects might
be hidden in the noise level of the assay. Therefore, to
increase precision, statistical pooling was considered.
Analysis of variance indicated that, since the appropriate interaction terms were not significant, it was legitimate to pool the gray matter serotonin concentrations
at each spinal cord level (results were pooled, not the
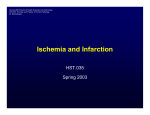
tissues). Figure 1 is a graphical representation of the
results of this analysis; asterisks again indicate significant changes from control.
Table 1 demonstrates that significant 5HT concentration changes occurred in a number of individual
areas. At the low lumbar level, 5HT declined only in
the anterior horn at 33 and 55 min of ischemia. However, when the gray matter areas were pooled at that level
no significant changes were found, as shown in figure
1. In the upper lumbar region several individual gray
matter areas were significantly reduced as shown on
table 1, but analysis of the pooled gray matter indicates
the pattern more clearly; figure 1 shows that in the
upper lumbar region pooled gray matter 5HT declined
significantly at 14 and 20 min of ischemia and then
returned to normal. At the low thoracic level, 5HT in
two gray matter areas was significantly reduced at 14
min and the pooled gray matter at that time was also
TABLE 1 Serotonin
Level
Low lumbar
Upper lumbar
Time
5
14
20
33
55
Posterior
gray
1.44
1.13
0.63
0.98
0.84
Areas
AnteLateral
rior
gray
gray
1.11
1.16
1.01
0.81
0.77
0.74
0.52*
0.84
0.89
0.69*
5
14
20
33
55
1.10
0.42*
0.64
1.10
1.21
0.95
0.74
0.61*
1.07
1.07
1.00
0.81
0.64*
1.37
1.28
1.22
5
1.17
1.26
14
0.66*
0.69*
0.80
20
1.05
0.79
1.08
33
1.28
1.01
1.01
55
1.14
1.07
1.25
Ratios of experimental to control groups.
Time is minutes of ischemia.
indicates significant change from control.
Low thoracic
VOL 14, No 4, 1983
STROKE
558
White
1.33
1.46*
0.91
1.18
0.69
1.42
0.90
1.02
1.36
1.31
1.11
0.85
0.46*
0.87
1.18
SEROTONIN
160
120
Percent
of
Control
80 -
40
20
40
60
Time(min)
FIGURE 1. Serotonin concentrations in various levels of spinal cord gray matter at progressively longer durations of ischemia. Triangles indicate low lumbar (LL) points, squares indicate upper lumbar (UL) points, and circles indicate low
thoracic (LT) points. Each point is the average of posterior,
lateral, and anterior gray matter at that level from 4 animals.
The dashed line indicates control values. Asterisks indicate
points that are significantly different from control.
decreased. In white matter, table 1 shows a significant
increase in 5HT in the low lumbar level at 14 min and a
significant decrease at 20 min in the low thoracic level.
At 14, 33 and 55 min of ischemia, 5HT measurements were made on anterior horn, lateral gray, posterior horn and white matter specimens from cervical
spinal cord. No significant changes from control values were found at any of these times.
5-Hydroxyindoleacetic Acid
Measurements of 5-HIAA were made simultaneously with serotonin in each sample. Posterior gray 5HIAA concentration from control animals at the low
thoracic and lumbar levels averaged 2.35 ± 0.20 ng/
mg protein (n = 60), lateral gray was 3.00 ± 0.11,
anterior gray was 2.92 ± 0.15, and white matter was
2.21 ± 0.17. No significant changes from control
were detected at any time of ischemia.
Norepinephrine
Norepinephrine was also measured in all of the same
tissue samples that were tested for 5HT. The average
NE concentrations in control rabbits were: posterior
gray matter, 2.26 ± 0 . 1 1 ng/mg protein (n = 60);
lateral gray matter, 2.08 ± 0.10; anterior gray matter,
2.92 ± 0.10; and white matter 1.56 ± 0.13. Table 2
summarizes the results seen in ischemia; the table
gives the ratios of the experimental to control values as
559
BIOGENIC AMINE CHANGES DURING ISCHEMIA/Z/vm and Stashak
NOREPINEPHRINE
160
-
120
Percent
of
Control
80
LT
^\
~
*LL
40
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
i
i
20
i
1
40
1
60
Time(min)
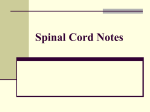
FIGURE 2. Norepinephrine concentrations in various levels of
spinal cord gray matter at progressively longer durations of
ischemia. Triangles indicate low lumbar (LL) points, squares
indicate upper lumbar (UL) points, and circles indicate low
thoracic (LT) points. Each point is the average of posterior,
lateral, and anterior gray matter at that level from 4 animals.
