Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuromuscular junction wikipedia , lookup
Alzheimer's disease wikipedia , lookup
Human brain wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuroeconomics wikipedia , lookup
Neuroregeneration wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Metastability in the brain wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Neuroplasticity wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Aging brain wikipedia , lookup
Development of the nervous system wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Neuroanatomy wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Anatomy of the cerebellum wikipedia , lookup
Block 6 – Neurology Learning Objectives Arunan Sriravindrarajah The following lecture objectives were ordered thematically TABLE OF CONTENTS Spinal Cord .............................................................................................................................................................. 5 Spinal Cord 1 – Cells, Receptors and Reflexes ................................................................................. 5 Spinal Cord 2 – The Tracts ....................................................................................................................... 7 Spinal Cord 3 – Dysfunctions and Deficits ....................................................................................... 10 Spinal Autonomic Organisation............................................................................................................. 12 Central Nervous System ....................................................................................................................................... 13 Fundamentals of CNS Development ................................................................................................... 13 Normal and Abnormal Development of the CNS ............................................................................ 15 Secretion and Absorption of the CSF ................................................................................................. 17 Imaging the Brain ...................................................................................................................................... 19 Seizures ................................................................................................................................................................. 20 Amino Acid Neurotransmission ............................................................................................................. 20 Anticonvulsants........................................................................................................................................... 22 Seizure Disorders ....................................................................................................................................... 24 Brainstem ............................................................................................................................................................. 24 Introduction to Brainstem....................................................................................................................... 24 Cranial Nerve Organisation .................................................................................................................... 26 Lower Brainstem Functions .................................................................................................................... 28 Stroke.................................................................................................................................................................... 29 Epidemiology of Stroke ............................................................................................................................ 29 Stroke – Prevention and Management .............................................................................................. 30 Blood Supply to the Brain ....................................................................................................................... 31 Brain / CNS Infection ............................................................................................................................................ 34 Blood Brain Barrier .................................................................................................................................... 34 Viral Encephalitis and Meningitis .......................................................................................................... 35 Case Conference – CNS Infections ...................................................................................................... 37 Antibiotics and the CNS ........................................................................................................................... 38 Headache and Migraine........................................................................................................................................ 39 Sensory Innervation of the Head and Functional Anatomy of Head Pain ............................ 39 Classification and Diagnosis of Headache ......................................................................................... 40 Pathogenesis and Treatment of Migraine ......................................................................................... 42 Vision .................................................................................................................................................................... 43 Visual Pathways – Anatomy ................................................................................................................... 43 The Eye – Normal and Abnormal ......................................................................................................... 45 1 Orbital Anatomy (Including Extraocular Muscles) ......................................................................... 46 Visual Pathways – Physiology ............................................................................................................... 48 Anatomy and Physiology of the Lens and Accommodation ....................................................... 51 Anatomy and Physiology of the Cornea ............................................................................................ 53 Basal Ganglia......................................................................................................................................................... 56 Basal Ganglia Circuitry – Normal ......................................................................................................... 56 Basal Ganglia Circuitry – Abnormal .................................................................................................... 58 Movement and Associated Disorders ................................................................................................................... 59 Motor Disorders .......................................................................................................................................... 59 Cerebellum – Coordinating Movement ............................................................................................... 60 Clinical Aspects of Parkinson’s Disease and Related Disorders ................................................ 63 Dementia .............................................................................................................................................................. 65 Anatomy of Attention and Memory ..................................................................................................... 65 Functional Imaging of the Brain ........................................................................................................... 67 Prion Diseases ............................................................................................................................................. 68 Pathogenesis of Alzheimer’s Disease ................................................................................................. 70 Cognitive Function and Dementia ........................................................................................................ 72 Emerging Therapies for Dementia ....................................................................................................... 74 Mental Illness ....................................................................................................................................................... 77 Anatomy of Emotional Systems ........................................................................................................... 77 Introduction to Major Mental Illness ................................................................................................... 78 Gene, Brain and Behavioural Basis for Psychiatric Illness ......................................................... 80 Neurotransmitter Disturbances in Depression ................................................................................ 81 Mechanism of Drug Action in Depression ......................................................................................... 82 Psychosis – An Overview ........................................................................................................................ 84 Antipsychotic Drugs .................................................................................................................................. 86 Bipolar Disorders ........................................................................................................................................ 88 Paediatrics ............................................................................................................................................................ 90 Assessment – Paediatric Self-Directed Learning Project (SDLP) ............................................. 90 Paediatric History Taking ........................................................................................................................ 90 Ethics .................................................................................................................................................................... 92 Introduction to Medical Ethics – Part I .............................................................................................. 92 Other..................................................................................................................................................................... 92 Introductory Lecture ................................................................................................................................. 92 Neuropathic Pain ........................................................................................................................................ 92 Autopsy Processes ..................................................................................................................................... 93 2 Framing Disability ...................................................................................................................................... 95 Temperature Regulation .......................................................................................................................... 96 Cranial Nerves – Clinical Perspective I .............................................................................................. 97 PPD Assessment ....................................................................................................................................... 101 Cortical Localisation ................................................................................................................................ 101 Auditory Pathways and Cochlear Implants .................................................................................... 102 Clinical Pharmacology of Old Age ...................................................................................................... 104 Overview of Multiple Sclerosis – Diagnosis .................................................................................... 105 Structure and Function of Peripheral Nerves – Common Neuropathies ............................. 109 Mobility Matters to T-Cells – How T-Cells Move and Cause Disease .................................... 110 Seminars ............................................................................................................................................................. 112 Neurotrauma .............................................................................................................................................. 112 Living with Disability – Pain ................................................................................................................. 114 Malformations in the Nervous System ............................................................................................. 115 Community Impact of Spinal Cord Injury ....................................................................................... 115 Cerebrovascular Disease ....................................................................................................................... 116 Case Conference – Clinical Disorders of the Autonomic Nervous System ......................... 117 Cranial Nerves – Clinical Perspective II........................................................................................... 118 Systematic Reviews ................................................................................................................................ 119 Neuroinfection ........................................................................................................................................... 120 Case Conference – Stroke .................................................................................................................... 121 Case Conference – Exercises in Critical Thinking and Diagnosis in Clinical Neurology – Part I ............................................................................................................................................................. 122 Brain Tumours ........................................................................................................................................... 123 Impact of Blindness ................................................................................................................................ 124 Case Conference – Exercises in Critical Thinking and Diagnosis in Clinical Neurology – Part II ........................................................................................................................................................... 126 Demyelinating Diseases ........................................................................................................................ 128 Muscle Weakness ..................................................................................................................................... 130 Case Conference – Exercises in Critical Thinking and Diagnosis in Clinical Neurology – Part III.......................................................................................................................................................... 131 Clinical Pathology of Movement Disorders ..................................................................................... 132 Community Impact of Neurodegenerative Disease in the Elderly......................................... 134 Motor Neurone Diseases........................................................................................................................ 136 Leaders in the History of Medicine .................................................................................................... 138 Dementia ..................................................................................................................................................... 138 3 Prevention in Psychiatry ........................................................................................................................ 140 Practical .............................................................................................................................................................. 141 Anatomy Practical 1 – Spinal Cord and Spinal Nerves .............................................................. 141 Physiology Practical 1 – Reflexes and Cutaneous Sensation................................................... 142 Anatomy Practical 2 – CSF, Meninges and Ventricles ................................................................ 142 Histology Practical 1 – Histology of Brain and Meninges .......................................................... 143 Anatomy Practical 3 – Normal Brainstem ....................................................................................... 143 Physiology Practical 2 – Eye Movements ........................................................................................ 143 Anatomy Practical 4 – Cranial Nerves .............................................................................................. 143 Pharmacology Practical 1 – Central Neurotransmitters............................................................. 144 Anatomy Practical 5 – Cortex – Structure and Function........................................................... 144 Physiology Practical 3 – Visual Testing ............................................................................................ 145 Anatomy Practical 6 – Visual Pathways ........................................................................................... 145 Anatomy Practical 7 – Motor Pathways ........................................................................................... 146 Anatomy Practical 8 – Forebrain Structures .................................................................................. 146 Anatomy Practical 9 – Anatomy Revision ....................................................................................... 146 4 SPINAL CORD SPINAL CORD 1 – CELLS, RECEPTORS AND REFLEXES Describe the different types of sensory receptors (i.e. tactile, Proprioceptive, pain and temperature) and the fibres that are associated with them (e.g. I, II, III) - The different types of sensory information are Tactile (i.e. touch / vibration), Proprioception (i.e. position) and Pain / Temperature The sensory receptors / fibres associated with each sensory modality are: o Proprioception Muscle Spindles (also known as Neuromuscular Spindles) – these are located parallel and adjacent to the muscle; this is carried via myelinated Type Ia Fibres (70120 m/s) Golgi Tendon Organs – these are carried via Type Ib fibres (70-120 m/s) Joint Receptors - these are carried via Type II fibres (~30-70m/s) o Pain / Temperature A-delta Free Nerve Endings – these Type III fibres have small amount of myelin and are associated with sharp, local pain which is typically superficial (~0.5-2m/s) C Free Nerve Endings – these Type IV fibres have no myelin and are associated with dull, diffuse pain which is typically visceral (~3-30m/s) o Touch Meissner – these are located in hairless skin and will detect touch; this is carried via myelinated Type II fibres (~30-70m/s) Merkel – these are located in all skin and hair, and will detect touch; this is carried via myelinated Type II fibres (~30-70m/s) Ruffini – these are located in all skin and will detect touch (stretch); this is carried via myelinated Type II fibres (~30-70m/s) Pacinian – these are located in the deep layers of the skin and will detect deep touch and vibration; this is carried via myelinated Type II fibres (~30-70m/s) o Vibration Pacinian – these are located in the deep layers of the skin and will detect deep touch and vibration; this is carried via myelinated Type II fibres (~30-70m/s) - Describe the cells (tract and interneurones) and subdivisions (dorsal horn, intermediate grey matter, ventral horn) of the spinal cord - There are two main cells within the Spinal Cord: o Projection Cells These will have their Axon leave the Grey Matter into the White Matter (and from there to other locations) These cells create messages and will be excitatory Examples of Projection Cells include Tract Cells (which have their Axons travel to the White Matter and then to the Brain) and Motor Neurones (which have their Axons travel to the White Matter and then to the peripheries) o Interneurones These will have their Axon remain within the Grey Matter These cells modify messages and can be either excitatory OR inhibitory The main subdivisions within the Spinal Cord are: o Dorsal Horn This will be associated with somatic sensory afferents (e.g. pain, temperature, tactile) These area of the Spinal Cord will contain both Projection Cells and Interneurons o Intermediate Grey Matter - 5 o This will be predominantly associated with Autonomic Motor Cells (although this is the location of the Spinal Cord where the sensory signals that trigger reflexes are received) The Preganglionic Motor Cells in this region are associated with the: Sympathetic Nervous System in the Thoracic and Lumbar parts of the Spinal Cord Parasympathetic Nervous System in the Sacral parts of the Spinal Cord Ventral Horn This will be predominantly associated with Somatic Motor Cells There are two main types of Motor Neurons in the Ventral Horn: Alpha-motor neurones – these will innervate the motor end-plate of skeletal muscle (and hence trigger contraction of skeletal muscles) Gamma-motor neurones – these will innervate muscle spindles (and hence are important from proprioception and the Stretch Reflex and GammaReflex Loop) The different locations / parts of the Ventral Horn are associated with motor innervations of different parts of the body; for example: Lateral Ventral Horn associated with Hand / Foot innervations, whilst Medial Ventral Horn associated with Trunk / Hip innervations) Anterior Ventral Horn associated with Extensor innervations, whilst Posterior Ventral Horn associated with Flexor innervations Describe the different reflexes (i.e. stretch, flexor, gamma reflex loop and Golgi tendon organ), and their functional significance - Whilst reflexes occur without having to send a signal to the higher centres in the brain, these higher centres can send signals down to the Spinal Cord to either deactivate or reactivate a reflex o Hence, clinical testing of reflexes can assess the function of the relevant peripheral motor and sensory spinal nerves as well as the relevant spinal cord level (as damage to this spinal cord level or above would prevent the descending inputs from the higher centre from modulating the reflex) There are four main types of reflexes: o Flexor Reflex This involves a sensory input from the sensory receptor travelling to the Grey Matter where it will synapse with an Interneurone The Interneurone is excitatory and will synapse with an Alpha- motor neurone innervating the agonist (i.e. flexor) muscles Furthermore, the initial sensory input will also synapse with an inhibitory Interneurone, which synapses with the Alpha- motor neurone innervating the antagonist (i.e. extensor) muscles Hence, the overall effect is to stimulate contraction of the flexor muscle and inhibit contraction of the extensor muscle Note: Initial sensory input from the sensory receptor will also travel to spinal levels above and below too, which triggers flexion of other joints as well (i.e. flexion of not only wrist, but also flexion of the elbow and shoulder [which has the effect of magnifying the initial flexion of the wrist]) This reflex is useful to withdraw parts of the body from harmful stimuli (e.g. pull hand away from hot stove) o Stretch Reflex This reflex has a similar mechanism to the Flexor Reflex (e.g. effect on both agonist and antagonist muscles), except the sensory input occurs from the Neuromuscular Spindle in the Muscle (rather than from sensory receptors) This reflex enables maintenance of muscle tone (and prevents muscle from becoming flaccid) o Gamma-Reflex Loop - 6 o This involves a signal from the higher centres travelling down the spinal cord and synapsing with the Gamma-motor neurones These Gamma-motor neurones will innervate the neuromuscular spindles, causing these spindles to activate (which triggers the Stretch Reflex [and hence results in contraction / increase in muscle tone]) This reflex enables centrally mediated maintenance of muscle tone Golgi Tendon Organ Golgi Tendon Organs are located in the tendon and will sense tendon tension When the tendon tension becomes excessive, these Golgi Tendon Organs will send a sensory signal to the Grey Matter where it will synapse with an Interneurone The Interneurone is inhibitory and will synapse with the Alpha-motor neurones innervating the relevant muscle (and hence trigger the muscle to stop contracting, and thus reduce the tendon tension) This reflex is useful to prevent excessive tendon tension, which could rupture the tendon / muscle SPINAL CORD 2 – THE TRACTS Describe tracts and pathways, and general patterns of projections between neural centres - ‘Tract’ refers to a collection of axons Tracts can have either a ‘topographic’ / ‘mapped’ projection pattern or a ‘diffuse’ projection pattern o ‘Topographic’ / ‘mapped’ projection refers to the sensory signals from one cell in a neuron being recognised in the exact same topography (i.e. orientation) in one cell in the recipient neuron This requires the projection to also be ‘Precise’ (i.e. projections from one cell within the neuron matching to a single cell in the recipient neuron) (this occurs in Somatic Pathways) o ‘Diffuse’ projections refer to sensory signals from one cell within the neuron matching to multiple different cells in the recipient neuron) (this occurs in Visceral / Arousal Pathways) Describe the anatomical organisation and function of the major ascending (i.e. dorsal column, spinothalamic, spinocerebellar) and descending (i.e. reticulospinal, vestibulospinal, corticospinal, rubrospinal) tracts o Ascending Tracts Dorsal Column Tract Function of the Dorsal Column Tract is to carry: o Touch (discriminative) and vibration from sensory receptors to the Thalamus o Conscious proprioception signals from proprioceptors (e.g. neuromuscular spindles) to the Thalamus ~80-90% of Axons from Tactile Receptors (or from Proprioceptors) will NOT synapse in the Dorsal Horn, but rather travel straight into the Dorsal Column Tract o The Lower Body Fibres will travel in the Dorsal Column Tract more medially (this is known as the Gracile Tract) o The Upper Body Fibres (above T5) travel in the Dorsal Column Tract more laterally (this is known as the Cuneate Tract) o Note: Dorsal Column Tract is located in the Dorsal Funiculus of the Spinal Cord The Gracile and Cuneate Tracts will synapse with a corresponding Gracile and Cuneate Nuclei respectively in the Medulla o These tracts will then cross to other side after synapsing at these nuclei and become the Medial Lemniscus Tract 7 o o The Medial Lemniscus Tract will travel towards and synapse with the Ventral Posterior (VP) nucleus within the Thalamus o The Thalamus will then communicate this signal to the Somatosensory Cortex The cell bodies of the Axons in the Dorsal Column Tract are in the ipsilateral Dorsal Root Ganglion Spinothalamic Tract This tract will commence in the Dorsal Horn of the Grey Matter (which is the synapse for the axons from the Nociceptors / Thermoreceptors [which travel via (but do not synapse with) the Dorsal Root Ganglion]) o The Tract will cross to the other side in the spinal cord via the Ventral White Commissure towards the Ventrolateral part of the Spinal Cord (mainly in the Ventral Funiculus of the Spinal Cord) Most of the fibres will cross at the same level of the spinal cord, although some fibres will cross a little higher Note: The Upper Body Fibres will travel through the medial aspect of the Ventrolateral part of the Spinal Cord, whilst the Lower Body Fibres will travel through the lateral aspect of the Ventrolateral part of the Spinal Cord o The Spinothalamic Tract will traverse up from the Anterolateral Spinal Cord towards and synapse with the Ventral Posterior (VP) nucleus within the Thalamus Note: Some of the Spinothalamic Tract will connect and synapse with the Brainstem (in the Brainstem Reticular Formation) instead, though the majority will go towards the Thalamus o The Thalamus will then communicate this signal to the Somatosensory Cortex o Note: Cell bodies of the Axons in the Spinothalamic Tract are in the Dorsal Horn o Note: The above was a description of the anatomy of the Lateral Spinothalamic Tract rather than the Anterior Spinothalamic Tract (which is more anterior is location in the spinal cord) Function of the Lateral Spinothalamic Tract is to carry pain / temperature from the body, whilst the Anterior Spinothalamic Tract is to carry light touch from the body Spinocerebellar Tract Function of the Spinocerebellar Tract is to carry unconscious proprioception signals directly to the Cerebellum Axons from Proprioceptors will synapse in the Dorsal Horn, and then travel towards the Anterolateral part of the Spinal Cord, before travelling up the Spinal Cord directly to the Cerebellum as the Spinocerebellar Tract o The cell bodies of the Axons in the Spinocerebellar Tract are in the ipsilateral Dorsal Root Ganglion o Note: The above was a description of the Dorsal Spinocerebellar Tract rather than the Ventral Spinocerebellar Tract (as the Dorsal Spinocerebellar Tract is the main pathway for unconscious proprioception) Descending Tracts (which can send both excitatory AND inhibitory signals) Vestibulospinal Tract This tract originates from the Vestibular Nuclei in the Brainstem and will descend ipsilaterally to the Gamma-motor neurons in the Spinal Cord o The Gamma-motor neurons will then activate the Gamma-Reflex Loop (i.e. Stretch Reflex) This tract innervates mainly on the extensor muscles of the trunk and lower limbs 8 This tract is very fast and excellent at correcting balance Reticulospinal Tract This tract originates from the Brainstem Reticular Formation in the Brainstem and will descend ipsilaterally to the Gamma-motor neurons in the Spinal Cord o The Gamma-motor neurons will then activate the Gamma-Reflex Loop (i.e. Stretch Reflex) in the muscle groups associated with posture and locomotion and will influence the muscle tone of these muscles o Note: Some of the Reticulospinal Tract will descend and activate Alpha-motor neurons, which innervate Visceral (Smooth) Muscle and influence their muscle tone Corticospinal Tract This tract is the dominant descending pathway! o This is the only descending tract that innervates the digits (and hence enables ‘skilled movements’) This tract originates from the Cortex (predominantly the Motor Cortex) and will traverse via large white matter highways towards the spinal cord The sequence of white matter highways are Corona Radiata, Internal Capsule, Cerebral Peduncle (Midbrain) and Pyramid (Medulla) o There are numerous other axons (besides the Corticospinal Tract) in the Corona Radiata, Internal Capsule and Cerebral Peduncle travelling to other destinations too (e.g. numerous Thalamacortical and Corticothymic Axons in the Internal Capsule) o In contrast, all of the Axons in the Pyramid relate to the Corticospinal Tract At the bottom of the Pyramid, ~80-90% of the Axons of the Corticospinal Tract will cross to the other side via the Motor (or Pyramidal) Decussation o The Axons that cross are referred to as the Lateral Corticospinal Tract These will descend the spinal cord to the Lateral Funiculus and synapse mainly with Alpha-motor neurons (though a small proportion will synapse with Gamma-motor neurons) o The Axons that do NOT cross are referred to as the Ventral Corticospinal Tract These will descend the spinal cord, but most of these Axons will then cross to the other side anyway in the spinal cord via the Ventral White Commissure (which is also where the Spinothalamic Tract crosses too) and synapse mainly with Alpha-motor neurons (though a small proportion will synapse with Gamma-motor neurons) o Note: The Alpha-motor neurones will innervate all musculature, but uniquely is the only tract that innervates the digits Rubrospinal Tract This tract originates from the Red Nuclei in the Midbrain of the Brainstem and will cross to the contralateral side at the Midbrain o The Rubrospinal Tract will then descend down the spinal cord and synapse with the Alpha-motor neurons Rubrospinal Tract is relatively small in humans and will act mainly to assist / support the Corticospinal Tract in its own function Identify the signs and symptoms for lesions of each major white mater tract - Dorsal Column Tract – Loss of ipsilateral touch / vibration sensation and conscious proprioception Spinothalamic Tract – Loss of contralateral pain / temperature sensation (as the Tract will cross sides lower down at the Ventral White Commissure) Spinocerebellar Tract – Loss of ipsilateral unconscious proprioception (which is difficult to clinically examine, as we can only examine conscious proprioception) - 9 - Vestibulospinal Tract – Loss of posture / balance and body lateropulsion (i.e. tendency to fall towards the side of the lesion of the Vestibulospinal Tract) Reticulospinal Tract – Loss of visceral control if there is a bilateral lesion of the Reticulospinal Tract), although a unilateral lesion is more difficult to identify (and will tend to resolve by themselves) Corticospinal Tract – Loss of voluntary ipsilateral movements (especially loss of hand / finger movements) (assuming lesion is below the Pyramids of the Medulla) Rubrospinal Tract - Inhibition of ipsilateral movement on the same side as the lesion SPINAL CORD 3 – DYSFUNCTIONS AND DEFICITS Describe the different types of sensory and upper and lower motor neurone lesions (and associated signs and symptoms) - Sensory lesions can be either central vs. peripheral o Whilst pain from a peripheral lesion can be sharper than pain from a central lesion, it is usually quite difficult to distinguish between a central vs. peripheral sensory lesion o Instead, motor examination (rather than sensory examination) is more effective at identifying if a lesion is central vs. peripheral There are two types of symptoms that occur following a sensory lesion: o Positive Symptoms – this involves abnormal sensations (e.g. tingling, pins and needles, burning, ‘phantom’ sensations) o Negative Symptoms – this involves loss of sensation o Note: Positive sensory symptoms commonly will precede negative sensory symptoms, and may be triggered by ischaemia, stretching or placement of pressure on the nerve o Note: ‘Phantom’ sensations involve the patient feeling severe pain in the limb / structure that is amputated This can occur as the Cortex has a pre-existing visual map of the peripheries (including the location of the absent limb / structure) it can take up to ~20 years for the Cortex to remap the body and realise the limb / structure is absent! If nerve endings at the point of amputation regrow, the signals sent from these nerves will be incorrectly interpreted by the Cortex (which can trigger the ‘phantom’ pain sensation in the amputated limb!) ‘Upper Motor Neuron’ refers to the CNS, whilst ‘Lower Motor Neuron’ refers to the PNS o Lower Motor Neuron lesion (i.e. Peripheral Motor Lesion) can result in: Paralysis / weakness Areflexia (i.e. lack of reflexes) (though incomplete lesion will only result in a diminishment [rather than absence] of reflexes) Atonia / flaccidity (due to lack of Stretch Reflex to maintain Muscle Tone) Atrophy (due to the lack of long-term usage of the muscle) Fasciculations / fibrillations (i.e. spontaneous firing of motor neuron [due to the damage to the neuron] resulting is small movements) o Upper Motor Neuron lesion (i.e. Central Motor Lesion) can result in: Paralysis (and if the Corticospinal Tract is affected, this will result in loss of skilled movements [i.e. ‘Clumsy Hand’]) Hyperreflexia (i.e. exaggerated reflexes, Clonus, Babinski’s Sign) This occurs due to the lack of Descending Supraspinal control to switch off / stop the reflex Note: Babinski’s Sign will occur in children under two years of age as their Corticospinal Tract is NOT fully myelinated and has not reached to the bottom of the Spinal Cord Spasticity (i.e. stiffness / contraction of muscles / limbs) This occurs due to the lack of Descending Supraspinal control to switch off the Stretch Reflex This typically develops ~2-3 weeks after the spinal / brain trauma and will particularly affect anti-gravity muscles (e.g. flexors of upper limb, extensors of lower limb and plantar-flexors) - - 10 Note: Spasticity can be relieved by stretching the tendon the muscle (as this triggers the Golgi Tendon Reflex, which will result in the muscle relaxing) Describe the common spinal cord deficits and their patterns of sensory and motor loss - Spinal Shock occurs following trauma / insult to the Spinal Cord, resulting in the immediate loss of reflexes (both somatic and visceral) below the level of the trauma o The loss of somatic reflexes has a similar impact / signs to a lower motor neurone lesion (e.g. paralysis, areflexia, fasciculations, etc.) o The loss of visceral reflexes will have different impacts depending on the level of the lesion (e.g. lesions T5-6 and below will not have cardiovascular impacts [but can have other impacts such as lack of Micturition], whilst lesions T4 and above will reduce blood pressure and heart rate due to loss of sympathetic stimulation to blood vessels and SA Node) o Passing Tracts are only affected by Spinal Shock IF they are a part of the lesion (otherwise, they will NOT be affected by the Spinal Shock) Spinal Shock occurs immediately following injury / insult to the Spinal Cord and may last between 1 hour to 6 weeks, though the average / norm is 2 weeks o Reflexes will gradually return over time, with the Visceral Reflexes typically returning prior to the Somatic Reflexes Autonomic Dysreflexia can occur in the first 12 months after Spinal Shock has finished o This will only occur after a complete Transection of the Spinal Cord (most commonly in the Cervical Spinal Cord or in the Upper Thoracic Spinal Cord [above T5-6] This results in half the body being controlled by the Sympathetic Nervous System, with the other half the body being controlled by the Parasympathetic Nervous System o Signs and symptoms are very visible and result from excessive sympathetic stimulation (e.g. headaches, sweating, goose-bumps and episodic excessive hypertension [i.e. BP > 200]) This is a severe condition that can result in death (mainly due to the excessive hypertension) The following spinal cord deficits may occur and may have the following patterns of sensory and / or motor loss: o Left Hemisection of Spinal Cord at T10 – Loss of ipsilateral tactile, contralateral pain and temperature and ipsilateral upper motor neurons signs all below the Umbilicus o Complete Transection of Spinal Cord at T1 – Loss of all sensation below the level of T1 bilaterally with loss of abduction / adduction of both hands (due to damage to peripheral nerves based at T1) and bilateral upper motor neuron signs below the level of T1 o Cauda Equina – Loss of all sensation and lower motor neuron signs below T12 bilaterally o Damage to the Ventral White Commissure across C4 to T3 due to Syringomyelia – bilateral loss of pain / temperature sensation and lower motor neuron signs across C4 to T3 Dermatomes (note: damage to ventral horn will result in lower motor neuron signs) - - - Describe the suspected mechanism behind spinal shock and autonomic dysreflexia - The mechanism for Spinal Shock is unclear o One particular hypothesis is that the spinal injury / trauma will result in cell damage, and that the neurons will take a couple of weeks to re-establish their synaptic connections (hence, the reflexes will return after a short period) o Another hypothesis is that inhibitory neurons are hyperactive immediately following spinal injury / trauma The mechanism for Autonomic Dysreflexia is unclear / unknown; one particular hypothesis is: o Pain stimuli (e.g. full bladder, gas in bowel, etc.) will travel to the Spinal Cord and trigger sympathetic stimulation o Normally, the sympathetic response would result in a signal in the ascending pathway towards the brain - 11 o o o However, the complete transaction prevents this signal from reaching the brain The sympathetic stimulation will result in vasoconstriction and eventually hypertension; this will result in the baroreceptors signalling to the brain there is excessive blood pressure However, the brain is unable to respond by sending signals via the descending pathway to cease sympathetic stimulation (due to the complete transaction) and instead compensates by reducing the heart rate and vasodilating all blood vessels above the transaction Note: The brain is unable to specifically switch off / stop sympathetic stimulation (and instead needs to act through alternative pathways) this is unsustainable in the long-term and can eventually result in mortality SPINAL AUTONOMIC ORGANISATION Identify the structural and functional organisation of autonomic neurones in the spinal cord - There are three divisions of the Autonomic Nervous System (ANS) o Sympathetic Nervous System (SNS) – this will have their preganglionic neurons within the Thoracic and Upper Lumbar segments of the spinal cord o Parasympathetic Nervous System (PNS) – this will have their preganglionic neurons within the Brainstem and Sacral segment of the spinal cord o Enteric Nervous System – this is within the gut and is very important (there are more neurons in the Enteric Nervous System than the entire spinal cord) o Note: Postganglionic Neurons typically have their cell bodies within the Ganglia Most of the sympathetic preganglionic neurons will be located in the Intermediolateral Nucleus (IML) of the Spinal Cord o Axons of these sympathetic preganglionic neurons can take three different pathways after emerging from the Vertebral Canal via the Ventral Root Option 1 involves terminating in the adjacent pre-vertebral ganglion in the Sympathetic Chain The preganglionic axon will synapse with the postganglionic neuron here The postganglionic neuron will send its own postganglionic axon via the Gray Ramus towards the mixed nerve (which travels to its target) Option 2 involves travelling up or down the Sympathetic Chain and synapsing with a ganglion at another spinal level Option 3 involves travelling via the Sympathetic Chain towards the target organ where it will synapse with this para-vertebral ganglion o Note: Parasympathetic Ganglia are generally very close to the target organ of innervations (rather than being closer to the spinal cord like Sympathetic Ganglia) There are sub-populations of preganglionic neurons, each of which controls a particular type of effector (e.g. blood vessels, heart, smooth muscle in gut, lungs etc., pupillary muscle, piloerector muscles, sweat glands, salivary glands etc) o There are also sub-populations within each major group (e.g. those that innervate blood vessels in skin are separate from those that innervate blood vessels in skeletal muscle, kidney etc.) o These different sub-groups can be independently controlled by inputs from spinal afferents or descending inputs from brain nuclei - - Describe the mechanisms by which autonomic neurones integrate excitatory and inhibitory inputs from peripheral receptors and centres in the brainstem and hypothalamus - Sympathetic preganglionic neuron (SPN) receives both excitatory and inhibitory synaptic inputs o Main excitatory neurotransmitter is Glutamate, and main inhibitory neurotransmitter is GABA Inputs to autonomic neurons are from spinal afferents, or descending inputs from brainstem and hypothalamus - 12 o - Preganglionic neurons receive inputs at the same spinal level (most of the time) from afferent fibres that enter from the Dorsal Root However, there is not a direct synapse between these afferent fibres and the Preganglionic Neurons Instead, inputs from Spinal Afferents to the Preganglionic Neuron will only be via an Interneuron (rather than directly synapsing) o Supraspinal inputs (i.e. descending inputs) to Preganglionic Neurons can be directly or indirectly (via either an excitatory and / or inhibitory interneuron) Sympathetic Preganglionic Neurons will receive direct supraspinal inputs from five distinct areas of the brain Three of these distinct areas are within the Medulla (i.e. Caudal Raphe Nuclei [which are midline], Ventromedial Medulla [more lateral] and Rostral Ventrolateral Medulla [most lateral]) One of these distinct areas is in the Pons (i.e. A5 Cell Group) One of these distinct areas is in the Hypothalamus (i.e. Paraventricular Nucleus) Note: Whilst there are other inputs from other parts of the brain, these are indirect inputs and must travel via one of the above five distinct pathways Tonic sympathetic stimulation of skin and muscle will be lost in a spinal cord injury due to loss of descending supraspinal input o However, there can still be reflex activation of the sympathetic nerve from inputs from Spinal Afferents CENTRAL NERVOUS SYSTEM FUNDAMENTALS OF CNS DEVELOPMENT Describe the main stages in the development of the CNS, including the development and differentiation of the neural tube - There will be a trilaminar embryo at Day 18 (Ectoderm, Mesoderm, Endoderm) o Ventral side of Ectoderm will develop into Skin, whilst Dorsal side of Ectoderm (i.e. Neural Plate) will develop into the Nervous System The differentiation into skin vs. nervous system is dependent on the level of signalling from the Bone Morphogenic Proteins (BMP) (i.e. higher signalling from BMPs results in skin, whilst lower signalling from BMPs results in Nervous System) o The Rostral end of the Neural Plate will ultimately develop into wider structures such as the Cortex, whilst the Caudal end of the Neural Plate will ultimately develop into narrower structures such as the Spinal Cord Development of a Neural Tube is a way to protect the highly sensitive Central Nervous System from damage (by surrounding the Central Nervous System / Spinal Cord by protective layers) ‘Notochord’ is a derivative of the Dorsal Mesoderm and is located in the midline deep to the Neural Plate o This plays an important role in the development of the nervous system via the release of a signalling molecule (Sonic Hedgehog [Shh]) In the first stage of Neurulation, the Neural Plate will invaginate downwards (following the Notochord) to form the Neural Groove o The edge of the Neural Plate will fold upwards, whilst the Neural Folds will bend and develop into a crest-like shape (at which point they will be known as the Neural Crest) In the second stage of Neurulation, the lateral borders of the Neural Plate will come together at the midline and fuse to form a continuous Neural Tube (which will eventually develop into the CNS) o The cells that constituted the Neural Folds will shift downwards on either side of the Neural Tube and become Neural Crest Cells (which will eventually develop into the PNS) Fusion of the lateral borders of the Neural Plate to form a Neural Tube occurs initially at the lower cervical areas and then extends both Rostrally and Caudally - - - - 13 o - - - - - The final parts of the Neural Tube to close are the Rostral and Caudal Neuropores (i.e. Rostral and Caudal ends of the Neural Tube); this occurs at Day ~24-26 and Day ~26-28 respectively o Failure of the Rostral Neuropore to close will result in the failure of the structures of the forebrain to differentiate this is labelled Anencephaly (which is typically fatal!) o Failure of the Caudal Neuropore (i.e. Spina Bifida) to close is more common than failure of the Rostral Neuropore (i.e. Anencephaly) to close The different vesicles / bumps of the Neural Tube will differentiate into different parts of the CNS o Prosencephalon will develop into the forebrain; this will separate into the: Telencephalon, which develops into the Cortex, Hippocampus, Amygdala, etc. Diencephalon, which develops into the Thalamus, Hypothalamus, Epithalamus and Dorsal Thalamus (as well as the Optic Cup from the outcropping from the Diencephalon) o Mesencephalon will develop into the Midbrain o Rhombencephalon will develop into the hindbrain; this will separate into the: Metencephalon, which develops into the Pons and Cerebellum Myelencephalon, which develops into the Medulla o Note: The different vesicles / bumps are not vertically in a line, but rather curved in the embryo o Note: These different vesicles / bumps will develop into the different Ventricles of the Brain The Notochord releases the signalling molecule Sonic Hedgehog (Shh) onto the Neural Plate o The impact of this signalling molecule is dose dependent, and so it will have its biggest impact on the midline of the Neural Plate (i.e. next to the Notochord) o Higher levels of Sonic Hedgehog (Shh) will signal to that tissue it is Ventral and hence induce the development of structures associated with the Ventral part of the Nervous System [e.g. Motor Neurons]) In contrast, high Bone Morphogenic Protein (BMP) will signal to Ectoderm tissue is should develop into skin o Lower levels of BMP will result in the Ectoderm developing into Neural Tissue (but this Neural Tissue will have special properties that induce the development of structures associated with the Dorsal part of the Nervous System [e.g. Sensory Neurons]) Neuroepithelial Stem Cells undergoing constant rounds of mitotic division, resulting in an exponential increase in the number of Neuroepithelial Stem Cells (i.e. ‘Neurogenesis’) o Eventually, a critical point will be reached at which these Stem Cells differentiate into Radial Glia Cells These Radial Glia Cells have long, thin processes that attach to both the superficial and deep surfaces Postmytotic Neurons that develop in the deep region will climb up the Radial Glia cells to migrate to the superficial surface These Postmytotic Neurons will then form a layer of cells superficial to the Ventricular Zone (VZ) called the Mantle Zone (MZ) Subsequent Postmytotic Neurons will form a layer deeper to the initial Mantle Zone layer of cells (though these more immature Postmytotic Neurons will still be part of the Mantle Zone) Note: The above pattern applies to MOST of the CNS (though the Cerebral Cortex and Cerebellum have their own pattern of development) o Note: All Neuroepithelial Stem Cells will be attached to both the deep and superficial surface! The Axonal Growth Cone of the Axon will provide the guidance for the Axon to direct it towards its target o There are sensory receptors on the Axonal Growth Cone that will detect the various signalling molecules o Based on the type of signalling molecule detected, the Axonal Growth Cone will either be attracted to or repelled from a particular direction (and hence its growth ultimately directed towards the target) There are typically many Intermediate Points to where the Axon will be attracted to in its long path towards the target 14 - - - - - Once the Axon reaches an intermediate point, the body will respond by either down-regulating the receptors that resulted in the growth to that Intermediate Point or activating a different receptor that is attracted to the next Intermediate Point This will result in the Axon now being directed towards the next Intermediate Point rather than the Intermediate Point already reached o Note: ‘Adhesion Substrate’ (e.g. fibronectin, laminin, etc.) is needed for the machinery of the Axonal Growth Cone to function In the process of CNS development, some Axons may incorrectly reach the incorrect target o However, this is a not a major problem if this only occurs in small numbers due to the process of Neuronal Death o ~30-50% of Neurons will undergo Neuronal Death (i.e. Pruning), which will enable the elimination of incorrectly directed and excessive Axons The survival vs. death of neurons is dependent on the ability of the individual neuron to pick up Neurotrophic molecules (e.g. Neurotrophin) o Neurotrophin is secreted by the target structure in limited quantities (though the quantity is sufficient to enable the required number of neurons for that structure to survive) Neurons with an increased ability to drive activity (i.e. make the post-synaptic structure fire) will preferentially attract these Neurotrophin o The Neurotrophin will travel retrogradally across the synapse and is taken up by the terminals of the neurons The Neutrotrophin will then travel back to the cell bodies of these Neurons and activate intracellular programs that promote cell survival The precise part of the target structure innervated by Neurons is dependent on the identity of the Neuron (rather than the location of Neuron) o This occurs as there is a map of the different receptors / target structures in the brain o The brain will seek to continue innervating the different receptors / target structures with the original Neurons as per this map (even if the location of the original Neuron changes) The maps indicating which neurons innervate which precise parts of the target structure are dependent on chemical signals o The identity of the neuron is influenced by the levels of receptors expressed by the Axonal Growth Cone (e.g. more receptors = Ventral Retina) o The precise part the target structure innervated will be dependent on the levels of Ligand expressed in the target structure (whereby the Ligand is associated with specific receptors) o Differences in the gradients of ligands will preferentially attract or repel Axons from innervating particular areas of the target structure ‘Refined Projections’ from a Neuron are much more dense and directed towards a smaller area o This will be more effective at driving the post-synaptic cell (compared to ‘Exuberant Projections’, which loosely target lots of cells) o Progressive refinement of projections will result in segregation of the inputs from the eyes Refinement of the projections will be dependent on the level of activity (i.e. if synapses are NOT used, neighbouring synapses may branch and ‘take over’ more territory for innervation NORMAL AND ABNORMAL DEVELOPMENT OF THE CNS Describe normal brain development and factors that interfere with brain development - Neurulation (i.e. development of Neural Tube) will occurs in Week 4 of development o 18 days after conception the embryo consists of 3 layers of cells Thickening of the Ectoderm in the midline leads to the development of the Neural Plate o 20 days the Neural Plate forms a deep Neural Groove o 22 days the Neural Groove has closed in the middle region to form the Neural Tube (but it is still open at either end) 15 o The Rostral opening / Neuropore closes on days 25-26, and the Caudal Opening / Neuropore on day 27-28 Describe the significance of prenatal exposure to environmental agents in the development of the CNS - Women who take >400 μg of folic acid / day, for at least 3 months before conception, decrease the probability their foetus will have a Neural Tube Defects by 70%–80% First trimester use of anticonvulsants Valproic Acid or Carbamazepine increases the probability of Spina Bifida about ~5-10x (note: this increased risk is not decreased by Folic Acid) Pre-pregnancy obesity (BMI >29) increases increase the probability of Spina Bifida about ~1.5-3.5x (note: this increased risk is not decreased by Folic Acid) Exposure to large quantities of alcohol (>8 drinks / day) can result in Foetal Alcohol Syndrome (FAS), which is associated with brain malformations, cognitive impairment / mild mental retardation, other organ malformation and characteristic facies (e.g. microcephaly, smooth philtrum, short palpebral fissures, etc.) - Describe the formation of a myelomeningeocele and anencephaly - Anencephaly results from the failure of closure of the Rostral / Anterior Neuropore o All the exposed brain tissue will degenerate such that whilst children with Anencephaly will live to birth, they will die soon after birth Spina Bifida results from the failure of closure of the Caudal / Posterior Neuropore o Children with Spina Bifida will live into adulthood and have a reasonable life expectancy Failure of the Neural Tube to close in Spina Bifida Cystica (i.e. Myelomeningocele) will result in the failure of Vertebrae and Epidermis to form on the Dorsal side of the Spinal Cord (as this will only develop on the dorsal side when the Neural Tube closes!) o The Central Canal will open into the Neural Placode (i.e. open part of the Neural Tube) resulting in the leakage of CSF and exposure of the Ventricular System to the outside world (i.e. no Blood-Brain Barrier) o There will be significant damage to the spinal nerves / spinal cord at the point of the Neural Placode (which typically results in the loss of nerve supply to the lower limbs [i.e. paraplegia], bladder and bowel) Note: Spina Bifida Occulta is relatively common (~10% of individuals) and usually occurs in the Lumbosacral region o This involves the Mesoderm failing to develop all the way around the Spinal Cord (when it should be able to, as the Neural Tube has closed) o As a result, there is failure of a Vertebrae to fully close around the spinal cord - - Describe the effects of abnormalities in the production, circulation and absorption of cerebrospinal fluid, with particular reference to hydrocephalus - The 4th Ventricle is continuous with the Central Canal o However, there is only a small amount of circulation down the Central Canal (as there is no pathway for CSF to leave the CSF except back through the 4 th Ventricle) o Instead, most CSF will leave the 4th Ventricle via the Foramen of Magendie and the Foramina of Luschka o Hence, blockage of CSF drainage via the Foramina of Magendie and Luschka will result in build-up of CSF in the Ventricles and hence Hydrocephalus Infants with untreated Hydrocephalus would have their head grow bigger and bigger as it became full of additional CSF o This expansion of the head is possible as the bones of the cranium are NOT fused in a newborn infant o However, the larger the build-up of CSF (and hence the size of the head), the greater the damage to the brain tissue - 16 o - - - Current treatment involves inserting a Ventriculoperitoneal Shunt (diverting the excess CSF from the Ventricles to the Peritoneal cavity) Complications can include blockage of the shunt and / or infection of the shunt Spina Bifida Cystica (i.e. Myelomeningocele) is often associated with Chiari Type II Malformation o Due to the CSF leakage from the Neural Placode, there is lack of CSF fluid/ pressure in the Ventricular System this results in the brain failing to expand o As a result, the size of the Posterior Fossa of the Cranium does not develop into the required size (i.e. the size is too small!) o When the Cerebellum then develops later (at ~Week 20 onwards), there is insufficient space in the Posterior region of the skull, which results in the Cerebellum pushing down into the Foramen Magnum o This will result in the Cerebellum pushing against the Brainstem and blocking drainage of the CSF from the Ventricles (which normally occurs from the 4th Ventricle to the Sub-Arachnoid Space via a pathway between the Cerebellum and Brainstem) Whilst this is not a problem when there is still an open leak of CSF from the base of the spine, this will become problematic once the open leak is sealed The equilibrium will be disturbed by the closure of the leak and will be a build-up of CSF in the cranium (resulting in Hydrocephalus!) ~5-10% of patients with Spina Bifida Cystica (i.e. Myelomeningocele) will NOT develop Hydrocephalus o As a result, a Ventriculoperitoneal Shunt is not inserted until there is evidence there is Hydrocephalus (which is gathered by regularly measuring the head circumference of the newborn baby) o This will avoid having to insert the lifelong shunt (which can potentially result in complications such as becoming infected) Alternative treatment for Myelomeningocele is pre-natal surgical repair in-utero o The theory is that closure of the Neural Tube earlier will increase the pressure of the CSF to the normal level earlier o This will result in the Posterior Fossa growing faster (and hence being able to accommodate the later growing Cerebellum) However, Prenatal Surgery will NOT prevent / avoid damage associated with the open neural tube (as this has already occurred) nor the brain damage that has already occurred There are considerable negative side-effects (e.g. risk of uterine rupture, exposure of mother to extensive surgery, increased rates of pre-term birth, etc.) o The advantage of Prenatal Surgical repair of Myelomeningocele is that it will reduce the need for Ventriculoperitoneal Shunts (which are high-maintenance and may still result in early mortality [i.e. 20% of children with Spina Bifida Cystica will die before reaching age 21]) SECRETION AND ABSORP TION OF THE CSF Identify the anatomy and physiology of cerebrospinal fluid secretion, circulation and absorption - CSF is an ultrafiltrate of Plasma; this process of filtration can be assisted via Energy Dependent Mechanisms and / or Facilitated Diffusion o CSF has a low protein content (due to BBB), high Cl- content and high water content as well as minimal levels of both White Blood Cells and Red Blood Cells o CSF provides a range of different functions such as reducing effective weight of brain to <50g, providing a constant environment for Neurons and Glia, removing extracellular metabolites, etc. CSF is found inside the Ventricular system of the brain and in the subarachnoid space outside the brain and spinal cord o Ventricular System of Brain consists of Lateral Ventricles, 3rd Ventricle and 4th Ventricle Each Lateral Ventricle will join to the midline 3rd Ventricle via the Foramen of Monro The 3rd Ventricle will then join to the 4th Ventricle via the Aqueduct of Sylvius The 4th Ventricle will then have three inferior openings (i.e. Foramen of Magendie in the middle, and Foramina of Luschka on either side) - 17 o - - - - There is a total volume of ~120-150mL of CSF in the body Lateral Ventricles will have ~25mL 3rd and 4th Ventricles will have ~5mL Sub-Arachnoid Space in the Cranium will have ~25mL; and Sub-Arachnoid Space around the Spinal Cord will have ~75mL of CSF CSF is produced mainly in the Choroid Plexus (~80%), but also the Ependyma o The Choroid Plexus is present in the 3rd and 4th Ventricles, as well as the Body and Temporal Horn of the Lateral Ventricles o There is a turnover of CSF of >3x per day (given daily production is ~500mL whilst total CSF is ~150mL) CSF Absorption is a pressure dependent process (i.e. requires a pressure gradient to drive absorption) o CSF Absorption occurs mainly via the Arachnoid Villi, but also via the Nerve Root sleeves and from the Parenchyma o Arachnoid Villi extend from the Subarachnoid Space (i.e. location of CSF) into the inner layer of the Dura Mater (i.e. location of blood / Venous Sinuses) Hence, this will connect the CSF towards and blood, thus enabling the absorption of CSF back into the blood Given CSF secretion is constant compared to CSF absorption which is pressure-dependent, there may be a mismatch / imbalance in the volume of CSF depending on the intracranial pressure o Note: CSF Pressure will change with every breath and every heart beat (as this changes cerebral blood flow and hence intracranial pressure) CSF Pressure should be measured at different locations depending on the position of the patient (i.e. measure in middle of back / spine for supine patients vs. near the ear for erect patients) Describe common CSF circulation disorders such as hydrocephalus and idiopathic intracranial hypertension - Common CSF Circulation Disorders include: o Hydrocephalus (i.e. increased CSF volume) This is a condition characterised by a dynamic imbalance between the production and absorption of spinal fluid that results in an increase in the size of the Ventricles within the brain This can be congenital vs. acquired, high vs. normal vs. low pressure or obstructive vs. communicating Note: Most Hydrocephalus will involve an Obstruction (rather than being Communicating [which could indicate a problem with absorption of CSF]) Acute Hydrocephalus will involve raised intracranial pressure -- > the cardinal symptoms of raised intracranial pressure are: Headache, Nausea, Vomiting, Lethargy, Drowsiness / Loss of Consciousness as well as Papilloedema and ‘Setting Sun’ sign (i.e. downward direction of the eyes) o Idiopathic Intracranial Hypertension (also known as Pseudotumour Cerebri) (i.e. increased CSF pressure [in the absence of an increase in CSF Volume or a mass lesion]) o Intracranial Hypotension (i.e. decreased CSF pressure / volume) o Meningitis / Ventriculitis (i.e. CSF space inflammation) Repair of Myelomeningocele (i.e. failure of caudal neural tube to close resulting in open Neural Placode) can initially cause accumulation of CSF as the body has not developed the mechanisms to absorb the CSF in sufficient quantities (as instead the CSF simply leaked from the open wound) o If the drain / shunt is not introduced, there is a high risk of Hydrocephalus o These children will commonly have a Chiari malformation whereby the Cerebellar Tonsils are displaced downwards into the top of the Spinal Canal) This also increases the risk of Hydrocephalus (as the pulling of the Cerebellum and Medulla through the Foramen Magnum can compress these structures resulting in blockage / closure of the Foramen of Magendie and / or Foramina of Luschka Note: There is limited ability to compensate for increased volume in the cranium (due to the rigidity of the skull and the lack of compressibility of the brain, blood and CSF) this is referred to as the ‘Munro-Kellie Doctrine’ - - 18 o o Whilst the body will attempt to compensate, increases in volume beyond a certain point will result in a rapid increase in intracranial pressure (which will eventually cause brain damage /death!) In contrast to adults, babies (~<1 year) will not have had their skull bones fuse together yet, so there is increased ability to compensate for additional volume (resulting in the size of the head significantly increasing) Describe the application CSF anatomy and physiology to the common treatment modalities for these conditions - Main treatment for Hydrocephalus is ‘CSF Shunting’ (i.e. insert tube that shifts CSF away towards a different location [e.g. Peritoneum, Atrium, Pleura]) o There is commonly a valve on the Shunt to regulate the amount of CSF ‘shunted’ ‘Third Ventriculostomy’ is another available treatment that involves creating a bypass from the Third Ventricle towards the Sub-Arachnoid Space (and hence circumvent any obstruction below the Third Ventricle) o Similarly, ‘Aqueductoplasty’ involves inserting a hole into the obstructed Aqueduct of Sylvius (thus re-enabling flow of CSF via the Aqueduct to the 4th Ventricle) Acetazolamide inhibits Carbonic Anhydrase (important enzyme for CSF production) and hence will decrease CSF production by ~30% (and hence reduce the CSF Pressure) ‘Lumbar Punctures’ can be utilised to reduce the level of fluid (and hence reduce the CSF Pressure) ‘Bilateral Subtemporal Decompressions’ involve drilling a hole on either side of the skull to create a little bit more room for the brain ‘Venous Sinus Stenting’ involves placing a stent in the Venous Sinus to reduce the resistance and hence pressure in the Venous Sinuses o This will result in increased CSF Absorption (as this is dependent on the pressure gradient between the Sub-Arachnoid Space and Venous Sinus) ‘Optic Nerve Sheath Fenestrations’ involve making small holes in the Optic Nerve Sheath to provide a pathway for CSF to escape o This does not necessarily reduce the intracranial pressure, but can help protect the patient’s eyes (especially important in Idiopathic Intracranial Hypertension) - - - IMAGING THE BRAIN Identify structures of the central nervous system as seen on radiographic images - Different features that can be identified on CT Scan include: o Extradural Haemorrhage – this will result in a convex hyperdensity area (i.e. ‘egg-shape) o Subdural Haemorrhage – this will result in a concave area (i.e. ‘crescent shape’) that may be hypodense or hyperdense o Subarachnoid Haemorrhage – this will result in Sulcus spaces within the brain being enhanced (due to the presence of additional blood) o Intracranial Haemorrhage – this will result in hyperdense area (due to blood) surrounded by a hypodense region (reflecting oedema around the haemorrhage) Acute bleeding in the brain will be Hyperdense, but this will gradually change over ~2-4 weeks to initially shift to Isodense and then Hypodense o This change in density occurs as proteins and products from the blood are eventually reabsorbed from the CSF - Describe particular radiographic modalities for brain imaging and their utility - The radiographic modalities available for brain imaging include: o CT Scan Advantages Excellent spatial and soft tissue resolution 19 o Rapid image acquisition Readily available Disadvantage Substantial radiation dose Lower quality images compared to MRI Scan MRI Scan Advantages Higher quality images compared to CT Scan No radiation dose Disadvantages Lack of accessibility Longer time for image acquisition SEIZURES AMINO ACID NEUROTRAN SMISSION Describe the functions of different neurotransmitters (excitatory vs. inhibitory) in the CNS - The major neurotransmitters in the brain are Glutamate and GABA (i.e. they account for ~90% of Neurotransmission in the Central Nervous System) o ~50% of neurons release Glutamate as an excitatory neurotransmitter o ~30-40% of neurons release GABA as an inhibitory neurotransmitter Glutamate is an acidic molecule in structure, highly abundant throughout the brain and acts as a excitatory neurotransmitter o Glutamate will result in the post-synaptic neurone being selectively permeable to positive ions (which will depolarise the post-synaptic neuron) o The quantity of Glutamate in the Synaptic Cleft is regulated by Transporters (which are present in Glial or Astrocyte cells), which can remove the amount of Glutamate in the Synaptic Cleft This Glutamate will be degraded to Glutamine and recycled back into the presynaptic neuron (where it is converted back to Glutamate and repackaged into the Synaptic Vesicles) GABA is synthesised from Glutamate itself (in the presence of the enzyme Glutamate Decarboxylase)and is similar in structure o However, the differences in structure are such that it is an inhibitory (rather than excitatory) neurotransmitter o GABA is highly abundant in a wide variety of interneurons and projection neurons ‘Excitotoxicity’ refers to excessive activation of Glutamate receptors ultimately resulting in cell death o This can be triggered by Ischaemia in the brain (as the resultant lack of ATP will result in the depolarisation of the cell membrane, and hence excessive electrical signalling [and thus excessive Glutamate release]) o Excessive Glutamate release will trigger excessive Ca2+ influx at the Post-Synaptic Terminal, which will result in activation of proteases, lipases, etc. that will cause cell death o Excitotoxicity is believed to lead to Stroke and Neurodegenerative Conditions (e.g. Alzheimer’s Disease, Parkinson’s Disease) in the long-term (though excessive Glutamate release may also trigger Convulsions in the short-term too) - - - Describe the functions of different neuroreceptors (fast vs. slow, excitatory vs. inhibitory) in the CNS - Glutamate will achieve its effects on neighbouring neurons by activating Ionotropic and Metabotropic Receptors specific for Glutamate 20 o - - Ionotropic Receptors will open an intrinsic ion pore when activated (which allow passage of Na+ and Ca2+ ions); there are two types of Ionotropic Receptors activated by Glutamate; these are: NMDA Receptors These receptors consist of four subunits (i.e. two NR1 subunits and two NR2 subunits) the type of subunits will dictate the properties of the receptor These receptors require Glycine to be a co-agonist (in addition to Glutamate) to activate the receptor This receptors has a resting Magnesium block (i.e. there is a Mg2+ ion blocking the ion pore in its resting state) These are slow-acting receptors AMPA Receptors These receptors consist of four subunits These receptors do NOT require Glycine to be a co-agonist (in addition to Glutamate) to activate the receptor These are fast-acting receptors Note: AMPA Receptors are smaller than NMDA Receptors Note: The resting Magnesium block of NMDA Receptors will not be removed even if there is binding of Glutamate and Glycine However, local depolarisation of the membrane from the opening of an adjacent AMPA Receptor will expel the Mg2+ ion from the ion pore of the NMDA Receptor (and hence open up the NMDA Receptor) NMDA Receptors are able to generate a larger electrical signal compared to AMPA Receptors (although AMPA Receptors are needed to remove the resting Magnesium block of NMDA Receptors) o Metabotropic Receptors will activate G-Proteins, which then trigger secondary signalling cascades that result in the end impact There are three main classes / subtypes of Metabotropic Glutamate Receptors All three classes are present on the post-synaptic terminal, whilst only Class II and III are present on the pre-synaptic terminal mGluR I trigger excitatory signals in contrast to mGluR II and III which trigger inhibitory signals (e.g. inhibit influx of Ca2+ on the pre-synaptic membrane) NMDA Receptors can trigger Long-Term Potentiation (i.e. Neuronal Plasticity), as it will allow the inflow of Ca2+ ions at the post-synaptic terminal that will ultimately increase the number of AMPA Receptors present on the Post-Synaptic Membrane o This increase in the number of AMPA Receptors will result in the generation of a stronger signal when Glutamate is released in the future GABA will achieve its effects on neighbouring neurons by activating the Ionotropic GABA-A Receptors and / or the Metabotropic GABA-B Receptors o GABA-A Receptors consist of five protein subunits around a central ion pore Each subunit consists of four Transmembrane Domains (whereby the 2 nd Domain will line the central ion channel pore) Whilst there are theoretically numerous different arrangements of the multiple GABA-A Receptor subunits, 85% of GABA-A Receptors will contain one of three particular combinations or Alpha, Beta and Gamma subunits This occurs as only certain sub-units can actually coexist, and so the actual number of combinations of sub-units is much less than the theoretical number of combinations Activation of these GABA-Receptors will allow passage of Cl- ions (and hence will make the post-synaptic terminal hyperpolarised [i.e. more negative]) Describe mechanisms of neurotransmitter release, the activation and inhibition of neuroreceptors and the removal of neurotransmitter from the synapse in generating a post-synaptic response 21 - - - Neurotransmitter release can be triggered from an Action Potential reaching the pre-synaptic terminal o The electrical signal (i.e. Action Potential) will reach the Pre-Synaptic Terminal where it will trigger an inflow of Ca2+ ions (which triggers the fusion of Synaptic Vesicles with the cell membrane itself) o The Synaptic Vesicles will release their contents (i.e. Neurotransmitter) into the Synaptic Cleft o The Neurotransmitters will diffuse across the Synaptic Cleft, where it will then react with proteins on the Post-Synaptic Terminal The impact of GABA neurotransmission can be enhanced by: o Increasing receptor activation (e.g. via Benzodiazepines, Barbiturates, Alcohol, Neurosteroids, General Anaesthetics) o Increasing GABA levels (by blocking reuptake of GABA via Tiagabine or Nipecotic Acid) o Inhibiting GABA metabolism (e.g. via Vigabatrin which inhibits the enzyme GABATransaminase, and thus increases the amount of GABA present in the pre-synaptic vesicle [by preventing the breakdown of GABA into Succinic Acid]) The impact of GABA neurotransmission can be antagonised by Bicuculline ANTICONVULSANTS Define ‘Epilepsy’ - Epilepsy is a disorder of the brain characterised by an enduring predisposition to generate epileptic seizures, and will require the occurrence of at least one unprovoked seizure (and a high-risk of recurrence of seizures) Epilepsy involves dysfunctional communication between neurons in the brain o The misfiring of neurons will trigger a predisposition to generate epileptic seizures - Describe different types of seizures - The different types of seizures include: o Focal Seizures (also known as Partial Seizures) This occur following activation of neurons in a relatively small, discrete region of the brain Symptoms of Focal Seizure will be dependent on the size and the function of the part of the brain affected o Generalised Seizures These will affect the whole brain (i.e. both hemispheres), and are associated with the loss of consciousness Different types of Generalised Seizures include: Tonic – rigid stretching / extension of extremities Atonic – sudden loss of muscle tone Myoclonic – repetitive muscle twitching Tonic-Clonic (i.e. ‘Grand-Mal’) – distinct Tonic Phase followed by a Clonic Phase (i.e. full body spasms with intermittent relaxation) Absence (i.e. ‘Petit-Mal’) – brief and intermittent loss of consciousness o Whilst the outward signs of this type of seizure are minimal, there is significant electrical activity triggered in the brain o There is often progression in the type / severity of seizures over a lifetime For example, some patients may initially have Focal Seizures that eventually develop into Generalised Seizures Describe the different mechanisms of action of antiepileptic drugs (including examples of those that decrease excitation and increase inhibition) - The different mechanisms of action of antiepileptic drugs include: 22 o - Decreased excitation Reduce firing frequency of neurons (via enhancing Na+ channel inactivation) Na+ channels are required for generating Action Potentials, so inactivating Na+ channels will reduce electrical activity / excitation Examples of drugs with this mechanism include Phenytoin, Carbamazepine and Lamotrigine Inhibit excitatory amino acid release (via blocking Ca2+ channels) Blocking Ca2+ channels will inhibit the secretion of Neurotransmitters from the Synaptic Vesicles at the Pre-Synaptic Terminal o This is used in the treatment of generalised absence seizures o Examples of a drug with this mechanism is Ethosuximide Similarly, inhibiting other proteins associated the secretion of Neurotransmitters from the Synaptic Vesicles at the Pre-Synaptic Terminal (e.g. SV2A) will reduce excitation o Examples of a drug with this mechanism is Levetiracetam Block excitatory amino acid action Inhibiting the post-synaptic Glutamate receptors will prevent action of the excitatory amino acid Examples of drugs with this mechanism include Topiramate and Felbamate o Increased inhibition Enhance GABA action Barbiturates will enhance the inhibition from GABA by: o Increasing the affinity of GABA-A Receptors to GABA o Increasing Cl- conductance through the GABA-A Receptor / Ion Channel o Prolonging the open time of the GABA-A Receptor / Ion Channel Alternatively, Benzodiazepines will enhance the inhibition from GABA by increasing the frequency of channel opening Inhibit GABA breakdown Inhibition of GABA Transaminase will result in a reduction in the breakdown of GABA to Succinic Semialdehyde (and hence increases the quantity of GABA available at the Pre-Synaptic Terminal for release into the Synaptic Cleft) Examples of a drug with this mechanism is Vigabatrin Inhibit GABA uptake Inhibition of GABA Transporters will increase the levels of GABA in the synaptic cleft Examples of a drug with this mechanism is Tiagabine (which is specific to GAT1 [i.e. GABA Transport 1]) Certain antiepileptic drugs will have multiple mechanisms of action, such as: o Sodium Valproate – Inhibit Na+ channels, block Ca2+ channels and inhibit GABA breakdown This drug is commonly used for treatment of Generalised seizures o Topiramate or Felbamate – Inhibit Na+ channels, block Glutamate action and enhance GABA action Describe the functional effect of a mutation that causes epilepsy - The extensive interconnection of neurons are such that changes in one particular gene can impact upon the neuronal balance / equilibrium, thus resulting in epilepsy There are several different genetic mutations associated with Epilepsy o These genetic mutations are typically are almost always associated with ion channels Examples of genetic mutations causing epilepsy include: o ‘GEFS+’ – this involves a mutation of K289M that decreases GABA-A receptor amplitude by decreasing the ability of GABA channels to conduct Cl- ions through the channel ion pores - 23 SEIZURE DISORDERS Describe the definition and classification of 'seizure' and 'epilepsy' - - Epilepsy is a disorder of the brain characterised by an enduring predisposition to generate epileptic seizures and by the neurobiologic, cognitive, psychological and social consequences of this condition o This is NOT a singular disease entity, but a variety of disorders reflecting underlying brain dysfunction Epileptic seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain Seizures are classified according to whether it is Generalised vs. Focal (i.e. Partial) vs. Unclassified Describe the neurophysiological changes associated with an epileptic seizure - Generalised Seizures will be bilaterally distributed (i.e. affects both hemispheres) and will involve networks in the brain o Patients with Generalised Seizures are unaware of the onset of the seizure and will lose consciousness during the seizure Focal Seizures will originate from one area of the brain (i.e. affects one hemisphere only), although it may involve a network that can cause the seizure to involve both hemispheres o Patients with Focal Seizures may have an ‘aura’ phase prior to the seizure where they are aware of the impending seizure - - Describe the role of EEG and other tests in the diagnosis - Neurophysiological activity can be measured using Electroencephalography (EEG) o This can be used to identify the origin of the seizure activity and hence assess whether a seizure is Generalised vs. Focal MRI Scan or CT Scan can determine the presence of any tumours / space occupying / infectious lesions that may be triggering seizure activity o The location of the lesion is likely to determine the type of signs exhibited by the patient o Note: CT Scan may miss several different malformations that can result in a seizure Therefore, an MRI Scan (which is more sensitive and can identify these additional malformations) MUST be conducted! Lumbar Puncture may be performed if Meningitis / Encephalitis is suspected (which could trigger a seizure) Blood tests and urine drug screen are also useful tests that provide information regarding other precipitants of seizures (e.g. drugs, electrolyte levels, glucose levels, etc.) PET and SPECT may also be utilised to identify the particular focus of seizure activity within the brain prior to surgical cortical resection - - BRAINSTEM INTRODUCTION TO BRAI NSTEM Identify the anatomical organisation of the brainstem, with particular reference to the brainstem reticular formation and its neurotransmitter pathways (i.e. serotonin, dopamine, noradrenaline and acetylcholine) - Brainstem will contain Sensory Cells, Motor Cells, Pathways, Cranial Nuclei and Reticular Cells Reticular Cells are a groups of cells (collectively termed as the ‘Brainstem Reticular Formation’ [BRF])that have a significant impact / influence on the function of both higher and lower centres o Brainstem Reticular Formation is located in the middle of the Midbrain, Pons and Medulla (i.e. all areas of the Brainstem) There are two main (closely-related) functions of the Brainstem Reticular Formation; these are: o Arousal / Mood Setter - 24 - - This is primarily associated with the Ascending projections (also known as the ‘Ascending Activating Reticular System’) These Ascending projections will set Forebrain activity to a particular level (such that it is an ‘arousal’ / ‘mood’ setter) These Ascending pathways will ‘sample’ / receive the inputs from the somatic / visceral worlds via the fibres from the ascending Spinothalamic Tract (that were directed towards the Brainstem Reticular Formation) Based on these inputs, the Ascending projections will then decide upon the level of forebrain activity / arousal (e.g. awake vs. asleep) and mood (e.g. happy vs. grumpy) Autonomic Policeman This is primarily associated with the Descending projections (via the Reticulospinal Tract) These Descending projections will send signals down the Spinal Cord based on inputs from the Somatic / Visceral worlds (e.g. Respiratory, Cardiovascular, Urogenital systems) These signals will influence the reflexes affecting these various Somatic / Visceral systems The different functions of the Brainstem Reticular Formation are carried out by distinct individual nuclei (each of which have distinct functions) o Each of these distinct individual nuclei that have been identified have been separately named and are no longer considered a part of the Brainstem Reticular Formation o As a result, the remaining Brainstem Reticular Formation does NOT have any particular functions allocated to any particular areas The following neurotransmitter systems exist within the Brainstem Reticular Formation: o Serotonin This is located in the Raphe Nuclei and connect throughout the brain Raphe Nuclei are a small groups of cells located in the midline of the Midbrain, Pons and Medulla o Acetylcholine This is located in the BRF Cholinergic Groups and connect throughout the brain BRF Cholinergic Groups are a large group of cells located throughout the Brainstem o Dopamine This is located in the Substantia Nigra and Ventral Tegmental Area (VTA) and connects to the Forebrain (e.g. Basal Ganglia, Amygdala, Hippocampus) These groups of cells is located in the Midbrain of the Brainstem (and can be identified by being pigmented, as Dopamine production has the by-product of Melanin) o Noradrenaline This is located in the Locus Coeruleus and connect throughout the brain This group of cells is located in the Pons of the Brainstem Describe the suspected functions of each neurotransmitter system and identify clinical signs/symptoms resulting from lesions at these sites - The functions of each neurotransmitter system in the BRF involve the regulation of the following (hence lesion in these systems will result in dysfunction of the following functions): o Serotonin Behaviour (via ensuring the Cortex understands what is happening in reality) (e.g. LSD impacts the Serotonergic system, resulting in dream-like state / hallucinations) Mood (via the impact on the Pre-Frontal Cortex, as low levels of Serotonin will result in depression) Aggression (via the impact at the Amygdala and Hippocampus, as higher levels of Serotonin in these areas will dampen / reduce the level of aggression) 25 o o o Pain (via the projection to the Dorsal Horn of the Spinal Cord, as Serotonin can dampen / reduce the signal / activity from pain afferents from the Dorsal Horn of the Spinal Cord) Blood Flow Control (via Serotonergic fibres wrapping around Cerebral Blood Vessels, as the level of the Serotonergic system can affect the diameter of the Cerebral Blood Vessels [e.g. underactive Serotonin system will trigger vasodilation of Cerebral Blood Vessels, which can result in headache]) Cholinergic Arousal (i.e. failure of the Cholinergic system will result in loss of consciousness / drowsiness / coma) Memory (via the projections to the Cortex and Hippocampus) ANS Control (via the descending projections to the Spinal Cord) (in particular the cardiovascular and respiratory systems) Pain (via the projection to the Dorsal Horn of the Spinal Cord, as Acetylcholine can dampen / reduce the signal / activity from pain afferents from the Dorsal Horn of the Spinal Cord) Dreaming (as Cholinergic cells in the Pons are the only group of cells that are active during REM sleep) Dopamine Behaviour (e.g. underactive Dopamine projections to the Cortex can result in negative symptoms of Schizophrenia [e.g. anti-social behaviour], underactive Dopamine projections to the Basal Ganglia can result in Parkinson’s Disease) Level of Focus on Movements Dopaminergic system will enable focusing on the desired movement only Conversely, there is suppression of non-desired movements (e.g. tremor of Parkinson’s Disease results from failure to suppress these unwanted movements) Pleasure / Motivation (as higher levels of Dopamine are associated with pleasure) Noradrenaline ANS Control (which can prepare the body for an emergency situation) Pleasure / Motivation (as higher levels of Noradrenaline are associated with pleasure) Blood Flow Control (via Noradrenergic fibres wrapping around Cerebral Blood Vessels, as the level of the Noradrenergic system can affect the diameter of the Cerebral Blood Vessels) Neural Plasticity (as high levels of Noradrenaline are associated with the establishment of new synapses at the sites of neural lesions) Global Attention (which can prepare the body for an emergency situation [e.g. heighten all senses in Fight or Flight response]) CRANIAL NERVE ORGANI SATION Describe the basic principles of how a cranial nerve nucleus functions - The Cranial Nuclei are where the various functions of the Brainstem arise (which are then distributed to the periphery via the Cranial Nerves) o The different functions of each Cranial Nerve generally will arise from a different Cranial Nucleus within the Brainstem o Hence, each Cranial Nerve may collect fibres from different Cranial Nuclei o Conversely, an individual function may arise from one Cranial Nucleus and be distributed to the peripheries via multiple Cranial Nerves (e.g. the Cranial Nucleus providing motor innervation to the Pharynx will have fibres in both CNIX and CNX) Describe the organisation of the cranial nerve nuclei in the brainstem 26 - Whilst there is only a single sensory, motor and autonomic column in the spinal cord, there is three sensory, two motor, one autonomic column in the brainstem o Each of the sensory, motor and autonomic nuclei will continue to have the same function at the other nuclei is the same column but each level of the column will have a different target o However, the cranial nuclei in the Brainstem are not directly above / below each other (i.e. not a continuous column) due to the physical presence of the Ventricles Describe the different functional columns and the cortical control of the cranial nerve nuclei (and the difference between upper and lower motor neurone lesion, using Cranial Nerve VII as example) - The different cranial nuclei columns are (from medial to lateral): o Somatic Motor (CNIII, CN IV, VI, XII) – these are located at the midline of the Brainstem These 4 motor nuclei that are in the midline are those that divide equally into 12 except for I and II, that is III, IV, VI and XII (whilst CNV, VII, VIII, IX, X and XI are in the lateral brainstem) o Autonomic (Edinger-Westphal CNIII, Superior Salivary CNVII, Inferior Salivary CNIX, Dorsal Motor Nucleus of Vagus Nerve CNX) – these are located immediately laterally to the Somatic Motor Cranial Nerve Nuclei (except Edinger-Westphal which is superior to the CNIII Cranial Nuclei) o Taste and Visceral Sensory (i.e. Nucleus Tractus Solitarius) – this is located in the Medulla The rostral aspect of the Nucleus Tractus Solitarius provides taste fibres to CNVII, CNIX and CNX, and is located lateral to the Dorsal Motor Nucleus of Vagus Nerve The caudal aspect of the Nucleus Tractus Solitarius provides Visceral Sensory to CNIX and CNX, and is located inferior to the Dorsal Motor Nucleus of Vagus and Hypoglossal Motor Nuclei Note: NTS is the ONLY Cranial Nerve Nucleus that has two functional columns (i.e. Taste and Visceral Sensory) o Pharyngeal Motor (Vmotor CNV, VIImotor CNVII, Nucleus Ambiguus CNIX and CNX) these are located relatively lateral [but not the most lateral] through the Pons and Medulla o Somatic Sensory (Vp, Vsp, Vmes CNV, Vp and Vsp CNVII, CNIX, CNX) Spinal Tract Nucleus of the Trigeminal Nuclear Complex (Vsp) is located caudally (extending from the Medulla to the Pons) will receive pain and temperature signals from the head Principal Nucleus of the Trigeminal Nuclear Complex (Vp) is located at the Pons and will receive tactile signals from the head Mesencephalic Nucleus of the Trigeminal Nuclear Complex (Vmes) is located rostrally at the Midbrain and will receive proprioceptive signals from the head Note: As a result, a lesion in one particular area of the Brainstem will result in the loss of a particular type of sensation throughout the entire head (rather than losing all types of sensation in only a limited part of the head) Note: The sensory signals from CNVII, CNIX and CNX towards the Trigeminal Nuclear Complex are primarily from the ear (though the bulk of sensory inputs for the Trigeminal Nuclear Complex are from CNV) o Special Sensory (Vestibular and Cochlear Nuclei CNVIII) these are located most laterally at the Pons There is a separate Vestibular Nuclei and Cochlear Nuclei that receive the signals from CNVIII (which consists of a Vestibular Nerve and Cochlear Nerve respectively) Cochlear Nuclei is more lateral than Vestibular Nuclei There are 4 cranial nerves in the Medulla, 4 in the Pons and 4 above the Pons (2 in the Midbrain) o Medulla = CNIX, X, XI and XII (i.e. Cranial Nerves 9-12) o Pons = CNV, VI, VII and VIII (i.e. Cranial Nerves 5-8) o Midbrain = CNIII and IV (i.e. Cranial Nerves 3-4) o Above Midbrain = CNI and II (i.e. Cranial Nerves 1-2) The Autonomic Nuclei all refer to Preganglionic Parasympathetic Cell Bodies o Edinger-Westphal Nuclei will innervate the Sphincter Pupillae and Ciliary Muscle (via CNIII) - - 27 o - Superior Salivary Nuclei will innervate the Sublingual, Submandibular and Lacrimal Glands (via CNVII) o Inferior Salivary Nuclei will innervate the Parotid Gland (via CNIX) Cortex will control the Cranial Nerve Nuclei via the Corticobulbar Tract (as the Cranial Nerve Nuclei appear like bulbs) o Most Corticobulbar Tract innervations are bilateral (with the exception of parts of the Cranial VII Nucleus and Cranial XII Nucleus which are innervated contralaterally) The part of the Cranial VII Nucleus that innervates the upper facial muscles will receive a bilateral innervation from the Corticobulbar Tract In contrast, the part of the Cranial VII Nucleus that innervates the lower facial muscles will receive a contralateral innervation from the Corticobulbar Tract o As a result, a Central Facial Nerve Lesion (i.e. Upper Motor Neuron Lesion) can result in the loss of the contralateral lower facial muscles only (as there is not bilateral central innervation for these lower facial muscles) In contrast, Peripheral Nerve Lesion (i.e. Lower Motor Neuron Lesion of VIImotor) will result in the loss of ipsilateral upper and lower facial muscles LOWER BRAINSTEM FUNCTIONS Describe the structure and function of the brainstem regions that control respiration and cardiovascular responses (including blood pressure) - The basic respiratory rhythm is generated by a group of neurons within the lower brain stem (i.e. Medulla and Pons) that are collectively called the ‘Respiratory Centre’ The activity / firing rate of the neurons in the Respiratory Centres (and hence inspiration) is regulated by inputs from the: o Medullary Chemoreceptors (which are sensitive to hypercapnia) Triggering of the Retrotrapezoid Nucleus in Caudal Pons / Rostral Medulla is the most powerful stimulus for respiration o Afferent input from Lung Stretch receptors and arterial chemoreceptors (which are primarily sensitive to hypoxia as well as being sensitive to pH); and This input is carried from CNIX and CNX via the Nucleus Tractus Solitarius o Motor Cortex (i.e. conscious respiration) The different Respiratory Centres in the Medulla and Pons include: o Dorsal Respiratory Group (DRG) – these consist mainly of inspiratory neurons (i.e. those which fire during inspiration) and are located in the Medulla o Ventral respiratory group (VRG) – these consist of both inspiratory neurons and expiratory neurons (i.e. those which fire during expiration) and are located in the Medulla o Pneumotaxic Centre – these consist of inhibitory inspiratory neurons (thus limiting inspiration) and are located in the superior Pons These neurons receive inputs from the Pulmonary Stretch Receptors in the Bronchi and Bronchioles These receptors send signals to the Pneumotaxic Centre to stop inspiration when lungs are highly inflated (which will minimise work as more effort is required to breath at higher volumes / pressures) this is known as the ‘Hering-Breur Reflex’ o Apneustic Centre – these costs of excitatory inspiratory neurons (thus promoting inspiration) and are located in the middle Pons Many inspiratory neurons have axons which descend to the spinal cord and control motor neurons supplying inspiratory muscle, and hence drive inspiration o In contrast, expiration is usually a passive process, although during active expiration some expiratory neurons (with axons which also descend to the spinal cord) drive expiration There are two basic theories to explain respiratory rhythmogenesis o ‘Pacemaker’ Theory – this suggests there are cells within the brainstem that are capable of generating action potentials themselves in a rhythmic manner (similar to the SA Node in the heart), which will drive respiratory rhythm The Pre-Botzinger Group of cells (located at the border of the Pons and Medulla) have this property of generating action potentials themselves in a rhythmic manner - - - - 28 o - - ‘Network’ Theory – this suggests that inspiratory neurons will have a positive feedback loop, such that excitation of the inspiratory neuron will further stimulate the inspiratory neuron (via a collateral axon) However, there will also be an inhibitory interneuron connected to the inspiratory neuron (via a collateral axon) This inhibitory interneuron will trigger the inspiratory neuron ceasing to fire once it is stimulated beyond a certain threshold The net effect will be a gradual increase in respiratory activity followed by a sudden termination Cardiovascular Response is controlled by the: o Rostral Ventrolateral Medulla (which regulates sympathetic outflow to heart, blood vessels, adrenal medulla) o Nucleus Ambiguus (which contains the Vagal Parasympathetic Preganglionic neurons that innervate the heart) Rostral Ventrolateral Medulla (RVLM) project directly to the IML of the Spinal Cord (i.e. sympathetic Preganglionic neurons) and hence are a major source of descending drive to sympathetic outflow o The RVLM is tonically active, which generates the tonic activity of the sympathetic nervous system (e.g. tonic vasoconstriction that assists in maintaining resting blood pressure) o The RVLM is also a critical component of the Baroreceptor reflex (which stabilises blood pressure) and Chemoreceptor reflex (which drives sympathetic activity) As such, the RVLM receives inputs (excitatory and inhibitory) from a wide range of peripheral receptors and from cardiovascular nuclei in the pons, midbrain, and forebrain (NTS via CVLM, PAG, Paraventricular Nucleus of the Hypothalamus, etc.) Describe the principles involved in cerebral autoregulation of blood flow - Cerebral Autoregulation of Blood Flow is the process that aims to maintain adequate and stable cerebral blood flow irrespective of systemic blood pressure o Brain is very sensitive for over- and underperfusion and so would not be able to cope with the regular changes in systemic blood pressure This regulation of cerebral blood flow is achieved primarily by small arteries and arterioles, which either dilate or contract under the influence of multiple complex physiological control systems The physiological mechanisms controlling contraction / dilatation of the small arteries / arterioles include: o Metabolic (via a negative feedback control system) o Neurogenic (via changes in sympathetic or parasympathetic innervation of vascular smooth muscle); and o Myogenic (i.e. direct detection by vessel of change in systemic blood pressure, and