The dashed line indicates control values. The asterisk indicates
the only point that is significantly less than control.
in table 1. Again, analysis of variance indicated that all
gray matter areas at a given spinal cord level could be
statistically pooled and results are shown in figure 2.
Pooled gray matter NE was significantly reduced from
control only in the low lumbar area at 55 min. No other
significant changes were detected in pooled gray matter at a given level. There were some individual gray
matter areas (as shown in table 2) that did change from
control at various other times but no pattern was apparent. In white matter, the NE concentration was significantly elevated in the lumbar level at 14 min of ischemia and significantly decreased at 55 min. At 14, 33
and 55 min of ischemia, NE measurements in cervical
spinal cord sections from animals subjected to ischemia at more caudal levels showed no significant
changes from controls.
Discussion
The findings of this study support the contention that
spinal cord biogenic amine concentrations change during the early stages of the infarction process. The 5HT
changes in gray matter indicate that in the most severely damaged region, there is a modest decline in 5HT
after the damage becomes permanent. In less ischemic
regions adjacent to the infarcted areas, changes in serotonin are more complex. During the times when irreversible changes are occurring in more ischemic areas,
there is approximately a 35% decrease in 5HT. However, when the damage finally becomes permanent in
the more ischemic regions, 5HT in the "marginal
areas" returns to normal. There is a significant decrease in the concentration of 5HT in gray matter as
rostal as the low thoracic area at 14 min of ischemia.
Since there was no similar change in the cervical sections at that time, the 5HT changes were not generalized. Therefore, it is probable that the "marginal region" extended a bit more rostrally briefly or that the
low thoracic sections were cut a bit too caudally in this
particular set of animals. No consistent pattern of
changes in 5HT occurred at more distant sites or at
other times. The importance of white matter 5HT
changes is not clear. The NE in the white matter near
the ischemic gray matter increases to 160% of control
during the early stages of ischemic but latter declines
to less than 50% of control. Consistent gray matter
decreases become clear only at 55 min of ischemia,
which is after the neurological damage has become
permanent in essentially all animals. We did not find
any generalized changes in 5HT, 5HIAA, or NE which
indicates that our methods are valid for use as a screening procedure.
The method of dissection was chosen to correlate
with morphological changes we observed previously.8
Since more damage had been seen in the anterior horns
than in other areas after brief periods of ischemia, we
thought there might be major biochemical differences
among these regions. The lack of significant interaction terms in the analysis of variance indicated that all
the gray matter areas at a given level were changing in
essentially the same way and pooling such data might
TABLE 2 Norepinephrine
Areas
Level
Low lumbar
Upper lumbar
Low thoracic
Time
Posterior
gray
Lateral
gray
Anterior
gray
White
1.05
5
1.00
1.25
1.19
14
1.27
1.28
1.14
1.62*
20
0.72*
0.78
0.96
1.00
33
0.93
0.91
0.70*
1.19
55
0.37*
0.57*
0.79
0.46*
5
0.96
0.91
1.04
1.24
14
0.76
0.82
1.11
0.52
20
0.91
0.92
0.70*
0.80
33
0.85
0.82
1.18
0.77
55
0.70
0.72
0.77
0.62
5
0.93
1.14
0.84
1.00
14
0.73
1.18
0.96
0.63
20
0.92
0.89
0.90
0.69
33
0.81
0.91
0.72
0.98
55
0.32*
0.72
1.04
0.86
Ratios of experimental to control groups.
Time is minutes of ischemia.
indicates significant change from control.
560
STROKE
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
give more reliable results because the sample size was
larger. With the possible exception of the anterior horn
5HT changes detected at the low lumbar level, there
does not appear to be any recognizable or consistent
pattern to the changes in isolated gray matter areas
where pooled data did not indicate significant differences. Thus, the pooled results (shown in figures 1 and
2) appear to be more meaningful indicators of the pattern of gray matter changes (i.e., significant changes
seen in individual areas does not guarantee that they
are scientifically important).
There have been a number of other studies of the
effects of strokes on biogenic amine concentrations.
Welch et al.15 measured 5HT concentrations in cortex
of gerbils 3 and 4 hours after unilateral carotid ligation.