corresponding change in calibre of the vessel) - STROKE EPIDEMIOLOGY OF STROKE Describe epidemiological features of stroke, its risk factors and the prognosis following stroke - Stroke is defined as rapidly developing symptoms and / or signs of focal, and at times global, loss of cerebral function, with symptoms lasting more than 24 hours or leading to death with no apparent cause other than that of vascular origin o Symptoms / signs of loss of cerebral function with no apparent cause other than that of a vascular origin that last < 24 hours are typically considered a Transient Ischaemic Attack (TIA) Epidemiological features of stoke suggest an increased risk of stroke with: o Elderly (i.e. 50% in people aged > 75 years) o Male o Family history of premature CVD - 29 - - - - o Ethnicity o Diabetes o Renal Failure / Microalbuminuria / CKD Modifiable risk factors for stoke include o Smoking o Hypertension o Hypercholesterolaemia o Weight o Waist Circumference (i.e. central adiposity) o Physical Activity Levels Prognosis for patients 1 year post-stroke are: o ~33% die o ~33% have persistent disability o ~33% recover Stroke patients will have significantly higher mortality immediately following the stroke (i.e. within initial 3 months) o The mortality rate for Stroke patients will be similar (albeit slightly higher) compared to NonStroke patients beyond this initial post-Stroke period o Prognosis for Stroke patients are poor due to elderly nature of stroke patients and the likelihood of recurrence of the stroke o Survival / recovery is more likely for patients with less pre-existing disability / illness, milder strokes, younger age, better lifestyle (i.e. no smoking, limited alcohol, good diet, exercise, etc.) and compliance with treatment Haemorrhagic strokes are associated with higher earlier mortality compared to Ischaemic strokes Most patients with a severe stroke will be able to regain some mobility (e.g. walking) within the first three months following a stroke o Stroke patients who still lack mobility three months after a stroke are unlikely to achieve improvements in mobility in the longer-term o Rehabilitation post- stroke will involve adapting to the reduced levels of mobility Describe methods of stroke prevention at different levels (primary, secondary and tertiary) and the evidence for these methods, including relevant clinical protocols and guidelines - Primary Prevention of Stroke will involve assessment of absolute CVD risk in next 5 years (based on Framingham equation) Secondary Prevention of Stroke will involve improving the modifiable risk-factors (per above) Tertiary Prevention of Stroke will involve: o Admission to dedicated Stroke Units immediately post-stroke Key characteristics of stroke unit include multidisciplinary care, specialist nursing staff, high proportion of Occupation and Physical Therapy, provision of information to carers, etc. Stroke Units have been shown via multiple trials to deliver reductions in death, institutionalisation and length of hospital stay o Treatment of risk-factors (e.g. hypertension, hypercholesterolaemia) o Anti-platelet therapy - STROKE – PREVENTION AND MANAGEMENT Describe general principles in the management of strokes and preventions strategies - Prevention of stroke will involve reducing / mitigating risk factors such as: o Atrial Fibrillation (i.e. via anti-coagulation) o Hypertension o Physical inactivity o Diabetes Mellitus 30 - - - o Smoking and Alcohol o Obesity o Hypercholesterolaemia (e.g. via Statins) o Diet (e.g. via Mediterranean diet, which has been linked with reduced incidence of Stroke) o Thrombophilia (from OCP, Congenital, Medications, Antiphospholipid Syndrome, etc.) Urgent assessment and treatment is needed following a Transient Ischaemic Attack (TIA) this can reduce the risk of a stroke by ~80%!!! o TIA patients have a high likelihood of suffering a subsequent stroke in the next 90 days General principles in the management of stroke include: o Differentiate between Ischaemic vs. Haemorrhagic Stroke This can only be distinguished via a CT or MRI Scan (and NOT clinically!) This is important as the treatment options will vary significantly o If Ischaemic Stroke, identify the location of the occlusion (i.e. precise area of vessel) o Revascularise (i.e. remove occlusion / thrombus) Occlusion of arteries is resolved through the use of thrombolytic agents (e.g. Tissue Plasminogen Activator [tPA]) Thrombolysis needs to be performed as soon as possible to minimise the damage to the brain o Furthermore, there is an increased likelihood of negative impact (rather than a positive impact) of treatment with tPA if the treatment is only provided >270 minutes after the stroke tPA will NOT be effective in the treatment of large clots (as stasis will result in the tPA not reaching the clot) Stent Retriever Devices are also able to remove clots and led to a significant improvement in morbidity Time is still of the essence when using these devices!!! (earlier removal of the clot will lead to superior outcomes!!!) o Avoid reducing blood pressure (via medication) in the initial ~24-48 hours following a stroke This will result in worse outcomes for patients (due to the level of brain perfusion depending on systemic blood pressure) Therefore, higher blood pressures following a stroke will increase cerebral perfusion and minimise the damage / disability from the stroke o Treatment of fever, hyperglycaemia and assessment of swallowing was found to reduce the likelihood of disability following a stroke Fever and hyperglycaemia increase the level of oxygen demand, and hence will increase the oxygen shortfall at the brain Ensuring ability to swallow prior to providing food reduces the risk of aspiration and hence pneumonia Early recognition of a stroke is CRITICAL! o Time = Brain (i.e. the longer time to receive treatment, the greater the infarction / damage to the brain) Every 15 minutes less door-to-needle time = 5% lower odds of in-hospital mortality o Use the pneumonic ‘FAST’ to detect stroke (i.e. Face, Arms, Speech, Time) o Stoke will typically have an acute onset with neurologic deficit and localising signs o Signs of stroke can also include Visual Field deficit (e.g. Hemianopia, Amaurosis Fugax, diplopia), weakness, speech deficit (e.g. aphasia, dysarthria) and cognitive deficits BLOOD SUPPLY TO THE BRAIN Understand the contribution of the vertebral and internal carotid system to the formation of the 'Circle of Willis' and to know the origins of the anterior, middle and posterior cerebral arteries and related communicating arteries - Blood supply to the brain is via an Anterior and Posterior system o Anterior system consists of the Internal Carotid Arteries (and its branches) and will supply the Anterior Cerebrum 31 o - - - - Posterior system consists of the Vertebral and Basilar Arteries (and its branches) and will supply the Posterior Cortex, Brainstem, Cerebellum and much of the Spinal Cord o Anterior and Posterior Systems are joined together by the Posterior Communicating Artery to form the Circle of Willis There can be significant anatomical variation in the appearance of the Circle of Willis Anterior system of blood supply to the brain will include: o Anterior Cerebral Artery (ACA) – this is a branch off the ICA towards the midline o Anterior Communicating Artery – this is the artery connecting the Left and Right ACA (and hence may enable collateral bloodflow between opposite hemispheres) o Middle Cerebral Artery (MCA) – this is a continuation of the Internal Carotid Artery (i.e. will flow directly from the ICA without any change in the diameter of the artery) o Anterior Choroidal and Ophthalmic Arteries – these are smaller arteries that branch off the Internal Carotid Arteries (although there is anatomical variation such that these arteries may branch off the Middle Cerebral or even Anterior Cerebral arteries in that general vicinity) o Posterior Communicating Artery – this is a branch off the ICA towards the midline and connecting with the posterior system of blood supply Posterior system of blood supply to the brain will include: o Vertebral Artery – this is a branch off from the Subclavian Artery o Anterior Spinal Artery – branches off the Vertebral Artery will combine at the midline to form this Artery, which will travel down the Anterior Median Fissure of the Spinal Cord) o Basilar Artery – this arises from the fusion of the Left and Right Vertebral Arteries, and will be located within a groove at the caudal Pons o Posterior Cerebral Artery (PCA) – this is a continuation of the Basilar Artery o Posterior Inferior Cerebellar Artery (PICA) – this is a branch off the Vertebral Artery o Anterior Inferior Cerebellar Artery (AICA) – this is a branch of the Basilar Artery caudally o Superior Cerebellar Artery (SCA) – this is a branch of the Basilar Artery rostrally o Circumferential Basilar Arteries – these branch off the Basilar Artery between the AICA and SCA ACA will branch into the Cingulate Branch (i.e. the superior branch) and the Callosal Branch (i.e. the inferior branch [which is directly adjacent to the Corpus Callosum]) near the commencement of the Genu of the Corpus Callosum MCA will branch into an Superior and Inferior Branches of the MCA in the Lateral Fissure of the Brain o This point of bifurcation of the Stem of the MCA is a common site for clot lodgement (as well as plaque build-up / atherosclerosis) Recognise the locations of the main perforating branches of the anterior, middle and posterior cerebral arteries - There are Cortical AND Deep (i.e. perforating) branches of the ACA, MCA and PCA The deep, penetrating arteries (collectively known as the Lenticulostriate Arteries) that branch off the ACA and MCA deep into the anterior forebrain (e.g. Basal Ganglia, Hypothalamus, Internal Capsule, etc.) are extremely fine / small o ACA deep branches will supply more anterior regions of the deep grey structures, whilst MCA deep branches will supply more posterior regions of the deep grey structures o Note: These arteries are extremely prone to rupture in the event of systemic hypertension o Note: These arteries are mostly terminal arteries (i.e. they form few if none connections with other arteries) The deep, penetrating arteries (collectively known as the Thalamoperforating and Thalamogeniculate Arteries) that branch off the PCA deep into the brain will supply the Thalamus ACA and MCA Perforating Branches will penetrate the inferior surface of the brain just anterior to the mammillary bodies and between the optic tracts and at the origin of the olfactory tracts PCA Perforating Branches penetrate the posterior perforated substance just behind the mammillary bodies - Revise arterial branches supplying the pons, cerebellum and brainstem 32 - Arterial supply of the Brainstem and Cerebellum is via the Anterior Spinal Artery, Posterior Spinal Artery, Vertebral Artery, Basilar Artery, PICA, AICA and SCA o Caudal Medulla is supplied by Anterior Spinal Artery, Vertebral Artery, PICA and Posterior Spinal Artery o Rostral Medulla is supplied by Anterior Spinal Artery, Vertebral Artery and PICA o Pons is supplied by Basilar Artery and AICA o Midbrain is supplied by Basilar Artery, SCA and PCA o Cerebellum is supplied by PICA, AICA and SCA o Note: Refer to diagrams in lecture slides to understand specific areas of Brainstem crosssection supplied by different arteries Know the functional territories of the major cerebral arteries - ACA will supply most of the medial surfaces of the hemisphere (including most of the Corpus Callosum except the Splenium) (i.e. up to the mid-/posterior Parietal Lobe), a small sliver of the lateral surface of the hemisphere closer to the midline and the medial part of the Inferior Ventral surface of the brain PCA will supply the Posterior Cortex (i.e. Occipital Lobe [which drives vision]), the inferior aspect of the Temporal Lobe, parts of the Thalamus (via Thalamogeniculate branches) and parts of the Hippocampus (which is important for memory) MCA will supply the remainder of the brain (which drives the motor, somatosensory, language, auditory, frontal eye fields, etc. functions) (i.e. this is a critical artery of the brain!!!) o This includes the lateral surfaces of the Cerebrum (excluding specific small slivers near the midline, the inferior aspect of the Temporal Lobe and the posterior aspect of the Occipital Lobe) and the lateral part of the Inferior Ventral surface of the brain Anterior Choroidal Artery will enter the Lateral Ventricle and provide the blood supply for the Choroid Plexus o Furthermore, the Anterior Choroidal Artery will also supply parts of the Hippocampus and parts of the Internal Capsule (i.e. posterior aspect of the Internal Capsule) o Therefore, damage to the Anterior Choroidal Artery will appear like a significant stroke (as it will damage the supply to the major neuronal pathway / highway between the Cortex and Lower Centres [i.e. the Internal Capsule]) MCA will supply the areas of the brain responsible for motor movement in the head / necks, upper limbs and upper trunk, whilst the ACA will supply the areas of the brain responsible for motor movement in the lower limbs and lower trunk Border zones (i.e. ‘watershed’ zones) are at the border of the main territories of major arteries where there is some overlap of blood supply o In contrast, core zones refer to the main territories of major arteries (with NO collateral blood supply) o Core zones are more vulnerable to ischaemia, whilst border zones are more vulnerable to global hypotension (e.g. secondary to cardiac arrest) - - - - - Understand the drainage of cerebral blood into venous dural sinuses - Cerebral Veins empty in the Dural Venous Sinuses, which ultimately will drain into the Internal Jugular Vein o Superficial veins generally lie on the surface of the cerebral hemispheres and drain into the Inferior Sagittal Sinus and Superior Sagittal Sinus o Deep veins drain internal structures and will eventually drain into the Inferior Sagittal Sinus, which drains into Straight Sinus (or alternatively drain directly into the Straight Sinus) Superior Sagittal Sinus and Straight Sinus will meet at the Confluence of Sinuses, which then drains into the Transverse Sinus o This will drain into the Sigmoid Sinus, which then drains into the Internal Jugular Vein Note: The Anterior regions of the brain will generally drain into the Cavernous Sinus o This drains via the Superior Petrosal Sinus towards the Transverse Sinus; or o This drains via the Inferior Petrosal Sinus towards the Internal Jugular Vein - - 33 - Note: There is also a Basilar Venous Plexus around the base of the brain that communicates with the Epidural Venous Plexus of the Spinal Cord Understand basic concepts of the multi-level control of blood flow by neuronal activity - Cerebral Blood Flow will be maintained at a constant rate in the normal range / variation of arterial blood pressure (i.e. ~70-150 mmHg) o This maintenance of Cerebral Blood Flow is implemented by changing the diameter of arterioles Local areas of Cerebral Blood Flow (i.e. <1mm) are controlled by local neuronal activity (i.e. higher neuronal activity results in higher local blood flow) o Neuronal Activity will impact upon capillaries and change the level of blood flow This will enable matching of metabolic demand for oxygen with the supply of oxygen o As Neurotransmitters impact upon neuronal activity (and hence Cerebral Blood Flow), drugs that impact on neurotransmitters will also impact upon Cerebral Blood Flow - Understand the consequences of loss of blood supply to cortical areas - Death of neurons will occur rapidly following cessation of cerebral blood flow (due to lack of oxygen supply) o These neurons will NOT regenerate / regrow, so the loss of function is permanent! BRAIN / CNS INFECTION BLOOD BRAIN BARRIER Identify anatomic structures that form the blood brain barrier - Blood-Brain Barrier results from the continuous tight junction between Endothelial Cells (rather than being caused by the Astrocyte Foot Processes) o Endothelial Cells form specialised, complex Tight Junctions around the cerebral capillaries (i.e. Blood-Brain Barrier) o These Endothelial Cells are covered by Pericytes, whilst there is a layer of Basement Membrane beneath them both o Astrocyte End-Feet is beneath the Basement Membrane, whilst the Astrocyte End-Feet will also lay down another Basement Membrane Layer beneath it However, these Endothelial Cells will only develop a blood-brain barrier in the presence of Astrocyte Foot Processes o Astrocyte Foot-Processes will direct the Endothelial Cells to form the continuous tight junctions (i.e. Blood-Brain Barrier) o Hence, tight junctions / BBB from Endothelial Cells will only develop in the CNS (i.e. they will NOT develop a blood-brain barrier if they are in the periphery) o Note: Astrocyte Foot-Processes also modulate / regulate blood flow locally (to the required level based on the level of local neuronal activity), secrete cytokines, chemokines and antimicrobial substances (i.e. immune-mediators) and induce expression of transporters in Endothelial Cells Claudins and Occludins are the most important adhesion molecules o These will attach the Endothelial Cell Leaflets / Projections to each other and anchor themselves extracellularly as well as into the Actin Cytoskeleton o This forms a very strong, tight adhesion molecule that pulls the two adjacent Endothelial Cells together o Note: Junctional Adhesion Molecules (e.g. Cadherins, Catenins) within Endothelial Cells play an important role in regulating lymphocyte and other inflammatory cell movement - - 34 Describe the specific function of the blood brain barrier and specific mechanisms by which certain molecules bypass it - Blood-Brain Barrier is a barrier between the blood supply and the brain that restricts the entry of certain molecule into the CNS o Note: Certain areas of the brain (e.g. Pituitary Gland, Pineal Gland, some areas of the Hypothalamus, Area Postrema) are NOT covered by the BBB as these areas of the brain either need to secrete hormones directly into the circulation and / or are continuously monitoring the circulation for changes in composition BBB exists as the CNS / brain is a unique organ and needs special protection compared to the rest of the body to protect it against: o Toxins (e.g. Bile Salts) o Circulating Neurotransmitters (e.g. Noradrenaline, Glutamate) o Circulating bacteria and immune cells Water-soluble molecules require specific transport across the BBB generally, and hence requires specialised transport mechanisms (rather than Pinocytosis) o In contrast, lipid-soluble molecules (e.g. Oxygen, CO2, Ethanol) will passively diffuse across the BBB o Note: Given the need for specialised transport mechanisms, there is abundant mitochondria in the cerebral capillaries (to support energy dependent transport mechanisms) Mechanisms available by which molecules bypass the BBB include: o Active transporters (e.g. GLUT-1 Transporter is the specific transporter for D-Glucose; this ensures the brain receives the Glucose it requires for operation) o Use of a pro-drug that only converts to the active drug past the BBB (e.g. Levodopa vs. Dopamine) o Attach molecule to another molecule with a specific transporter (e.g. Nerve Growth Factor can be attached to Transferrin, which are both transported past the BBB via the Transferrin Transporter) o Exposure of brain capillaries to hyperosmolar solutions this will result in shrinkage of endothelial cells and opening of the intercellular space / BBB for passage of molecules Molecules such as bacteria may enter the CNS through direct implantation (i.e. following trauma), extension from contiguous focus of infection (e.g. Middle Ear Infection) and / or haematogenous spread o Haematogenous spread is the most common way for bacteria to enter the CNS o Organisms can spread haematogenously through the BBB if there is a failure of tight junctions (e.g. due to bacterial damage of the endothelial cells themselves), infection of a monocyte / macrophage crossing the BBB (e.g. HIV) or via pinocytic vessels (which normally transport protein into the brain) - - - - VIRAL ENCEPHALITIS AND MENINGITIS Understand the epidemiology of aseptic meningitis in Australia - Aseptic Meningitis is a syndrome of meningeal inflammation in which common bacterial pathogens cannot be identified in the CSF o This generally implies a benign clinical course and a lack of long-term neurologic sequelae ~80% of Aseptic Meningitis cases are caused by Enteroviruses, with Herpes Simplex Virus Type 2 and Arboviruses being two other common viral causes of Aseptic Meningitis o Most Enterovirus infections occur in children under five years old (with a second, smaller peak of Enterovirus infections during age ~25-35), so these are the main ages for incidence of Aseptic Meningitis Aseptic Meningitis has a seasonal variation and will typically occurs in Summer / Autumn o This seasonal variation in Aseptic Meningitis is primarily due to the seasonal variation in Enterovirus - - Define the pathogenesis and clinical features of viral meningitis 35 - - Transmission of Enterovirus (and hence most viral meningitis) is via Faecal-Oral or Person-to-Person routes o Enterovirus will invade and replicate in lymphoid tissue, resulting in a Viraemia that will enable its spread to other tissues (e.g. CNS) o Note: The peak of the Viraemia will coincide with the peak of the disease Clinical features of Enterovirus Meningitis include: o Fever o Vomiting o Headache o Neck Stiffness and Photophobia (which both indicate presence of Meningeal inflammation) o Duration of illness is generally < 1 week and almost all patients recover fully after a short convalescence (~2-3 weeks) o CSF will generally reveal a moderate white blood cell count (50 - 103 cells) and the absence of bacterial pathogens o Note: Enteroviruses may be isolated from CSF by cell culture in only ~ 50% of cases Know the major causes of encephalitis in Australia and southeast Asia - Acute Viral Encephalitis is a severe disease of the grey matter of the brain o Viral encephalitis is accompanied by high mortality rates and high rates of neurological sequelae (e.g. mental retardation, seizures, motor and sensory deficits) Causes of Encephalitis include: o Herpes Simplex (most common cause) o Rabies (especially developing countries, but NOT Australia) o Flaviviruses (which are Arthropod-borne) (e.g. Japanese Encephalitis, Murray Valley Encephalitis, West Nile Encephalitis) o Paramyxoviruses (note: these involve Zoonosis) (e.g. Hendra, Nipah) - Describe the three pathogenetic patterns of viral encephalitis - Three pathogenetic patterns of viral encephalitis involve: o Acute Necrotising Encephalitis this involves destruction of infected neurons as a result of virus-induced cytopathology (e.g. HSV Encephalitis) o Damage to Neurons from Inflammatory Response to Infection (e.g. Flavivirus Encephalitis) o Disturbance of Neuronal Function (e.g. Rabies, HIV Encephalitis) Describe the clinical features of viral encephalitis - Viral Encephalitis usually commences with non-specific clinical features such as fever, headache, myalgia, cough and vomiting o This rapidly progresses to neurological signs / symptoms such as alteration of consciousness, seizures, motor, sensory or language disturbances HSV Encephalitis Infection primarily involves the Temporal Lobes and causes extensive tissue necrosis Japanese Encephalitis may manifest initially via ~2-3 day prodromal illness of fever, cough, myalgia, etc. followed by convulsions and altered consciousness ( o Parkinsonian syndrome classically occurs early in convalescence (10-14 days after onset) o Paralysis is more common in the upper than lower limbs o Note: Bilateral haemorrhagic Thalamic lesions on MRI are highly characteristic of Flaviviral Encephalitis Lesions are also observed frequently in the Cerebrum, Midbrain, Pons, Cerebellum and Basal Ganglia as well as the Anterior Horn of the Spinal Cord Nipah Virus Encephalitis commences with fever, vomiting and reduced consciousness o However, there are distinctive clinical signs such as segmental myoclonus, hypertension, tachycardia, areflexia and hypotonia o MRI will show multiple discrete hyperintense lesions in the white and gray matter - - 36 Understand the major means of prevention of viral encephalitis - Prevention of Viral Encephalitis will involve: o Immunisation o Vector control (e.g. reduction of mosquitos) o Avoidance of exposure (e.g. mosquito nets) Note: There is no specific treatment for Japanese Encephalitis Virus, so the main control will involve preventing initial infection - Understand the pathogenesis and clinical presentation of acute disseminated encephalomyelitis - Acute Disseminated Encephalomyelitis (also known as Post-Infectious Encephalomyelitis) is an acute autoimmune disease of the CNS that occurs within days to weeks of a viral illness or vaccination (e.g. Varicella, Measles, URTI) o There is ~1 in 1,000 risk of contracting Post-Infectious Encephalomyelitis following a Measles Infection, though only a ~1 in 1,000,000 risk following a Measles Vaccine Acute Disseminated Encephalomyelitis involves demyelination of the CNS due to antibodies against Myelin Basic Protein (MBP) o Certain viral infections or vaccines may express a peptide structurally similar to MBP (i.e. Molecular Mimicry) Clinical presentation of Acute Disseminated Encephalomyelitis include: o Abrupt onset ~2-30 days after viral infection or vaccination o Multifocal neurologic deficits including visual, speech, movement and sensory deficits Note: MRI will show several multifocal white matter lesions in this condition o Altered consciousness (e.g. lethargy, coma) o Seizures (focal or generalised) o Personality changes o Note: The disease progresses for 4-5 days, after which the patient begins to recover - - CASE CONFERENCE – CNS INFECTIONS Describe different aetiologies of CNS infection and their clinical features - CNS infection may arise due to bacteria, virus, fungal or other organisms o Streptococcus pneumoniae and Neisseria meningitidis are the two most common bacteria causing Bacterial Meningitis (although Group B Streptococcus is the most common cause of Bacterial Meningitis in children <1 month old) CNS infection may be associated with fever, vomiting and headache as well as neurological signs (e.g. focal signs, altered consciousness, o Meningitis will particularly also result in neck stiffness and / or photophobia (except children < 1 year old, who do NOT have neck stiffness when they have Meningitis) An example of the development of a CNS infection involves repeated or inadequately healed Acute Otitis Media, which then leads to Chronic Mastoiditis and hence bone breakdown o There can then be a Posterior Fossa Extradural Abscess that will cause palsies in CNV, CNVI and CNVII o Whilst initially the extradural pus is walled off, this may track into the Cerebellum where it will form an Abscess that will cause Hydrocephalus and Papilloedema o Eventually, the organisms will break through into the subarachnoid space to cause frank Meningitis - - Describe investigations for CNS infections and broad management principles - Investigations conducted during CNS infections include: o Blood Sugar Level (to rule out hypoglycaemia) o FBC (to identify any systemic illness) o Electrolytes (to rule imbalance of electrolyte for signs / symptoms) 37 o o - EUC (to assess contraindication for renally excreted medication) Lumbar Puncture (except when there is raised ICP and possible mass lesion) Do NOT conduct a lumbar puncture in the presence of raise intracranial pressure (which may be exhibited via Papilloedema or Focal Neurological Signs) UNLESS a mass lesion (e.g. tumour, brain abscess) has been excluded Conducting a Lumbar Puncture in the presence of papilloedema due to a cerebral abscess carries a mortality rate of approximately 25%! If a lumbar puncture is conducted, this will change the pressure in the CNS if there is a mass lesion, the change in pressure may result in herniation of the brain / coning! Mass lesion can only be excluded with CT or MRI Scan Note: Absence of Papilloedema does NOT always exclude raised intracranial pressure (though it will commonly be present if there is raised intracranial pressure) Note: Triad of headache, vomiting and papilloedema are highly suggestive of raised Intracranial Pressure o Brain Imaging (e.g. MRI Scan, CT Scan) CT Scans are avoided for children if possible due to the risk of radiation exposure (this risk is especially heightened if the child is < 1 year old) Broad principles of management include: o Transport patient to tertiary hospital (as need their these additional facilities to care for patient with severe CNS infection) o In the event of Bacterial OR Viral Meningitis / Encephalitis, treatment should include Corticosteroids prior to the Antibiotics / Antivirals to minimise secondary inflammatory / auto-immune pathology o Commence empirical antimicrobial therapy prior to identification of the particular organism causing the CNS infection (i.e. treat with Cephalosporin (for bacteria) and Acyclovir (for virus)) Change / tailor antimicrobial therapy once the causative organism is identified o If the patient exhibits a seizure (due to brain inflammation), treat them with IV Phenytoin to prevent further seizures ANTIBIOTICS AND THE CNS Understand the main principles of antibiotic use, including: o Mean inhibitory concentration (MIC) o Single versus combination antibiotic therapy; o MIC is the lowest antibiotic concentration which inhibits growth of an organism Certain drugs will be effective if their dosage if greater than the MIC for a set % of the dosing interval (e.g. Beta-Lactams requires antibiotic level to exceed MIC >40% of the dosing interval [as well as ideally being ~5x MIC]) However, certain drugs effectiveness will be proportional to the peak concentration of the drug relative to the MIC (e.g. Aminoglycosides, Quinolones) The combination of two different drugs may be synergistic (i.e. both drugs are more effective) or alternatively antagonistic (i.e. one drug inhibits the other drug) For example, Vancomycin and Ceftriaxone in combination are significantly more effective in treatment of Pneumococcal Meningitis that individually The development of antibiotic resistance; and Antibiotic Resistance has developed due to the over-usage of antibiotics For example, there has been a significant increase in the % of Streptococcus pneumoniae organisms resistant to Penicillin in the treatment of Meningitis Antibiotic resistance is a larger problem for CNS infections (rather than systemic infections) due to the poorer penetration of antibiotics within the CSF (and hence cannot increase the antibiotic levels as easily) 38 o More resistant organisms have a higher MIC, and hence may require usage of more potent drugs than Penicillin / Beta-Lactams The use of antibiotics for treating CNS infections Lipid soluble antibiotics dissolve readily in brain endothelial cell membranes and diffuse out into the CNS In contrast, highly water soluble antibiotics are almost universally excluded from the brain unless inflammation present Alternatively, the higher the free plasma concentration and the lower the molecular weight, the greater the penetration of the antibiotic into the CSF Empiric Therapy for CNS infections is provided given the significant associated mortality 3rd Generation Cephalosporins (e.g. Cefotaxime, Ceftriaxone) and Pencillin IV administration for ~7-10 days are used to treat Meningitis prior to identification of the specific organism causing the Meningitis o Note: Vancomycin is often now added in empiric therapy given the increase in Penicillin resistance (e.g. Streptococcus Pneumoniae) o Note: Beta-lactams are commonly used to treat Meningitis as the high therapeutic ratio is such that higher doses are possible with this drug class Once the organism is identified, the drugs / medications will be changed to be more specific / narrow to the organism (e.g. Penicillin for non-resistant Streptococcus pneumoniae) Note: Listeria monocytogenes is treated with Penicillin or Ampicillin (but NOT Cephalosporins) Corticosteroids (e.g. Dexamethasone) are also provided, as this will minimise the inflammatory impact of antibiotic therapy, and hence avoid damage to the host tissues (e.g. reduce neurological complications and deafness) (without compromising the effectiveness of the antibiotic) Corticosteroids must be administered prior to or simultaneously with the antibiotics (there is no positive effect if the Corticosteroids are administered after the antibiotic!) HEADACHE AND MIGRAINE SENSORY INNERVATION OF THE HEAD AND FUNCTIONAL ANATOMY OF HEAD PA IN Identify the anatomical innervation of the head and neck relating to pain, including the trigeminal, upper cervical, glossopharyngeal and vagal nerves - CNVII, CNIX and CNX will provide sensory innervation for the Concha of the Auricle o Dura Mater of the Posterior Cranial Fossa is also innervated by the Vagus Nerve (CNX) o C2, C3 and C4 Spinal Nerves also provide innervation for the neck and back of the head CNV (Trigeminal Nerve) provides sensory innervation for the rest of the face, sensory innervation for the Dura Mater of the anterior and Middle Cranial Fossa and motor innervation for the muscles of mastication o CNV leaves the Rostral Pons laterally (i.e. at the level of the Principal and Motor Nuclei of the Trigeminal Nerve) and has a small medial motor root and large lateral sensory root There are four main nuclei for the CNV: o Principal Nucleus of CNV is located laterally in the Rostral Pons and receives synapses for tactile sensation of the face o Motor Nuclei of CNV is located medial to the Principal Nucleus in the Rostral Pons, and sends motor signals of CNV o Spinal Nuclei of CNV is located laterally in the Caudal Pons and Medulla, and receives synapses for pain and temperature sensation of the face It also receives inputs from CNIX and CNX Nerves too! - - 39 o - - - - Mesencephalic Nuclei of CNV is located laterally in the Midbrain and received proprioceptive input from the TMJ joint, Extraocular Eye Movements and Periodontal Ligaments The cell bodies for the Proprioceptive sensory fibres of CNV are located in this Mesencephalic Nuclei Trigeminal Ganglion contains the cell bodies for the Pain, Temperature, Touch sensory fibres of the Trigeminal Nerve o Trigeminal Ganglion is located in the Medial Apex of the Petrous Temporal Bone in a bony depression known as ‘Meckl’s Cave’ Fibres from the Spinal Nuclei of Trigeminal will eventually synapse in the Ventroposterior Nucleus (VPN) of the Thalamus o The Pain and Temperature Fibres from the Spinothalamic Tract will also synapse here, thus resulting in pain and temperature fibres for the whole body (including the head and neck) being transmitted to the Cortex Spinal Nuclei of Trigeminal Nerve (and the adjacent Spinal Tract of Trigeminal Nerve) has a somatotopic order o Rostral Spinal Nuclei reflects pain and temperature innervation of the nose (i.e. centre of face) o Caudal Spinal Nuclei reflects pain and temperature innervation of top of the head and jaw (i.e. periphery of face) o Middle of Spinal Nuclei reflects pain and temperature innervation of the area in-between the nose and head/jaw (i.e. middle concentric circle of face) CNV1 (Ophthalmic Branch of Trigeminal Nerve) may sometimes forget to synapse in the Caudal Spinal Nuclei of Trigeminal Nerve and instead synapse with the C1-C3 Spinal Nerves o If this occurs, then neck pain can end up being referred to the forehead resulting in the sensation of a headache CLASSIFICATION AND D IAGNOSIS OF HEADACHE Describe and distinguish different classes of headache, their classifications and signs and symptoms - The different types of headache include: o Migraine Onset – Early morning hours or daytime, reaches its peak of severity in ~30mins Duration – ~4-72 hours (if untreated) Severity – Moderate / severe (and is exacerbated by physical activity) Pain severity will peak in ~1 hour from onset, and will be severe enough to inhibit activities Location – Unilateral Character – Dull pain that progresses to throbbing / pulsating pain Signs / Symptoms – Nausea, vomiting, photophobia, phonophobia, visual disturbances (e.g. flashes of white, zig-zag lines, etc.), focal neurological signs Triggers – Stress, menstruation, alcohol, sleep deprivation, medications, foods (e.g. chocolate, cheese, fatty foods, onions, etc.) Treatment – Analgesics, Ergot Alkaloids, Triptans, Anti-Emetics ‘Classical Migraine’ has an aura immediately prior to its commencement (e.g. visual disturbances) There sometimes may also have been other mood, appetite and /or energy changes in the day preceding the migraine Note: ‘Common Migraine’ will NOT have an aura Note: Migraine may be secondary to other pathologies (e.g. stroke, tumour, etc.), so it’s important to exclude these other pathologies prior to a diagnosis of migraine o Tension Headache Onset – Gradual onset Duration – 30 minutes to 7 days Severity – Mild to moderate (and NOT aggravated by physical activity) 40 - - Location – Bilaterally, on the temples and back of head and neck Character – Tightening / pressing (i.e. non-pulsating) Signs / Symptoms – Pressure or band like on either side of the head Notably, there is typically an absence of vomiting, nausea, photophobia and phonophobia Triggers – Stress, anxiety, depression Treatment – OTC medications Note: Tension headaches persist with varying intensity for weeks to months or even longer, and usually does NOT affect activities Note: Tension headaches are more common than migraines o Cluster Headache Onset – Within an hour or two after falling asleep or at predictable times during the day Duration – Brief, but occurring in ‘clusters’ Location – Unilateral pain around one eye or one side of the face Severity – Severe Signs / Symptoms – Nasal stuffiness, eye watering (on same side as pain) Treatment – Oxygen, Ergots / Triptans, NSAIDs, Verapamil Note: Cluster headaches will persist nightly or daily for a period of several weeks to months Note: Cluster headaches are uncommon, but can be treated with Migraine o Subarachnoid Haemorrhage Onset – Sudden Severity – ‘Worst headache in my life’, but improves with time Note: There are circumstances where Intracranial Haemorrhage will not fit these characteristics, so do not necessarily rule out if this happens Signs / Symptoms – Nausea, vomiting, fever, photophobia, neck pain / stiffness, focal neurological signs (including altered consciousness) Triggers / Risk Factors – Anticoagulants, Hypertension, Elderly Treatment – Surgery, antihypertensives, supportive care Headaches may also occur in the following circumstances: o Meningitis Onset – Rapidly progressive Signs / Symptoms – Neck pain / stiffness, back pain, photophobia, seizures, altered consciousness, vomiting o Stroke Onset – Sudden Signs / Symptoms – Focal neurological signs Note: Stroke will commonly not involve a headache, but there are rare circumstances where a headache is present o Temporal Arteritis Severity – Severe Signs / Symptoms – Visual changes, prominence / tenderness of Temporal Artery, Polymyalgia Rheumatica (i.e. proximal muscle pain in multiple locations) This generally affects people > 55 years o Tumour Onset – Progressive over weeks and months Headache occurs due to raised Intracranial Pressure This type of headache may be difficult to distinguish from Tension Headaches o Cervical Arthritis Typically most intense after a period of inactivity o Hypertensive Headache Onset tends be in the early morning May be provoked by excitement and / or emotional stress Time of onset and duration of headache are important factors distinguishing between different types of headache 41 - Red flags that may signify a serious headache that requires urgent treatment include: o New headache after 40 years (as most primary, benign headaches occur prior to 40) o Different to previous headaches (as most primary, benign headaches have stable symptoms) o Fever with neck stiffness (e.g. Meningitis or Subarachnoid Haemorrhage) o Abrupt onset (e.g. Subarachnoid Haemorrhage or Stroke) o Anticoagulant use (e.g. Subarachnoid Haemorrhage or Stroke) o Altered consciousness (e.g. Subarachnoid Haemorrhage, Meningitis or Stroke) o Persistent focal neurological symptoms (e.g. Subarachnoid Haemorrhage, Meningitis or Stroke) o Significant head trauma (e.g. Subarachnoid Haemorrhage, Skull Fracture) o Seizures (e.g. Meningitis) o Immunosuppressed (as there is a higher risk of brain infection) PATHOGENESIS AND TRE ATMENT OF MIGRAINE Describe the migraine phenomenon and different hypotheses in the pathophysiology of this condition (e.g. vascular, inflammatory and cortical spreading depression hypotheses) - The phases of Migraine include: o Interictal Phase o Prodrome and Aura (only in ‘Classical Migraine’) o Headache (~15-30 mins after Aura) o Termination o Postdrome Aura may involve visual changes (e.g. zigzag lines, blurred vision, blind spots) that progress slowly across an area of the visual field, tremor, vertigo, paraesthesia, etc. Headache will be unilateral and throbbing pain, with associated vomiting, nausea, photophobia and phonophobia There are several different hypotheses regarding the pathophysiology of headache (though it is now generally viewed as a neurovascular disorder); these include: o Vascular Theory This theory suggests intracerebral vasoconstriction results in the Aura, whilst extracerebral vasodilation results in the headache However, the changes in blood flow (i.e. vasoconstriction and vasodilation) do NOT coincide with the changes in symptoms, so the empirical evidence for the Vascular Theory is limited! o Cortical Spreading Depression This theory indicated there is a slowly advancing wave of neural inhibition through the Cortex This inhibition may activate the Trigeminal Nucleus Caudalis, hence resulting in sensitisation of central pain pathways Alternatively, cerebral blood flow changes associated with the wave of inhibition may initiate the headache Note: The wave of inhibition is preceded by a transient, intense wave of excitation, which could be responsible for the Aura o Neurogenic Inflammation Theory Activation of Trigeminal Nerve fibres projecting to Meninges and Blood Vessels causes pain directly as well as the release of CGRP (+ Substance P, Nitric Oxide, NKA) from sensory nerve terminals These neuropeptides trigger vasodilation and neurogenic inflammation of the Dura Mater Note: Release of CGRP correlates with pain of headache, whilst concentration of CGRP is correlated to the severity of the headache Note: CGRP has a normal function of being a vasodilator, so this may be released following a trigger that results in vasoconstriction of intracranial blood vessels - 42 o Stimulation of the Trigeminal Ganglion will also result in activation of the Trigeminal Nucleus Caudalis in the Brainstem, hence activating the ascending central pain pathways (which trigger nausea, pain, etc.) Describe principles in the management of migraine and the use of different drug classes for this condition - Serotonin plays an important role in the pathogenesis of Migraine given the existence of both inhibitory (5HT-1) and excitatory (5-HT2) Serotonin receptors on the Trigeminal Ganglion / Nerves / Nuclei and the intracranial blood vessels respectively o Stimulation of 5-HT1 receptors will result in vasoconstriction, whilst stimulation of 5HT-2 receptors will result in vasodilation Treatment of Migraine may involve: o NSAIDs – inhibition of Prostaglandins will reduce sensitivity of nerve to pain-producing substances (e.g. Bradykinin, Histamines, Serotonin, etc.), and hence reduce inflammation o Ergotamines – this is partial agonist of 5-HT1d, and hence will block vasodilation and neurogenic inflammation of the Dura Mater o Triptans – this is an agonist of 5-HT1b and 5-HT1d, and hence will both block vasodilation and neurogenic inflammation of the Dura Mater AND inhibit activation of ascending central pain pathways Triptans will take ~30minutes to be effective, so it’s important to promptly administer Triptans upon the commencement of the Aura to be able to stop the migraine as soon as possible o Note: Both Triptans and Ergotamines are contraindicated in patients with cardiovascular disease due to their vasoconstrictive properties Prophylaxis treatments to prevent migraine include: o Beta-adrenoceptor agonists (e.g. Propanolol, Metoprolol) – mechanism is unknown o Calcium channel antagonists (e.g. Verapamil) – decrease in Ca2+ entry reduces cellular excitability o 5-HT2 receptor antagonists (e.g. Methysergide, Pizotifen) – this blocks vasodilation and consequent inflammation o Anticonvulsants (e.g. Sodium Valproate, Gabapentin) – this increases inhibitor GABA neurotransmission and hence reduces cortical excitability (i.e. reduced Trigeminal Neurotransmission and Cortical Spreading Depression) o Antidepressants o Note: Each of the above drugs each have particular adverse side-effects - - VISION VISUAL PATHWAYS – ANATOMY Identify the anatomical and functional organisation of the central visual pathways from the retina to the cortex (i.e. optic nerve, optic tract, superior colliculus, pretectum, suprachiasmatic nucleus, lateral geniculate nucleus, pulvinar, optic radiation, primary and secondary visual cortex) - ‘Peripheral’ structures of the eye (i.e. Retina, Optic Nerve, Optic Chiasm, Optic Tract) are actually part of the CNS, and will behave accordingly if damaged o Retina is a sensory surface that is part of the outgrowth of the embryological Diencephalon, and has photosensitive cells (i.e. cells receptive to light) o Optic Nerve is actually like a central tract containing fibres of the CNS from the Retina to the Cortex ‘Central’ structures of the eye include Hypothalamus, Brainstem, Thalamus, Optic Radiation and Cortex o Hypothalamus and Brainstem will be the site of termination for a small proportion of Optic Fibres (mainly to enable reflexes) o Thalamus is the site of termination for most of the Optic Fibres - 43 - - - - - - - o Optic Radiation connects the Thalamus and Cortex There are two main cell types in the Retina: o Ganglion Cells are the projection cells of the Retina (i.e. their axons project from the Retina towards the Visual Cortex via the Optic Nerve) o Photoreceptors (i.e. Rods and Cones) will detect light and have all of their processes with the Retina Cones enable colour vision and day vision, whilst Rods enable grey / black and white vision and night vision Note: There are no photoreceptors at the Optic Disc (which is the site of where all the Axons of the Ganglion Cells collect and go into the Optic Nerve), and hence this results in a ‘blindspot’ There are two main types of Ganglion Cells: o Magnocellular – these large-sized cells are involved in detecting movement / motion o Parvocellular – these medium-sized cells are involved in detecting colour / colour borders Ganglion Cells are adjacent to the Vitreous Humour (i.e. medially / superficially), whilst Photoreceptors are adjacent to the Choroid (i.e. laterally / deep) o However, the Fovea Centralis of the Central Retina is the one exception where the Photoreceptors are adjacent to the Vitreous Humour As a result, the light will directly hit the photoreceptors at the Fovea Centralis o Furthermore, the density of photoreceptors is extremely high at the Fovea Centralis, resulting in greater visual acuity o Ganglion Cells have been shifted from the Fovea Centralis outwards creating a large build-up / ‘mountain’ of Ganglion Cells around the Fovea Centralis this region is referred to as the ‘Macula Lutea’ Each of the Ganglion Cells in the Macula Lutea connect to an individual photoreceptor in the Fovea Centralis, resulting in a 1:1 transmission ratio This transmission ratio is very high compared to the periphery where ~100 Photoreceptors may connect to 1 Ganglion Cell (resulting in a dilution of the initial light stimulus) o Hence, the direct exposure to light, density of photoreceptors and transmission ratios are best in the Central Retina (resulting in peak visual acuity at the Central Retina) The split between the Nasal Retina (from which Nasal Optic Fibres arise) and Temporal Retina (from which Temporal Optic Fibres arise) is at the Fovea Centralis (and NOT at the Optic Disc) o As a result, the Nasal Retina is larger than the Temporal Retina (as the Fovea is located towards the Temporal edge of the edge) Image Forming Visual Pathway involves the Lateral Geniculate Nucleus (LGN) of the Thalamus and Primary Visual Cortex (V1) of the Occipital Lobe LGN will reorganise the inputs received from the Retina into a more understandable form that is transmitted to the Visual Cortex for interpretation o LGN will organise / map the stream (i.e. motion vs. colour), topography (i.e. which part of the visual field) and laterality (i.e. left vs. right eye) for the contralateral visual field There are four main functional layers of the LG (though the total number of layers is typically greater [e.g. 6 layer]) o Top / outer two layers relate to Colour, whilst bottom / inner two layers relate to Motion o Two of the layers relate to the Ipsilateral side (i.e. 1st and 3rd layer), whilst two of the layers relate to Contralateral side (i.e. 2nd and 4th layer) o Each layer is topographically mapped to different parts of the contralateral visual field (i.e. different parts of visual field depending on Rostral-to-Caudal and Medial-to-Lateral location within each layer) Rostral = Peripheral Retina vs. Caudal = Central Retina Medial = Superior Retina vs. Lateral = Inferior Retina o Note: This system of layers in the LGN enables the synchronisation / harmonisation of the inputs for the same visual field from the two different eyes Primary Visual Cortex (V1) is located on the upper and lower banks of the Calcarine Sulcus in the Occipital Lobe 44 o - This will receive the mapped view of the Visual Fields from the LGN, and maintain this mapping of topography, streams (i.e. movement vs. colour) and laterality (i.e. different parts of the Primary Visual Cortex reflect the particular topography, streams and laterality) Inferior Bank V1 = Inferior Retina vs. Superior Bank V1 = Superior Retina Rostral V1 = Peripheral Retina vs. Caudal V1 = Central Retina There are multiple non-image forming visual pathways involving: o Suprachiasmatic Nucleus (Sch) This is a major nucleus of the Hypothalamus located immediately above the Optic Chiasm This nuclei receives inputs from a distinct group of Ganglion cells, many of which are photosensitive (i.e. sensitive to light) The Suprachiasmatic Nucleus projects to the Pineal Gland and will trigger the release of Melatonin (which is a hormone that maintains Circadian Rhythm) Hence, light levels influence Circadian Rhythm via the Suprachiasmatic Nucleus o Pretectum This region is located in the posterior Midbrain This region received input from Ganglion Cells and will project to the EdingerWestphal Nucleus, which is responsible for parasympathetic innervation of the Sphincter Pupillae and Ciliaris Muscles of both eyes Hence, this is critical for the Pupillary Reflex and Accommodation o Superior Colliculus This has significant connections to the muscles of the neck and the muscles of the eye, and will enable both Attention or Avoidance Different parts of the Superior Colliculus will enable Attention vs. Avoidance o Pulvinar This is a large proportion of the Thalamus (i.e. posterior aspect of Thalamus) This structure receives a range of inputs from different modalities (e.g. vision, somatosensory, audition) and integrates these inputs This structure is also effective at identifying relevant objects in the visual field and driving attention on these objects (by sending signals to the Superior Colliculus to focus attention on a specified object) o Secondary Visual Cortices (V2-V5) These areas are important for enabling visual appreciation of orientation (V2, V3), colour (V4), motion (V5) and facial recognition (V5a) Describe major signs and symptoms associated with lesions of each region, particularly the different visual cortices - Damage to the Optic Nerve (pre-Optic Chiasm) will result in the complete loss of vision from one Damage to the Optic Chiasm will result in Bitemporal Hemianopia Damage to the Optic Tract (post-Optic Chiasm) will result in a homonymous hemianopia Damage to the Optic Tract in the Temporal Lobe (i.e. Meyer’s Loop) will result in a Superior Quandrantanopia o In contrast, damage to the Optic Tract in the Parietal Lobe (i.e. Baum’s Loop) will result in a Inferior Quandrantanopia Lesion in the Primary Visual Cortex will result in a Homonymous Hemianopia, but with Macula Sparing (i.e. vision retained in the centre of the visual field) Note: When discussing visual deficits, ALWAYS discuss in terms of Visual Field Deficits (rather than the Retinal Fibres that are not operating) - THE EYE – NORMAL AND ABNORMAL Describe, in general terms, the process by which the eye projects an image from the retina - The Retina is a 10-layered structure, though there are three main components o Photoreceptor (i.e. Rods / Cones) will relay signal to first-order neuron (Bipolar Cells) 45 - - o Bipolar Cells relay signal onto second-order neuron (Ganglion Cell) o Ganglion Cells then send the signal to the LGN of the Thalamus Photoreceptors in the centre of the Retina are each connected to an individual Ganglion Cell o In contrast, several / hundreds of Photoreceptors in the periphery of the Retina are together connected to an individual Ganglion Cell o This results in excellent visual acuity in the centre of the Retina, whilst a broader visual field in the periphery of the Retina There are three different sub-types of Cones (i.e. S, M, L Cones), each sensitive to a different colour Axons from Ganglion Cells in the top half of the Retina will NEVER cross to the bottom half of the Retina on its path to the Optic Nerve o Similarly, Axons from Ganglion Cells in the bottom half of the Retina will NEVER cross to the top half of the Retina on its path to the Optic Nerve o This understanding of anatomy will assist in understanding visual field defects following damage to the eye Describe the processes of accommodation, distant and near vision - Accommodation refers to the constriction of the pupil to focus on a near object Distance and near vision will require the lens to be able to adjust appropriately to focus the signal directly onto the Retina o Failure to precisely focus the signals directly onto the Retina will result in loss of visual acuity (i.e. loss of resolving power of the eye) Direct Pupil Light reflex will involve the pupil constricting to direct light, whilst Consensual Pupil Light Reflex will involve the contralateral pupil constricting in response to the ipsilateral pupil being exposed to light Relative Afferent Pupillary Defect will result in a constriction of the affected eye as a consensual response to illumination of the other eye, but will have dilation of the affected eye as a direct response to illumination of the affected eye o This occurs as the affected eye does NOT transmit the signal (due to Retina or Optic Nerve damage [i.e. pre-Optic Chiasm]), resulting in the eye simply dilating back to normal (as there is no longer any consensual input, and the eye interprets no direct input either) - - ORBITAL ANATOMY (INCLUDING EXTRAOCULAR M USCLES) Identify the major anatomical features of the orbit - Refer to lecture slides for relevant additional images The Orbital Axis is divergent and does not look straight ahead o As a result, in order to maintain a straight visual field, the Extraocular Muscles will not be directly in line with the Orbital Axis Orbit is a quadrilateral pyramid, with the Apex of the Orbit located in the back of the Orbit o Orbital Rim is the anterior boundary of the Orbit (i.e. everything in front of the Orbital Rim is NOT considered part of the Orbit, but rather part of the Eyelid) This is an incomplete circle discontinuous at the Fossa for the Lacrimal Sac Orbital Rim will attach to the Orbital Septum via the Arcus Marginalis (which is the localised thickening of the rim) Boundaries of the Orbit consists of the following bones o Roof – Frontal, Lesser Wing of Sphenoid o Floor – Maxillary, Zygomatic, Palatine o Medial Wall – Maxillary, Lacrimal, Ethmoid, Sphenoid o Lateral Wall – Greater Wing of Sphenoid, Frontal, Zygomatic The following are openings through the Sphenoid Bone into the Orbit o Optic Canal (which contains Optic Nerve, Ophthalmic Artery, Sympathetic Nerve Fibres) o Superior Orbital Fissure (which contains CNIII, CNIV, CNVI, CNV1, Superior Ophthalmic Vein, Sympathetic Nerve Fibres) - - - 46 o - - - - - Inferior Orbital Fissure (which contains CNV2, Parasympathetic Nerve Fibres to Lacrimal Gland, Inferior Ophthalmic Vein) Orbit is adjacent to the Frontal, Maxillary and Ethmoid Sinuses Sella Turcica is where the Optic Canal flows into the Cranium (i.e. in-between the Cavernous Sinuses) Ophthalmic Artery will travel inferolaterally to the Optic Nerve (CNII) as they both pass through the Optic Canal o Note: In a minority of cases, the Ophthalmic Artery will travel superiorly to the Optic Nerve (CNII) o The Central Retinary Artery is a branch of the Ophthalmic Artery, and will run within the centre of the Optic Nerve (CNII) Optic Nerve (CNII) transmits input from the Retina towards the Cortex (i.e. vision) Nasociliary Branch of the Ophthalmic Branch of the Trigeminal Nerve (CNV1) is the branch that innervates the eyeball (and hence is important for Corneal Reflex) o Frontal Branch of the Ophthalmic Branch of the Trigeminal Nerve (CNV1) provides supraorbital and supratrochlear innervation Parasympathetic fibres innervates Sphincter Pupillae and the Ciliary Muscle (via Ciliary Ganglion), as well as the Lacrimal Gland (via Pterygopalatine Ganglion) Sympathetic fibres innervate Dilator Pupilae and Muller’s Muscle (also known as Superior Tarsal Muscle) of the Upper Eyelid (via Superior Cervical Ganglion) o Note: These fibres pass through the Ciliary Ganglion, but do NOT synapse here Opening of eyelids occurs via the Levator Palpebrae Superior Muscle and Muller’s Muscle, whilst closing of eyelids occurs via Orbicularis Oculi Drainage / distribution of tears from the Lacrimal Gland occurs as a result of blinking o Palsy of Orbicularis Oculi Muscle will result in the failure of tears to appropriately drain from the superolateral Lacrimal Gland towards the Puncta (and thus towards the Lacrimal Canaliculi, Lacrimal Sac and Nasolacrimal Duct and ultimately into the Inferior Meatus), resulting in tears falling down the person’s face o Note: Puncta refer to the visible holes in the medial aspect of the eye through which tears drain towards the Lacrimal Canaliculi Ophthalmic Artery is the major arterial supply to the Orbit giving rise to branches such as the Central Retinal Artery, Ciliary Arteries, Lacrimal Artery, Muscular Arteries, Extraorbital Arteries (e.g. Supraorbital Artery, Supratrochlear Artery, etc.), etc. o Venous drainage is via the Superior and Inferior Ophthalmic Vein and Infra-Orbital and Supra-Orbital Veins o Note: Lack of valves in these Orbital Veins mean that infection can easily spread both directions, resulting in a spread of infection from the face into the Intracranial spaces (resulting in high mortality!) Describe the function of the extraocular muscles - There are six key extraocular muscles, which have the following functions: o Medial Rectus – Adduction o Lateral Rectus – Abduction o Superior Rectus – Elevation, intorsion and adduction o Inferior Rectus – Depression, extorsion and adduction o Superior Oblique – Intorsion, depression, abduction o Inferior Oblique – Extorsion, elevation, abduction o Note: Levator Palpebrae Superior is another eye muscle and is responsible for elevation of the eyelid All four Rectus Muscles originate from the Common Tendinous Ring (CTR), whilst the Superior Oblique and Levator Palpebrae Superior originate from the Sphenoid Bone and the Inferior Oblique originates from the Maxilla Bone Innervation of the eye muscles are via: o Superior Oblique Muscle – Trochlear Nerve (CNIV) o Lateral Rectus Muscle – Abducens Nerve (CNVI) o Other Remaining Eye Muscles – Occulomotor Nerve (CNIII) - - 47 - ‘H-shaped’ eye muscle test will assess the six extraocular eye muscles by isolating the actions of each of these muscles individually o Superior and Inferior Rectus can be tested in isolation during abduction, whilst Superior and Inferior Oblique can be tested in isolation during adduction VISUAL PATHWAYS – PHYSIOLOGY Identify the structure of the retina, the types, function and density of photoreceptors and the concept of parallel ganglion cell processing - Retina is part of the CNS, and is the location where light is converted into an electrical signal o The Retina will process the light input and sends an edited / processed electrical signal to the Cortex o Part of the processing conducted by the Retina is to compare the light intensity levels of different parts of the visual field There are ~10 layers of the Retina, with the Photoreceptor Cells (i.e. Rods and Cones) being the deepest layer of the Retina o Rods are the photoreceptors that are highly sensitive and useful for night-time vision, but only delivers poor visual acuity o In contrast, the Cones are photoreceptors that are useful for day vision, colour vision (as each of the three sub-types of cones [L, M, S] express pigments that detect different wavelengths [Red, Green, Blue respectively]) and high visual acuity Photosensitive pigments (Rhodopsin and Opsins) are highly concentrated in the outer regions of the photoreceptors o These photosensitive pigments have the structure of a G-protein coupled receptors (e.g. 7 transmembrane domains, coupled protein) and are bound (via the protein) to Retinal (which is a Vitamin A derivative) Stimulation of photoreceptors by light will produce Hyperpolarisation, whilst darkness produces Depolarisation o Depolarisation in the dark is due to the presence in the outer segments of the Photoreceptors of high concentrations of cGMP This depolarisation will trigger the constant release of Glutamate from the photoreceptor o cGMP will keep the Cationic Membrane Channels open, thus enabling the inflow of positive ions (e.g. Na+, Ca2+) This inward flow of positive ions will result in the depolarisation of the membrane of the photoreceptors Note: There is also an outward flow of K+ ions too, and this combination of inwards Na+ and Ca2+ plus outward flow of K+ ions is known as the ‘Dark Current’ o In contrast, hyperpolarisation in the light occurs due to light resulting in a reduction in the concentration of cGMP in the outer segments of the Photoreceptors (i.e. Phototransduction) This will close the Cationic Membrane Channels, thus preventing the inflow of Na+ and Ca2+ ions However, there is still an outward flow of K+ ions, so the membrane of the photoreceptor will become hyperpolarised Note: The hyperpolarisation (i.e. electrical signal) will decrease the release of Glutamate (i.e. neurotransmitter) from the photoreceptor This reduction in the rate of release of Glutamate is the signal that is transmitted to post-synaptic neurons Phototransduction Process that results in light triggering reduction in cGMP and hyperpolarisation involves: o Retinal (i.e. Vitamin A derivative) will be in the conformation ‘11-cis’ in the dark, which results in the inactivation of the photosensitive pigment Rhodopsin However, exposure to light (i.e. photoisomerisation) will result in the Retinal changing conformation to ‘All-trans’ - - - - 48 - - - This ‘All-trans’ Retinal will induce conformational changes in the protein aspect of Rhodopsin, resulting in the activation of Rhodopsin o Activated Rhodopsin will move within the membrane and collide with an inactive G-Protein This binding of Rhodopsin to the G-Protein (Alpha sub-unit) will induce conformation changes in the G-Protein (Alpha sub-unit), which causes it to exchange GDP for GTP o This active G-Protein (Alpha sub-unit) will move in the membrane and collide with Phosphodiesterase This binding of active G-Protein (Alpha sub-unit) with Phosphodiesterase will induce a conformation changes in the Phosphodiesterase molecule, which causes it to expose its catalytic site for the breakdown of cGMP to GMP As a result, there will be a reduction in cGMP (due to its breakdown to GMP) o Therefore, exposure to light will trigger a secondary messenger amplification cascade that results in a reduction in cGMP and a closure of the Cationic Membrane Channel Note: There is an Amplification Cascade as each photon will interact will only a single Rhodopsin molecule, but each Rhodopsin molecule will interact with hundreds of G-Proteins, which each interact with hundreds of Phosphodiesterase molecules, which each can breakdown hundreds of cGMP molecules Photoreceptors transmit a signal to Bipolar Cells via the neurotransmitter Glutamate (whose rate of release will vary depending on the polarisation level of the photoreceptor membrane) o There are ~10 different Bipolar Cells (9 of which connect to the Cones, and only 1 of which connects to the Rods) o However, the various types of Bipolar Cells can be classified into two main categories – ON vs. OFF Bipolar Cells ON Bipolar Cells respond in a different way to OFF Bipolar Cells to the same change in neurotransmitter Glutamate ON Bipolar Cells will depolarise in the presence of light (i.e. reduced Glutamate levels), and result in increased activity of the downstream Ganglion Cell (which transmits signal to LGN of Thalamus) OFF Bipolar Cells will hyperpolarise in the presence of light (i.e. reduced Glutamate levels), and result in decreased activity of the downstream Ganglion Cell (which transmits signal to LGN of Thalamus) The presence of these two different categories of Bipolar Cells increases our ability to discriminate light levels This is an example of Parallel Processing of Light Levels (i.e. two different systems send signals related to the same input) Receptive Field surrounding a Retinal Ganglion Cell will have an inner excitatory circle known as the ‘Excitatory Centre’, followed by an outer inhibitory circle, known as the ‘Inhibitory Surround’ o This can result in the Mach Bands visual illusion (i.e. uniform band of grey appears to change colour shade from left to right, as there is a darker band of grey on the left and a lighter band of grey on the right) o The presence of an Excitatory Centre and Inhibitory Surround will result in the perception of a difference / change in colour within each individual band, as the Retina will receive different inputs from the adjacent bands (which are different colours) towards the edge of the band of focus This phenomenon of ‘Lateral Inhibition’ results in different levels of Inhibition from the Inhibitory Surround, causing the visual illusion of a change in colour This serves the function of enhancing the contrast between two adjacent regions of similar colour This is one example of the type of processing of visual input conducted by the Retina Trichromatic Colour Vision results from the three sub-types of Cones each having pigments that are sensitive to light of different wavelengths o There are three different genes that encode for the three different pigments with different wavelength sensitivities 49 o - - - The incidence of colour vision problems in much higher in males compared to females (as the L and M genes are on the X Chromosome, which males only have one copy) The Central Area of the Fovea only posses L and M cones (but no S cones) o Each of these cones are connected to a single ON Bipolar Cell and a single OFF Bipolar Cell, which then each connect to a single Ganglion Cell o One-to-one transmission ratio contributes to higher visual acuity of signals from the Fovea There are multiple types of Ganglion Cells that each detect specific features / information, including local contrast detectors, wavelength sensitive (i.e. colour), direction selective, fast motion detectors and luminosity detectors o Direction selective Ganglion Cells will transmit signals depending on the direction of the light input (and hence can provide an understanding of the motion of an object) Every single point in the Retina is covered by a Receptive Field of a different type of Ganglion Cell o Thus, every single point of the Retina hit by a light source will be simultaneously analysed with regards to its contrast, colour, movement and other characteristics this phenomenon is referred to as ‘Parallel Processing’ o Each of the different types of information will be transmitted via separate channels to the Thalamus / Visual Cortex where it will be interpreted holistically Describe retinal diseases and approaches to their treatment - Common causes of blindness / pathologies of the eye include: o Age-Related Macular Degeneration Dry version is a slow, progressive disease with a decline in central visual function Wet version is a rapid disease that results from neovascularisation of abnormal retinal vessels that then leak proteins and lipids (resulting in substantial vision loss) o Glaucoma This will affect the peripheral vision initially, and so many patients will not recognise this visual field loss until it has significantly progressed This involves enlargement of the Optic Cup, such that there is a loss of neuroretinal rim surrounding the Optic Cup (but still within the Optic Disc) If the neuroretinal rim width does NOT follow Inferior >Superior>Nasal>Temporal (‘ISNT Rule’), then Glaucoma is present o Cataract This involves clouding of the Lens leading to a decrease in vision and will develop slowly over time (especially with ageing) o Diabetic Retinopathy This will involve microvascular complications leading to microaneursyms, dot / blot haemorrhages, cotton wool spots, neovascularisation, etc. o Central Retinal Artery Occlusion This will result in the whole of the Fundus appearing whitish due to being ischaemic and oedematous However, the Fovea / Macular may appear relatively normal (i.e. ‘cherry-red spot’) as the Retina is very thin at this point (and hence can be supplied by the Choroidal Circulation) Furthermore, the Optic Nerve will be a normal colour as this is supplied by the Choroidal Circulation (i.e. Ciliary Arteries) o Giant Cell Arteritis Patients will present with the appearance of a Central Retinal Artery occlusion, BUT ALSO with a very pale Optic Nerve This indicates the Optic Nerve is also ischaemic too, and hence both the Retinal and Choroidal Circulation are affected this suggests an occlusion of the Ophthalmic Artery Describe visual pathways from the retina to other brain areas - Conscious vision (i.e. motion and colour) are transmitted via the Magnocellular (motion) and Parvocellular (Colour) ganglion cells respectively to the LGN of the Thalamus 50 o - - LGN of the Thalamus will then project to Layer IV-C of the Primary Visual Cortex, which then projects to the Secondary and Association Visual Cortices o Areas of the Visual Cortex away from V1 will become more specialised / specific (e.g. V5 Cortex focusing on movement and facial recognition vs. V4 focusing on colour and object perception) Intrinsically Photosensitive Ganglion Cells are cells that express the photopigment Melanopsin, and can capture information about the absolute (NOT relative) level of light o These can detect light independent on any inputs from photoreceptors or Bipolar Cells o These cells will transmit signals to the Suprachiasmatic Nucleus of the Hypothalamus (i.e. area of the brain associated with Circadian Rhythms), and hence is important in setting the biological clock and regulating activity / Melatonin levels These cells will also send signals to the IML, and hence play a role in controlling pupil diameter Retina also has connections to the Pretectum of the Midbrain and Superior Colliculus that will enable particular eye reflexes and certain eye and neck movements (e.g. attention / avoidance) o There are also projections to the Pulvinar of the Thalamus that will integrate with other audition and somatosensory inputs to identify relevant objects and drive attention on these objects (via its connections to the Superior Colliculus) ANATOMY AND PHYSIOLO GY OF THE LENS AND ACCOMMODATION Describe the two forms of cells in the lens (i.e. epithelial cells and fibre cells), and that their proliferation and differentiation determines lens growth - The Lens develops from the part of the Ectoderm (Lens Placode) that is adjacent to the part of the Optic Vesicle that will eventually develop into the Retina o The Lens Placode will thicken and invaginate inwards to form the Lens Pit Note: The Retina-part of the Optic Vesicle will invaginate with the Lens Placode too o The Lens Placode will separate inwards off the Ectoderm to form the Lens Vesicle (which forms the Lens) o The Ectoderm that replaces the Lens Placode (i.e. on the surface of the Lens Vesicle) will form the Cornea o Note: There are molecular interactions between the Retina, Lens Placode and Cornea to ensure the Lens forms in front of the Retina, and the Cornea forms in front of the Lens There are two main types of cells within the lens: o Epithelial Cells (which attach firmly to the Lens Capsule); and o Fibre Cells Lens Epithelium will form from the anterior half of the Lens Vesicle, whilst Primary Fibres of the Lens are formed from the posterior half of the Lens Vesicle o The Lens will grow over time as Lens Epithelium cells will divide ‘Germinative Zone’ is a circular band of Lens Epithelium cells above the equator where most of the Lens Epithelium Cell division will occur The rate of proliferation of Lens Epithelium Cells in the Germinative Zone is much slower than the rate of proliferation in other parts of the body (e.g. skin) in the Adult o The progeny of the cell divisions of the Lens Epithelium that travel below the equator will differentiate / elongate into Secondary Fibres of the Lens, which result in the growth of the Lens o Note: Everything within the Lens will remain in the Lens, as it is surrounded by an extremely thick extracellular matrix (i.e. Lens Capsule) - - Describe dynamics of fibre differentiation and that the acquisition of their hexagonal shape and curvature is important for lens structure and function - There is high level of cellular organisation / packing / order of the fibres of the Lens (e.g. the apical tips of the Fibres of the Lens will form ‘Y-shaped’ sutures) o There will a ‘Y-shaped’ suture at both the Anterior Pole and Posterior Pole of the Lens 51 o - - - - - These ‘Y-shaped’ sutures will become increasingly complex with age (rather than being the simple Y-shape that is present in the Lens of a Foetus) Epithelium Cells that shift below the equator will differentiate into Secondary Fibres of the Lens o It will elongate in size and initially be concave in shape o However, as the cell continues to elongate, it will change shape to initially straight and then convex o These cells undergo directed migration at both the Anterior and Posterior Poles to eventually form the ‘Y-shaped’ sutures at both the Anterior and Posterior Poles o Directed Migration will ensure the tips of these fibres align perfectly with the tips of fibres from another part of the Lens (which is needed to form the ‘Y-shaped’ sutures) FGF (Fibroblast Growth Factor) induce differentiation of Lens Epithelium Cells into Lens Fibres o There is significant FGF present in the Vitreous Humour (i.e. posterior to the Lens), which induces differentiation of Epithelium cells below the Equator into Secondary Lens Fibres The hexagonal shape of Lens Fibres enables these fibres to pack together closely in a regular pattern (and have minimal space between them [thus avoiding the need for opaque connective tissue between them]) o This regular packing of the lens is critical to ensuring lens transparency! (i.e. avoid Cataracts) There is also Protrusive Processes on each Lens Fibre that interlocks / interdigitates with hole on other Lens Fibres to increase the strength of cell-to-cell adhesion (i.e. like a ‘ball-and-socket’) o The strength of these connections enable the lens to hold together under the significant forces experienced during accommodation Otherwise, the fibres would part under the stress of accommodation and result in Cataracts Furthermore, this avoids the need from connective tissue materials to keep the Lens together (which would be problematic as they are opaque [i.e. Cataracts]) Curvature of Lens Fibres enables the Lens to focus an image precisely on the Retina o Note: Changes to the curvature of the Lens (i.e. accommodation) can occur through contraction / relaxation of the Ciliary Muscle, Zonular Fibres and thus Lens Recognise that good cell-cell communication is central to fluid circulation and transport of small molecules in the lens - Nutrients are derived from Aqueous and Vitreous Humours o Glucose and other sugars enter Lens by simple diffusion assisted by a mediated transfer process o Lens Epithelial Cells express high levels of glucose transporter (GLUT1) to transport glucose from the Aqueous Humour o Lens Fibre Cells express mostly GLUT 3(high affinity glucose transporter), which implies glucose transport from Vitreous Humour Fluid circulation and transport of small molecules in the Lens is hypothesised to be dependent on an ion gradients through the Lens o Equatorial Epithelial Cells possess Na+ pumps that pump Na+ ions out of the lens (and hence will also result in water / fluid flow out of the Lens at the Equatorial Epithelial Cells) o The Na+ ions and fluid will re-enter the lens via the Anterior and Posterior Pole (to rebalance the electrochemical gradient on the inside of the Lens [which became negative due to the pumping out of Na+ ions]) o This continual cycle of fluid (which transports nutrients / metabolites) in and out of the Lens results in a good fluid circulation system o Note: The above is one potential hypothesis for fluid circulation Alternative hypotheses / models for fluid circulation / excretion of nutrients / metabolites include Gap Junctions and Aquaporins o Gap Junctions can mediate cell-to-cell transport of small molecules, and are present in high concentrations in Lens Fibre Cells o Aquaporins are an intrinsic proteins of Lens Fibre Cells, and will enable the transport of water and molecules into and out of the Lens Mutations in Aquaporin genes have been shown to result in Cataracts - - 52 Recognise that the main lens pathologies of the lens are presbyopia and cataract and that both are commonly associated with ageing - ‘Presbyopia’ refers to the loss of ability to accommodate o This is associated with ageing (usually occurs in the 50s) and will result in difficulty focusing on near objects (i.e. long-sightedness) o Major factor is the loss of lens flexibility so that it cannot change its curvature ‘Cataract’ is a disease that occurs when the lens is NOT transparent (and hence cannot appropriately transmit and focus light on the Retina) o This is a common age-related disease (i.e. most people will have some degree of Lens Opacification by the age of 70) - Describe cellular and molecular features of lens pathology - Lens will increase in size over life due to the continued division of the Epithelium Cells o Given everything within the Lens will remain in the Lens (as it is surrounded by an extremely thick extracellular matrix [i.e. Lens Capsule]), there is an increase in density and hence a loss of flexibility of the Lens o This reduction in flexibility will reduce the ability of the person to Accommodate (i.e. ‘Presbyopia’) High concentration of Crystallin Proteins (~90% of total Lens Proteins) within the Lens provides the Lens their refractive properties o The ability of these Crystallin Proteins to remain soluble at high concentrations is CRITICAL!! o Denaturing of Crystallin Proteins (i.e. loss of structure of Proteins) will result in the proteins becoming insoluble and forming aggregates (i.e. Cataracts) that scatter light Modern Cataract Surgery will remove the Lens Fibres (but retains the Lens Epithelium) and replace it with a Plastic Lens Implant o Key complication of Cataract Surgery is Posterior Capsule Opacification (PCO) o This involves the Lens Epithelium (which remains following surgery given their firm adherence to the Lens Capsule) proliferating and progressing posteriorly, but differentiating into opaque fibrous areas (rather than Secondary Lens Fibres) o Whilst fibrosis is a normal wound healing response, this is undesirable in the Lens as it will result in opacity - - ANATOMY AND PHYSIOLO GY OF THE CORNEA Describe the anatomy of the cornea, including its various layers - Cornea is the transparent window at the anterior aspect of the eye that lets light into the Globe o Anterior Chamber filled with the liquid Aqueous Humour is located behind the Cornea o Iris is the coloured structure in the middle of the Aqueous Humour between the Cornea and Lens (with the Pupil being the hole in the centre of the Iris) o Posterior Chamber filled with the liquid Aqueous Humour is located between the Iris and the Lens o Vitreous Humour is a jelly-like substance located behind the Lens o Retina is at the back of the Globe behind the Vitreous Humour Sclera (white and opaque) and Cornea (transparent) are continuous in the eye o The Limbus is the area at the junction of the Sclera and Cornea o The root of the Iris is located adjacent to the Limbus, and this angle is where the Aqueous Humour will drain out of the Anterior Chamber via the Canal of Schlemm o Aqueous Humour is produced from the Ciliary Body, which is located posterior to the Iris in the Angle of the Iris and Ciliary Processes There are several different layers of the Cornea (from superficial to deep): o Epithelium - - 53 - - - This stratified squameous epithelium forms the anterior ~10% thickness of the Cornea and will form a mechanical barrier These cells are joined by Desmosomal Junctions and will be interspersed with pain fibres Damage to Epithelium of Cornea will heal rapidly without any problems o Bowman’s Layer – this is a 10micrometre layer of denser Stroma o Stroma This dehydrated collagen lamellae layer forms 90% of the Corneal thickness This will contain a few fibroblasts that are activated in inflammation Damage to the Stroma will take weeks to months to heal, and will leave a scar o Dua’s Layer – this is a 15micrometre layer of denser Stroma (with few cells) o Descemet Membrane – this is a 10micrometre layer of strong basement membrane for the Endothelium o Endothelium This consists of a simple squameous epithelium of non-dividing cells joined by waterproof Tight Junctions This contains a series of pumps that will pump out water from the Corneal Stroma into the Anterior Chamber (and hence keeps the Corneal Stroma dehydrated and thus transparent) Cornea is avascular nature (which is necessary to ensure the Cornea is transparent) o Nutrients are supplied by the Aqueous Humour and Limbal Vessels o Oxygen is supplied by the Limbal Vessels There is extensive nerve supply within the Cornea arising from the Ophthalmic Branch of Trigeminal Nerve (CNV1) o Nerves are transparent and so can be present without ruining the transparency of the Cornea (unlike blood vessels) o Significant nerve supply ensures the Cornea is very sensitive, which will assist in the prevention of trauma / disruption to the Cornea Anterior Cornea provides ~67% of the Optical Power of the Eye (as this is the main interface between air and liquid in the eye) o Lens only provides ~33% of the Optical Power of the Eye, but this optical power is variable by changing the shape of the lens (which enables accommodation!) o Note: The other key function of the Cornea is to protect the deeper structures of the eye (hence presence of tough stroma and significant innervation) Identify the anatomy of the ocular surface, including eyelids and conjunctiva - Eyelids consist of skin, muscle (e.g. Orbicularis Oculi, Levator Palpebrae Superior), fibrous tissue (e.g. Tarsal Plates), Tarsal Glands, Orbital Septum and Conjunctiva o Eyelids are particularly important to protect the Cornea from trauma, excessive light, chemicals, dryness, etc. o Eyelids can retract / drop to enable vision upwards / downwards respectively Fibrous Tissue of the Eyelids (i.e. Tarsal Plates) gives the eyelids shape / structure Tarsal Glands (also known as Meibomian Glands) are important for the development of the Tear Film on the surface of the Cornea by producing the Superficial Lipid Layer o This Superficial Lipid Layer prevents evaporation of the deeper Aqueous Layer of the Tear Film (which is secreted by the Lacrimal Glands) o There is also a Mucous Layer adjacent to the Corneal Epithelium, which acts to enable ‘wetability’ of the bilipid Corneal Epithelium (and is secreted by the Lacrimal Gland and Conjunctival Goblet Cells) o Note: Function of Tear Film is protection, support and nutrition of the Cornea and Conjunctiva, as well as smoothing the surface of the Cornea (i.e. optimise Optical Interface) As such, the Tear Film will contain ions, antibodies, antibacterials, metabolites and inflammatory mediators Conjunctiva in a thin, vascular, transparent mucosa consisting of stratified epithelium o This will adhere to the Limbus, the Globe and reflect onto underside of Eyelids - - 54 o This has a good ability to regenerate, but only a few nerves Describe some common conditions relating to the ocular surface and their management, including chemical burns, blepharitis and dry eyes - ‘Corneal Ulcer’ will refer to the loss of Corneal Epithelium and the exposure of the Corneal Stroma o Fluorescein is a substance that is absorbed by the Corneal Stroma, so it can be used to assess whether the Corneal Stroma is exposed (i.e. presence of Corneal Ulcer) o Note: Bottom 1/3 of the Cornea are more likely to be exposed, and hence are more likely to be the site of a Corneal Ulcer Optical aberrations of the eye include: o Myopia (i.e. focal point is prior to the Retina) o Hyperopia (i.e. focal point is post the Retina) o Astigmatism (i.e. Cornea is not perfectly spherical, resulting in different focal points for light approaching the vertical meridian vs. horizontal meridian) o Note: Treatment may involve glasses, contact lenses, LASIK surgery, etc. ‘Arcus Senilis’ involves the deposition of cholesterol and lipids in the peripheral Corneal Stroma o This occurs with age, but typically does not affect vision ‘Blepharitis’ involves inflammation of the eyelid margins o This can result in foaming on the lid margin as a result of bacteria metabolising the fatty exudates from the inflamed Tarsal Glands o This will usually be chronic and symmetrical, resulting in red, gritty, dry eyes o Treatment involves applying warm compress to the eyelids (as the warmth will melt the fatty exudates within the eyelids) and following with a eyelid massage (which will push the fatty exudates out) ‘Chalazion’ involves the blockage of the Meibomian Gland, resulting in the formation of round, painless nodules in the eyelid (consisting of retained secretions from the Meibomian Gland) o This may disappear spontaneously is ~3-6 months o Treatment will be similar to Blepharitis (i.e. warm compress and massage), although an incision may be made to cut out the nodule ‘Foreign Body’ stuck to the inner surface of the eyelid may cause vertical scratches of the Cornea (as a vertical scratch will occur with every blink) o Foreign bodies will result in pain, redness and potentially infection / iritis o Foreign bodies can be removed with either a cotton body or needle, and may involve application of topical antibiotics If using a needle, always keep it tangential to the eyeball (to minimise the risk of puncturing the globe) o Note: Remember to exclude penetrating injury (i.e. into the Anterior Chamber) if there is a foreign body! This involves applying Seidel’s Test (i.e. apply Fluorescein to the eye and assess whether there is an outflow of Aqueous Humour that pushes the tear film on the Cornea away [which only occurs in a Penetrating Corneal injury]) Complete rupture / puncture of the Cornea can result in the Aqueous Humour flowing out the eye and the pulling of the Iris towards the Cornea Any complete rupture of the Cornea is an emergency and will require immediate treatment via sutures to close this rupture (and hence make the Cornea watertight) ‘Chemical Injury’ should be treated with immediate and copious irrigation (i.e. water, saline) o This will wash out / remove chemicals and minimise the damage to the eye ‘Herpetic Dendritic Ulcer’ is typically unilateral and recurrent o This will result in a red, sore eye, but can be treated with an Acyclovir ointment ‘Corneal Abscess’ will result in a white, opaque spot on the Cornea (i.e. infiltrate) o This can result in pain, redness and decreased vision o This will require immediate referral to an Ophthalmologist! ‘Keratoconus’ refers to thinning and pointing of the Cornea, which will result in large refractive errors o Treatment will require replacement with a Corneal Transplant / Graft - - - - - - 55 BASAL GANGLIA BASAL GANGLIA CIRCUI TRY – NORMAL Identify anatomy of the basal ganglia nuclei (e.g. caudate-putamen, globus pallidus, subthalamus, substantia nigra and pedunculopontine nucleus) - There are six nuclei in the Basal Ganglia: o Caudate and Putamen (i.e. Striatum) Caudate and Putamen are known together as the ‘Striatum’ and are one functional mass (albeit separated by the Internal Capsule) Note: Rostrally, both structures remain continuous (i.e. are NOT separated by the Internal Capsule) Caudate will wrap around adjacent to the Lateral Ventricle Tail of Caudate will become the Roof of the Inferior Horn of the Lateral Ventricle Rostral part of the tail of the Caudate will become the Amygdala (which itself is located immediately in front of the Hippocampus) Striatum will contain: Spiny projection cells (GABA-Sp and GABA-Enk) (i.e. inhibitory) to the Global Pallidus Aspiny interneurones cells (GABA- and Ach+) Striatum will receive afferent inputs from the Somatosensory, Motor and Prefrontal Areas of the Cortex, as well as from the Substantia Nigra Pars Compacta The main outputs from the Striatum are to the Globus Pallidus o Globus Pallidus Globus Pallidus has two distinct cytoarchitectonic regions (per below), and is located adjacent to the Putamen Globus Pallidus Internus – this is the internal / medial segment of the Globus Pallidus Globus Pallidus Externus – this is the external / lateral segment of the Globus Pallidus Both the Globus Pallidus Internus and Externus contain large GABAergic inhibitory cells The main afferent inputs are from the Striatum and Subthalamus Main outputs are to the Ventral Lateral Nucleus of the Thalamus (i.e. motor component of the Thalamus), Subthalamus and Pedunculopontine Nucleus o Subthalamus Subthalamus is extremely closely connected to the Globus Pallidus, and is located below the Thalamus Afferent and efferent connections are to the Globus Pallidus and Substantia Nigra Pars Reticulata Subthalamus is an extremely active / frisky region full of excitatory Glutaminergic cells o Substantia Nigra There are two main components of the Substantia Nigra: Substantia Nigra Pars Reticulata – this is very similar to the Globus Pallidus Internus (i.e. same type of cells and connections) and can be almost viewed as a single entity (for functional purposes) o Hence, this receives afferents from the Subthalamus, send efferents to the Thalamus and Pedunculopontine Nucleus and contains GABAergic inhibitory cells Substantia Nigra Pars Compacta – this contains the Dopaminergic Cells and contains Neuromelanin o This receives afferents from the Cortex and sends efferents to the Striatum 56 o o Note: Dopamine can be either excitatory or inhibitory depending on the post-synaptic receptor o Note: Melanin is a by-product of the production of Catecholamines (e.g. Dopamine) as a result, this region of the brain is black (due to the presence of Neuromelanin) Pedunculopontine Nucleus This forms part of the Brainstem Reticular Formation (and hence is an important part of the Reticulospinal Tract, which plays an important role in locomotion and muscle tone) This region contains both Cholinergic and Glutaminergic Neurons (both excitatory) This region of the Basal Ganglia will receive inputs from the Globus Pallidus and Substantia Nigra Pars Reticulata, and sends outputs to the Spinal Cord Identify normal circuitry and major connections (+neurotransmitters) of the basal ganglia (direct and indirect pathways) - Direct Pathway of the Basal Ganglia involves activating the Thalamus and Pedunculopontine Nucleus o Activation of the Thalamus will result in a message then being transmitted to the Cortex, which then originates skill movements o Similarly, activation of the Pedunculopontine Nucleus will originate global movements(e.g. locomotion) o Therefore, the activation of the Thalamus and Pedunculopontine Nucleus (i.e. Direct Pathway) enables all types of movements Indirect Pathway of the Basal Ganglia involves suppressing unwanted movements, and hence will enable the brain to focus upon the desired movements Direct Pathway originates in the Striatum via the GABA-SP Neurons o These send inhibitory projections towards the Globus Pallidus Internus, which itself sends inhibitory GABAergic projections towards the Active Zone of the Thalamus and Pedunculopontine Nucleus o Hence, increased GABA release from the Striatum will ultimately result in greater activation of the Active Zone of the Thalamus and Pedunculopontine Nucleus (thus resulting in excitation / activation of movement) Indirect Pathway originates in the Striatum via the GABA-Enk Neurons o These send inhibitory projections towards the Globus Pallidus Externus, which itself sends inhibitory GABAergic projections towards the Subthalamus o Subthalamus sends excitatory Glutaminergic projections towards the Globus Pallidus Internus, which itself sends inhibitory GABAergic projections towards the Suppressed Zone of the Thalamus and Pedunculopontine Nucleus o Hence, increased GABA release from the Striatum will ultimately result in greater activation of the Subthalamus and hence greater inhibition of the Suppressed Zone of the Thalamus and Pedunculopontine Nucleus (thus resulting in inhibition / suppression of movement) Substantia Nigra will operate in the Active Zone only (in both the Subthalamus and Pedunculopontine Nucleus) and make this area as excited as possible o Dopaminergic connection from the Substantia Nigra to the Striatum will excite the Direct Pathway AND inhibit the Indirect Pathway Excitation of the Direct Pathway will further excite the Active Zone Inhibition of the Indirect Pathway will further excite the Active Zone (by removing any inhibition of the Active Zone) o This difference in excitation vs. inhibition occurs due to different types of post-synaptic receptors in the Direct vs. Indirect Pathways There are D1 Receptors (excitatory) on the GABA-SP Neurons compared to D2 Receptors (inhibitory) on the GABA-Enk Neurons Insufficient Dopamine will result in relative inhibition of the Direct Pathway and excitation of the Indirect Pathway (which together results in less activation of the Active Zone) o However, the Direct Pathway may still be activated via the release of excitatory Glutamate from the Cortex - - - - 57 o - In contrast, the Indirect Pathway will be overexcited without Dopamine as the Cortex is not able to inhibit this pathway (as it only able to release excitatory neurotransmitters to the Basal Ganglia) This will result in an overactive Subthalamus, ultimately resulting in the Global Pallidus Internus excessively inhibiting the Active Zone It is the excessive excitement of the Indirect Pathway that is the key problem arising from Dopamine insufficiency Note: The precise Active Zone and Suppressed Zone will change depending on the particular movement required Describe suspected functions associated with the basal ganglia and the way in which these nuclei may work in the great scheme of motor control system - There are suggestions the Basal Ganglia plays an important role in: o Focusing on particular actions and / or thoughts o Planning actions / movements (via linking different cortical areas together), including converting idea of movement into the expression of the movement For example, Secondary Motor Cortex (which is main area for planning movement) will receive Proprioceptive information from the Somatosensory Cortex via the Basal Ganglia Similarly, Secondary Motor Cortex can receive information on social norms from the Prefrontal Association Cortex via the Basal Ganglia o Storing Automated Motor Programmes (e.g. writing, dancing, locomotion, etc.) Automated Motor Programmes are learned via the Cerebellum but are stored in the Basal Ganglia Therefore, problems with Basal Ganglia can result in difficulty in starting / initiating these Automated Motor Programmes as well as stopping these Automated Motor Programmes BASAL GANGLIA CIRCUI TRY – ABNORMAL Describe the abnormal circuitry and suspected mechanisms behind the signs and symptoms of Parkinson disease and other motor disorders such as chorea and ballism - Parkinson’s Disease involves the loss of Dopaminergic Cells in the Substantia Nigra, which will result in the loss of the Dopaminergic Terminals / terminations in the Striatum o This loss of Dopaminergic input results in failure to inhibit the Indirect Pathway, ultimately resulting in the increased inhibition of the Thalamus and Pedunculopontine Nucleus o Note: Loss of Dopaminergic input has less of an impact on Direct Pathway, as this can still be stimulated via Glutamate release from the Cortex o Note: Signs of Parkinson’s Disease will result after the loss of ~50-70% of the total Dopaminergic Cells / Terminals Tremor of Parkinson’s Disease is associated with the Thalamus (i.e. via projection to Cortex which controls skilled movements) o Anterior aspect of the Ventral Lateral Nucleus of the Thalamus (i.e. motor nucleus) is supplied by the Globus Pallidus Internus (and hence Indirect Pathway), whilst the Posterior aspect of the Ventral Lateral Nucleus of the Thalamus is supplied by the Cerebellum o These two inputs are in equilibrium in normal people o However in Parkinson’s Disease, the anterior aspect in excessively suppressed, resulting in excessive Cerebellum input o This excessive Cerebellum input is what causes the bursts of activity from the Thalamus to the Cortex that ultimately results in Tremor Therefore, treatment for excessive Tremor in Parkinson’s Disease can involve surgical reducing the inputs from the Cerebellum (to re-achieve equilibrium) Statues of Parkinson’s Disease is associated with increased inhibition of the Pedunculopontine Nucleus (i.e. which controls global movements) - - 58 o o - Akinesia / Bradykinesia results from reduced stimulation of the Alpha-Motor Neuron Rigidity results from reduced stimulation of the Interneuron, which results in increased stimulation of the Alpha-Motor Neuron responsible for muscle tone (i.e. hypertonia) Chorea involves degeneration of the GABA-Enk cells will result in a lessening of the volume of the Striatum and an underactivity of the Indirect Pathway o This ultimately results in insufficient suppression of unwanted movements, resulting in Dyskinesia (i.e. opposite of Parkinson’s Disease) Describe which pathways degenerate and which are over- and under-active - Parkinson’s Disease involves the loss of Dopaminergic Cells in the Substantia Nigra, which will result in the loss of the Dopaminergic Terminals / terminations in the Striatum o This loss of Dopaminergic input results in failure to inhibit the Indirect Pathway (i.e. overactivity of Indirect Pathway), ultimately resulting in the increased inhibition of the Thalamus and Pedunculopontine Nucleus o Note: Loss of Dopaminergic input has less of an impact on Direct Pathway, as this can still be stimulated via Glutamate release from the Cortex Chorea involves degeneration of the GABA-Enk cells of the Striatum, which will result in a lessening of the volume of the Striatum and an underactivity of the Indirect Pathway o This ultimately results in insufficient suppression of unwanted movements (i.e. excess