They reported decreased concentrations on the infarcted side, but the time periods studied are long after
irreversible damage is done. Furthermore, gerbils are
highly subject to seizures during infarction, which
would have unpredictable effects on neurotransmitter
concentrations.16, " Members of this group18 reported
that unilateral common carotid artery occlusion in gerbils resulted in decreased NE by one hour after occlusion in the ischemic hemisphere. They also reported
that after occlusion of one carotid, there was a decrease
in 5HT within 5 min in both hemispheres which persisted essentially unchanged for up to one hour. Subsequently some of the members of this same group19
reported that, one hour after occlusion of one hemisphere with multiple large emboli, NE increased in
both hemispheres, 5HT remained unchanged and,
5HIAA increased.
Brown et al.20 reported decreased 5HT and NE concentrations during global ischemia produced by raised
intracranial pressure. These decreases were observed
after 7.5 min of ischemia and the decline continued
after 30 min of subsequent restoration of flow. The
"bloodless" global ischemia produced by raising intracranial pressure is unlike the focal ischemia which is
the most common medical problem. Calderini et al.21
exposed rats to bilateral carotid occlusion plus hypovolemia for 15 min and found no changes in NE, 5HT and
5HIAA, but NE and 5HT declined in some groups
during 30 min of subsequent recirculation.
Mrsulja and associates22'23 measured neurotransmitters in cerebral tissue of gerbils during infarction produced by unilateral carotid occlusion. Serotonin and
NE concentrations were shown to decrease relative to
those of the opposite hemisphere. These results are
difficult to interpret because the concentrations of
monoamines in the perfused hemisphere may change
after infarction of the opposite side.24-25 In another
paper this group26 found that, after 15 min of cortical
ischemia produced by bilateral carotid occlusion in
gerbils, 5HT declined to 78% of control in frontal
cortex but was unchanged in basal ganglia. During that
same period NE declined to 78% in cortex and 50% in
basal ganglia.
Zervas and associates27'28 measured NE after 24
hours of unilateral common carotid ligation in gerbils.
Norepinephrine was shown to be decreased on the in-
VOL
14, No 4, 1983
farcted side. These measurements were made long
after irreversible changes occurred. Robinson et al. 29,30
showed ipsilateral decrease in NE in rat cortex or
brainstem after arterial occlusion many hours after irreversible changes occurred.
Kogure et al.25 reported NE declined for at least 4
hours in both hemispheres of rats after carotid infarction produced by injection of microemboli. Again, the
biochemical measurements were made long after damage was irreversible.
Harrison and associates 3132 studied 5HT, 5HIAA
and NE in gerbils 3.5 hours after carotid ligation and
found decreased concentrations of all these substances
in both the infarcted and control hemispheres. These
studies were conducted long after damage was irreversible.
To summarize, although a number of groups have
studied various aspects of the effects of biogenic
amines on CNS ischemia, none has used a model of
focal ischemia that is as reproducible as the rabbit
spinal cord infarction model. Many of the previously
reported results suggest, as does the present paper, that
substantial rapid declines in 5HT and NE occur. But,
most of these previous studies were not designed to
evaluate the early time periods when the changes were
becoming irreversible and therapeutic intervention
might be expected to be most effective.
These prior studies were hampered by the complexity of the cerebral models that were used, and it was
particularly difficult to examine change occurring in
any marginally viable tissue that may border irreversibly damaged regions. Screening studies have been
successful in other circumstances when large and uncomplicated changes occur. However, the biogenic
amine changes during ischemia appear to be more subtle. Therefore, we hoped that use of a simpler system
would help to reduce the complexity of the problem.
We recognized that such screening tests are rarely definitive, especially when we had no a priori hypotheses
concerning which changes might occur or their locations. We were primarily searching for suggestions of
the types and locations of changes that might indicate
more rigorous follow up studies.
The rapid alterations of biogenic amines reported in
this paper may have substantial implications for understanding the pathophysiology of ischemia and suggesting possible therapeutic manipulations. The absolute
size of the changes may be larger than was apparent in
this study because the precise location of the structures
involved has not yet been completely established. For
example, if large changes occur in very localized
areas, they may have been missed in this study which
was a survey. Also, it is possible that substantial
changes in turnover rates of biogenic amines are occurring. Since a steady state is not present during the early
stages of infarction, such turnover studies are currently
impossible. However, it is clear that 5HT is not being
rapidly degraded to 5HIAA since the 5HIAA concentrations do not change.