activation of the Thalamus and Pedunculopontine Nucleus), resulting in Dyskinesia (i.e. opposite of Parkinson’s Disease) - MOVEMENT AND ASSOCIATED DISORDERS MOTOR DISORDERS Describe the phenomenon of involuntary movements, pathophysiology of dystonia and the classification of movement disorders (video examples will be included in this lecture) - Movement disorders can be classified as: o Hyperkinesia (including Dystonia) o Tremor o Akinesia o Ataxia Dystonia is an extremely broad condition that encompasses numerous difference diseases (e.g. Chorea, Ballismus, Tardive Dyskinesia, Athetosis, etc.) o Dystonia is a syndrome of involuntary, sustained, often repetitive contractions of opposite muscles that lead to abnormal movements or posture (e.g. twisting) o Onset is common in childhood / adolescence (i.e. ~5-10 years) Each patient with Dystonia will have the same type of muscle contractions throughout life (resulting in the same appearance throughout life) o However, each patient with Dystonia may have a different set of muscles that are contracting (and hence will have a different appearance) Pathophysiology of Dystonia involves: o Being unable to suppress particular muscles (i.e. cannot suppress antagonist muscles, and instead activate both agonist and antagonist muscles [i.e. ‘Co-Contraction’]) This occurs due to reduced GABA inhibitory signal from the Global Pallidus Internus (and hence results in a failure to suppress the unwanted movements via the Thalamus) o Failure to link sensation to motor function As a result, sensory inputs may not affect motor function resulting in involuntary movement This is why it is believed peripheral injuries can sometimes result in a Focal Dystonia (due to the disruption of sensory input to motor function) - - - 59 o - - - Abnormal Plasticity There may be an overlap in the somatosensory areas of the brain in Dystonic patients This can cause disorganised somatotopic representation and disturbance of afferent inputs, which may then trigger abnormal movement representation The different types of Dystonia include: o Focal Dystonia Blepharospasm – this involves involuntary twitching, blinking, closure or squeezing of the eyelids and is a common type of Dystonia Laryngeal Dystonia – this involves a voice disorder due to involuntary movement / spasm of the larynx muscles during speech Cervical Dystonia (also known as Spasmodic Torticollis) – this involves involuntary contraction of the neck muscles, resulting in twisting and turning of the head / neck to one side or back / forwards o Task-Specific Dystonia (which is often unilateral and can result from overtraining) Writer’s Cramp Musician’s Cramp Putter Dystonia (also known as ‘Yips’) Dystonia can also be classified between Primary Dystonia (i.e. Dystonia in the absence of any apparent cause) and Secondary Dystonia (i.e. Dystonia due to another cause) o Causes of Secondary Dystonia include Metabolic, Neurodegenerative, Structural, Vascular, Infection, Trauma, Tumour, Toxins, Medications, etc. o There are also genetic mutations associated with Dystonia (which mostly are located / effective within the Basal Ganglia) Botox is a highly effective treatment for Dystonia, as this will travel retrogradally into the pre-synaptic nerve terminal and will block Acetylcholine release (and hence prevents muscle contraction) Other types of Dyskinesia / Hyperkinesia beyond Dystonia include: o Athetosis – this will involve slow, irregular, writhing movements of the digits and face o Chorea – this involves brief, constant pseudo-purposeful motion that is unpredictable and may appear ‘dance-like’ This can be caused by Huntington’s Chorea (genetic), Auto-Immune Chorea (e.g. SLE), Sydenham’s Chorea (e.g. Rheumatic Fever) or Chorea from Blood Disorders (e.g. Polycythaemia) o Tardive Dyskinesia – this involves repetitive movements including tongue protrusion, grimacing, bucco-lingual, lip smacking, puckering, etc. in addition to fast limb movements This is more likely in females and the elderly, and can result several years after the treatment with Neuroleptics o Tardive Dystonia – this involves Retrocollis and repetitive motions This is more likely to affect young males, and can result several years after the treatment with Neuroleptics o Akathisia – this refers to the inability to sit still (although there is some suppressability in the immediate-term) o Hemiballismus – this involves proximal-to-distal flinging / throwing movement that may appear ‘dance-like’ o Myoclonus –this involves brief involuntary twitching CEREBELLUM – COORDINATING MOVEMEN T Identify structure and function of the cerebellum - Cerebellum is located in the Posterior Cranial Fossa and covered superiorly by the Tentorium Cerebelli Key landmarks of the Cerebellum include the: o Arbor Vitae – this is the branched, tree-like Cerebellar White Matter o Culmen – this is the highest / most rostral aspect of the Cerebellum o Primary Fissure – this is the deepest fissure within the Cerebellum o Fastigium – this is the point where the White Matter of the Cerebellum comes together 60 o - - - - - - Roof of the fourth ventricle formed by Superior and Inferior Medullary Vellum Superior Medullary Velum is the inferior component of the Superior Cerebellar Peduncle Inferior Medullary Velum is inferior to the Superior Medullary Velum, and contains some Choroid Plexus on its surface There are three lobes within the Cerebellum: o Anterior Lobe – this is anterior to the Primary Fissure o Posterior Lobe – this is posterior to the Primary Fissure o Flocculonodular Lobe – this is a structure located inferior to the Anterior Lobe and is adjacent to the dorsal Brainstem There are three Cerebellar Peduncles (visible on the anterior aspect of the Cerebellum): o Superior Cerebellar Peduncle (mainly output fibres) o Middle Cerebellar Peduncle (contain fibres from the Pons that innervate the contralateral Cerebellar Hemisphere) o Inferior Cerebellar Peduncle (both input and output fibres) Vermis is the medial aspect of the Cerebellum, whilst the Hemispheres (i.e. lateral lobes) are the lateral aspects of the Cerebellum The Cerebellum has two somatotopic body maps roughly similar to the homonculi (though not as continuous and precise as the Cortex Homonculi) o One representation in the midline of the Anterior Lobe provides a full body map focused on global movement (with each Cerebellar Hemisphere representing movement of the ipsilateral limb) Hence, lesion of the Anterior Lobe may result in Ataxic Gait Note: Head and Trunk are represented on the midline itself, with limbs represented adjacent laterally o One representation towards the midline of the Posterior Lobe provides a fully body map focused on skilled movement Hence, lesion of the Posterior Lobe may result in Intention Tremor, Dysmetria, etc. Note: Head and Trunk are represented just adjacent to the midline, with limbs represented further laterally o Note: These representations are ‘Fractionated’, which means the somatotopic organisation is not continuous, and instead particular areas of the Cerebellum are associated with specific parts of the body Blood supply from the Cerebellum is via the PICA, AICA and SCA There are three deep cerebellar nuclei (i.e. Dentate, Fastigial and Interpositus Nuclei) o Dentate Nuclei is the easiest of the deep cerebellar nuclei to identify on prosections (most lateral) o Fastigial Nuclei is the most medial nuclei o Interpositus Nuclei (consisting of twin medial nuclei of Globose and single lateral nuclei of Emboliform) is located in-between the Dentate and Fastigial Nuclei There are three layers of the Cerebellar Folia (i.e. Grey Matter) o Molecular Layer – this is the most superficial layer and contains mostly fibres (but not cell bodies) o Purkinje Cell Layer – this is a single layer of very large cells (i.e. can be seen on microscope without staining) o Granule Cell Layer – this is the deepest layer and is full of cell bodies o Note: White Matter of Folia is located deep to the Granule Cell Layer ‘Mossy Fibres’ are the excitatory input fibres to the Cerebellum (whether via the Spinocerebellar or Pontocerebellar Tracts) o Each Mossy Fibre will repeatedly bifurcate and end up with ~1 billion Mossy Fibres Axonal Terminals (i.e. Rosette) in each hemisphere o Each Rosette synapses with ~20 Granule Cells (and hence there are ~20 billion Granule Cells in each hemisphere) o Each Granule Cell sends fibres to the surface of the Cerebellar Cortex (i.e. Molecular Layer), which then bifurcate to form excitatory Parallel Fibres o These Parallel Fibres will then synapse with Purkinje Cells and Basket Cells 61 o - - Each Parallel Fibre will excite the Purkinje Cell it synapses with, but will inhibit the adjacent parallel Purkinje Cell (via its synapse on the inhibitory Basket Cells) This means that only the strongest Parallel Fibre will effectively transmit signals (as the weaker adjacent Parallel Fibres are inhibited from having an effect by Basket Cells activated by the stronger Parallel Fibres) This will ensure the signal via the Parallel Fibres is only for a specific, focused space o There is also an inhibitory feedback loop via the Parallel Fibres synapsing with Golgi Cells These Golgi Cells will send inhibitory signals to the Rosette, and terminate the signal via the Parallel Fibres This will ensure the signal via the Parallel Fibres is only for a specific, focused period of time o The combined effects of the Basket and Golgi Cells will a sharpening of the signal in both space and time ‘Climbing Fibres’ are another source of excitatory input fibres to the Cerebellum o These originate from the contralateral Inferior Olivary Complex o These fibres are strongly excitatory, but are much less numerous than Mossy Fibres o These Climbing Fibres will synapse directly on ~2-10 Purkinje Cells (and do so in such a complete manner that each Purkinje Cell can only receive inputs from one Climbing Fibre) o Repeated Firing of Climbing Fibres will result in a long-term slow-down of Cerebellar Activity (i.e. Long-Term Depression) It has been suggested this may be an adaptive response reflecting Cerebellar Learning The only output from the Cerebellum is via Purkinje Cells, which are GABAergic (i.e. inhibitory), towards the Deep Cerebellar Nuclei o Dentate Nuclei project to the contralateral Ventrolateral Nucleus of the Thalamus (which projects to the Motor Cortices) o Globose, Emboliform and Fastigial Nuclei project to the contralateral Red Nucleus and Reticular Formation (both in the Brainstem) o Lateral Vestibular Nuclei (also known as Deiter’s Nuclei) project to the Vestibulospinal Tract and Reticular Formation Note: Lateral Vestibular Nuclei is located in the Medulla of the Brainstem (and NOT the Cerebellum), but is analogous to the Deep Cerebellar Nuclei (i.e. receives inputs from Purkinje Cells) Identify three major subdivisions of the cerebellum, their connections and function - The three major subdivisions of the Cerebellum are: o Spinocerebellum (also known as Paleocerebellum) This contains the Vermis and Paravermal Regions This receives afferents from the ipsilateral Spinal Cord, and sends efferents to the contralateral Red Nucleus and Thalamus to the Cortex (via the Interpositus and Fastigial Nuclei) This area of the cerebellum is concerned with monitoring movement as it is executed as well as integrating various sensory inputs to plan and execute complex movements Note: There is a region within the Vermis of Cerebellum that receives and represents visual and auditory information (i.e. Visuocerebellum and Audiocerebellum) o Cerebrocerebellum (also known as Neocerebellum or Pontocerebellum) This contains the lateral hemispheres This receives afferents from the Cerebral Cortex via the Pons, and sends efferents to the contralateral Cortex via the Thalamus (via the Dentate Nuclei) This area of the cerebellum is involved in coordinating synergy of different muscle groups to generate complex movements o Vestibulocerebellum (also known as Archicerebellum) 62 - This is similar to the Flocculonodular Lobe and is mainly concerned with maintaining posture and balance This sends efferents to the ipsilateral Lateral Vestibular Nuclei (also known as Deiter’s Nuclei), which sends projections to the Vestibulospinal Tract of the Spinal Cord Cerebellum influences the same side of the patient, so a cerebellar lesion will affect movement / coordination on the same side of the body Describe outcomes of cerebellar dysfunction - Cerebellar dysfunction will vary depending on the location of the lesion, but may result in: o Spinocerebellum lesion No specific known deficits in humans, but could be similar to decerebration in animal experiments Note: Spinocerebellum is associated with integrating sensory inputs to plan movements and monitoring movements as they are executed, so a lesion here may result in failure to perform these activities effectively o Cerebrocerebellum lesion Loss of muscle tone / fatigue Asynergia (i.e. lack of coordination) Dysmetria (i.e. hypermetria / pastpointing) Nystagmus Intention tremor Dysdiadochokinesia Speech disturbances (e.g. slurred speech, separating of syllables) o Vestibulocerebellum lesion Unsteadiness, swaying, falling Tendency to fall backwards when walking Muscle tone not changed all the time Signs are usually bilateral Cerebellum is also involved in pre-programmed automated movement, so cerebellar dysfunction may prevent the learning of such movements (i.e. ‘muscle memory’ in sport, music, etc.) - CLINICAL ASPECTS OF PARKINSON’S DISEASE AND RELATED DISORDERS Describe the cardinal features of Parkinson disease and how it is diagnosed - Cardinal features of Parkinson’s Disease are: o Tremor This occurs when the patient undertakes postures that are driven by sub-conscious motor activities (e.g. sitting, standing, walking) In contrast, this tremor generally does not occur in the patient is completely relaxed (e.g. supine) as the patient is not undertaking a posture, so the term ‘Resting Tremor’ is a misnomer This type of tremor may be elicited by asking patient to walk or conduct a cognitive task (e.g. mathematical problems) However, this type of tremor is suppressed when engaging in a voluntary motor task (and so it’s not really a major problem affecting quality of life) o Hypokinesia / Akinesia / Bradykinesia This involves the suppression of small, ‘fidgety’ movements rather than not being able to do all movements or doing them slowly There is particular trouble with rapidly sequenced repetitive activities (e.g. brushing teeth) o Rigidity This results from involuntary co-contraction of muscles For example, Arm-Swing is commonly reduced in these patients due to involuntary contraction of the muscles of the arm (which reduce passive arm swing 63 - - Note: Co-contraction is a high-energy usage state, so Parkinson’s Disease patients are commonly thin (potentially due to high consumption of energy) Treatment of Parkinson’s Disease is typically with: o Dopamine Precursor and Peripheral Dopa Decarboxylase Inhibitor (e.g. Levodopa with Carbidopa or Benserazide) This will enable the Dopamine precursor to reach the CNS, where it will be converted to Dopamine to replace the deficiency of Dopamine o Dopamine Agonists (e.g. Bromocriptine, Cabergoline, Pergolide) o MAO / COMT Inhibitors (to prevent metabolism of Dopamine) o Tri-Cyclic Antidepressants (to prevent re-uptake of Dopamine) o Anti-Cholinergic Drugs – this rebalances the Dopamine and Cholinergic inputs in the Striatum, resulting in reduced tremor Diagnosis of Parkinson’s Disease will be based on clinical history and signs / symptoms, but will need to be confirmed by observing some response to the combination of Dopamine Precursor and Peripheral Dopa Decarboxylase Inhibitor therapy Describe different types of cerebellar lesions and their associated deficits - - Vestibular system is an integral part of the Cerebellum (and hence Cerebellar lesion will affect balance [as well as coordination]) Nystagmus, Saccadic Dysmetria and Impaired Pursuit are Eye Movement problems associated with Cerebellum lesions o Sacchadic Dysmetria involves the eyes having to conduct multiple Saccadic movements rather than a Single Saccadic movements (as the loss of Cerebellar modulation means the brain not accurately judge the required distance to move [similar to Intention Tremor / Overshooting in Finger Nose Test]) The four eye movement systems (i.e. Saccade, Pursuit, Vestibular, Vergence) all arise from different areas of the brain o Smooth Pursuit Eye Movements are only possible if there is a visual target to tracks (and the visual target does NOT move too fast too) o Lesion of the Cerebellum will result in inability to conduct Smooth Pursuit Eye Movements (and instead it will appear like Saccade Eye Movements only) Focusing on an object when turning the head will enable the suppression of the Vestibular-driven Nystagmus o However, the ability to suppress the Vestibular-driven Nystagmus is dependent on the presence of a Cerebellum (which normally integrates the input from the Visual System to suppress the Vestibular-Driven Nystagmus) o Patients will Cerebellar lesions will continue to have significant Nystagmus even when attempting to track an object whilst the head is turned (as the visual input is not able to suppress the Vestibular-Driven Nystagmus) The Neural Integration of position and velocity is performed in the Brainstem but is modulated by the Cerebellum o There is an issue with this integration when the vision is in lateral gaze (resulting in Lateral Gaze Nystagmus) o When holding the gaze in the lateral position though for a prolonged period, the level of Nystagmus is reduced This occurs as the Cerebellum will over time create an compensatory opposite movement to cancel out the Lateral Gaze Nystagmus However, if the eyes are quickly moved towards the centre, this compensatory opposite movement still occurs resulting in a Rebound Nystagmus in that opposite direction Note: Refer to ‘Cerebellum – Coordinating Movement’ lecture notes for additional information Describe different types of tremor based on their characteristic features - There are several different types of tremor such as: - - - - 64 o o o o Physiological Tremor – this is the standard physiological movement / frequency in all people; this is rarely visible and has no clinical significance Essential Tremor (i.e. Benign Familial Tremor) – this noticeable tremor is inherited, and will be further exacerbated by the same stimuli for tremor as all people (e.g. Adrenaline) Intention Tremor (i.e. Cerebellar lesion) – this occurs at the end of purposeful movement (e.g. touch finger of examiner) Postural Tremor (i.e. Parkinson’s Disease) – this occurs when the body is in certain postures (e.g. sitting, standing, etc.) Describe prognosis and complications associated with Parkinson disease - Parkinson’s Disease is a progressive disease that will ultimately result in significant disability, the loss of independence and death! Late-stage clinical feature of Parkinson’s Disease include: o Loss of righting reflexes o Disordered sleep (e.g. REM Sleep Disorder) o Autonomic dysfunction (e.g. constipation, orthostatic hypotension) o Neuropsychiatric dysfunction (e.g. depression, dementia) o Pain Loss of Righting Reflex will make it difficult over time to remain upright, which can ultimately result in these patients becoming bed-bound (which will eventually result in death!) - - DEMENTIA ANATOMY OF ATTENTION AND MEMORY Identify anatomical regions involved in attention (global and specific) and memory (procedural and declarative) and the connections between these regions - Global Attention involves a subcortical modulatory network in the Brainstem Reticular Formation and Basal Forebrain (i.e. Ascending Reticular Activating System) releasing the following neurotransmitters to activate the Cortex and activate / inhibit the Thalamus (i.e. impose sleep/wake cycle) o Serotonin (released from the Midbrain Raphe) o Dopamine (released from the Ventral Tegmental Area of the Midbrain) o Noradrenaline (released from the Locus Coeruleus of the Pons) o Acetylcholine (released from the Pedunculopontine Nucleus of the Midbrain and Basal Forebrain Nucleus) o Histamine (released from the Tuberomamillary Nucleus of the Hypothalamus) o Orexin (released from the Lateral Hypothalamic Nucleus) o Note: These neurotransmitters are released widely throughout the Cortex (except the Posterior Cingulate Gyrus) Exception is Dopamine, which is NOT released in the Parietal and Occipital Lobes, or Cerebellum (i.e. back half of brain) Exception is Acetylcholine, which is NOT released in the Cerebellum Specific Attention involves multiple different specific attentional centres in the Thalamus and Cortex such as: o Unimodal Thalamus (e.g. LGN, MGN) – this amplifies / filters sensory input to the Cortex (whilst the Corticothalamic loop sharpens and focuses the inputs received by the Cortex) o Superior Colliculus This is responsible for reflexive attention based on visual and somatosensory inputs (as well as enabling ‘blindsight’) Outputs travel to Frontal Eye Fields, Pulvinar and Brainstem areas with direct connections to head and neck muscles o Pulvinar of the Thalamus – this directs attention to novel / relevant stimuli amongst distracters in the environment - 65 o - - - Parietal Association Cortex This combines and integrates various sensory inputs and enables spatial attention (i.e. perception of how body fits into spatial world) (e.g. body awareness, visual field awareness) Lesion of Parietal Association Cortex can result in Neglect Syndrome o Dorsolateral Prefrontal Cortex (DLPFC) – this suppresses distracters, and hence enables shift of attentional focus o Anterior Cingulate Gyrus – this is important for focusing attention (i.e. stimulus selection) and a mediating response (e.g. monitoring errors) Memory is believed to exist within the connections between the different neurons of the brain (rather than being solely in a particular site itself) o For example, Auditory-aspects of Memory will be located in the Auditory Cortex, whilst Visual-aspects of Memory will be located in the Visual Cortex These different areas are connected together to form the specific total memory that includes both these visual and auditory aspects (in addition to other aspects from the other relevant Cortices) o Hippocampal Activity (via Entorhinal Cortex) maintains activity in the relevant network of distributed brain areas, which will enhance the efficiency of these memory networks Procedural Memory (i.e. habits / skills, unconsciously acquired motor programs, etc.) will involve the Basal Ganglia and Cerebellum Declarative Memory (i.e. facts and concepts, autobiographical, episodic, etc.) formation will specifically require the Medial Temporal Lobe (i.e. Hippocampus, Entorhinal Cortex, Amygdala) o Hippocampus and Medial Temporal Lobe will direct long-term declarative memories to be stored in the particular Modality-Specific and Association Cortices o Hence, removal of the Medial Temporal Lobe was shown to prevent formation of any new declarative memories (although older, pre-existing memories will be retained as they are already stored in the Cortex) o Similarly, damage to the Cortex is associated with loss of existing memories (i.e. retrograde amnesia) Note: Left and Right Cortex are associated with particular types of memories; for example: o Unilateral damage to the Right Medial Temporal Lobe will result in a deficit in accumulating Visuospatial memories o Unilateral damage to the Left Medial Temporal Lobe will result in a deficit in accumulating Verbal memories Describe mechanisms involved in short-term and long-term memory and the role of the hippocampus - Hippocampus is a long curved structure located in the floor of the Inferior (also known as Temporal) Horn of the Lateral Ventricle o Hippocampus is continuous with the Subiculum, which itself continuous with the Entorhinal Cortex o Entorhinal Cortex is associated with Olfaction, and is critical to memory accumulation (i.e. removal of Entorhinal Cortex only will result in inability to form new memories [i.e. anterograde amnesia]) Entorhinal Cortex received inputs from the Hippocampus and will project out to the rest of the Cortex Similarly, Entorhinal Cortex received inputs from the rest of the Cortex and projects to the Hippocampus This creates a reverberating, amplifying loop that will reinforce memories, and hence is important for formations of short-term memories Hippocampus and Medial Temporal Lobe will also direct long-term declarative memories to be stored in the particular Modality-Specific and Association Cortices Dorsolateral Prefrontal Cortex plays a key role in short-term working memory, including retrieval of old stored information and strategies for storing new memories - 66 o - The main output is towards the Mediodorsal Thalamus, which thus may be an important structure in memory retrieval (i.e. lesions may result in retrograde amnesia) Neurotransmitters such as GABA and Glutamate will result in greater inhibition of particular receptors, resulting in decreased memory consolidation Sleep improves both procedural and declarative memory consolidation (whilst sleep deprivation reduces memory formation) FUNCTIONAL IMAGING O F THE BRAIN Describe structural and imaging techniques for examining cortical structure and function, focusing on MRI and functional MRI - High resolution in scanning is CRITICAL given the small size of structures in the brain (e.g. <0.5mm) o CT Scans do NOT provide sufficient detail of the various specific cortical tissues (though can detect large haemorrhage or ischaemic areas [i.e. Stroke!]) o In contrast, MRI Scans provide more detailed anatomical images, as well as enabling functional imaging MRI involves lining up protons in tissues with a large magnet and then measuring how long it takes for the protons to return to normal o Length of time to return to normal will vary depending on the type of tissue (which thus enables differentiation of different anatomical structures) o 3-Dimensional MRI images are possible by using gradients of magnetic fields to line up the protons (which thus provides information on the 3D structure) T1 MRI Image will have white matter being white, grey matter being grey and fluid being dark o In contrast, T2 MRI Image will have fluid as white colour (and hence these T2 MRI Images can make it easier to identify pathology, given a lot of pathology is ‘wet’) Structural resolution in MRI images depends upon: o Radiofrequency Pulse Interval (from Magnet) o Magnet strength o Slice interval o Time for acquisition Functional MRI (fMRI) involves the use of Blood Oxygen Level Dependent (BOLD) contrast o This technique provide functional information about the brain (i.e. neuronal activity) o BOLD techniques alone provide poor spatial and temporal resolution, and so are used in conjunction with an high resolution MRI (to provide higher quality spatial and temporal resolution) fMRI with BOLD scan will involve the following sequence: o Step 1 – Conduct a slower high resolution T1 Scan to provide anatomical detail o Step 2 – Conduct a fast low resolution baseline BOLD T2 Scan o Step 3 – Conduct a fast low resolution ‘task’ BOLD T2 Scan o Step 4 – Deduct Step 2 from Step 3 (to isolate task-specific functional activity) and overlay on anatomical detail from Step 1 o Note: Faster speed of BOLD Scan is needed as the action / thought / behaviour being measured will only be present for a short period (rather than the several minutes needed for a high resolution scan) Another type of scan available is Positron Emission Tomography (PET) Scan o This technique can provide information about glucose usage (and hence metabolism) within the brain o Disadvantage is the low spatial and temporal resolution (which is why these scans are commonly overlayed / combined with a CT or MRI Scan) - - - - - - Describe the basis of the fMRI signal and correlation of neuronal activity and blood flow - fMRI images precisely detect differences in oxygenation of blood flow (rather than differences within neurons themselves) 67 o o However, the level of oxygenation within blood flow can act as a proxy for neuronal activity (as more active neurons will require additional blood supply with increased oxygenation) Note: Increased neuronal activity will initially have a dip in blood oxygenation (as oxygen is consumed without the inflow of additional highly oxygenated blood), followed by a significant increase in blood oxygenation (as the inflow of additional highly oxygenated blood occurs) Describe caveats in interpretation of functional studies and future directions in imaging techniques - Key challenge in interpretation of fMRI include: o How to develop the appropriate task to assess for a particular behaviour / emotion Failure to select the appropriate task will result in misleading / incorrect results (as the underlying behaviour / emotion is not actually being recorded) o Difficulty in comparing the tissues across different people (given anatomical variations) o Artifacts arising in MRI scans (especially near junction of tissue and air [e.g. sinuses, ear canal, etc.] or due to motion) Future directions in imaging techniques include: o Diffusion Tensor Imaging (DTI) This will enable tracking of the location and direction of Fibre Tracts in-vivo This is possible as water within fibre tracts (i.e. within lipid tissue of oligodendrocytes) will have limited movement (i.e. high FA) By identifying this limited movement of water, the fibre tracts can be mapped The generation of the map showing the location and direction of Fibre Tracts is currently quite manual (and hence is not ready for clinical use) However, it is a matter of time until these maps can be generated (as it will simply require more powerful mathematical / computing abilities, which can be expected to develop over time) Potential application of this technology in the future will be to identify the location of damaged axons following head trauma o Diffuse Optical Tomography (DOT) or Infrared Optical Imaging (IROI) This is effectively BOLD imaging via infrared light passed into the brain (with optical absorption of haemoglobin) This has potential advantages of allowing monitoring active behaviour, intraoperative imaging and more rapid image / function generation - PRION DISEASES Describe main features of prion disease, including pathogenesis, microscopic changes and symptoms - ‘Prion’ is a shortened term that means ‘Protein-only Infectious Agent’ o There are a range of human (infectious, sporadic and genetic) and animal prion diseases Cellular Prion Protein (PrPc) is a cell surface protein present throughout the body o This protein has a normal amino acid structure, with some Beta-pleated sheets Prion Disease occurs from a conformational change in the harmless Cellular Prion Protein (PrPc) to the pathogenic PrPSc (via the intermediate Beta-PrP) o Intermediate Beta-PrP has more Beta-pleated sheets compared to harmless Cellular Prion Protein It is believed the intermediate form is infectious, though this is still be confirmed o Pathogenic PrPSc has fibrils formed due to packing of various sub-units of the normal Cellular Prion Protein These Fibrils are known to be infectious! Transformation of harmless Cellular Prion Protein (PrPc) into Pathogenic PrPSc is proposed to occur via these possible two mechanisms: - - 68 o - - - - - - - - Mechanism 1 – Interaction with another molecule (‘Protein X’) that facilitates change in conformation to pathogenic form o Mechanism 2 – Harmless form transforms to the Pathogenic form, which then elongates (i.e. ‘seeds’) into Fibrils via addition of the normal Cellular Prion Protein o Note: Evidence has suggested another molecule is not needed for change in conformation, so mechanism 2 is more likely to be the relevant mechanism Route of infection of Prion Disease can be orally, direct inoculation into CNS or contamination of surgical instruments / blood products o Note: There is little evidence of airborne spread of Prion Disease Prion Disease will readily replicate in the Spleen prior to replication in the Brain o These Prion Diseases typically have a very long incubation period prior to symptomatic presentation of the disease Neurotoxicity of Prion Disease may be due to small aggregates of the Prion Protein (rather than the large Fibrils) from the Prion interrupting the intracellular processing of the proteins o Prion Infection is believed to interrupt intracellular processing of proteins by switching off translation by activating an Unfolded Protein Response (UPR) Microscopic changes in Prion Disease / Prion infected tissue include: o Spongiform degeneration (i.e. ‘full of holes’) o Formation of Plaques containing misfolded Prion Proteins (these cause neuronal death!) Symptoms of Sporadic Creutzfeldt-Jakob disease (sCJD) include: o Rapidly progressive dementia o Two or more of: Myoclonus Cortical Blindness Pyramidal signs Cerebellar signs Extrapyramidal signs Akinetic mutism o Signs of sCJD include: ‘Cortical Ribboning’ (i.e. increase signalling in the peripheral cortex) on DWI MRI Periodic Sharp Wave Complexes on EEG Lesion in the Deep Nuclei in the Caudate and Putamen on T2 FLAIR MRI o Note: sCJD is an extremely aggressive disease and may result in death within a few months (and even as rapidly as ~4 weeks!) sCJD in younger individuals has a different, longer course compared to sCJD in older individuals o Furthermore, the presenting clinical signs will be different (i.e. more likely to have visual and affective disorders at onset) Variant CJD (vCJD) is different from Sporadic CJD (sCJD), and occurs following exposure to Bovine Spongiform Encephalitis (BSE) (i.e. ‘Mad Cow’s Disease’) o vCJD proteins were found throughout the body and not only in the CNS (which is where sCJD is only found) o As a result, a tonsil biopsy could be used ante-mortem to identify the presence of vCJD (as the vCJD proteins will migrate to the tonsils) o Note: T2 FLAIR MRI are also likelier to show a lesion in the Pulvinar Nuclei of the Thalamus (rather than the Deep Nuclei in the Caudate and Putamen as per sCJD) Proposed treatments of Prion Diseases have not been particularly effective (though some drugs that have been shown to have some effect on cell lines that permit transformation of Prion Proteins [e.g. Dapsone, Amphotericin B, Iodorubicin, Porphyrins, Chlorpromazine, etc.]) o The only treatment that has had some effectiveness involves inserting tubes into the patient’s brain and administering Pentosan Sulphate (which is a drug that stops the accumulation of Aminoglycans) This treatment has prolonged the lives of some patients (up to 5 years), but will NOT cure the disease o Promisingly, Monoclonal Antibodies (Mab) were found to inhibit prion replication in presymptomatic infected mice 69 However, these Monoclonal Antibodies did not have any impact if only administered once the mice commenced presenting signs (which would the equivalent timing of treatment in humans) PATHOGENESIS OF ALZH EIMER’S DISEASE Define dementia and understand its increasing prevalence in Australia - Dementia is a symptom (i.e. progressive loss of cognitive function) rather than being a diagnosis itself o There are a range of conditions that can result in Dementia (e.g. Alzheimer’s Disease, Vascular Dementia, Dementia with Lewy Bodies, etc.) Prevalence of Dementia increases exponentially with age o Trend towards ageing population will see a growing number of people with Dementia (i.e. higher prevalence) o Progressive nature of disease (i.e. long time to morbidity) and lack of effective treatments will also result in increasing number of people with Dementia (as they do not die quickly or get cured) Diagnosis of Alzheimer’s Disease is commonly made by frontline medical staff (i.e. General Practitioners) based on cognitive testing (e.g. MSE, MMSE) o Diagnosis can only be confirmed post-mortem via neuropathology (although there can be ambiguity in the histopathological diagnosis) - - List the gross and microscopic features of the Alzheimer’s disease (AD) brain - Gross features of Alzheimer’s Disease includes: o Significant atrophy to the brain (resulting in expansion in the size of the Sulci and decrease in the size of the Gyri) Most severe atrophy will occur in the Parietal and Temporal Lobes o Atrophy / damage to the Medial Temporal Lobe (including Hippocampus) this is one of the most severely affected areas in Alzheimer’s Disease Microscopic features of Alzheimer’s Disease include: o Deposition of Neuritic Plaques (also known as Senile Plaques or A-Beta Plaques) These extracellular plaques involve a central core of mainly Amyloid (A-Beta Plaques) that is surrounded by distorted Neuritic Processes These are found throughout the Cortex, except in the Primary Cortices (e.g. Primary Motor Cortex, Primary Visual Cortex, etc.) Note: A-Beta Plaques are believed to initially be diffuse, but then will attract and stick to additional amyloid, resulting in the formation of Neuritic Plaques possessing a solid amyloid core These Plaques may then progress to lose their Neuritic Processes leaving behind the Amyloid Core only o Deposition of Neurofibrilliary Tangles These intraneuronal structures are particularly found in the Medial Temporal Lobe and Hippocampus Major component of these structures is hyperphosphorylated Tau Note: Accumulation of Tau is significantly more prominent in the Hippocampus compared to the Amyloid Plaques Astrocytosis and Microgliosis may occur surrounding the Amyloid Plaques and Neurofibrilliary Tangles o Presence of Microglia suggest there may be some inflammation involved in the brain Note: Tau provides stability to Microtubules (which are the intraneuronal organelles that transport substances) o However, hyperphosphorylation of the Tau will result in this Tau protein no longer attaching to Microtubules but rather sticking to itself (leading to the formation of Neurofibrilliary Tangles) o This intraneuronal development of Neurofibrilliary Tangles will eventually result in the death of the neuron - - 70 - This will lead to the neuron becoming a ‘Ghost Neurofibrilliary Tangle’ (which cannot be removed from the brain) Note: Amyloid Cascade Hypothesis suggests that AD commences with formation of Neuritic Plaques, which subsequently induce formation of Neurofibrilliary Tangles and hence neuronal death o This hypothesis is challenged by other hypotheses which suggest Tau, Oxidative Stress, Inflammation, etc. are the key determinant / precipitating factor in AD Know how AD pathology relates to clinical symptoms - Atrophy / damage to the Hippocampus and Medial Temporal Lobe results in the memory loss characteristic of Alzheimer’s Disease o Tau Neurofibrilliary Tangles will initially target the Hippocampus and Entorhinal Cortex, which may explain why memory loss is the initial presenting symptom for Alzheimer’s Disease The location / spread of the Amyloid Plaques and Neurofibrilliary Tangles throughout the brain can provide an understanding of the staging / progression / severity of the disease (e.g. significant progression when plaques located in high levels in the Posterior Cingulated Gyrus and / or Tangles in high levels throughout the Neocortex) o Spread of Tau Neurofibrilliary Tangles (rather than the spread of Amyloid Plaques) is much closely aligned / correlated with the spread of Alzheimer’s Disease Indeed, the region specific spread of Neurofibrilliary Tangles can be used for diagnosis of Alzheimer’s Disease o However, it should noted that the development of Amyloid Plaques and Neurofibrilliary Tangles is common with age, and by themselves do NOT cause Alzheimer’s Disease - Explain the difference between monogenic and sporadic forms of AD - Monogenic AD refers to AD resulting from a mutation in a single gene, whilst Sporadic AD refers to AD with no familial or geographic clustering o <10% of AD is Familial, and <1% of AD has an identified mutation Monogenic forms of AD typically have an earlier age of onset (~30-50) and clinical features focusing more on verbal IQ / naming and perception o In contrast, sporadic forms of AD typically have a later age of onset (~70’s) and clinical features focusing more on memory loss and reduction in mental speed Monogenic forms of AD may result from mutations in the following particular genes involved in the deposition of Neuritic Plaques: o Amyloid Precusor Protein (Chromosome 21) (which is the precursor to Neuritic Plaques) o Presenilin-1 (Chromosome 14) or Presenilin-2 (Chromosome 1) (which are involved in the conversion of Amyloid Precusor Protein into an Amyloid structure) o Note: Mutations in the Tau gene have NOT been associated with Familial Alzheimer’s Disease Sporadic form of AD will involve the affected patients having a genetic susceptibility to the disease that is triggered over time by environmental factors o This form of the disease in NOT monogenic, but nonetheless is believed to be more likely in the presence of certain genes - - - Be familiar with known risk factors for sporadic AD - Known risk factors for Sporadic AD include: o Age o Dementia in first degree relative o E4 Allele of ApoE gene (which may reduce the age of onset of AD) Two copies of the E4 allele increases the risk of AD by 12x Single copy of the E4 allele increases the risk of AD by 2.5-3x Note: The presence of two copies of the E4 allele does NOT necessarily predict the person will ultimately contract AD o Female 71 - - Probable associations for Sporadic AD include: o Diabetes o Smoking o Head injury Note: Higher education is believed to be a protective factor against AD Explain the basis for the current use of acetylcholinesterase inhibitors in AD - Nucleus Basalis of Meynert is the location of Cholinergic Neurons in the Brain, and will project to the Hippocampus and assist with memory formation o The occurrence of Neurofibrilliary Tangles in the Nucleus Basalis of Meynert will result in the death of Cholinergic Neurons o As a result, treatment with Acetylcholinesterase Inhibitors (i.e. to increase the amount of Acetylcholine) has been considered, and has proven to have some success COGNITIVE FUNCTION A ND DEMENTIA Describe major management principles of a patient with Alzheimer disease, including the management of the cognitive, mood and behavioural aspects of Alzheimer disease and emerging therapies - There are no curative treatments available for Alzheimer’s Disease or other forms of Dementia, so management will focus on symptom control / relief and supportive care o Cholinesterase inhibitors are associated with modest benefit in cognitive measures and ADLs, but can had side-effects of GIT issues and dizziness o NMDA Antagonists have been approved by the FDA for treatment of moderate to severe AD, and has been associated with improved cognition This can be used safely in conjunction with Cholinesterase Inhibitors o Anti-depressants or Anxiolytics can be used to treat depression / anxiety associated with Dementia o Behaviour modification may be achieved via psychotherapy and / or drugs (e.g. AntiPsychotics, Mood Stabilisers) o General supportive care is another important element that should be provided throughout the disease course (especially given significant transition of lifestyle / quality of life) o Note: Promotion of mental activity may slow the progression of AD o Note: Genetic counselling / screening may be offered in AD (especially if younger onset and / or family history of AD) given the possible monogenic forms of AD Emerging / experimental therapies for Alzheimer’s Disease are numerous and include: o Monoclonal Antibodies that target Amyloid o Vaccination with Amyloid species o Beta-secretase Inhibitors (to inhibit Amyloid formation) - Describe major causes of Dementia and their features - There are several different causes of Dementia (e.g. Alzheimer’s Disease, Vascular Dementia, Dementia with Lewy Bodies, etc.) o Dual pathology is highly common (e.g. ~50% of patients diagnosed clinically with AD will also have another type of dementia revealed based on the post-mortem pathology) Whilst there is an increased risk of Dementia with increased age, a significant proportion of the elderly are NOT demented o Hence, Dementia is NOT to simply be expected as a normal part of ageing Deposition of Amyloid occurs diffusely throughout the whole brain and may commence ~30 years prior to the clinical presentation with Alzheimer’s Disease o It is strongly suspected that Amyloid deposition will occur initially and affect Neurons, which will then trigger the formation of Tau Neurofibrilliary Tangles within the Neuron o These Tau Neurofibrilliary Tangles will disrupt the downstream connection of the affected Neurons - - 72 - - - - - - - o Ultimately, there may be a diffuse synaptic loss throughout the brain Whilst imaging cannot confirm Alzheimer’s Disease, the presence of atrophy in the Medial Temporal Lobe may support such a diagnosis o However, patients will this level of atrophy will be clinically very demented, and so the clinical diagnosis should have been made much earlier o Alternatively, high contrast and serial imaging can highlight the gradual atrophy of the Medial Temporal Lobe over time, which can assist with diagnosis o Alternatively, PET Imaging may be able to identify hypometabolised areas of the brain, which can then be compared to known areas of damage in Alzheimer’s Disease to assess whether this diagnosis is likely Pittsburgh B Compound can be used (in conjunction with PET Scan) to identify the presence of Amyloid Plaques (which can be a pre-clinical sign of future AD!) and its progression However, the limitation of these Amyloid detection technique is that several different pathologies may result in Amyloid deposition, and hence this is not a specific investigation o Note: These ‘high-tech’ diagnostic techniques are not being used clinically, but have rather been used in research settings Initial presentation of Alzheimer’s Disease involves the impairment of Anterograde Memory o As Alzheimer’s Disease progresses, there will be impairment of broader executive function / attention In contrast, other forms of Dementia may involve the impairment of broader executive function / attention prior to memory (e.g. Dementia with Lewy Bodies) o There will further deficits in language, apraxia, perceptual abilities, etc. as Alzheimer’s Disease progresses further Depression and Anxiety are common side-effects / consequences of Alzheimer’s Disease o Other neuropsychiatric behaviours such as agitation, disruption and sleep disturbances may occur later Management of Alzheimer’s Disease will involve: o Multidisciplinary Team o Genetic screening / counselling (especially if young onset or presence of family history of AD) o Behaviour modification (e.g. psychological therapy, drugs, etc.) o Medications (e.g. Cholinesterase inhibitors) o Information o Supportive care Vascular Dementia is another form of dementia that can coexist with AD and will also increase in probability with age o There is a significantly worse mortality prognosis for Vascular Dementia patients (compared to Alzheimer’s Disease) o This may be due to the increased risk of cardiovascular and cerebrovascular disease in these patients Vascular Dementia can be difficult to distinguish clinically from AD, but does generally have a subcortical cognitive profile (i.e. slower processing speeds) rather than having difficulty with memory Management of Vascular Dementia will involve: o Secondary prevention (e.g. manage hypertension, diabetes, smoking, lipids, etc.) o Behaviour modification (e.g. psychological, drugs, etc.) o Supportive care o Note: There are no disease modifying therapies for Vascular Dementia, although Cholinesterase Inhibitors can be effective given the high prevalence of dual pathology with Alzheimer’s Disease However, the adverse cardiovascular side-effects of Cholinesterase Inhibitors may result in more problems through their use o Note: Other causes of dementia need to be excluded too! Dementia with Lewy Bodies (DLB) is a later-onset dementia (i.e. 2nd most common late onset dementia) that will involve presence of Parkinsonism in addition to Dementia 73 o - - - - DLB be differentiated from Parkinson’s Disease as the rigidity and akinesia are symmetrical (rather than being asymmetric as in Parkinson’s Disease) o Patients with DLB will commonly have early visual hallucinations, fluctuating cognition and REM Sleep Behaviour Disorders (i.e. ‘Acting Out’ dreams) o Eventually patients with Dementia with Lewy Bodies will degenerate across all domains (similar to Alzheimer’s Disease) so the early signs / symptoms are critical in diagnosing the condition o Note: Dementia with Lewy Bodies is similar to Parkinson’s Disease in that they are both Alpha-synucleinopathies Management of DLB involves use of: o Cholinesterase Inhibitors (limited data for use, but associated with slower neuropsychiatric decline) o Atypical Anti-Psychotics Atypical Anti-Psychotics can improve behavioural symptoms, but there is a risk they will worsen the Parkinsonian signs / symptoms o Supportive care Parkinson’s Disease Dementia (PDD) are likely to have problems at onset with executive function (rather than memory) o There are limited management options available, although the Cholinergic drug Rivastigmine has behaviour benefits for ~15-20% of patients, and other non-pharmacological such as cognitive / memory training, counselling and optimising of home environment can be helpful o Supportive care is another critical element of management Frontotemporal Dementia (FTD) has there variants based on the site of pathology (i.e. Behavioural, Semantic and Progressive Non-Fluent Aphasia) o Behavioural variant will commonly involve deterioration in the Orbitomedial Frontal Cortex (which is the area of the brain involving inhibition / impulse control) This has a slow, progressive onset and will result in changes in behaviour / personality (e.g. disinhibition, apathy, loss of empathy / warmth, etc.), of which the person has no insight Memory and language function will generally remain good in these patients o Semantic Dementia is more likely when the pathology is in the Left Hemisphere of Temporal Lobe This involves loss of vocabulary / memory for language, but good day-to-day memory o Progressive Non-Fluent Aphasia is more likely when the pathology is in the Dorsolateral Frontal Cortex (i.e. Broca’s Region) This involves loss of fluent conversational ability (e.g. laboured, stuttered), but retention of vocabulary Management / treatment options for FTD are generally limited, so management consists mainly of supportive care History is critical for the correct diagnosis of patients with Dementia! o In particular, it is CRITICAL to understand the history at the time of onset (as this is when the differences between the different Dementia syndromes are more apparent) EMERGING THERAPIES F OR DEMENTIA Describe the potential for therapeutics for prevention and treatment of dementia - It has been proposed that dementia can be prevented via: o Treating vascular risk factors (e.g. hypertension, dyslipidaemia, etc.) o Physical activity / exercise o Appropriate nutrition / diet o Cognitive training / social activity o Note: Evidence for the above is limited, but there are currently studies underway to assess their effectiveness 74 - - Management/ treatment of Dementia will involve identifying the particular deficits / symptoms and offering therapeutics to treat these o No curative treatment is currently available for Dementia, but the symptoms / signs may potentially be treated (whether pharmacologically or non-pharmacologically) and quality of life improved o Note: Supportive care and education should also be provided to patients with Dementia Management/ treatment for Dementia should remember to assess for the presence of other conditions that cause cognitive decline that are treatable (e.g. deficiency of Vitamin B12 and / or Folate, Hypothyroidism and both high or low levels of Na+, Ca2+ or Glucose) o These reversible causes of cognitive decline should be assessed in patients with Dementia as correcting these offers a simple way to improve cognitive function o Furthermore, it is critical to optimise the vision and hearing of patients with Dementia (as loss of these sensory modalities will exacerbate any cognitive decline present) o Note: It is also important to distinguish Dementia from Delirium and Depression, both of which are readily treatable Describe current therapies and their place in management of dementia - Management of dementia should be multi-disciplinary and involve three groups (i.e. patient, family / carers and medical / support services) o At all times, it is important to consider the psychiatric / behavioural changes, co-morbidities and the needs of the carer Current therapies available for Dementia include: o Education and support for carers / families Examples include home care packages (Community Aged Care Packages, Dementia Support Services, etc.), Carer Respite Centres, Support Groups (e.g. Alzheimer’s Association) There is evidence that patients whose families received education and support are able to remain at home longer (rather than being admitted to a residential facility) o Drugs / Medications Cholinesterase Inhibitors or Cholinergic Agents (e.g. Donepezil, Rivastigmine) for mild-to-moderate Dementia Cholinesterase Inhibitors can cause heart block and / or syncope, so their use should be closely monitored / carefully considered in patients with Cardiovascular problems / risk factors NMDA Receptor Antagonists (e.g. Memantine) for moderate-to-severe Dementia Adverse side-effects include agitation, diarrhoea, hallucinations, insomnia, fatigue, etc. Note: These have only been studied in combination with Cholinesterase Inhibitors, and have no benefit if provided instead of Cholinesterase Inhibitors Gingko Biloba This is being used by many patients suffering Dementia despite the lack of evidence for its effectiveness as well as the adverse side-effect of bleeding o Treatment of Behavioural and Psychological Symptoms of Dementia (e.g. hallucinations, agitation, apathy, insomnia, etc.), such as: Establishing calming and safe environment (e.g. home modification, personal alarm, routines, orientation tools, etc.) Identifying and treating other precipitants (e.g. medications, visual / hearing impairments, etc.) Anti-Psychotics or Mood Stabilisers (e.g. Anti-Epileptics such as Sodium Valproate) Pharmacological management will be mainly for acute periods of severe agitation, aggression and / or distressing / dangerous hallucinations (as long-term usage carries significant risk such as higher mortality!) Do NOT use drugs for treatment of wandering, repetitive behaviour, disruptive vocalisation or resistive behaviour! - 75 - - o Treatment of Depression (both non-pharmacological and pharmacological) Both Cholinesterase Inhibitors and NMDA Receptor Antagonists provide a small improvement in cognitive function, but do NOT modify the disease course o Evidence suggests the small improvement in cognitive function delivered by Cholinesterase Inhibitors and NMDA Receptor Antagonists may be statistically significant, but is NOT clinically significant For example, another study showed dementia patients treated with Cholinesterase Inhibitors had no difference in the time to institutionalisation as placebo o Given the adverse side-effects of Cholinesterase Inhibitors and NMDA Receptor Antagonists, it is questionable whether this treatment should be provided Any improvement appears to be driven by Placebo effect, and hence this may be an expensive and ineffective form of treatment o Note: There is even less evidence for use of Cholinesterase Inhibitors in other types of Dementia Management of mild-to-moderate Dementia will mainly involve some supportive care, but patients are generally able to live in their home and complete IADLs o In contrast, severe Dementia will require formal support / residential care with a focus on providing basic palliative care Describe potential new therapies and how they can be evaluated - There is a considerable pathway / pipeline for Alzheimer’s Disease medications as this is a highly attractive market for drug companies o This focus on Alzheimer’s Disease offers hope that effective treatments may be developed in the future for Alzheimer’s Disease New treatment / therapies aim to modify the disease course by focusing on the abnormal proteins deposited in the brain in Dementia; these include o Anti-Beta-Amyloid Therapies; this can involve: Reduced production of Amyloid (i.e. decrease Beta- and / or Gamma-Secretase, increase Alpha-Secretase) Reduced aggregation (i.e. Chelators) Removal of Amyloid (e.g. IVIG, Monoclonal Antibodies, Vaccination against Amyloid) o Anti- Tau Therapies Reduced aggregation (via inhibitors) Reduced phosphorylation of Tau via Tau Phosphorylation Kinase Inhibitors [e.g. GSK3 inhibitors]) Other non-proteinopathy therapies proposed include: o Anti-oxidants o Anti-inflammatories o Inhibitors of excitotoxicity o Enhancement of Mitochondrial Function (which can increase neuroprotection) o Neurotrophins (i.e. Nerve Growth Factors) Mouse study found injecting young mouse plasma into old mouse would improve cognition of the older mouse o Similar treatment in humans that slow-down ageing process may offer a pathway for treatment / minimisation of Dementia Many of the above proposed therapies have resulted in negative trials, though continued research is being conducted o Indeed, it is proposed these therapies need to be provided in the pre-clinical / prodromal phase of AD to be effective o These pre-clinical studies plan to be evaluated using clinical and biomarker measures of response (e.g. PET Amyloid Imaging, MRI Volumetrics, etc.) New therapies are being evaluated by their effect of improving cognitive impairment and function o There are suggestions that future drugs should be evaluated based on cognitive improvement alone, with post approval studies of effects on function - - - - - 76 MENTAL ILLNESS ANATOMY OF EMOTIONAL SYSTEMS Identify and locate the components of the limbic system and describe their connections and function - ‘Emotion’ refers to a body state, whilst ‘Feeling’ refers to a conscious perception / narrative Components of the Limbic System include: o Hypothalamus – this regulates homeostasis and controls autonomic and visceral responses o Thalamus – this directs sensory and limbic relay, as well as attention and memory o Amygdala – this receives visual, olfactory, visceral and sensory input, is important for fear / loathing, directing emotional behaviour and influencing memory (especially of fearful stimuli) o Cortex Temporal (i.e. Hippocampus, Parahippocampus) – these areas are critical for memory Anterior Cingulate Cortex – this is important for the experiencing of emotion (i.e. ‘feelings’) and understanding emotion in others Components of the Extended Limbic System include: o Insular Cortex o Orbitofrontal Cortex o Ventromedial Prefrontal Cortex o Brainstem Reticular Formation and Basal Forebrain Ascending Reticular Activating System (which communicate via neurotransmitters throughout the Cortex to set the overall mood / global attention) Amygdala projects to the Limbic Cortex, Hypothalamus, Basal Ganglia, BRF and organisation areas for Lower Motor Neurons and is critical for directing emotional behaviour (including autonomic, cognitive and skeletalmotor behaviours) o Amygdala receives inputs from the Thalamus, Hypothalamus, Hippocampus, PAG and Cortex (hence receiving a wide range of sensory inputs) o There are three major nuclei of the Amygdala Basolateral Nucleus – this receives significant incoming sensory input and will magnify this input Corticomedial Nucleus – this is interconnected with the Olfactory Centres Central Nucleus – this controls bodily reactions and is interconnected with the Hypothalamus and Periaqueductal Grey (PAG) o Amygdala is important in pairing sensory stimulus with emotional output Lesion of Amygdala will result in the failure of this link to exist, such that the emotional / fear / autonomic response to the relevant sensory stimuli does not occur o Amygdala assists with interpretation of emotion in other people, so lesion of Amygdala will result in reduced reaction to aggression / anger in others o Amygdala receives inputs for the Hippocampus amongst other areas, this results in the link between fear / emotion and memory o Note: As the Amygdala connects to a variety of structures (e.g. BRF, Lateral Hypothalamus, Medulla, etc.), fear / emotion (which is recognised by the Amygdala) can have widespread impacts throughout the body Hypothalamus is anterior to Mammillary Bodies and is adjacent to the Third Ventricle o Hypothalamus will impact the visceral / autonomic and somatic / skeletalmotor response based on sensory inputs from various other structures in the body (e.g. Brainstem Reticular Formation, Amygdala, Olfactory, Hippocampus, etc.) Anterior Cingulate Cortex (ACC) has extensive connections with Amygdala, PAG, Autonomic regions of Brainstem and Anterior Thalamus o ACC appears to be important in understanding emotion in others and will be activated in emotionally charged tasks - - - - 77 o - - - - - - - Ventral aspect of ACC is involved with affective / visceral autonomic reactions, which Dorsal aspect of ACC is involved with cognitive reactions o ACC is involved in error correction and the visceral ‘funny feeling’ response to an error o Lesion to ACC can result in feeling on emotional ‘flatness’ (e.g. reduced autonomic response to emotive stimuli, muteness, reduced pain appreciation, reduced self-awareness, etc.) o There is changed levels of activity in the ACC during depression and romantic love (i.e. both strong emotions) Insular Cortex received inputs from the viscera, taste and pain centres o Insular Cortex projects to the Amygdala, and hence may play an important role between linking Visceral states with emotions o Insular Cortex will particularly be activated when people have a feeling of disgust, but also when feeling romantic love Orbitofrontal Cortex is the last area of the brain to develop and is important in regulating one’s own emotional displays, regulating how to respond to other’s emotions and selecting behaviours to comply to the situational social norm o This area of the brain undergoes significant expansion during the teenage years and up until the early 20’s, which may explain why teenagers commonly engage in socially inappropriate behaviours and / or may be insensitive to others Ventromedial Prefrontal Cortex has higher activation during happiness and lower activation during depression o This area also appears to be an impulse inhibitor, with increased activation when attempting to control emotions (same as the Orbitofrontal Cortex) Both voluntary and emotional systems are connected to the lower motor neurons o These are two different upper motor neuron pathways to supply the lower motor neurons o Hence, damage to one upper motor neuron system will not necessarily damage the other pathway There has been no specific anatomic location identified associated / unique to a particular emotion (e.g. love, reward, depression) o Instead, a combination of areas are involved in each of these emotions Head injuries / trauma will commonly damage areas of the Limbic System (due to the location of these areas of the brain being directly adjacent to Frontal and Occipital Bones) o These injuries / trauma can result in loss of memory and decreased inhibition (resulting in socially inappropriate behaviours) Frontotemporal Dementia may present at onset with inappropriate behaviour, loss of inhibition, etc. as these areas of the Cortex suppress these inappropriate behaviours Understand the interaction of the visceral (emotional) motor system with cognitive areas - There is evidence that cognitive perception of a stimulus and emotion expression in response to a stimulus are interrelated and will influence each other Emotion is displayed via stereotypical behaviour (e.g. facial expression, tachycardia, startle, run away) o This stereotypical behaviour will prepare the person for the required response as well as communicating emotion to others - INTRODUCTION TO MAJOR MENTAL ILLNESS TBD – not provided for 2015 - Psychiatric Disorders are illnesses or disease states, manifest by abnormalities of thinking, feeling and behaving, that cause the individual significant distress or significantly impair their ability to work, play and love o The key feature of a Psychiatric Disorder is that it will cause significant distress or significantly impair their ability to work, play and love o Whilst some anxiety / feelings of stress is normal and indeed may be needed to focus and maximise performance, excessive anxiety / stress will inhibit performance levels 78 - - - - - - - - - Mental illness is extremely common (~25% of the population) and will be seen in lots of patients regardless of the practice setting (e.g. GP, Hospital, etc.) o Mental illness will frequently persist throughout life and cause high levels of disability and distress (as well as costs to the health system and society as a whole) o There is significant stigma present regarding mental illness that includes fear, shame and pessimism regarding those affected Psychiatric Disorders can be classified according to: o ‘Categorical Approach’ – this will classify the core symptoms of each disorder; or o ‘Dimensional Approach’ – this focuses on a particular area / feature (that can be common to several disorders) Different categories of Psychiatric Disorders include: o Organic Disorders (e.g. Delirium, Dementia, etc.) o Psychotic Disorders (e.g. Schizophrenia, Delusional Disorders) o Mood Disorders (e.g. Depression, Dysthymia, Bipolar Disorder) o Anxiety Disorders (e.g. GAD, OCD, PTSD, Panic Disorder, Phobia) o Personality Disorders o Somatoform Disorders (e.g. Conversion Disorder) o Substance Disorders (e.g. Abuse, Dependence) o Other Disorders (e.g. Sleep Disorder, Munchausen’s Syndrome) o Intense Reactions (e.g. Complicated Bereavement) o Patient Role (i.e. ‘sick’ role) Diagnosis of Psychiatric Disorders can involve difficult clinical judgments, as interpretation of psychological symptoms will be influenced by cultural, social and personal beliefs of the psychiatrist / psychologist as well as society in general o This requires clinicians to make judgments about what is culturally ‘acceptable’ / ‘normal’ and hence introduces a level of subjectivity to diagnosis! o As a result, it is important for clinicians to speak with transcultural personnel who can explain different cultural beliefs (and hence whether the patient is acting consistent or inconsistent with the particular culture’s beliefs) ‘Delusion’ are fixed beliefs that are not amenable to change in light of conflicting evidence and will involve an incorrect interpretation / perception of an actual stimulus present (e.g. misinterpret shadow as a snake) o In contrast, ‘Hallucination’ involves an perception / interpretation that occurs without an actual stimulus (e.g. hearing voices) Symptoms and signs of Mental Illness will include: o Behaviour o Emotion / Mood o Relationships o Thinking (content and form) o Perception o Cognition o Insight and Judgment Mental illnesses / disorder with arise from a combination of genetic predisposition and environmental factors (may be multiple different environmental factors) o There is no single gene resulting in mental illness, although there is a genetic predisposition amongst some individuals It is CRITICAL to examine Psychiatric patients for other co-morbidities (especially other medical conditions) o Mental illness patients have a significantly higher death rate from a range of other medical conditions compared to the broader population o Psychiatric patients are commonly overlooked for these other conditions due to their highlyvisible Psychiatric signs (which are commonly present too) o Furthermore, medications for Psychiatric conditions often have side-effects that increase the likelihood of other medical conditions Treatment options for Mental Illness include: o Biological (i.e. Pharmacological, Electroconvulsive Therapy [ECT]) 79 o o ECT is a very effective treatment for very severe melancholic depression Psychological (e.g. CBT, Dynamic Therapy, Counselling) ‘Cognitive Psychological Therapy’ is very effective for mild-to-moderate depression (i.e. as effective as anti-depressants) ‘Dynamic Psychological Therapy’ involves a psychologist psycho-analysing the patient to understand the nature of their problems Social GENE, BRAIN AND BEHAVIOURAL BASIS FOR PS YCHIATRIC ILLNESS Describe the interplay of molecular, genetic, developmental and environmental factors in the development of mental disease - Genetics are an important driver of behaviour (e.g. inheritance of anxiety, addiction, sleep cycles, spirituality, assortative mating, etc.) o Genetics create a predisposition towards certain behaviour o Genetics though may only express themselves at different specific ages and / or following different specific environmental exposures As a result, the rate of expression of particular genes in a society will depend on the particular environmental exposures available in that society (e.g. alcohol addiction cannot occur in a society without alcohol) o Genetics will influence not only onset of a disease, but also the course / natural history of the disease and response to treatment of the disease Environmental influences / differences will become increasingly important as people age o As a result, genetic differences may not be evident at younger ages (due to extremely similar environments at younger ages) o Examples of environmental exposures include toxins (e.g. lead), excessive stress, education, abuse, etc. Brain development / size will change over time (e.g. synaptic proliferation in childhood, synaptic pruning in adolescence, maintenance of synapses in adulthood) o As a result, there may be different genetic influences at different ages (in addition to different environmental exposures at different ages), which will give rise to different phenotypes at different ages o For example, Adolescence is the key time period for the onset of major mental disorders o Genes will have different ages of onset (rather than only having an onset in adolescence) As a result of people living longer, this will result in the emergence of new phenotypes Note: There are also different environment exposures / influences as people age, which will also increase the likelihood of expression of different genes There is a complex interplay between genes and environments in the onset of mental disorders rather than being due to one or the other o Gene-Environment approach suggests that genetics will modulate the impact on environmental influences and determine whom will develop a mental disorder after exposure to the same environmental influence There are two main influences driving genetics in mental disorders: o Single Nucleotide Polymorphisms (SNPs) – these are common variations that each impart an extremely small increase in risk, but cumulatively may together result in the incidence of mental disorders The identification of individual SNPs resulting in mental disorders may be difficult to replicate in further studies given the wide range and small role of SNPs in mental disorders (and hence the impact of each SNP is dependent on the unique context) ~30-50% of heritability for most genetic disorders (e.g. anxiety, depression, substance abuse, etc.) will arise from the genetic variation from common SNPs Note: This increase in risk of mental disorders will be dependent on the presence of a large number of these small variations o Copy Number Variations (CNVs) – these are rare mutations that each impart a significant risk of mental disorders - - - - 80 - - - The older the age of the parent, the greater the number of CNVs transmitted to the child Expression of these CNVs though will be strongly influenced by environmental patterns around parenting There is strong evidence that the different mental disorders (e.g. schizophrenia, bi-polar disorder, depression, etc.) have common genetic variations There are numerous genes that have been identified as being associated with Schizophrenia (particularly immune-system and Glutaminergic neurotransmission related genes) o The relative risk level of developing Schizophrenia can be calculated as a Risk Score Profile depending on the number and type of Schizophrenia-related genes present in your genome The genes increasing the risk of mental disorders (e.g. Bipolar Disorder, Schizophrenia and Depression) are believed to have effect via one or more of the following pathways: o Neuronal Pathway – this relates to how neurons communicate, grow and function (i.e. genes of brain development and synaptic connection) o Immune Pathway – this is extremely sensitive to the environment, and so will be heavily influenced by environmental influences o Histone Pathway – this relates to the impact of Epigenetics (affecting either parents and transmitted to child, or affecting the child directly) Depression is associated with structural brain changes (e.g. frontal and subcortical atrophy) Circadian Rhythms / sleep cycles play a key role in the development of a range of affective disorders (e.g. Depression, Bipolar Disorder) Challenge with DSM classifications of mental disorders is the significant heterogeneity / variability within mental disorders o The wide variability within each mental disorder makes the classification of each mental disorder to have low reliability (which makes it extremely difficult to study the genetics of the mental disorder, as it is not clear what should be studied) o Alternative approach being considered is to study particular dimensions of each mental disorder (e.g. sleep-wake cycle, social avoidance, anxiety) that can be common across many disorders, rather than unreliable classifications of particular disorders NEUROTRANSMITTER DISTURBANCES IN DEPRESSION Describe key neurotransmitters and neural circuitry regulating mood - Depression as an emotional state is a part of the normal spectrum of moods within humans, but Depression as a clinical disease will occur when this emotion state is prolonged o Diagnosis of Depression as a Clinical Disease requires it to involve depressed mood, anhedonia + 3 other symptoms for >2 weeks in duration, such that it affects social / occupational functioning Depression symptoms are classified into: o Emotional (e.g. depressed mood, anhedonia) o Cognitive (e.g. feelings of worthlessness, recurrent thoughts of death, inability to concentrate etc.) o Vegetative (e.g. weight change, change in appetite, change in sleep patterns, psychomotor changes) o Note: Different areas of the brain are associated with the different types of depression symptoms Key neural circuitry will affect mood; this includes: o Amygdala and Nucleus Accumbens involved in Emotions o Frontal Cortex and Hippocampus involved in Cognition o Hypothalamus involved in Vegetative symptoms o Note: There are connections between these areas via Dopaminergic, Glutaminergic and GABAergic pathways Hypothalamic-Pituitary-Adrenal (HPA) Axis is an neuroendocrine system that is hyperactive in patients with depression, with increased Corticotrophin-Releasing Factor (CRF) and thus ACTH and Glucocorticoids, but conversely decreased negative feedback - - - 81 o - - - - Hypothalamus is induced to release more CRH by inputs from the Amygdala, Hippocampus and Monoamine Brainstem Nuclei o HPA Axis is an essential component of an individual’s ability to cope with stress Major neurotransmitters involved in Depression include: o Noradrenaline o Serotonin (5-HT) o Dopamine o GABA Noradrenaline and Serotonin are released not only at the synapse but also along their varicosities into the surrounding extracellular space too o These two types of neurotransmitters are different in that they are tonically released due to spontaneous firing in addition to being released in rapid bursts following specific stimuli Most cell bodies for Noradrenaline are located in the Locus Coeruleus (LC) whilst most cell bodies for Serotonin are located in the Raphe Nuclei o These cell bodies project to the Limbic, Cortical and Hypothalamic regions, which emphasise the importance of these structures in the regulation of mood Reuptake transporters (e.g. NAT [for Noradrenaline], SERT [for Serotonin]) are the main mechanism for terminating the action of Monoamine Neurotransmitters at the synaptic cleft o Once these Monoamines are taken up into the pre-synapse, they are transported via lowaffinity transporters into the Vesicles for storage o Alternatively, MAO-A will degrade Monoamines present in the Cytoplasm of the Pre-Synapse (but NOT degrade vesicular stores of Monoamine) Understand the pathophysiology of depression relating to monoamine hypothesis - Monoamine Theory of Depression states that depression is caused by a functional deficit of monoamines at certain sites in the brain o Evidence supporting this theory included that antidepressants have their action on monoamine systems o However, there was some evidence against this theory (i.e. symptoms only diminish several weeks after augmentation of Serotonin and Noradrenaline) Revised Monoamine Theory of Depression suggested it was the monoamine receptor hyperresponsiveness (rather than monoamine deficiency) that resulted in Depression o Evidence supporting this theory included that diminishing of symptoms coincided with receptor downregulation o However, biochemical evidence regarding this theory is mixed (e.g. no change in urine or cortex of levels of Serotonin or 5-HIAA) Hence, the precise pathophysiology is unclear although it is believed abnormal monoamine levels are associated with complex cellular events and adaptive changes - - Appreciate the role of trophic factors in depression - Brain Derived Neurotrophic Factor (BDNF) is critical to the birth, survival and maturation of neurons in both development and in adults o There is a theory that excess HPA Axis activity will trigger increased levels of Glucocorticoids, which result in neuronal loss in the Hippocampus, which results in decreased BDNF and neurogenesis o Furthermore, Depression may be related to a genetic polymorphism in BDNF o Note: Antidepressants are believed to enhance BDNF signalling and hence neurogenesis MECHANISM OF DRUG ACTION IN DEPRESSION Recognise the classes of drugs used in the treatment of depression, providing examples of each 82 - - Different classes of drugs available for treatment of depression include: o Tricyclic Antidepressants (TCAs) (e.g. Amitryptyline, Clomipramine, etc.) o Monoamine Oxidase Inhibitors (MAOIs) (e.g. Phenelzine, Tranylcypromine, Moclobemide, etc.) o Selective Serotonin Uptake Inhibitors (SSRIs) (e.g. Sertraline, Fluoxetine, Citalopram, Paroxetine, etc.) o Atypical Antidepressants Tetracyclic Antidepressants (e.g. Mirtazapine, Mianserin) NRI (e.g. Reboxetine) SNRI (e.g. Venlafaxine, Duloxetine) There are several non-pharmacological treatments available too for Depression (e.g. cognitive behaviour therapy, psychological interventions) that are as effective as Antidepressant medications o Combination of Pharmacological and Non-Pharmacological therapies will lead to the best outcomes for patients Understand the pharmacological action, clinical efficacy and side/ adverse effect profiles of antidepressant drugs - Antidepressants will provide relief / improvement for the three types of depression symptoms (i.e. cognitive, emotional, vegetative) Antidepressants will improve mood over time, but do NOT cause an instant euphoria o Exception is the usage of MAO Inhibitors in non-depressed individuals, which may trigger feelings of euphoria and increased motor activity The different antidepressants available include: o Tricyclic Antidepressants (TCAs) This will block / inhibit re-uptake of Serotonin and Noradrenalin, resulting in increased Serotonin and Noradrenalin levels in the Synaptic Cleft This is used for treating major depression and anxiety disorders (e.g. OCD, phobias) This is the most effective treatment for severe depression and is the ‘gold standard’ against which to measure antidepressant effects against However, TCAs also block Muscarinic Acetylcholine, Histamine and AlphaAdrenoceptors too, resulting in side-effects in the CNS (e.g. respiratory depression, drowsiness, delirium), Cardiovascular (e.g. bradycardia, hypotension, arrhythmias) and Cholinergic areas (e.g. dry mouth, constipation, sweating, urinary retention) Note: TCAs have a narrow therapeutic window (toxicity can be reached at ~2x – 6x the therapeutic dose) and its usage / levels need to be closely monitored o Monoamine Oxidase Inhibitors (MAOIs) This will inhibit breakdown of Serotonin and Noradrenaline in the pre-synapse, thus resulting in increased leakage of monoamines in the synapse / extracellular space Note: There is no additional ‘release’ of Neurotransmitter from Vesicles upon normal activation (although total Neurotransmitter levels do increase given the leakage from the Cytoplasm) This is used for treating major depression, atypical depression, anorexia and bulimia nervosa, phobias (e.g. social phobia, panic disorder, phobic anxiety) MAO Inhibitors are the most effective antidepressant class for treatment of Atypical Depression There are two sub-types of MAOIs Irreversible and non-selective (e.g. Phenelzine, Tranylcypromine) inhibitors Reversible and selective (e.g. Moclobemide) Note: There are other MAO Inhibitors used for the treatment of other conditions (e.g. Seligiline [MAO-B Inhibitor] for treatment of Parkinson’s Disease) MAOIs have mild side-effects affecting the CNS, Cardiovascular, GIT and Cholinergic areas - - 83 - Phenelzine is only a 2nd-line Therapy for Major Depression given its adverse side-effect of liver toxicity (which should be avoided if possible by using other 1st line treatments if possible!) o Selective Serotonin Uptake Inhibitors (SSRIs) SSRIs have a similar mechanism to TCAs (i.e. block presynaptic re-uptake) except they are selective to Serotonin At therapeutic levels, SSRI are 50x more selective to binding to the Serotonin transporters (vs. Noradrenaline Transporters) in comparison to TCAs There is also significantly less binding to Muscarinic Acetylcholine, Histamine and Alpha-Adrenoceptors too As a result of this improved selectivity, there is reduced side-effects from usage of SSRI (especially cardiotoxic side-effects) This is used for treating major depression, dysthymia and anxiety disorders (e.g. OCD, panic disorder) SSRIs are now the first-line therapy for the treatment for certain (though not all) anxiety disorders SSRIs have increased Seritonergic side-effects, resulting in increased side-effects in the CNS (e.g. confusion, insomnia, drowsiness) and GIT (e.g. nausea, diarrhoea, vomiting) compared to other Anti-Depressants o Atypical Antidepressants (which encompasses multiple different classes of drugs) These are used for treating and preventing relapse of major depression and anxiety disorders (e.g. GAD, social phobias) Tetracyclic Antidepressants block Alpha-2 Adrenoceptors (i.e. autoreceptors) , which will trigger an increased release of Serotonin and Noradrenaline (as there is less negative feedback) NRIs (Noradrenaline Reuptake Inhibitors) will ONLY bind to the Noradrenaline Transporters SNRIs (Serotonin and Noradrenaline Reuptake Inhibitors) will bind to both the Serotonin and Noradrenaline Transporters SNRIs have a similar target to TCAs, but possess different chemical structures so they are more selective to these two transporters compared to TCAs Note: None of the above drugs are more effective than TCAs, though they generally have fewer side-effects and less acute toxicity General considerations for the use of Antidepressants include: o When prescribing Antidepressants, start with the lowest dose and gradually increase as needed Similarly, when deprescribing, abrupt cessation should be avoided (can lead to withdrawal) o Patients with depression will be continued on Anti-depressants for ~6 months after the depressive symptoms have ended in order to reduce the risk of Depression Relapse o Combination of drugs does NOT increase therapeutic efficacy, but does significantly increase the risk of adverse drug reactions o There is an increased risk of suicide in people taking antidepressants Increased suicide risk may be due to anti-depressants taking several weeks to be effective The failure for immediate relief may increase despair amongst depressed patients, and hence increase the risk of suicide o Note: ~30% of patients will NOT respond to Anti-depressants, so this needs to be considered when using Anti-depressants PSYCHOSIS – AN OVERVIEW List the range of disorders that may be part of the syndrome of psychosis 84 - Range of Disorders that may be part of the syndrome of Psychosis include: o Schizophrenia / Schizophreniform / Schizoaffective o Mood Disorders (e.g. Bipolar Disorder, Psychotic Depression) o Delusional Disorders o Personality Disorders o Paranoid Disorder o Organic Disorders (e.g. Delirium, Dementia, Substance-induced) Describe the symptoms and signs of psychosis - Signs and symptoms of Psychosis include: o Positive Symptoms (e.g. hallucination, delusions, lack of awareness of condition) o Negative Symptoms (e.g. affective blunting, alogia [i.e. poverty of speech], amotivation, asociality / apathy) Blunted affect in Psychosis can be exacerbated by the anti-psychotics used as treatment, as these anti-psychotics can cause rigidity of the facial muscles resulting in a blunted, Parkinsonian affect Loss of social network due to Asociality is particularly problematic as social networks can be protective in the long-term against mental illness o Excitement (e.g. aggression / hostility, disorganisation of thought and behaviour) Increased Hostility in Psychosis is exacerbated by Substance Abuse and can result in Aggression (which can lead to murder!) o Cognitive Dysfunction (e.g. attention, memory, planning, problem solving, processing speed) o Anxiety / Depression / Suicide There is significant variability in cognitive performance depending on the particular cognitive domain tested, though verbal functioning and speed of processing are particularly affected o However, there is a similar pattern in the level of decline by cognitive domain for all mental disorders o These cognitive deficits really interfere with the ability of the person to interact and involve themselves with society Hence, it is important treatment to treat this cognitive decline in order to maximise the level of inclusion of these psychosis patients with society o Note: Whilst most Psychotic illness have high levels of functional impairment, Schizophrenia has the most marked deterioration in level of functioning Anxiety can result both from the direct effects of the delusions / hallucinations involved with Psychosis (e.g. persecution delusions), but also upon recovery from the psychotic episode due to fear of the stigma attached to people with psychosis - - Discuss the different pathophysiological models of Schizophrenia - Different pathophysiological models of Schizophrenia include: o Dopamine Model of Schizophrenia Increased levels of Dopamine are associated with increased incidence / symptoms of Schizophrenia Hyperactive Dopaminergic projections to the Striatum lead to positive symptoms Hypoactive Dopaminergic projections to the PFC cause cognitive and negative symptoms o NMDA / Glutaminergic Model of Psychosis NMDA dysfunction is related to schizophrenia Patients with Anti-NMDA Brain Antibodies are treated with IVIG and other immunological therapies Discuss neurodevelopmental and gene x environment models of psychosis - Neurodevelopmental Model of Schizophrenia suggests that the presence of genes associated with Schizophrenia will result in progressive synaptic pruning over time and ultimately Schizophrenia 85 o - - - There is a significant loss of Cortical Grey Matters in patients with Schizophrenia, with the loss of Neuropil, Axons / Dendrites and smaller neurons However, it is clear that environmental exposures will impact upon the risk of developing Schizophrenia give environmental exposures will affect how genes are expressed o Conversely, the impact of environmental factors on developing Psychosis will be modulated by the presence of particular genes (i.e. Gene x Environment Models) o For example, the risk of developing Schizophrenia from Cannabis usage was modulated by the presence of particular genetic variations (i.e. higher risk if Val/Val Allele of COMT) Both genetics and environment are clearly important in the development of Psychosis o Family history is the biggest risk factor for the development of Schizophrenia o Other risk factors include maternal infection / stress (e.g. bereavement) during 2nd Trimester, obstetric complications, maternal starvation and / or childhood abuse Genes identified as being associated with Schizophrenia relate to Synaptic Plasticity and Dopaminergic Function o Immune Function genes were also associated with Schizophrenia (which is consistent with the view that the pathogenesis may be inflammatory) o Note: There are common genes involved with Schizophrenia, Bipolar Disorder and Depression Outline the biopsychosocial approach to treatment in schizophrenia - Treatment of Schizophrenia should be holistic and consider biological, psychological and social aspects o Biological treatments include pharmacotherapy and physical health (i.e. general health) o Psychological treatments include psychoeducation, CBT, cognitive remediation o Social treatments include family, vocational and financial support Anti-Psychotics are effective treatment for the Positive Symptoms, Excitement and Anxiety / Depression o However, they are ineffective with the Negative and Cognitive symptoms of Schizophrenia and hence other non-pharmacological treatments are required for these symptoms o Furthermore, there are a range of side-effects that must be considered (e.g. Akathisia, Extrapyramidal, Cholinergic, Sedation, Cardiovascular, Endocrine, Dermatological, etc.) o Note: Second-Generation Anti-Psychotics (e.g. Risperidone, Aripiprazole, Olanzapine) are preferably used for the treatment of Psychosis If these are not effective, Clozapine is a highly effective anti-psychotic that can be used (but this has particularly problematic adverse side-effects and so should be avoided if possible) Schizophrenia patients has poor physical health (e.g. CVD, Stroke, Respiratory disease, etc.), both due to higher exposure to risk factors and lack of appropriate treatment o This results in a reduction in life expectancy of ~15 years (similar to ATSI population) o Hence, it is critical to remember to treat these co-morbidities / general health of patients with Psychosis Psychoeducation and Family Therapy can assist with understanding the condition and helping a family cope / deal with the condition o Cognitive remediation and Social Skills Training are other psychological treatments that can assist in improving the cognitive skills and negative symptoms of psychosis patients, and hence increase their functioning and integration in society - - - Describe the social marginalisation of people with a psychosis - People with psychosis suffer from discrimination and marginalisation from society o They are less likely to be employed or own their own home, whilst they are more likely to be homeless or making frequent housing moves o There is also increased social isolation with patients with psychotic illnesses ANTIPSYCHOTIC DRUGS 86 Understand antipsychotic drug action and the pathophysiology of schizophrenia relating to the dopamine hypothesis - Schizophrenia is a cognitive function / thought disorder (rather than being a mood disorder) Dopamine hypothesis for Schizophrenia suggests that: o Excess levels of Dopamine increase neurological activity which leads to the symptoms of Schizophrenia Initially, Hypoactive Dopaminergic projections to the PFC cause cognitive and negative symptoms This leads to Hyperactive Dopaminergic projections to the Striatum , which lead to positive symptoms o Schizophrenia will result in increased Dopamine receptor number and sensitivity o Note: Deficiencies in another neurotransmitter system (e.g. GABA, Glutamate) which modulate the effects of Dopamine may lead to Dopaminergic overactivity There are two types of Dopamine receptors in the CNS: o D1-like receptors (i.e. D1, D5) – these are excitatory and mainly located on the post-synapse o D2-like receptors (i.e. D2, D3, D4) – these are inhibitory and located on both the pre- and post-synapse All antipsychotic drugs have antagonist effects at Dopamine D2 receptors o There is a linear correlation between therapeutic efficacy and affinity for Dopamine D2 receptors o Clinical efficacy is consistently achieved when Dopamine D2 receptor occupancy reaches ~60-80% for Typical Antipsychotics and ~40-60% for Atypical Antipsychotics o Note: There are side-effects from this mechanism of action given the importance of Dopamine in movement and Endocrine regulation Antipsychotics will change the equilibrium at the synapse that will reduce the level of cell firing in the long-term o The antagonism of D2 receptors both at the pre- and post-synapse will initially increase the rate of cell firing in the short-term o However, this will result in a compensatory increase in expression of D2 receptors both preand post-synapse in the long-term that will reduce the rate of cell firing o Hence, Antipsychotics will reduce the positive symptoms of Schizophrenia (although they have little impact on the negative and cognitive symptoms of Schizophrenia!) - - - Recognise the principle drugs used in the treatment of schizophrenia; their pharmacological action, clinical efficacy and side effect profiles - Atypical Anti-Psychotics are the first-line treatment recommended for Schizophrenia and may result in improvement of positive symptoms within ~4-6 weeks and negative symptoms within ~6-12 months o Atypical Anti-Psychotics have greater therapeutic efficacy compared to Typical AntiPsychotics, and is effective in ~30% of ‘treatment resistant’ patients (especially use of Clozapine) o Atypical Anti-Psychotics will also ameliorate both positive and negative symptoms of Schizophrenia (unlike Typical Anti-Psychotics which only treat positive symptoms) Improvement in negative and cognitive symptoms is CRITICAL, as these are the symptoms that result in the largest ongoing impact / reduction in quality of life (rather than the positive symptoms) o Atypical Anti-Psychotics has fewer side-effects compared to Typical Anti-Psychotics o Note: Clinical outcomes are improved and rate of relapse decreased following maintenance treatment with antipsychotics Typical Anti-Psychotics (First-Generation) have a mechanism of action primarily via antagonism of Dopamine D2 Receptor (~80% at therapeutic dosage) Atypical Anti-Psychotics (Second-Generation) have a mechanism of action via high-affinity antagonism of Dopamine D2 Receptor (~60% at therapeutic dosage), as well as high affinity for 5-HT2 receptors and moderate affinity for Alpha-Adrenergic Receptors - 87 o - 5HT-2 Receptors are NOT involved in the generation of symptoms (as drugs affecting 5HT-2 receptors only do not result in improvement of any symptoms) o Binding of 5HT-2 Receptors though will offset some of the adverse side effects of antagonising D2 Receptors (which is a mechanism of action of all antipsychotics) o Note: Aripiprazole (which is a Quinolinone Derivative) is a D2-Partial Agonist (rather than being a D2-Antagonist like the other Antipsychotics) Key side-effects of Typical Anti-Psychotics include movement disorders, anticholinergic effects and endocrine abnormalities and arrhythmia o These are present, but to a lesser extent / severity in Atypical Anti-Psychotics o However, Atypical Anti-Psychotics have a higher risk of Metabolic Syndrome (i.e. weight gain, insulin resistance, dyslipidaemia) o Note: These side effects are highly problematic and can result in poor compliance / adherence to treatment with Antipsychotics Differentiate atypical from typical antipsychotics in terms of chemical classes, clinical efficacy and side effect profiles - Typical Anti-Psychotics (First-Generation) include: o Phenothiazines (e.g. Chlorpromazine, Thioridazine) o Butyrophenones (e.g. Haloperidol) o Thioxanthenes (e.g. Flupenthixol) Atypical Anti-Psychotics (Second-Generation) include: o Diazepines (e.g. Clozapine, Olanzapine) o Dibenzothiazepines (e.g. Quetiapine) o Benzamides (e.g. Amisulpride) o Benzisoxazols (e.g. Risperidone) o Quinolone Derivative (e.g. Aripiprazole) - BIPOLAR DISORDERS Be aware of the epidemiology, genetics and demographic characteristics of patients with bipolar disorder and to appreciate the common comorbid medical and psychiatric conditions - Bipolar Disorder will involve shifts and swings between highs (i.e. mania) and lows (i.e. depression) o These swings are not the normal responses to shifts in circumstances, but pathological Bipolar Disorder can be subclassified into: o Bipolar I = Major Depressive Episode + Mania o Bipolar II = Major Depressive Episode + Hypomania Bipolar Disorder has a lifetime prevalence of 2.9% in Australia with a mean age of onset of ~17-21 o Whilst there is no gender difference in the incidence of Bipolar Disorder, women are more likely to seek help (compared to men who are more likely to avoid treatment and engage in self-medication with alcohol / drugs) ~15% of Bipolar patients will complete suicide (which is a higher proportion than patients with depression or Schizophrenia) o Males are 4x more likely than females with Bipolar Disorder to complete suicide Common comorbidities with Bipolar Disorder include Anxiety Disorders, Substance Abuse and ADHD o Obesity and metabolic syndrome are also more likely (potentially due to side-effects of Atypical Antipsychotic treatment) Maintaining regular circadian rhythms (i.e. sleeping and waking up at regular times) will have a significant impact on the prognosis of patients with Bipolar Disorder BDNF is believed to have a significant impact in Bipolar Disorder, although its exact impact is still unclear - - - - - List the signs and symptoms characteristic of bipolar mania and depression 88 - - Signs and Symptoms of Mania in Bipolar Disorder include: o Activity / Behaviour Hyperactive / restless ‘Unlimited’ energy Decreased need for sleep Pressure speech Erratic, unpredictable, risk-taking Increased libido and hypersexuality Excessive spending / overgenerous Increased goal directed behaviour o Thought Form Racing thoughts Distractable o Thought Content Inflated self-esteem / grandiosity Mood congruent hallucinations and delusions Signs and Symptoms of Depression in Bipolar Disorder include: o Hypersomnia o Hyperphagia o Leaden paralysis o Psychomotor retardation o Psychotic features / pathological guilt o Lability of mood Recognise the typical presentation of hypomania, mania and depression - Mania will present with hyperactive behaviour and thought form as well as delusional / inflated thought content(per earlier list) o Mania can be sufficiently severe to result in hospitalisation, psychosis and occupational / social dysfunction o In comparison, Hypomania will have similar overall signs / symptoms as Mania, but is a less severe form and hence will not result in hospitalisation, psychosis and occupational / social dysfunction Bipolar Depression has contrasting signs / symptoms compared to Unipolar Depression o Bipolar Depression results in hypersomnia, hyperphagia, leaden paralysis, etc. and will have an earlier age of onset and shorter duration depressive episodes o Unipolar Depression results in insomnia, reduced appetite, normal / increased activity, etc. and will have a later age of onset and prolonged depressive episodes - Understand the treatment options available for Bipolar Disorder - Different treatment will be required for Bipolar Disorder patients depending on their particular mood state (e.g. different treatment in mania vs. depression vs. average) Treatment of Bipolar Mania can involve: o Lithium Carbonate This will result in dehydration, so it’s CRITICAL for patients to hydrate regularly There is a narrow therapeutic