The lack of rapid changes in the most ischemic areas
is not surprising because, at a low blood flow rate,
BIOGENIC AMINE CHANGES DURING ISCHEMIA/Z/vm and Stashak
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
rapid alterations in tissue concentrations of biogenic
amines cannot occur unless they are degraded. We
have shown that such metabolism of 5HT did not occur
and apparently the same is true of NE although catecholamine metabolites were not measured in this
study. Whether there are alterations in the location of
these substances (for example, release from neurons or
platelets to other locations) cannot be established by
the methods used in this study.
The rapid 5HT changes in the border zone of the
lesion that occur at precisely the time that damage is
becoming irreversible are particularly interesting. Reversible changes occur at the lesion edge, and this
suggests that pharmacological manipulations could potentially alter these responses. The viability of the tissue at the lesion edge is presumably precarious during
ischemia and tissue in this region which might otherwise be irreversibly damaged could be potentially salvaged if 5HT is causally related to the destruction
process. The relatively larger changes that occur in this
transitional region compared with the more modest
changes in completely infarcted tissue and at more
distant sites suggest that 5HT is actively participating
in the development of the lesion; whether these effects
are harmful or helpful is still not clear. Furthermore,
since the damage becomes irreversible so quickly,
only a pharmacological manipulation would have any
reasonable chance of success in clinical situations (for
example, surgical intervention in most cases would be
impractical). There are a large number of drugs that
can alter 5HT actions, thus, further investigation is
justified by these findings.
The reasons for the early increase in 5HT in white
matter is not clear. However, the white matter is not
infarcted within the time periods studied in this model.
Thus, further studies will be necessary to confirm and
clarify this finding.
The NE changes are of a different character. In gray
matter there is a gradual decline in the infarcted region
that only becomes statistically significant at 55 min,
i.e., after damage is irreversible. In white matter, there
is an initial brief increase of NE in the ischemic tissue,
but by 55 min the concentration has declined significantly from control. The meaning and importance of
this white matter finding is not currently clear. The
relatively slow decline in NE in gray matter may simply reflect the effects of nonspecific damage, and the
lack of changes in the NE concentrations in the marginally damaged areas does not clearly implicate this
biogenic amine in initiation of irreversible damage.
In conclusion, since nervous tissue serotonin concentrations are changing in a time course that closely
follows the onset of clinical deficits, it appears that this
biogenic amine may be involved in the processes that
cause irreversible deficits. There are other substantial
changes that occur in the CNS during ischemia, for
example, energy metabolism is markedly altered.33
The time and course of these changes does not match
the occurrence of irreversible deficits, and therefore it
is not clear that energy metabolism changes are involved in initiating the irreversible damage. Similarly,
561
in this paper it was shown that norepinephrine changes
occur somewhat after the onset of clinical injury. However, these energy metabolism and NE changes probably eventually play a role in tissue destruction. Further investigations clearly indicated are studies of the
precise correlation of spinal cord blood flow with
biochemical and morphological changes, and pharmacological manipulations which alter biogenic amine
concentrations. It may then be possible to more completely establish a cause-effect relationship between
the biochemical changes observed and the ultimate
neurological and histological consequences of CNS
infarction.
Acknowledgment
We would like to thank John Venditto for excellent technical assistance. This project was supported by PHS grants NS 00456 and NS
15827.
References
1. Schmidt CF: Central nervous system circulation fluids and barriers. In Handbook of Physiology, Vol. 3. Field J, Magoun HW,