window for Lithium, so it’s important to regularly monitor plasma concentration levels to prevent toxicity (and ensure efficacy) o Sodium Valproate o Atypical Antipsychotics (e.g. Aripiprazole, Olanzapine, Quetiapine) o Carbamazepine o Benzodiazepines o Note: Combinations of the above are often needed, though aim for monotherapy if possible Treatment of Bipolar Depression can involve: o Lamotrigine. Lithium and Quetiapine (i.e. Atypical Anti-Psychotic) are the most effective treatments for Depressive Episodes in Bipolar Disorder - - 89 o - - - - Alternatively, combination therapies (e.g. SSRI + Lithium, SSRI + Valproate, Valproate + Lithium) can be an effective treatment for Depressive Episodes in Bipolar Disorder o Note: Generally avoid TCAs in combination therapies as these have a higher likelihood of triggering ‘switching’ Antidepressants are not particularly effective at treating the Depressive periods of Bipolar Disorder (despite similar clinical presentations) o Indeed, Antidepressants may actually exacerbate Depressive periods and / or result in ‘switching’ (i.e. rapid switch from depressive to manic episode) o Similarly, Mood Stabilisers are more effective at treating Manic episodes of Bipolar Disorders and less effective at treating the Depressive episodes Lifestyle factors (e.g. diet, exercise, sleep, light levels, etc.) have a significant impact on the severity of Bipolar Disorder o Improving lifestyle can result in a significant improvement in the management of Bipolar Disorder Psychoeducation is an important part of managing Bipolar Disorder and involves teaching patients to better understand their condition (e.g. red-flags / triggers) so they know when to seek help and what to do in those circumstances o Furthermore, this education will assist patients take greater control in managing their condition and optimising lifestyle factors Electroconvulsive Therapy (ECT) is extremely effective for Bipolar Disorder (~80% remission rate), but this is a risky procedure (e.g. anaesthetic, hospitalisation, risk of memory loss) PAEDIATRICS ASSESSMENT – PAEDIATRIC SELF-DIRECTED LEARNING PR OJECT (SDLP) TBA - Paediatric History will need to include considering of ‘ADING’ (per below) in addition to components of adult history: o Antenatal / Perinatal o Development o Immunisations o Nutrition o Growth o Note: Remember to also ask about demographic information too! Physical examination / development assessment should cover the five key domains (i.e. gross motor, fine motor, speech / language, social, hearing / vision) There is a range of ‘normal’ development milestones for each of the different domains o Delay in a single domain is not necessarily an issue given this range of development o However, it is more concerning if there is a developmental delay in multiple domains (or regression in any domain!) - PAEDIATRIC HISTORY T AKING Understand the content differences between a medical history for a paediatric patient compared with an adult - Paediatric History will include greater focus on the following (in addition to the typical components of an Adult History): o Antenatal and Perinatal History (e.g. Pregnancy, Gestational Age at Delivery, Labour / Delivery, APGAR, Neonatal issues, etc.) o Development History o Immunisation History o Nutrition 90 o o o Growth (Note: ALWAYS plots the Weight, Length / Height and Head Circumference against the age and gender growth chart plots!) Family History Social History (e.g. family structure, home environment, schooling, etc.) Understand how the age of the child has an impact on obtaining an appropriate medical history - Younger children will be unable to communicate as effectively as older people, so this will mean that the type of questions asked will need to use age-appropriate language o Indeed, most of the history for a child is likely to be taken from a parent / carer instead! o However, always aim to take some of the history from the child if possible (greater % of the history can be taken the older the child) o Note: Children aged 4 or over may be able to provide some of their own history When taking a history of a child, it is important that appropriate preparations are taken beforehand o This may involve having appropriate ways to distract the child, siblings, etc. when speaking the parent / caregiver (who generally will give most of the history) o Alternatively, having toys and the parent present may make the child more comfortable, and hence more willing to speak with the examiner - Understand all the ramifications of the parents or caregivers as historian in obtaining a medical history for a paediatric patient - Paediatric History Taking is distinct from Adult History Taking as the history is commonly taken from another person (i.e. parent and / or carer) rather than the child themself o This means the types of questions asked are different as it can be difficult to elicit symptoms (and instead there is a need to focus on signs) Parents know their child extremely well so pay close attention to any concerns the parent / carer may have o The parent / carer has been with the child since birth and can readily identify any abnormalities o However, do NOT assume the parent’s interpretations of signs / symptoms are always correct (as they are NOT trained medical professionals) One parent may not know all the relevant details of the child’s condition, so it may be necessary to speak with both parents together o However, if there are any disagreements between the parents, this will make things difficult Parents are likely to be extremely stresses / emotional if their child is sick, so it may be more difficult to take a history from them - - - Understand the appropriate wording of questions in taking a paediatric history, and appropriate use of questions - Communicating with the child directly will require use of age appropriate language, which places limitations in the type / complexity of questions that can be asked (e.g. “point to where the sore is” [when asking child about headache]) Other examples of age-appropriate words may include ‘poo’, ‘ouch’, ‘sore’, etc. Develop an awareness of clinical settings in which it is appropriate to obtain a complete medical history compared to a more limited, focused history - The context of the presentation will affect the extent / comprehensiveness of the history taken: o During life-threatening presentations, it is preferable to take a more limited focused history (i.e. following the pneumonic ‘AMPLE’ – Allergies, Medications, Prior Medical History, Last Meal, Events [i.e. mechanism of injury, injuries, signs, treatments]) o However, if there is a non-urgent situation, then a more complete medical history will be preferred 91 Understand how to examine a paediatric patient - Examination of a paediatric patient will include assessment of: o Well vs. unwell (e.g. pale, jaundiced, lethargic / altered consciousness, dyspnoeic, etc.) o Growth (including plotting on Growth Chart) o Nutrition (as poor nutrition can be observed via changes in hair, skin, muscle bulk, fats, etc.) o Dysmorphic Features (e.g. Cushing facies, Acromegaly facies, Down facies, etc.) o Development o Other (e.g. IV, NGT, scars, aids, etc.) Note: It is CRITICAL to have the parent and child become comfortable with the examiner prior to being able to conduct a physical examination o Otherwise the child will be scared and non-compliant with the ‘stranger’ who is touching them o Taking a history is a good way to build rapport with the child and their parent prior to conducting a physical examination - ETHICS INTRODUCTION TO MEDI CAL ETHICS – PART I TBA - Ethics does NOT just involve the significant, large-scale dilemmas (e.g. euthanasia, abortion, etc.), but also smaller, day-to-day decisions / approaches (i.e. ‘Microethics’) o Microethics are pervasive throughout medicine in the way doctors approach their patients, communicate their patients, offer particular treatments / recommendations, etc. Becoming a good doctor will require developing a sense of ‘other’ developing this empathy / understanding of other’s situations / perspectives will guide the doctor in providing the most appropriate care - OTHER INTRODUCTORY LECTURE An introduction to Stage 2 and Block 6 NEUROPATHIC PAIN Describe the definition of neuropathic pain - ‘Neuropathic Pain’ is pain caused by a lesion or disease of the somatosensory nervous system o In contrast, ‘Nociceptive Pain’ is pain that arises from actual or threatened damage to nonneural tissue and is due to the activation of nociceptors Neuropathic Pain is commonly sharp, burning, shooting, electric pain that will occur in an area of sensory deficit o In contrast, Nociceptive Pain is commonly dull pain that will occur from an area with sensation - Describe the pathophysiological changes associated with neuropathic pain, and the possible mechanisms responsible for these changes - Neuropathic Pain can occur following damage to the: o Nerve (e.g. transaction, compression, crush / stretch, neuropathy) o Dorsal Root Ganglia (e.g. compression, inflammation, root avulsion) o Spinal Cord (e.g. contusion, tumour, hemisection, syrinx, inflammation) 92 o - - - Brainstem / Thalamus / Cortex (e.g. infarction, inflammation, tumour, trauma, electrical imbalance [e.g. Epilepsy], chemical imbalance [e.g. Parkinson’s Disease]) There are genetic factors that result in some patients being more susceptible to neuropathic pain o These genetically susceptible people produce increased levels of GTP Cyclohydrolase (GCH1), which is a particular enzyme associated with Neuropathic Pain The pathophysiological changes that occur with Neuropathic Pain may include increased sensitivity to stimuli, spontaneous activity / neurotransmission, loss of central inhibition of pain and neuroplasticity There are several different mechanisms proposed for the development of Neuropathic Pain including: o Central Sensitisation of Dorsal Horn Neurons – Nerve injury can result in increased Na+ and Ca2+ channel expression, which will result in increased electrical activity This will trigger increased release of Glutamate in the Dorsal Horn, which will activate NMDA Receptors in Post-Synapse, eventually resulting in gene transcription and long-term changes in the post-synaptic cell The post-synaptic cell will thus develop increased cell activity / responsiveness (which can result in neuropathic pain!) (i.e. Central Sensitisation of Dorsal Horn Neurons) Note: Glial cells are also involved in this mechanism that increases cell activity / responsiveness via release of pro-inflammatory cytokines, ATP, Nitric Oxide, etc. o Spontaneous Activity of Transmission Neurons – this may be a cause of ‘Phantom Pain’ following amputation o Reduction of Central Inhibition – Damage to the spinal cord may prevent signals from descending inhibitory pathways (which can increase the person’s sensitivity to pain) o Sprouting Hypothesis – Given touch nerve endings in the Deep Dorsal Horn sprout / re-grow into the Superficial Dorsal Horn (which has cells that transmit Pain), this sprouting contributes to increased sensitivity to pain from normal touch stimuli o Maladaptive Neuroplasticity – this will result in activation in the areas of the Cortex associated with the amputated limb following stimulation of adjacent areas of the Cortex o Various other peripheral mechanisms (e.g. upregulation of peripheral receptors / ion channels, spontaneous ectopic activity in damaged primary afferent nociceptors, phenotypic changes in pain pathways) Treatment for Neuropathic Pain will involve preventing the above mechanisms (i.e. reduce activity in PNS and CNS, block neuroplasticity, block spinal sprouting, etc.) o However, these medications that reduce CNS activity will unfortunately have significant adverse side-effects too (e.g. inhibition of memory) o Anti-depressant and Anti-convulsants are the most common medications currently used to treat Neuropathic Pain o These treatments have low effectiveness (i.e. the best treatments available for Neuropathic Pain will only deliver a 50% reduction in pain in 1/3 patients) AUTOPSY PROCESSES Describe the sequence of events that lead to serious morbidity and death for a patient - The sequence of events that lead to morbidity / death will depend on the particular patient and their circumstances Examples of such sequences include: o Carcinoma of the colon lung metastases bronchial obstruction pneumonia death o Motor vehicle accident fracture of C2 vertebra cardiorespiratory arrest o Atherosclerotic disease in a patient with hyperlipidaemia and hypertension aneurysm of ascending aorta rupture of aneurysm haemopericardium cardiac tamponade acute cardiac failure death - Describe what is meant by 'cause of death', and describe how the cause of death is determined in different circumstances, making reference to the degree of certainty with which the cause of death is recorded 93 - ‘Cause of Death’ refers to the specific disease or injury that started the sequence of events leading to the death This will require understanding the sequence of events that resulted in the death, and recording each of these steps in the sequence as the cause of death Note: ‘Manner of death’ refers to ‘how’ the person died (e.g. homicide, suicide, accident, natural disease, therapeutic complication, undetermined) List the criteria for the diagnosis of death - Conventional diagnosis of death involves confirming: o Absence of heartbeat (i.e. circulation) o Absence of breathing (i.e. respiration) o Fixed pupils (that are also usually dilated) (i.e. neurological) Note: More complex definitions may be used in the context of organ transplantation or “brain death” with assisted ventilation - Outline the legal duties of a medical practitioner with regard to the diagnosis of death, determination of the cause of death and the preparation of a death certificate - When a person dies, the medical practitioner (potentially including an intern) should: o Check for signs of life (i.e. circulation, respiration, neurological) and confirm that the person is dead o Complete a Death Certificate Form o Note: Death should also be specified within the medical record of the patient too Completion of the Death Certificate Form will require specifying the cause of death (i.e. including the sequence leading up to the ultimate cause of death) and other co-morbid conditions o Cause of Death entered into the Death Certificate should be based on the reasonable belief of the clinician o The clinician does NOT have to be definitive / 100% confirmed about the cause of death, but instead only have a reasonable belief that this is the cause of death o Note: If the Autopsy identifies a different Cause of Death to that listed in the initial Death Certificate, then a new Death Certificate can be reissued If the Death Certificate cannot be completed, then the death is reported / referred to the Coroner - List the types of circumstances in which a medical practitioner is not permitted to issue a death certificate and must refer the death to the Coroner - Circumstances where a medical practitioner cannot issue a death certificate and must refer the death to the Coroner include: o Believes that the manner of death was anything other than natural disease o Does not know the patient, or has not seen him/her in the last 6 months o Has no idea what the cause of death is likely to have been o Other circumstances as defined in State legislation, such as: Violent / unnatural death Sudden death with cause unknown Suspicious or unusual circumstances Death in police custody or during police operations Death of resident of mental health facility Death from an accident (unless person >72 years where accident attributable to age) Death during health-related procedure that was NOT a reasonably expected outcome Death of child in care, a child reported under child protection legislation within 3 yr, a child who is a sibling of a child reported within 3 yr, or a child who may have suffered abuse or neglect 94 Death of person living in residential care for disabled persons or a disabled person who receives services to enable independent living in the community Describe how an autopsy contributes to the determination of the cause of death - Autopsy involves a comprehensive examination of the body and its organs, and will enable the identification of pathology through the body o There are different levels of investigations (e.g. external investigation vs. full post-mortem) that can be conducted depending on the needs of the Coroner o The Coroner will aim to utilise the most minimally invasive investigation as possible (to maximise the dignity of the patient) that will still provide the necessary information for the coroner In conjunction with the Police Report to the Coroner(which will contain a narrative that can explain why the person’s death has been referred to the Coroner), this will enable identification / confirmation of the underlying cause of death - Explain the process of death certification to the next-of-kin of a patient who has died, including (for appropriate cases) the autopsy process and the role of the Coroner - Death certification involves detailing a cause of death for the patient who has passed away o All registered medical practitioners can complete a Death Certificate, except in certain specified circumstances in which the death must be referred to the Coroner The Coroner is tasked with investigating the death and confirming the cause of death o The Coroner will aim to utilise the most minimally invasive investigation possible to confirm the cause of death and issue a Death Certificate o In certain circumstances, this will require an Autopsy to be conducted, which will involve assessment of the different internal cavities of the body and the different organs Small specimens of tissue may be removed for assessment under microscopy or toxicology However, the rest of the organs / tissue are returned to the body, which will then be restored / sewn up, after which the body will be returned to the family Note: Organs are not retained for ‘museum’ or research purposes, and any retention for further testing is minimal and only occurs with family knowledge - FRAMING DISABILITY Identify examples of disability discrimination in past and current medical practice - Disability discrimination in the past includes forced sterilisation of the disabled o However, there continues to be forced sterilisation of disabled people (mostly women) in the past ~20 years o Current law requires court approval for forced sterilisation (which will only be granted if sterilisation is the most appropriate treatment and necessary to save life or prevent serious damage to health) o Despite the legal requirement for court approval, there is anecdotal evidence of an increasing numbers of disabled girls being sterilised without such court approval (as carers / medical practitioners know they will not meet the threshold required for approval!) Alternatively, discrimination of the disabled can occur through: o Low expectations – these can become self-fulfilling and / or internalised by the person themselves (e.g. segregated education and work) o Limited information / life experience – this results in the person being aware of available options o Barriers to access (e.g., print, complexity, big words, presenting information too quickly) o Fragmented information about disability services - 95 o Rigidity of service models (inflexible eligibility criteria, service gaps, etc.) Describe how disability can be understood as a human rights issue - Disability can be viewed as a human rights issue given the past and current history of discrimination against disabled people ‘UN Convention on Rights of Persons with Disabilities’ aims to guarantee certain human rights for all disabled people that will enable them to live their life fully and be a full member of society o In particular, these rights must include respect for the person, their physical / mental integrity and their autonomy - Compare different ways of understanding disability - There are multiple different paradigms for viewing / interpreting disability; these different paradigms have their own particular advantages and disadvantages: o ‘Medical Model of Disability’ focuses solely on the impairment / medical condition (but does NOT consider social and environmental factors) o ‘Holistic Model of Disability’ views disability as an outcome of the interaction between a person’s impairment, their individual characteristics, their activity / participation and their environment o ‘Social Model of Disability’ views disability as a social construct used to oppress a minority group who challenge social norms via their ‘impairment’ Examine the likely reasons for the changes in life expectancy among people with Down syndrome - The dramatic improvement in life expectancy for People with Down Syndrome post-WWII is not only due to the development of antibiotics (to treat respiratory infections) and cardiac surgery (to treat congenital heart issues), but also that these people are now provided with the best medical care o People with Down Syndrome were previously discriminated against and not provided with the best medical care Identify specific health care needs of people with Down syndrome - Particular heath care needs for people with Down Syndrome include treatment of: o Congenital Heart Problems o Alzheimer’s Disease o Developmental / cognitive impairment o Predisposition for obesity o Hearing problems TEMPERATURE REGULATI ON Describe mechanisms of body temperature regulation, including mechanisms of heat exchange, the consequences and management of hyperthermia and the role of the hypothalamus in thermal regulation - Body temperature varies with a Circadian Rhythm (amplitude of 1 degree) such that temperature is lowest at 3-6am and highest at 3-6pm o In women, body temperature will also vary based on menstrual cycle (i.e. usually increasing about 1 degree during the post-ovulatory phase) Heat production by the body will vary depending on the metabolic rate; this metabolic rate can be changed by: o Voluntary and involuntary muscle activity o Hormones (e.g. Thyroxine, Adrenaline) o Tissue temperature (such that a rise in tissue temperature itself can increase metabolic rate) Heat loss from the body can occur through several different mechanisms including: - - 96 o - - - - Radiation Heat is gained or lost by radiation at a rate that is proportional to the temperature difference between the skin and the radiating body, and the surface area of the exposed skin o Conduction This is only significant when the skin is in contact with a conducting surface (e.g. ice, ground) o Convection This occurs when heat is carried by air or water from the skin Rate of convective heat loss will be proportional to the temperature difference between the skin and the ambient environment, and the body surface available for convective exchange and the convective heat transfer coefficient Convective Heat Transfer Coefficient is highly variable depending on the scenario (e.g. 5x as wind velocity increase, 100x if immersed in water) o Evaporation Humans can dissipate nearly all heat produced by evaporating sweat Rate of evaporative heat loss will depend on Evaporative Heat Transfer Coefficient, Water Vapour Pressure gradient between the skin and air and body surface available for evaporative heat exchange Note: There will be less / reduced evaporation heat loss in highly humid environments as the water vapour pressure of the air will be higher o Note: The key factor preventing Hyperthermia is the convection of heat away from the core towards the skin via blood Physiological factors such as dehydration, heart failure, autonomic incapacity can impact upon the effectiveness of heat loss o These differences will impact on the ability to sweat as well as changing the blood flow to the skin (and hence the level of heat convected away from the core) Hypothalamus plays a key role in thermal regulation by receiving ascending thermoregulation inputs and sending descending thermoregulation signals o Pre-Optic Nuclei of the Hypothalamus is responsible for heat loss (and receives inputs from thermoreceptors and fever-producing stimuli [i.e. Prostaglandin, secondary to cytokines from immune cells]) o Dorsomedial Hypothalamus is responsible for heat conservation (and receives inputs from related to circadian rhythms / behaviour) Pre-Optic Nuclei of the Hypothalamus projects to the Dorsomedial Hypothalamus, which then projects to the Raphe Pallidus Nuclei in the Medulla, which then sends projections to: o Sympathetic Preganglionic Neurons in the Spinal Cord, which regulate sympathetic activity to skin blood vessels (i.e. vasoconstriction vs. vasodilation) o Sympathetic Preganglionic Neurons in the Spinal Cord, which regulate sympathetic activity to Brown Adipose Tissue (which can produce non-shivering heat) o Skeletal Muscles, which produce heat by shivering (by activation of Fusiform Fibres) There are two separate ascending thermoregulation pathways o Pathway 1 will synapse in the Pons (at the Parabrachial Region) and then project to the PreOptic Nuclei of the Hypothalamus o Pathway 2 will synapse in the Thalamus and then project to the Sensory Cortex (and hence provides the person with a conscious awareness of the temperature [i.e. heat vs. cold]) o Note: Temperature Regulation is still possible even if one of the pathways are damaged CRANIAL NERVES – CLINICAL PERSPECTIVE I Describe the clinical examination of the cranial nerves and identify clinical features for specific cranial nerve lesions - CNI – Olfactory Nerve o Common causes of loss of smell (i.e. anomsia) or altered smell sensation include cold / stuffed nose, smoking, medications (e.g. aminoglycosides) and trauma 97 - - - Trauma will commonly result in a bilateral loss of smell whilst a cold / stuffed nose will commonly result in a unilateral loss of smell o One of the earliest events in Parkinson’s and Alzheimer’s Disease is the loss of smell o Olfactory Tract is connected to the Amygdala (and hence is associated with memory) CNII – Optic Nerve o Visual Field Testing is CRITICAL to identify the specific loss of visual field (and hence be able to accurately isolate the location of the lesion) It is CRITICAL to understand the Visual Fields / Deficits diagram!!! for example: Lesion of the Optic Chiasm will result Bitemporal Hemianopia Lesion of the Post-Optic Chiasm will result in an Homonymous Hemianopia Lesion of the Optic Nerve will result in complete loss of vision from one eye Note: There is a loop of the Optic Tract is the Temporal Lobe referred to as ‘Meyer’s Loop’, whilst there is a loop of the Optic Tract in the Parietal Lobe referred to as ‘Baum’s Loop Lesion in Meyer’s Loop will result in a superior visual field loss Lesion in Baum’s Loop will result in a inferior visual field loss o Glistening White Optic Disc (with clear edges) is indicative of Optic Atrophy In contrast, blurry Optic Disc (including blurring of edges) is indicative of Papilloedema o Note: Visual Fields are recorded / plotted according to the patient’s perspective (i.e. right eye field is on the right side of the page, left eye field is on the left side of the page) CNIII – Occulomotor Nerve o Superior and Inferior Oblique Muscles can be isolated for testing by asking the patient to adduct their eyes Elevation of the eyes in the adducted position will test the Inferior Oblique Muscle Depression of the eyes in the adducted position will test the Superior Oblique Note: In contrast, Superior and Inferior Rectus Muscles can be isolated for testing by asking the patient to abduct their eyes o Each of the eye muscles have a specific sub-nuclei within the Brainstem as well as a separate sub-nuclei for parasympathetic innervation (i.e. Edinger-Westphal Nucleus) o Aneurysm of the Posterior Communicating Artery can result in compression of the Occulomotor Nerve (CNIII) resulting in loss of motor innervation of the relevant ocular muscles o Demyelination as an underlying cause of Optic Nerve damage will have a relapsing and remitting course (i.e. acute onset followed by recovery before remitting and occurring again) In contrast, Tumours will have a slow progressive onset whilst Vascular causes will have an acute / sudden onset o Parasympathetic fibres innervating the eye lie on top of the Occulomotor Nerve (CNIII), so compression to the Occulomotor Nerve from the top will result in both a CNIII Nerve Palsy and a constriction of the pupil this is suggestive of an Aneurysm! In contrast, ischemia of CNIII (from capillaries inferior to the nerve) will result in only CNIII Nerve Palsy (but NO constriction of the pupil as the Parasympathetic Fibres are unaffected) this is suggestive of diabetic ischemia o ‘False image’ in Diplopia is ALWAYS the outer / lateral image, and is derived from the affected eye This occurs as the affected eye does not move is the appropriate direction, so the inputs to the eye hit the incorrect part of the Retina As the different areas of the Retina are mapped to different parts of the Visual Fields, this will result in the brain interpreting the visual input to be coming from a different direction (thus creating the ‘false image’ more laterally) Note: Identification of the affected eye can be performed by covering each eye and determining which eye when covered removes the lateral image (this will be the affected eye!) CNIV – Trochlear Nerve o Paralysis of the Superior Oblique Muscle will result in a loss of intorsion and depression of the eye 98 - - - The patient will compensate for such a paralysis by tilting their head inwards (i.e. Patient with Right Superior Oblique Muscle Paralysis will title their head towards the left) CNVI – Abducens Nerve o This is the most susceptible cranial nerve for Raised Intracranial Pressure Therefore, CNVI Nerve Palsy is NOT necessarily a localising sign and may result from a pathology (e.g. tumour, haematoma, etc.) in the other side of the brain (which causes an increase in Intracranial Pressure) Overall Eye Muscles (CNIII, CNIV, CNVI) o Medial Longitudinal Fasciculus (MLF) is a pathway that connects the Occulomotor, Trochlear and Abducens Nuclei (i.e. CNIII, IV and VI) This is a key structure enabling conjugate gaze (i.e. both eyes move in the same direction at the same time) by enabling synchronous movement of the different eyes muscles o Lateral Rectus of one eye (i.e. Abducens Nucleus) and Medial Rectus of the other eye (i.e. Occulomotor Nucleus) are connected via the Medial Longitudinal Fasciculus (MLF) The Abducens and Occulomotor Nuclei being connected via the MLF are on opposite sides of the brainstem (with the connecting MLF contralateral to the Abducens Nuclei and ipsilateral to the Occulomotor Nuclei) This connection ensures that both eyes move horizontally synchronously (i.e. horizontal conjugate gaze) Lesion of the MLF is referred to as a ‘Internuclear Ophthalmaplegia’ (INO), and will result in the failure of the other eye to adduct (i.e. due to loss of input to the Occulomotor Nucleus responsible for adduction by the Medial Rectus) This occurs as the direction of the signal is from the Abducens Nuclei towards the Occulomotor Nuclei) Note: The eye that successfully abducts may also have Nystagmus (fastphase directed medially) in response to the failure of the other eye to adduct Note: MLF also connects the Occulomotor and Trochlear Nuclei on the same side of the brainstem Occulomotor Nuclei innervates a range of ipsilateral Ocular Muscles, whilst Trochlear Nuclei innervates contralateral Superior Oblique Muscle The MLF is the pathway via which the Vestibular Nuclei sends signals to coordinate these eye muscles to enable smooth pursuit eye movements Note: The fibres connecting the Occulomotor and Trochlear Nuclei that enable both eyes move synchronously (i.e. vertical conjugate gaze) travel via the Tectospinal Tract (which is carried within the MLF) o Direction of the fast-phase in Nystagmus will be towards the same side of the lesion (if due to a Cerebellar lesion), but the opposite side of the lesion (if due to a Vestibular lesion) o Ocular light reflexes will involve CNII (Optic Nerve) as the afferent nerve and CNIII (Occulomotor Nerve) as the efferent nerve There will be a different pattern of light reflexes (in both the target eye and consensual eye) depending on the site / location of the lesion o Horner’s Syndrome (i.e. Ptosis, Meiosis, Anhydrosis) results from a loss of sympathetic innervation of the eyes (whilst parasympathetic innervation remains) CNV – Trigeminal Nerve o Pain and Temperature Sensation for the Head and Neck is via the Spinal Trigeminal Nucleus / Tract in the Brainstem The different topographical areas of the Spinal Trigeminal Nucleus / Tract (i.e. Rostral vs. Caudal) will innervate different areas of the head and neck in an ‘onion ring’ distribution; in particular: Rostral Spinal Trigeminal Nucleus / Tract (in the Pons) will provide pain and temperature sensation for the mouth, teeth and pharyngeal cavity (i.e. central face) 99 - - - - - - Middle Spinal Trigeminal Nucleus / Tract (in the Upper Medulla) will provide pain and temperature sensation for the nose, cheeks and lips (i.e. middle face) Caudal Spinal Trigeminal Nucleus / Tract (in the Lower Medulla) will provide pain and temperature sensation for the scalp, ears and chin (i.e. peripheral face) This ‘onion ring’ distribution of the Spinal Trigeminal Nucleus / Tract differs from the Dermatome distribution of the three branches of the Trigeminal Nerve (CNV) and is reflective of different embryological development o Assessment of the muscles of mastication can also be used to test for a CNV lesion o Corneal Reflex involves both eyes blinking when a wisp of cotton wool touches the cornea (with the cotton bud arriving from the side of the eye) This assesses both the afferent CNV1 (Ophthalmic Branch of Trigeminal Nerve) and efferent CNVII (Facial Nerve) CNVII – Facial Nerve o Lower Motor Neuron Facial Nerve (CNVII) Palsy will result in a same level of weakness throughout all the areas innervated by CNVII This can result in hyperacusis (due to weakness of innervation to the Stapedius Muscle) and inhibition of taste Note: Bell’s Palsy is an examples of Lower Motor Neuron Facial Nerve Palsy o In contrast, Upper Motor Neuron Facial Nerve (CNVII) Palsy will result in: Less weakness of the upper facial muscles (compared to the lower facial muscles which will have greater weakness) (such that person may be able to wrinkle their forehead); and Minimal impact on Emotional Facial Responses (compared to Voluntary Facial Responses which are completely lost) CNVIII – Vestibulocochlear Nerve o Lesion will result in loss of the Vestibulo-Ocular Reflex (which can be tested via the Head Impulse Test) CNIX – Glossopharyngeal Nerve AND CNX – Vagus Nerve o CNIX and CNX (Glossopharyngeal and Vagus Nerves) are closely related topographically, and are commonly tested together Gag Reflex involves testing CNIX (as the afferent nerve) and CNX (as the efferent nerve) Lesion of CNIX on one side will result in failure to trigger Gag Reflex upon stimulation of one side of the Pharynx, but the triggering of the Gag Reflex upon stimulation of the other side of the Pharynx (unless there is a bilateral CNX lesion) Note: Avoid testing Gag Reflex if possible (due to discomfort the patient) and instead attempt to utilise other tests (e.g. ability to swallow, patient cough, etc.) o CNIX (Glossopharyngeal Nerve) can be tested in isolation by assessing sensation in the Pharynx / Soft Palate, swallowing (difficulty if there is CNIX weakness) and /or taste in the posterior 1/3 of the tongue (though this is rarely tested) o CNX (Vagus Nerve) can be tested in isolation by asking patient to cough (‘bovine’ cough if there is CNX weakness), produce a high-pitched note (unable to do if there is CNX weakness) and swallow (difficulty if there is CNX weakness) CNXI – Accessory Nerve o This can be assessed by asking patient to shrug their shoulders (Trapezius Muscle) and / or rotate their head against resistance (Sternocleidomastoid Muscle) CNXII – Hypoglossal Nerve o Lesion will result in the tongue being atrophied and / or pushed towards the side of the lesion (as the ‘strong’ side of the CNXII will push the tongue towards the weaker / lesioned side) Other potential pathologies (and accompanying signs) to consider include: o Cavernous Sinus Syndrome – this will result in compression of CNIII, IV, V1, V2 and VI (which pass through this sinus) resulting in a constellation of signs / symptoms affecting these nerves 100 o o Cavernous Sinus is also a site of venous drainage, so compression of the Cavernous Sinus may also result in swelling of that side of the face Acoustic Neuroma – this can result in a lesion at the Cerebellopontine Angle resulting in compression of CNV, VII and VIII Note: Angle of the Jaw (and further posterior) has sensory innervation by the C2 Spinal Nerve However, this area at the angle of the jaw / ear is a border zone where there can be sensory innervation by CNV3 (Trigeminal – Mandibular Branch), CNVII (Facial Nerve), CNIX (Glossopharyngeal Nerve) and C2 Spinal Nerve This is important as shingles of any of these nerves can result in vesicles in the ear PPD ASSESSMENT Consider the role of peer assessment in moderating group behaviour, building on their experience in Stage 1 - Peer assessment will provide an understanding of one’s strengths and development points o This awareness will provide guidance of how and where to change behaviours to optimise group performance CORTICAL LOCALISATION Describe concepts of laterality in the function of the CNS - One side of the brain will generally receive inputs / send afferents to the contralateral side of the body (e.g. motor, sensory) There is a dominant and non-dominant hemisphere in the brain o The dominant hemisphere will have different functions compared to the non-dominant hemisphere o Left Dominant Brain is significantly more prevalent (i.e. ~99% of Right-Handed people and ~60% of Left-Handed people have a Left Dominant Brain) Dominant Hemisphere will contain the key speech / language areas (i.e. Broca’s Area and Wernicke’s Area) as well as different functions from the Parietal Lobe o As a result, there are specific signs / symptoms associated with a lesion in the dominant hemisphere (compared to the non-dominant hemisphere) o For example, with regards to a lesion of the Parietal Lobe: Dominant Parietal Lobe lesion will result in AALF (Acalculia, Agraphia, Left-Right Disorientation, Finger Agnosia) as well as Ideomotor and Ideational Apraxia (i.e. inability to imitate or conceptualise / plan movements respectively) Non-dominant Parietal Lobe lesion will result in Neglect, Constructional and Dressing Apraxia and Anosognosia (i.e. person unaware of disability) - - Describe the location and function of higher centres, speech and language areas - Primary Motor Cortex is located in the Frontal Lobe between the Pre-Central and Central Gyrus o This is responsible for contralateral motor control o Primary Motor Cortex has a somatotopic arrangement such that that the medial areas are associated with the feet / legs, whilst the lateral areas are associated with the Face / Neck Secondary Motor Cortex is located immediately anterior to the Primary Motor Cortex o This is responsible for motor sequencing (e.g. co-ordinating bimanual tasks) Frontal Eye Fields are located in the Frontal Lobe anterolateral to the Secondary Motor Cortex o This is responsible for contralateral eye movements and head turning o Destruction of this area (e.g. stroke) will result in eye movement towards the side of the lesion, whilst activation of this area (e.g. seizure) will result in eye movement away from the side of the lesion Prefrontal Association Cortex is located in the anterior aspect of the Frontal Lobe - - 101 o - - - - - - - This is responsible for cognitive function, thinking, behaviour (e.g. motivation, inhibition of socially unacceptable behaviour) and primitive reflexes Broca’s Area is located in the lateral Frontal Lobe adjacent to the Lateral Fissure in the Dominant Hemisphere o This is responsible for the motor production / expression of speech o Lesion to this area will result in difficulty to generate speech / language (though can understand speech / language from other) (i.e. Expressive Dysphasia) These patients are aware of their deficit, and hence will become frustrated Wernicke’s Area is located in the Temporal Lobe near the Lateral Fissure in the Dominant Hemisphere o This is responsible for the understanding of speech / language o Lesion to this area will result in a failure to understand language from others and a failure to generate meaningful speech (but can be able to fluently speak) (i.e. Receptive Dysphasia) These patients are unaware of their deficit Arcuate Fasciculus is the connection between Broca’s and Wernicke’s Areas in the Dominant Hemisphere o Lesion of this area will result in ‘Conductive Dysphasia’ whereby there is normal comprehension, inability to repeat words or phrases and fluent but meaningless speech o These deficits occurs as there is a inability to apply the understanding of different speech to its expression (due to the loss of key link), but expression is still possible Note: Global Dysphasia (affecting both Broca’s and Wernicke’s Area) is more common than Expressive or Receptive Dysphasia alone The different types of Dementia (and their clinical signs / symptoms) reflect the different sites of the pathology in the brain: o Frontotemporal Dementia Behavioural variant occurs due to damage to the Prefrontal Cortex Progressive Non-Fluent Aphasia variants occurs due to damage to the Left Frontal Lobe (i.e. Broca’s Area) Semantic Dysphasia variant (i.e. loss of understanding / reading of words) occurs due to damage to the Left Temporal Lobe (i.e. Wernicke’s Area) o Alzheimer’s Dementia and its loss of memory occurs due to damage to the Hippocampus and Entorhinal Cortex Primary Somatosensory Cortex is located in the Parietal Lobe between the Post-Central and Central Gyrus o This is responsible for receiving contralateral sensory input o Primary Somatosensory Cortex has a somatotopic arrangement such that that the medial areas are associated with the feet / legs, whilst the lateral areas are associated with the Face / Neck Parietal Association Cortex is located posterior to the Secondary Somatosensory Cortex o This is responsible for processing multiple different sensory inputs o Lesion will result in loss of contralateral sensation, 2-point discrimination, astereognosis, dysgraphaesthesia Primary Visual Cortex is located on the upper and lower banks of the Calcarine Sulcus in the Occipital Lobe, and is responsible for vision o If there is a lesion in the Occipital Lobe, ‘Macular Sparing’ will occur when the lesion is more anterior, whilst ‘Homonymous Hemianopia’ will occur when the lesion is more posterior AUDITORY PATHWAYS AN D COCHLEAR IMPLANTS Identify the anatomical organisation of the auditory pathways - Sound will undergo several different sub-cortical stages of processing before a person becomes aware of the sound o There are also several descending connections from the Cortex that modulate what auditory signals ascend towards the Cortex Auditory Pathway commences at the Ear (which is sub-divided into the External, Middle and Inner Ear) - 102 o - - - - - - External Ear will funnel sound towards the Middle Ear (i.e. Tympanic Membrane, Ossicles), which then vibrate causing the vibration of fluids in the Inner Ear o Note: ‘Conductive Hearing Loss’ occurs due to a blockage (e.g. physical block, fluid, etc.) in the External and / or Middle Ear preventing the sound from arriving at the Cochlear Inner Ear contains three semi-circular canals, Vestibule and Cochlear, act to enable sense of balance and hearing ‘Organ of Corti’ is located within the Cochlear (sitting upon the Basilar Membrane), and is the structure that transduces sound waves (which cause movement of fluid within the Cochlear) into electrical impulses that are transmitted to the Brain o Movement of fluid will result in bending of Basilar Membrane Basilar Membrane is not a uniform structure, but instead has different width and rigidity along its length (which allows different parts of the Basilar Membrane to detect different frequencies of sound) o Single Layer of Inner Hair Cells within the Organ of Corti will detect movement of Basilar Membrane resulting in transmission of electrical signal towards the Brain Tectorial Membrane will vibrate following movement of Basilar Membrane resulting in the Inner Hair Cells to move This physical movement of the Inner Hair Cells causes the opening of ion channels at the tips of the Inner Hair Cells This opening of ions channels results in inflow of K+ ions into the Scala Media, which results in depolarisation of the Inner Hair Cells Depolarised Inner Hair Cells will then release vesicles the cause depolarisation of the Auditory Nerve Fibres (and hence conversion of the sound into an electrical signal for transmission to the Brain) Note: There are another three layers of Outer Hair Cells within the Organ of Corti that provide support to the Cochlear and will amplify / refine the frequency selectivity of the Cochlear There are two types of Auditory Nerve Fibres: o Type 1 Auditory Nerve Fibres have large cell bodies, myelinated axons and exclusively contacts a single Inner Hair Cell However, multiple Type 1 Auditory Nerve Fibres will contact each single inner hair cell o Type 2 Auditory Nerve Fibres has small cell bodies, small calibre unmyelinated axons and contact multiple Outer Hair Cells o Note: Less information in known about Type 2 Fibres given they are difficult to access (due to their small size) ‘Synaptic Ribbon’ is a special structure at the synapse of the Inner Hair Cell and Auditory Nerve Fibre that enables the rapid release of vesicles at a constant rate at the Auditory Nerve Fibre o The rate of release of Vesicles will depend on the polarisation status of the Inner Hair Cell (i.e. hyperpolarised = less release vs. depolarised = more release) Exposure to loud noises can result in the reduction in the number of Auditory Nerve Fibres connected to each inner hair cell o This will result in progressive hearing loss over the long-term (which CANNOT be reversed!) o This type of hearing loss is known as ‘Sensorineural Hearing Loss’ (i.e. problem with mechanotransduction of sound to electrical impulse, connection between inner hair cells and auditory nerve fibres or within the Auditory Nerve itself) The different auditory nerve fibres connected to the same inner hair cell will respond to the same sound differently o There is intrinsic variation within Type 1 Auditory Nerve Fibres (e.g. 40% with low spontaneous firing rate vs. 60% with high spontaneous firing rate) o These differences in spontaneous firing rate will result in different sensitivity to sound (i.e. high spontaneous firing rate fibres have very low thresholds for recognising sound) Auditory Nerve will connect to the Cochlear Nucleus, which then sends signals to multiple, various higher auditory centres o Low and High Threshold Auditory Fibres will mostly project to similar areas in the Cochlear Nucleus, but will give rise to different types of synapses 103 o o o There is a Tonotopic Orientation within the Cochlear Nucleus such that: Low frequency auditory nerve fibres project into Ventral regions of the Cochlear Nucleus High frequency auditory nerve fibres project into Dorsal regions of the Cochlear Nucleus Note: This Tonotopic Orientation is retained in the Primary Auditory Cortex too There are several different cell types within the Cochlear Nucleus that recognise different features of sounds (e.g. Spherical Bushy Cells, Octupus Cells, Stellate Cells, etc.) For example, Spherical Bushy Cells are important for sound localisation Endbulbs of Held are the end of the Acoustic Nerve Fibres, and will surround Spherical Bushy Cells Deafness will result in significant atrophy of the Endbulbs of Held (i.e. plasticity!) Describe the concept of sound and its scientific basis - Sound is vibrations in the air that will vary based on: o Frequency (i.e. number of cycles per second) – this is measured in Hertz o Loudness (i.e. Amplitude / Energy / Air Pressure) – this is measured in decibels (dB) o Timing – this involves consideration of onset, duration and change Describe the general principles in the operation of a cochlear implant - Cochlear Implant involves transmitting sound activity directly to the Auditory Nerve Fibres, bypassing the hair cells o This will circumvent / ‘cure’ deafness resulting from impaired Cochlear mechanics (i.e. nonfunctional Inner Hair Cells) Cochlear Implant has two main components (i.e. External and Internal component) o External Component consists of a microphone to detect sound (akin to a hearing aid) and a processor to transmit the sound to a receiver embedded in the Cochlear o Internal Component consists of a Receiver, which converts information from the Processor and activates the Electrode Array in the Cochlear Spiral, which then produces an electric current that activates the Auditory Nerve Fibres The Electrodes will be arranged in a Tonotopic manner, such that specific frequency sounds will activate specific electrodes (and hence specific Auditory Nerve Fibres) o Note: The resolution of the Cochlear Implant is much lower than the resolution of a normal Cochlear, but it is still a significant improvement compared to deafness! Earlier implantation of the Cochlear Implant (i.e. prior to child developing language) is associated with improved hearing compared to later implantation due to brain plasticity o Endbulb Synapses in the Cochlear Nucleus will more readily adapt / convert to become normal the earlier the Cochlear Implantation (i.e. due to provision of normal acoustic stimuli) o Furthermore, the number of inhibitory synapses will return to the normal level following early Cochlear implant (i.e. due to provision of normal acoustic stimuli) - - CLINICAL P HARMACOLOGY OF OLD A GE Describe changes in pharmacokinetics and pharmacodynamics in old age - There is