and Hall VE, (eds), American Physiological Soc: Washington DC,
1960, pp 1745-1750
2. Molinari GF, Laurent JP: A classification of experimental methods
of brain ischemia. Stroke 7: 14-17, 1976
3. Yatsu FM: Biochemical mechanisms of ischemic brain infarction.
In Handbook of Clinical Neurology, Vol. 27. Vinken PJ and Bruyn
GW (eds), American Elsevier, New York, 27-37, 1976
4. Waltz AG: Clinical relevance of models of cerebral ischemia.
Stroke 10: 211-213, 1979
5. Zivin JA, DeGirolami U: Spinal cord infarction: A highly reproducible stroke model. Stroke 11: 200-202, 1980
6. Zivin JA, DeGirolami U, Hurwitz EL: A quantitative study of the
spectrum of neurological deficits in experimental nervous system
ischemia. Arch Neurol 39: 408-412, 1982
7. Zivin JA, Reid JL, Saavedra JM, Kopin IJ: Quantitative localization of biogenic amines in the spinal cord. Brain Res 99: 293-301,
1975
8. DeGirolami U, Zivin JA: Neuropathology of experimental spinal
cord ischemia in the rabbit. J Neuropath Exp Neurol 41: 129-149,
1982
9. Zivin JA, Doppman JL, Reid JL, Tappaz ML, Saavedra JM, Kopin
IJ, Jacobowitz DM: Biochemical and histochemical studies of biogenic amines in spinal cord trauma. Neurol 26: 99-107, 1976
10. Lowry OH, Rosenrough NJ, Fair AL, Randall RJ: Protein measurement with the folin phenol reagent. J Biol Chem 193: 265-275,
1951
11. Reinhard JF, Moskowitz MA, Sved AF, Fernstrom JD: A simple,
sensitive and reliable assay for serotonin and 5-HIAA in brain
tissue using liquid chromatography with electrochemical detection.
LifeSci27: 905-911, 1980
12. Henry DP, Starman BJ, Johnson DG, Williams RH: A sensitive
radioenzymatic assay for norepinephrine in tissues and plasma.
Life Sci 16: 375-484, 1975
13. Winer BJ: Statistical Principles in Experimental Design, second
edition. McGraw-Hill, New York, 1971
14. Zivin JA, Bartko JJ: Statistics for disinterested scientists. Life Sci
18: 15-26, 1976
15. Welch KMA, Chabi E, Buckingham J, Bergin B, Achar VS, Meyer JS: Catecholamine and 5-hydroxy-tryptamine levels in ischemic
brain: Influence of p-chlorophenylalanine. Stroke 8: 341-346,
1977
16. Calderini G, Carlsson A, Nordstrom CH: Monoamine metabolism
during bicuculline-induced epileptic seizures in the rat. Brain Res
157: 295-302, 1978
17. Welch KMA, Wang TPF, Chabi E: Ischemia-induced seizures and
cortical monoamine levels. Ann Neurol 3: 152-155, 1978
18. Gaudet R, Welch KMA, Chabi E, Wang TP: Effect of transient
ischemia on monoamine levels in the cerebral cortex of gerbils.
Neurochem 30: 751-757, 1978
562
STROKE
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
19. Ishihara N, Welch KMA, Meyer JS, Chabi E, Naritomi H, Wang
TPF, Nell JH, Hsu MC, Miyakawa Y: Influence of cerebral embolism on brain monoamines. J Neurol Neurosurg and Psych 42:
847-853, 1979
20. Brown RM, Carlson A, Ljunggren B, Siesjo BK, Snider SR: Effect
of ischemia on monoamine metabolism in the brain. Acta Physiol
Scand90: 789-791, 1974
21. Calderini G, Carlsson A, Norstrom CH: Influence of transient
ischemia in monoamine metabolism in the rat brain during nitrous
oxide and phenobarbitone anaesthesia. Brain Research 157: 303310, 1978
22. Lust DW, Mrsulja BB, Mrsulja BJ, Passonneau JV, Klatzo I:
Putative neurotransmitters and cyclic nucleotides in prolonged ischemia of the cerebral cortex. Brain Res 98: 394-399, 1975
23. Mrsulja BB, Mrsulja BJ, Spatz M, Klatzo I: Brain serotonin after
experimental vascular occlusion. Neurol 26: 785-787, 1976
24. Ginsberg MD, Reivich M, Giandomenico A, Greenberg JH: Local
glucose utilization in acute focal cerebral ischemia: Local dysmetabolism and diaschisis. Neurol 27: 1042-1048, 1977
25. Kogure K, Scheinberg P, Matsumoto A, Busto R, Reinmuth OM:
Catecholamines in experimental brain ischemia. Arch Neurol 32:
21-24, 1975
26. Cvejie V, Micic DV, Djuricic BM, Mrsulja BJ, Mrsulja BB:
27.
28.
29.
30.
31.
32.
33.
VOL
14,
No
4,
JULY-AUGUST
1983
Monoamines and related enzymes in cerebral cortex and basal
ganglia following transient ischemia in gerbils. Acta Neuropath 51:
71-77, 1980
Lavyne MH, Moskowitz MA, Larin F, Zervas NT, Wurtman RJ:
Brain H3-catecholamine metabolism in experimental cerebral ischemia. Neurol 25: 483-485, 1975
Zervas NT, Hori H, Negora M, Wurtman JR, Larin F, Lavyne MH:
Reduction in brain dopamine following experimental cerebral ischemia. Nature 247: 283-284, 1974
Robinson RG, Shoemaker WJ, Schlumpf M, Valk T, Bloom FE:
Effect of experimental cerebral infarction in rat brain on catecholamines and behavior. Nature 255: 332-334, 1975
Robinson RG, Shoemaker WJ, Schlumpf M: Time course of
changes in catecholamines following right hemispheric cerebral
infarction in the rat. Brain Res 181: 202-203, 1980
Harrison MJG, Marsden CD, Jenner P: Effect of experimental
ischemia on neurotransmitter amines in the gerbil brain. Stroke 10:
165-168, 1979
Harrison MJG, EllamLD: Role of 5HT in the morbidity of cerebral
infarction — a study in the gerbil stroke model. J Neurol, Neurosurg, and Psych 44: 140-143, 1981
Siesjo BK: Brain Energy Metabolism. John Wiley and Sons. New
York, 1978
Ischemic Brain Edema With and Without Reperfusion:
An Experimental Study in Gerbils
FAUSTO IANNOTTI, M.D.
AND JULIAN HOFF,
M.D.
SUMMARY Tissue water and rCBF from the same area of brain was measured in gerbils with cerebral
ischemia. In one experiment we related the severity of ischemia that developed after one hour of carotid
occlusion to the amount of edema which formed. In a second experiment brain made ischemic for one hour
was reperfused for one hour to assess the effect of reperfusion of ischemic tissue upon edema formation. We
identified a critical threshold (10-14 mMOOg-'min-') for the reversibility of the ischemic process, above
which edema can resolve upon reperfusion. When postocclusion rCBF was less than 10 mMOOg-'min- 1 ,
edema was maximal at the end of occlusion and did not resolve with reperfusion. Autoregulation was
preserved in ischemic tissue in which the edema process resolved with reperfusion.
Stroke Vol 14, No 4, 1983
RESTORATION OF BLOOD FLOW to ischemic
brain is now clinically feasible.1 Logic dictates that
reperfusion of ischemic brain tissue should improve
brain function and might improve outcome from an
ischemic event, but clinical and laboratory experience
indicate that edema formation associated with ischemia may actually be aggravated by reperfusion. '•2 This
conflict between logic and experience poses a practical
question for clinicians: Should ischemic tissue be reperfused and, if so, under what circumstances?
Both the duration and the severity of ischemia influence the effects of reperfusion.2 The duration of ischemia from which recovery of function can be expected
varies from species to species, and is affected by temperature, drugs, anatomical variants, age and other
From the Section of Neurosurgery, University of Michigan, Ann
Arbor, Michigan.
Supported by NIH Grant NS 17760.
Address correspondence to: Julian T. Hoff, M.D., Section of Neurosurgery, C5088 Outpatient Building, Box 54, Ann Arbor, Michigan
48109.
Received July 14, 1982; revision accepted March 17, 1983.
factors. The severity of ischemia is influenced by the
degree of perfusion of a core of tissue with its own
exclusive capillary bed and by the perfusion of that
tissue through collateral vessels able to react to the
ischemic event nearby. Thus, acute occlusion of a major cerebral artery may cause severe or even complete
ischemia in a small area, moderate ischemia in a larger
adjacent area, and no ischemia in peripheral areas perfused normally by abundant collateral vessels.
We developed an animal model that provides a spectrum of low flow states for one hour after acute carotid
occlusion.3 4 Measurement of rCBF and tissue water
from the same area of brain in this preparation has
allowed us to relate the severity of ischemia to the
severity of edema which forms during the first hour
after occlusion and to identify the effects of reperfusion
upon rCBF and edema in the same tissue.5
In earlier studies, brain water content was closely
related to the severity of ischemia. The rCBF threshold
for edema formation, identified in our gerbil model,
coincided with that found in the primate model by
Symon, et al.6 The ischemia threshold for edema formation we demonstrated was slightly higher than that
The effect of ischemia on biogenic amine concentrations in the central nervous
system.
J A Zivin and J Stashak
Downloaded from http://stroke.ahajournals.org/ by guest on June 18, 2017
Stroke. 1983;14:556-562
doi: 10.1161/01.STR.14.4.556
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1983 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://stroke.ahajournals.org/content/14/4/556
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not
the Editorial Office. Once the online version of the published article for which permission is being
requested is located, click Request Permissions in the middle column of the Web page under
Services. Further information about this process is available in the Permissions and Rights Question
and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/