significant diversity in the range of lifestyle / functionality / health of elderly patients o This creates variation of pharmacokinetics and pharmacodynamics amongst elderly patients Pharmacokinetic changes that occur in old age include: o Reduction rate of in Absorption; this may be due to: Achlorhydria – this reduction in acidity in the stomach can impair the absorption of certain drugs (e.g. ampicillin, iron, ketaconazole) Reduction in Gut Motility – this will result in increased time to maximal absorption and reduced peak concentration (although the total dosage of the drug will be the same) - 104 - Increase in Gut Permeability – this will result in increased passive diffusion and reduced active transport of drugs Note: Overall, drug absorption will be slower in elderly patients (although the total dosage absorbed will be the same) o Reduction in First Pass Metabolism This will increase the concentration of the drug in the systemic circulation However, if the drug is a pro-drug (i.e. requires metabolism into the active component), reduction in first pass metabolism will reduce the concentration of the active drug in the systemic circulation o Change in Volume of Distribution due to increased proportion of fat and reduced proportion of muscle (i.e. sarcopaenia) This will increase the Volume of Distribution for Fat-Soluble Drugs, but reduce the Volume of Distribution for Water-Soluble Drugs As a result, the loading dose of the drug will have to be adapted to the different in volume of distribution (i.e. higher loading dose for fat-soluble drugs, lower loading dose for water-soluble drugs) o Reduction in Elimination / Clearance of Drugs This reduction in clearance occurs in both Hepatic Metabolism and Renal Excretion Note: Maintenance Dosage Rate will depend on the rate of clearance of a drug, so the maintenance dosage rate will need to be adjusted downwards accordingly Pharmacodynamic changes that occur in old age include: o Age-related changes in most organs (in addition to the impact of disease) can alter responses to medications o Ageing also results in reduced homeostatic reserve in many systems, such that many medications may not have the same impact in the elderly o CNS will become more sensitive to medications with age (e.g. Opioids, Benzodiazepams), whilst ANS will become less sensitive to medications with age (e.g. Beta-Adrenergic Agonists) Describe implications of these changes for safe and effective prescribing for older patients - These pharmacokinetic and pharmacodynamic changes in the elderly have implications on: o Dosing (both loading and maintenance) general rule is to halve the dose for the elderly o Effectiveness of medications o Hazards / adverse side-effects High index of suspicion is needed for ADRs to prevent Prescribing Cascade (i.e. misdiagnosis of ADRs as a new medical condition, and then offering treatment for this ‘new condition’, which then results in further ADRs) First Geriatric Principle is that elderly patients will typically present with one of the geriatric giants (i.e. falls, confusion, incontinence, failure to cope) regardless of what is the underlying cause o It is important to consider whether the presentation is actually due to an Adverse Drug Reaction (e.g. steroid usage resulting in visual impairment and proximal myopathy, which ultimately causes a Fall) o Identification of adverse drug reactions provides a simple and easy way to relieve symptoms (i.e. by stopping usage of the drug!) Polypharmacy (5 or more drugs) significantly increases the risk of ADRs o Aim to discontinue medications is possible, as this will reduce risk of ADRs and commonly will have no clinical consequences (e.g. 40% of elderly patients with antihypertensives withdrawn will remain normotensive) - - OVERVIEW OF MULTIPLE SCLEROSIS – DIAGNOSIS Describe the definition of multiple sclerosis and the main clinical features, course, prognosis and epidemiology and outline the main diagnostic investigations (MRI, VER and CSF) - Multiple Sclerosis (MS) is a chronic inflammatory demyelinating disease of the CNS 105 - - - - - - - o This will be characterised by the dissemination of lesions is space AND time MS is the most common cause of neurological disability in young adults o There are ~24,000 people with MS in Australia and prevalence is ~70/100,000 o Average age of onset of 34 o Females are more likely (2.6x) to be affected than males o Note: The increase in prevalence and incidence of Multiple Sclerosis is recent years is due to an increase in prevalence and incidence in young females There are several different clinical courses of MS: o Relapsing-Remitting This involves repeated cycles of acute symptomatic episodes followed by no symptoms Eventually, there will be incomplete recover from the acute flares such that each subsequent flare results in worsening baseline disability levels There is no deterioration in function (i.e. increased disability) between acute episodes This is the most common clinical course of MS (affecting most people with MS) o Primary Progressive This involves a steady deterioration in function (i.e. increased disability) from the beginning of the disease (though there may not some periods of occasional plateaus before function recommences deterioration) o Secondary Progressive This initially appears as a Relapsing-Remitting Course, but then shifts to a steady deterioration in function (i.e. increased disability) between acute flares o Progressing Relapsing This involves steady deterioration in function (i.e. increased disability) from the beginning of the disease, with occasional flares along the way Underlying disease in MS is progressive, though the Relapsing-Remitting course occurs due to only certain episodes reaching the clinical threshold to exhibit as a Relapse o As the underlying disease progresses over time, then the likelihood and frequency of acute clinical episodes will increase Clinical features / symptoms at disease onset include: o Motor Symptoms (e.g. weakness, unsteady gait, sphincter disturbance) o Sensory Symptoms (e.g. numbness, paraesthesia, pain, Lhermitte’s Sign) o Ophthalmological (e.g. Optic Neuritis, Diplopia, Nystagmus) o Note: MS will involve a gradual onset of symptoms / signs rather than a sudden onset Motor weakness / symptoms is the main initial presenting complaint in ~50% of MS patients o This weakness (e.g. hemiparesis) will particularly occur following exercise or exposure to heat Onset of hemiparesis will be a subacute onset or slowly progressive o Spasticity may also occur in MS patients (worse in lower limbs than upper limbs), resulting in unsteady gait and sphincter disturbance Sensory symptoms include: o Numbness o Paraesthesia o Sense of swelling / constriction around limbs or trunk o Pain (e.g. Trigeminal neuralgia / painful tonic spasms / shooting paroxysms to extremities) o Lhermitte’s Sign (i.e. electrical sensation that runs down the back and into the limbs elicited by bending the head forward) o Impaired proprioception / useless hand o Vertigo Optic Neuritis is a common early symptoms of MS and will result in: o Blurred vision / visual loss in one eye o Pain on movement of eye (due to eye movement stretching of CNIII) o Optic atrophy on fundoscopy o Central or Paracentral Scotoma 106 o - - - - - - - - Internuclear Ophthalmoplegia due to lesion in MLF (this is highly specific for MS in young, female patients) Prognosis for MS patients is highly variable with no reliable predictors at disease onset o Benign course is more likely if there is an earlier age of onset, monosymptomatic onset, rapid remission after initial symptoms, long period to second relapse, minimal pyramidal and cerebellar deficits in first five years) o 50% will need assistance walking, whilst 25% will be working full-time 10 years from onset o Mean survival is ~30 years after onset Grey Matter pathology in MS is difficult to identify using MRI imaging, but does correlate with disability progression and cognition o However, loss of Brain Volume (as evidenced by increase in size of Ventricles) is the best biomarker for neurological disability and progression of the disease Pathophysiology of MS involves autoimmune attack resulting in demyelination, axonal loss and tissue damage o Acute MS Lesions will result in the distal end of axons retracting into round bulbs Diagnosis of Multiple Sclerosis requires identification of two separate lesions in the CNS separated by space and time o This can be identified either via clinical signs / symptoms or via imaging (i.e. MRI Scan) o The advantage of imaging is that it can distinguish between new and old lesions, and hence satisfy the criteria of two lesions separated by time (even if only one clinical episode has occurred so far) Imaging is a key diagnostic tool available for MS o Gadolinium Enhancement CT Scan is the best imaging technique to identifying Acute MS Lesions These lesions are visible on T1 CT Scans are visible as ‘black holes’ (given the axons retract into round bulbs) Gadolinium normally cannot cross the Blood-Brain Barrier, but will do so in the event of inflammation (as the tight junctions breakdown) As a result, Acute MS Lesions are clearly visible on Gadolinium Enhancement CT Scans (as bright areas) Note: Gadolinium will only cross the Blood-Brain Barrier within the first ~4 weeks following clinical symptoms, after which the Blood-Brain Barrier repairs o In contrast, MRI T2 FLAIR imaging can identify previous / older MS lesions (as bright areas) Electrophysiology (i.e. Visual Evoked Response [VER] / Visual Evoked Potential [VEP]) can be useful for monitoring the progression of the patient o The slowing of electrical conduction is indicative of Demyelination (whilst the reduction in amplitude of electrical conduction in indicative of loss of Axons) o The role of Electrophysiology for diagnosis has been supplanted by the usage of MRI Scans CSF in MS will have characteristic features such as presence of oligoclonal IgG and IgG Index > 0.7 (90% of MS patients) o Protein levels may also be mildly raised, whilst cell count is normal (or slightly raised in flares) o Note: CSF examination is no longer required given the availability of imaging to diagnose Multiple Sclerosis There are a range of differential diagnoses for MS including other autoimmune diseases, spinal cord compression / syndromes, retinopathies, etc. o Furthermore, the primary differential diagnosis for unidentified white matter lesions on an MRI are vascular causes (e.g. microvascular ischaemic change) o It is common for misdiagnosis of white matter lesions to occur, so typically look for consistent clinical signs too prior to diagnosing patient with MS Describe genetic and environmental factors associated with MS and its risk factors - Genetic risk factors associated with MS include presence of the HLA-DRB1*1501 allele 107 o - Given Monozygotic Twins have a 30% probability of contracting Multiple Sclerosis, whilst Dizygotic Twins have a 5% probability of contracting Multiple Sclerosis, this suggests other genetic association with MS (although there is still a significant environmental component) Environmental risk factors associated with MS include living further away from the equator o It is believed this may be due to differences in sunlight exposure and hence Vitamin D levels Describe principles of management of a patient with MS, including types of treatment and targets, management of acute attacks and disease modifying agents - A range of effective treatments (both oral and intravenous) have been developed in the past 20 years (e.g. Interferon Beta-1B, Mitoxantrone, etc.) o These new drugs are effective in inflammatory Relapsing Remitting MS, and will reduce frequency and disability from relapse (and hence progression of disease) o However, these drugs do NOT have any effect on neuronal loss, and hence are ineffective for Progressive MS The classes of treatments available include: o Injectables Interferon-Beta-1B (which reduces synthesis of pro-inflammatory cytokines, increases synthesis of anti-inflammatory cytokine and inhibits T-Cell attack of neurons) Glatiramer Acetate (mechanism of action is unknown) o Oral Teriflunomide (which inhibits the synthesis of proliferating lymphocytes by inhibiting the enzyme DHODH needed for de novo synthesis of Pyrimidine) Fingolimod (which prevents release of T-Cells from Lymph Nodes by downregulating S1PR1 receptors on T-Cells in Lymph Nodes) Dimethyl Fumarate (which reduces inflammation by activating the Nrf2 antioxidant pathway) o IV Therapies Natalizumab (which prevents T-Cells crossing the Blood-Brain-Barrier) Alemtuzamab (which depletes T-Cells and B-Cells by binding to CD52 on their surface) Note: These IV therapies are highly efficacious, but have greater risks of side-effects Teriflunomide has a ~33% relative reduction in Relapse Rate compared to Placebo o Hence, the benefit from this drug is similar to those of the older-style injectable drugs (but not as effective as the latest / newer oral therapies) o Adverse side-effects include nausea, vomiting, liver dysfunction and teratogenicity Regular monitoring via blood tests are required for patients on this drug to ensure liver function is not compromised Fingolimod has a ~50% relative reduction in Relapse rate compared to Interferon-Beta or Placebo o However, adverse side-effects include affects to cardiac tissue (potentially resulting in a Bradyarrhythmia) and the endothelial cells of the Retina (potentially resulting in Macular Oedema) Dimethyl Fumarate (i.e. BG-12) has a ~50% relative reduction in Relapse rate compared to Placebo o Side-effects include flushing, GIT issues (e.g. diarrhoea, nausea, abdominal pain), Progressive Multifocal Leukoencephalopathy (PML) (which occurs due to opportunistic CNS infection by the JC Virus) Natalizumab is highly effective will result in a significant reduction in relapse rates (~70%) and disability progression (~40%) o However, continued treatment of the drug is necessary or relapses may recommence! o This drug proved that stopping T-Cells from entering the CNS will stop acute inflammatory disease However, this drug is not effective is stopping / preventing progressive MS (i.e. neurodegeneration) o However, the prevention of T-Cells from entering the CNS increases the risk of CNS infections / disease such as PML (via JC Virus) - - - - - 108 - - There is a limited amount of time this drug can be used before the risk of PML increases to an unacceptable level (and hence this will only temporarily delay MS) Alemtuzumab is a powerful lymphocyte depleting therapy (that works by binding onto CD-52 molecule on lymphocyte) that will be effective within 5 days of treatment commencement The latest therapies for Multiple Sclerosis all have an immunosuppressive mechanism of action (compared to the older Injectables which did not have immunosuppressive mechanisms of action) o As a result, patients on the newer therapies can be predisposed / at-risk of opportunistic infections (e.g. HSV) Immunoablative therapies are also possible and will offer a prolonged benefit (although NOT a cure), but with a substantial up-front risk of infection New avenues for research into MS treatments include understanding how to promote remyelination o Remyelination will occur in early disease, but this process will fail with ongoing / progression of disease o It is believed remyelination eventually fails due to Oligodendrocyte Progenitor Cells failing to differentiate into Myelinating Oligodendrocytes o Animal models have shown that that treatments that support differentiation of Oligodendrocytes (e.g. Anti-LINGO-1) will promote remyelination STRUCTURE AND FUNCTI ON OF PERIPHERAL NER VES – COMMON NEUROPATHIES Identify the structure and function of peripheral nerves - Function of the Peripheral Nerve will depend on the type of Peripheral Nerve o Motor nerves innervate skeletal muscles and are necessary for conscious control of muscle o Sensory nerves receive sensory input from the periphery and transmit it to centrally for recognition Structure of peripheral nerves will be different between Motor and Sensory Nerves o Motor Peripheral Nerves will have their cell body in the Anterior Horn of the Spinal Cord and emerge from the Spinal Cord via the Ventral Roots Motor Nerves will have a motor end plate at the neuromuscular junction, which is where / how the motor nerve will innervate the skeletal muscle o Sensory Peripheral Nerves will have their cell body in the Dorsal Root Ganglion outside the Spinal Cord and emerge from the Spinal Cord via the Dorsal Roots There are mechanoreceptors located at the end of Sensory Nerves that detect the different sensations (e.g. Pacinian Corpuscle detects vibration and pressure) o Note: Both motor and sensory peripheral nerves themselves will be myelinated (by Schwann Cells), with repeated Nodes of Ranvier along the nerve Myelin consists of layers of compressed Schwann Cell plasma membrane o Each Schwann Cell will only myelinate one axonal segment from one axon o In contrast, Oligodendrocytes (CNS version of Schwann Cells) will myelinate ~20-30 axonal segments from multiple axons o Note: Myelination will enable more rapid movement of signals through the axon There are three layers of connective tissue within each peripheral nerve o Endoneurium will surround individual axons and is the innermost layer o Perineurium surrounds each individual nerve fascicle and is the middle layer o Epineurium surrounds multiple fascicles (i.e. to form the peripheral nerve) and is the outermost layer Axonal Regrowth refers to a cut / damaged axon attempting to grow back o In peripheral nerves this usually implies growth close to the original course o Note: Axonal Regrowth is not as effective as the original Axon, as the series of small growth cones (that cluster together) are not as effective as a single larger Axon Nerves / motor neurons will aim to reinnervate muscles that no longer have any nerve supply o Therefore, when the loss of nerve supply is due to loss of motor neurons, the remaining motor neurons will take over the nerve supply to all the tissue - - - - - 109 o o o This will enable a relatively good recovery of gross motor function following loss of motor neurons, although the movement will be more clumsy (due to the loss of individual motor neurons) Furthermore, the electrical signal from the remaining motor neurons will become less reliable given higher firing due to the greater workload As a result, motor nerves are typically resistant to damage (due to compensatory effect) and hence symptoms only appear late In contrast, sensory nerves are less resistant to damage (adjacent sensory nerves do not reinnervate the same area), so symptoms appear early / immediately following damage Describe common pathologies and clinical manifestations of common peripheral neuropathies (axonal and demylinating) - Neuropathies can be classified accordingly to: o Modality (i.e. motor vs. sensory vs. sensorimotor) o Site of Pathology (i.e. axonal vs. demyelinating) o Mechanism of Pathology (i.e. diabetic, inflammatory, toxic, hereditary, deficiency) o Fibre size (i.e. large vs. small) Diabetic neuropathy is the most common neuropathy (given the widespread prevalence of Diabetes and Obesity) and will affect ~50% of diabetic patients o This can involve a peripheral sensory neuropathy, autonomic neuropathy and / or focal neuropathy (i.e. due to local entrapment or radiculoplexopathy) Deficiency neuropathies can occur due to deficiencies of: o Vitamin B12 (e.g. due to Pernicious Anaemia) – this is important for neuronal metabolism, and can result in both axonal loss and demyelination o Vitamin B1 / Thiamine (e.g. due to excess alcohol) – this will cause a distal small fibre neuropathy (i.e. sensory > motor) Hereditary motor and sensory neuropathies tend to be length dependent and involve Demyelination (e.g. Charcot-Marie-Tooth Disease) Inflammatory neuropathies can include: o Guillain-Barre Syndrome / AIDP – this can result in loss of reflexes and / or paralysis / weakness Weakness is typically ascending in nature and may peak after days to weeks, and is followed by spontaneous improvement o Chronic Inflammatory Demylinating Polyneuropathy (CIDP) – this involves a fluctuating course and a sub-acute onset of weakness o Vasculitic Neuropathy – this occurs due to occlusion of blood vessels by inflammatory processes, resulting in several infarcts and a Mononeuritis Multiplex Axonal neuropathies tend to be length dependent and more commonly affect small fibres o Causes include diabetes, vitamin deficiencies, inherited disorders, toxins, etc.) Clinical differentiation of Axonal vs. Demylinating Peripheral Neuropathies can be quite difficult o However, widespread reflex loss (especially in muscles groups without wasting / weakness) is more of a feature of Demyelination o In contrast, stocking sensory loss and selective loss of ankle jerk reflexes in the presence of distal wasting is more typical of Axonal Loss o Note: Nerve Conduction Studies are the best method for differentiating between Axonal vs. Demyelinating Peripheral Neuropathies - - - - MOBILITY MATTERS TO T-CELLS – HOW T-CELLS MOVE AND CAUSE DISEASE Identify and describe the key steps involved in the trafficking of naïve and newly activated effector and memory T cells into and away from secondary lymphoid tissues - Naive T-Cells and B-Cells have not interacted with their specific antigen yet and so will recirculate through the blood and peripheral lymphoid organs 110 o - - - However, upon activation with the specific antigen, these mature T-Cells and B-Cells will no longer remain within the peripheral lymphoid organs but instead home towards the site of the antigens (i.e. site of infection) Naive T-Cells express specific homing receptors that result in them being attracted to lymph nodes o Naive T-Cell express the receptors L-Selectin and CCR7, which will bind to a L-Selectin Ligand and CCR7 Chemokine respectively expressed within the High Endothelial Venules of the Lymph Node o This enables the T-Cells to enter the Lymph Node tissue to inspect the APC’s present for whether their relevant antigen is present Naive T-Cells will shift out of the lymph nodes when they commence re-expressing Sphingosine 1 Phosphate Receptor 1 (S1PR1) o Newly arriving T-Cells will express low levels of S1PR1 because engagement in blood with S1P leads to S1PR1 internalisation This means they are unable to respond to the high levels of S1P (lipid chemoattractant) in the medullary sinus, efferent lymphatics and blood Note: S1P gradient is maintained / created due to the presence of S1P lyase (i.e. degrading enzyme) throughout tissues o If Naive T-Cells do NOT engage with their cognate antigen after several hours, they will reexpress S1PR1 on their surface This will result in the Naive T-Cells responding to the S1P gradient and exiting the lymph node (as this is where there are high levels of S1P) o Note: This time taken to re-express S1PR1 gives the T-Cell sufficient time within the Lymph Node to inspect the APC’s present for whether their relevant antigen is present However, if the relevant antigen is not present, the T-Cell will leave the lymph node and recirculate through the blood to other lymph nodes Activated T-Cells down-regulate their L-Selectin and CCR7 Receptors resulting in the Activated T-Cell no longer being attracted to the HEV of Lymph Nodes (and hence will no longer recirculate through the Lymph Nodes) o This allows these activated Effector T-Cells to move towards the periphery (where there is infection / inflammation) o Furthermore, there is upregulation of different receptors that result in the Activated T-Cells being attracted towards the sites of infection / inflammation in the periphery (which express chemokines / cytokines that attract Activated T-Cells) Activated T-Cells increase their expression of S1PR1, E-Selectin Ligands, P-Selectin Ligands, CCR6, CXCR3, LFA-1 and VLA-4 These receptors / adhesions molecules will result in the Activated T-Cell being attracted to the periphery (where there are high levels of S1P), where there will bind to the Endothelial Cells of inflamed tissue (which express E-Selectin, P-Selectin, ICAM-1/VCAM-1, etc.) Chemokines / cytokines released from local inflammatory cells will result in the nearby Endothelial tissue expressing various ligands / chemokines that attract / bind to passing Activated T-Cells o Alternatively, Activated T-Cells may travel to B-Cell Follicles to activate the B-Cells and promote the generation of antibodies from the B-Cells Appreciate the importance of chemokine receptors and adhesion molecules in the navigation of T cells around the body particularly: o CCR6, CCR7, CXCR3 and CXCR5 o Selectins, LFA-1 and VLA-4 - CCR7 and L-Selectin Receptors are expressed on Naive T-Cells, and will direct these T-Cells towards the Lymph Nodes (which expresses L-Selectin Ligand and CCR7 chemokine) E-Selectin and P-Selectin Ligands are expressed on Activated T-Cells and will bind to E-Selectin and PSelectin expressed on Endothelium o This will result in the Activated T-Cells slowing down / ‘rolling’ across the Endothelium o Note: TNF-Alpha and IL-1 released from local inflammatory cells results in nearby endothelial tissue expressing E-Selectin and P-Selectin - 111 - - - CXCR3 is expressed on Activated T-Cells and will bind to chemokines such as CXCL10 released from the Endothelium o This will result in the activation of the Integrins (i.e. LFA-1, VLA-4) and chemotacic migration o Note: Interferon-Gamma released from local inflammatory cells results in nearby endothelial tissue releasing CXCL10 LFA-1 and VLA-4 are Integrins expressed on Activated T-Cells that bind to LIgands (i.e. ICAM-1/VCAM1) on the Endothelium in the Periphery o This results in the stable arrest of the T-Cell on the Endothelium, and its extravasation from the blood into the inflamed tissue o Note: Chemokines released from local inflammatory cells result in increased affinity of T-Cell Integrins (e.g. LFA-1, VLA-4) to their Ligands on the Endothelium (e.g. ICAM-1/VCAM-1) CXCR5 is expressed on Memory T-Cells and is believed to direct them towards B-Cell Follicles to provide help to mature / activate B-Cells (and hence produce antibodies) CCR6 is expressed by Effector Memory T-Cells and is believed to regulate the migration / recruitment of these T-cells to sites of inflammation Realise that by understanding how T cells “find their way”, new immunotherapies can and have been developed to target these processes, particularly: o Fingolimod to target S1P receptors o Natalizumab to target VLA-4 - Fingolimod has the effect of downregulating the expression of S1PR1 receptors by Activated T-Cells o These T-Cells will not be able to respond to the high levels of S1P in efferent lymphatic vessels o As a result, the T-Cells will remain in the lymph node and NOT enter the peripheral circulation (thus suppressing their immune action) o Fingolimod will in particular prevent Th17 Central Memory T-Cells from leaving the lymph nodes and entering the blood (where it can then enter the CNS and result in damage for patients with MS) Fingolimod is a very effective treatment for Multiple Sclerosis compared to Placebo or Interferon-Beta o Note: This mechanism of action applies to ALL T-Cells (and not only the Encephalitogenic TCells) and hence can cause adverse side-effects due this powerful widespread immunosuppressive effect o Note: Despite being a S1PR1 Agonist, Fingolimod is NOT degraded by S1P lyases Natalizumab is a monoclonal antibody that binds specifically to VLA-4 o This prevents VLA-4 from binding to ICAM-1/VCAM-1 on the Endothelium, and hence prevents the Activated T-Cell from crossing the endothelium into the tissue o Similarly, T-Cells bound by Natalizumab cannot cross the Blood-Brain-Barrier to attach myelin in Multiple Sclerosis Note: The mechanism of action for Fingolimod and Natalizumab applies to ALL T-Cells (and not only the Encephalitogenic T-Cells) and hence can cause adverse side-effects due this powerful widespread immunosuppressive effect - - SEMINARS NEUROTRAUMA Relate the macroscopic and microscopic pathology of neurotrauma to its clinical features, complications and outcomes - Different types of Neurotrauma include: o Primary Focal Injury (i.e. Blood Vessels) Contusions Haematomas (i.e. intracerebral, sub-arachnoid, sub-dural, epidural) Lacerations (of brain surface) 112 - - - - - - - - o Primary Diffuse Injury (i.e. Axons) o Progressive Damage (e.g. Free Radicals / Inflammation, Calcium Influx) o Additional Injury (e.g. Hypoxia, Swelling) o Functional Damage Damage to the brain from trauma will be at the point of primary impact (i.e. Coup) and point of secondary impact (i.e. Contrecoup) o Secondary impact refers to movement of the brain in the skull after the initial trauma resulting in damage to the brain on the opposite side of the trauma >20mm of blood in the brain are referred to as a Haemorrhage, and this can be fatal! (due to increased intracranial pressure) o In contrast, a Contusion involves an area of blood <20mm, and this is typically not an urgent problem No matter at which point of the head the trauma is incurred, there is a stereotypical pattern of damage / contusions to the brain at the bottom of the brain (particularly at the Frontal Lobe) on the skull o This occurs as the brain will shake in the skull irrespective of the precise location of the trauma o As the skull is ridged at the bottom, the bottom / undersurface of the brain (particularly at the Frontal Lobe) will incur damage / contusions Yellow colour on surface of brain relates to the Haemosiderin from blood (which indicates prior history of contusions / damage to the brain) o This is common in post-mortems of alcoholics and epilepsy patients (as these people are likely to have regular / repeated falls) o This scarring may result in seizures in the brain Epidural / Extradural Haemorrhage will result in an egg-shaped appearance of blood on CT Scan o In contrast, Sub-Dural Haemorrhage will result in a crescent-shaped appearance of blood on CT Scan Fracture to the skull can be very dangerous as these patients may have a ‘Delayed Haemorrhage’ (i.e. small bleed which progresses to a large bleed in the brain) The thinnest bone in the head is posterolateral to the ‘temple’ of the head o The Middle Meningeal Artery (which arise from the External Carotid Artery) is directly behind this bone o Hence, trauma at this location can result in the rupture of this Artery (resulting in an Extradural Haemorrhage) o The Extradural Haemorrhage will shift the brain away from the haemorrhage in the skull (which will compress the brain against the skull, resulting in death) Subdural Haemorrhage will results in Oedema in the brain (which can shift the brain away from the oedema in the skull [which will compress the brain against the skull, resulting in death]) o Causes of Subdural Haemorrhage involve rapid angular acceleration of the brain; this may be due to Motor Vehicle Accidents, Punches, Falls, etc. o Chronic Subdural Haemorrhages are possible too due to repeated bleeding and then healing of the venous rupture Healing of bleed with involve the formation of Fibrous Tissue This will require the formation of new capillaries towards the site of the bleed However, these capillaries could re-bleed, resulting in a cycle of bleeding and healing Note: The brain will NOT be shifted to one side in the event of Chronic Subdural Haemorrhage (given the slow onset, progressive nature of the pathology) Diffuse Axonal Injury (DAI) is commonly caused by rotational forces within brain, which result in shearing injuries to axons Diffuse head injuries will not be visible macroscopically, but instead can only be identified microscopically (e.g. under silver stain or via Beta-Amyloid Precursor Protein) o Axons will be transacted, resulting in swelling of the distal part of the Axon (i.e. at the point of the transection) (as there is no pathway for the neurotransmitters from the Axon) o Diffuse Axonal injuries are usually more severe in the midline of the brain (as the direction of the Axons are in the opposite direction [i.e. shearing effect] from the two sides of the brain) 113 o - Diffuse Axonal injuries are likely to occur from traumas that result in the head moving from side-to-side o More severe Axonal injuries will result in greater bleeding that can be observed macroscopically (i.e. haemorrhage into Lateral Brainstem or Corpus Callosum) o Severe Axonal injuries will result in shrinking of the brain Traumatic Brain Injury will trigger the release of Glutamate from nerve endings, which result in the excess entry of Ca2+ in the post-synapse, which then triggers excitotoxicity to the tissue LIVING WITH DISABILI TY – PAIN Differentiate between acute and chronic pain and the implications for management - Acute pain will expire in the short-term in contrast to chronic pain, which will persist (potentially lifelong) o There is no cure for Chronic Pain, so the only realistic option in managing this chronic pain Management options should account for the lifelong nature of care needed, and so strong, addictive painkillers (e.g. Opioids) used for Acute Pain should be avoided! o This is important as Chronic Pain is the source of significant disability, and is also associated with depression / poorer quality of life Recognise the roles of personal and environmental contributors to the impact of persisting pain, their identification and management options - Perception of pain and disability will depend on a range of personal and environmental factors such as: o Social pressures (e.g. financial difficulties, loss of job, etc.) o Prior treatment failures o Unhelpful thoughts / beliefs o Level of activity o Note: These above factors will affect how someone responds to the pain and hence their quality of life As a result, the preferred management approach for Chronic Pain needs to involve a multifactorial approach that considered these different factors o Improving on these other areas will place the person in a more positive frame of mind / approach to life that will result in the perception of less pain Community beliefs about pain will need to be changed, such that people understand that being active despite pain is preferable (rather than ceasing activity if there is pain) o This will enable management of the various personal / environmental factors that result in the perception of pain / disability - - Understand the major ethical issues associate with pain and its management - Key ethical issues can include: o Right for Pain Relief Patients may demand strong pain-killers in the short-term to relieve excessive pain, even if this provides no long-term benefit Should doctors provide such treatment to provide acute relief or withhold such medications in the hope of implementing long-term improvements (e.g. exercise) o Clinician’s Beliefs Recommendations to chronic pain sufferers seem to reflect persona attitudes of doctor rather than evidence (e.g. ‘be careful’, ‘let pain be your guide’) Doctors need to avoid these biases and be more evidence-based o Access to Opportunities Some people may not have an occupation that will allow them to adjust their role to their chronic pain 114 This lack of opportunity may result in them losing their job, becoming more isolated and have greater disability / perception of pain MALFORMATIONS IN THE NERVOUS SYSTEM TBD – new in 2015 - Malformations of the Nervous System are the second most common malformations in babies (after cardiac malformations) o Many of the malformation of the Central Nervous System is due to problems with Neuronal Migration (i.e. migration from the Ventricular Zone towards the Mantle Zone / Cortex) The earlier in development a malformation occurs, the more severe the morphologic and functional phenotype o It is the timing of the malformation, rather than the size of the insult that will impact the severity of the morphologic and functional phenotype Brain weight and body height are closely related (i.e. taller people have heavier brains) Distinction between Grey and White Matter is difficult to identify in a babies brain, as the White Matter is underdeveloped (e.g. lack of myelination) o Full myelination may only be achieved by the age of early 20’s There is a less Gyri (and hence less surface area of the Brain) in the Premature Baby Brain o There will be increased Gyration over the 9 months of pregnancy o Gyration should generally be completed by the end of the 9 months of pregnancy o Note: The weight of the brain and the number / level of Gyration can be used to accurately estimate the age of the foetus Premature babies commonly will have haemorrhages in the Brain near / or within the Ventricles o There is increased risk of haemorrhages due to the respiratory distress occurring in Premature babies (which results in fluctuations of Blood Pressure) o The Germinal Matrix (which contains the Neuroblasts) is located adjacent to the Ventricles, and can be affected by such haemorrhages Babies / young children have bigger heads relative to size of their bodies (compared to Adults) Ultrasounds can be used to investigate the brain of a baby (as the Fontanelle provides an opening to view the brain) Anencephaly and Spina Bifida typically occur separately (rather than both occurring at the same time) as there are different signalling pathways associated with the closure of the Rostral Neuropore vs. closure of the Caudal Neuropore o Folic Acid Supplementation during early pregnancy (i.e. within the first 4 weeks prior to Neurulation) will reduce the likelihood of Anencephaly and Spina Bifida Frontal Encephalus involves the brain bulging out the front of the face Holoprosencephaly (i.e. failure of the Forebrain to split into two hemispheres) is commonly associated with a congenital lack of smell sense (as the Olfactory Bulb does NOT develop) - - - - - - COMMUNITY IMPACT OF SPINAL CORD INJURY Describe specialist contributions of health professionals other than doctors in the management of patients with spinal cord injury (e.g. specialist nurses, psychologists, physiotherapists, occupational therapists and social workers) - A range of different health professionals are involved in the management of spinal cord injury patients o Specialist Nurses are important for providing the specific care needed for SCI patients (e.g. bladder care, bowel care, skin care, etc.) o Psychologists are critical to help patients adapt / respond to their new and very different life, as well as dealing with the depression that can affect SCI patients o Physiotherapists will assist in rehabilitation of SCI injury patients and maximising their movement 115 o - Occupational Therapists will assist in adapting the home / occupational environment to make it easier for the SCI patient to live and work o Social Workers will connect SCI patients to the various services specifically available for them, and will help them adapt to their new situation There is a ~3-4x more people with Nontraumatic SCI compared to Traumatic SCI, although the effects of the SCI are the same regardless of the cause Severity of SCI is communicated via the ASIA (American Spinal Injury Association) Classification (i.e. A, B, C, D, E) CEREBROVASCULAR DISE ASE TBD – new in 2015 - Occulomotor Nerve will travel between the Posterior Cerebral Artery and Superior Cerebellar Artery o This junction is a common site of a Berry Aneurysm (which can thus result in an Occulomotor Palsy) Circle of Willis provides collateral blood supply to the brain (in the event that one of the key arteries are blocked / occluded) o This is particularly important for neonates / babies as the movement of their head is such that Vertebral Artery is commonly compressed / occluded The most common cause of Stroke is an occlusion at the beginning of the Internal Carotid Artery (which is outside the brain!) o This can result in a blockage of the Anterior System (i.e. Anterior Cerebral Artery and Middle Cerebral Artery) o Middle Cerebral Artery blockage is more common than Anterior Cerebral Artery (as the Anterior Cerebral Artery commonly receives collateral blood supply via the Anterior Communicating Artery) It is uncommon for an Atherosclerotic Plaque to completely stenose / occlude an artery o Instead, a thrombus is more likely to form on the Plaque, and it is this thrombus that occludes the artery Infarct will initially result in an increase in the size of the infarcted tissue due to swelling o Therefore, infarcts adjacent to the Brainstem are very dangerous as the increase in size can place pressure on the Brainstem resulting in significant adverse effects (e.g. death!) o The infarcted tissue will eventually decrease in size as the swelling decreases Coagulative Necrosis will occur following ischemia / infarction o The architecture of the dead tissue is preserved for at least a couple of days (as the lysosomal enzymes are denatured and hence proteolysis is blocked) o This tissue will eventually develop in Liquefactive Necrosis, and leave behind a cavity (which is surrounded by Glial tissue that will wall-off this cavity) The timing of the infarcts can be estimated by the nature of cells in the histological section (e.g. neutrophils immediately following the infarct, macrophages a week after the infarct, etc.) Shrunken ‘red neurons’ are red due to the loss of nucleic acid in their cytoplasm o These neurons can still live if oxygen perfusion is returned to these neurons soon Blood flow (rather than oxygen) is the critical need for the brain o This is why compressions (rather than breaths) are more important in CPR! Haemorrhagic infarcts can result following the breakdown of an embolus o The blood vessels downstream from the occluding embolus will be damaged by the occlusion (as the blood vessels themselves undergo ischaemia and will become prone to rupture) o Reperfusion of these downstream vessels following breakdown of the embolus can result in rupture of these downstream vessels (as the higher pressure blood can cause a rupture of these weakened vessels) Fat emboli can result from a fracture (as the fat is released from the bone marrow), which can then travel to the brain and result in a stroke Superficial haemorrhages occur due to blockage of the superficial venous system o This type of haemorrhage is likelier is dehydrated babies and pregnant women - - - - - - - 116 - Amyloid deposits on blood vessels will weaken blood vessels and increase the likelihood of rupture (and hence haemorrhage!) CASE CONFERENCE – CLINICAL DISORDERS OF THE AUT ONOMIC NERVOUS SYSTEM Describe the main clinical disorders associated with dysfunction of the autonomic nervous system - Drooping of eyelid can result from lesion in CNIII (Occulomotor) and / or limitations of the Sympathetic Nerve innervation (e.g. due to Horner’s Syndrome) o Limitations of the Sympathetic Nerve innervation will only result in a partial droop (NOT a complete droop) but will also result in pupil constriction Patient with neck pain and Horner’s Syndrome may have a Carotid Artery dissection (as the Sympathetic Chain will travel within the Carotid Sheath) ‘Seizure at horror movie’ may actually be Vasovagal Syncope, whilst ‘light-headedness with exercise’ may be pre-syncope due to insufficient sympathetic stimulation to cope with the higher oxygen demands Cardio-inhibitory / Vaso-Vagal syncope (i.e. loss of sympathetic tone) is the most common cause of syncope o This may appear like convulsions / seizure during this syncope, so it’s important to take an accurate history and conduct the appropriate tests to be able to identify the precise cause of the collapse Neurally Mediated Syncope (NMS) (e.g. Vaso-Vagal) can be diagnosed using comprehensive history and examination, Electrophysiology studies or the ‘Tilt Test’ o Tilt test involves placing a patient on a flat table with a foot support, then tilting the table upward for a period of time to observe changes in blood pressure and heart rate o Test will be positive if there is a drop in heart rate and / or blood pressure (which can result in light-headedness or loss of consciousness) ‘Marked face sweating’ can sometimes occur if this is the only area that is able to sweat (as the sympathetic innervation of the lower body is inhibited due to an autonomic neuropathy [e.g. triggered by Diabetes]) o Autonomic neuropathy can also result in Constipation, Reflux and Bloating after Meals (due to lack of Gastric emptying reflexes and GI motility reflexes) Clinical disorders resulting in autonomic neuropathy include: o Acute Acute Pandysautonomia Botulism Guillain-Barre Syndrome Porphyria Drugs and Toxins o Subacute Paraneoplastic Sjogren’s Syndrome Diabetes Drugs and Toxins o Chronic Amyloidosis Diabetes Chronic Pandysautonomia Sensory Neuropathy with Autonomic failure (e.g. Idiopathic, Sjogren’s, Paraneoplastic) Familial Dysautonomia Cholinergic or Adrenergic Multi-System Atrophy (MSA) (this presents with Central Autonomic Dysfunction and Parkinsonian features) - - - - - 117 - Pure Autonomic Failure (i.e. any primary autonomic failure without central nervous system findings) Small Fibre Neuropathy is a clinical disorder whereby there is constant burning sensation superficially on the soles of the feet, prickling / itching sensation, dull/deep aching pain in the feet, etc. o Small fibres are involved in pain and temperature sensation! CRANIAL NERVES – CLINICAL PERSPECTIVE II Describe the clinical examination of the cranial nerves and identify clinical features for specific cranial nerve lesions - Refer to notes for ‘Cranial Nerves – Clinical Perspective I’ lecture Peter Gate’s ‘Rule of 4’ (i.e. 4 rules of 4) is an easy way to remember / understand the location of the different brainstem structures (e.g. cranial nuclei, tracts, etc.) and the possible constellation of symptoms / deficits that can be occur from lesions in particular areas; the rules are: o Rule 1 – There are 4 structures in the ‘midline‘ beginning with M Motor Pathway (i.e. Corticospinal Tract) Motor Nuclei and Nerves (for CNIII, IV, VI and XII per below) Medial Lemniscus Medial Longitudinal Fasciculus o Rule 2 – There are 4 structures to the ‘side‘ (lateral) beginning with S Spinocerebellar Tract Spinothalamic Tract Sensory Nuclei of Trigeminal Nerve (CNV) Sympathetic Pathway o Rule 3 – There are 4 cranial nerves in the Medulla, 4 in the Pons and 4 above the Pons (2 in the Midbrain) Medulla = CNIX, X, XI and XII (i.e. Cranial Nerves 9-12) Pons = CNV, VI, VII and VIII (i.e. Cranial Nerves 5-8) Midbrain = CNIII and IV (i.e. Cranial Nerves 3-4) Above Midbrain = CNI and II (i.e. Cranial Nerves 1-2) o Rule 4 – The 4 motor nuclei that are in the midline are those that divide equally into 12 except for I and II, that is III, IV, VI and XII (whilst CNV, VII, VIII, IX, X and XI are in the lateral brainstem) o Note: Blood supply to the Midline Brainstem structures is via the Paramedian Branches (i.e. small penetrating branches off the Basilar Artery), whilst Lateral Brainstem structures are supplied via the Circumferential Branches (e.g. SCA, AICA, PICA) If there are signs of both a Median and Lateral Syndrome, then consider whether there is an occlusion within the Basilar Artery itself (as this would block the Paramedian AND Circumferential branches) Babies will have different, particular reflexes (i.e. primitive reflexes) compared to adults (e.g. Grasp Reflex) o If these primitive reflexes re-emerge later in life, this is a sign of an underlying pathology Upper Motor Neuron Lesions will have the following features: o Weakness in Group of Muscles o Hypertonia (i.e. Spasticity) o Hyperreflexia o No marked trophic changes or muscle wasting o No denervation Lower Motor Neuron Lesions will have the following features: o Weakness of Individual Muscles o Atonia o Areflexia o Pronounced muscle wasting and trophic changes o Fasciculations o Denervation - - - 118 SYSTEMATIC REVIEWS Outline differences between types of reviews - The different types of reviews include: o Systematic Reviews o Narrative Reviews o Meta-Analysis o Individual Patient Data Reviews o Overviews Narrative Review are a good place to start when learning about a topic; they are: o Broad in scope o Not necessarily comprehensive o Potentially biased o Qualitative in nature Systematic Review are not good for general summaries of clinical problems; they are: o Good place to look for specific clinical questions o Utilise comprehensive sources and explicit search strategies o Rigorous and evidence-based o Typically involve meta-analysis (quantitative) in addition to qualitative summary - - Describe the role of meta analysis, a forest plot and its components - Meta Analysis is a statistical technique for combining data from multiple similar studies into a quantitative summary statistic (a weighted average of the individual study effects). o This allows formal testing of whether there are between study effects (heterogeneity) and why they might exist o Key difference between Meta Analysis and Narrative Reviews is that a Meta Analysis is holistic and involves statistical analysis Forest Plot is a graphical display designed to illustrate the relative strength of treatment effects in multiple quantitative scientific studies addressing the same question Key components of Forest Plot include: o Squares- represent the study’s estimate o Square size corresponds to the study’s weight o Lines through the squares estimate the Confidence Interval o Vertical line is the “line of no effect” (no difference) o Diamond at the bottom represents the summary estimate o The tips of the diamond represent the CI of the summary estimate - List at least two reasons why we need systematic reviews - Systematic Reviews are useful as they: o Increase power to detect intervention effects (which can prevent delay in introducing effective treatments) o Explore between study differences (which can enable more tailored/ individualised therapy) o Summarise vast amount of medical literature Reproduce search techniques for Systematic Review - Comprehensive search strategy for Systematic Review will include: o Define the question: PICO (M) o Find all the literature that addresses that question o Extract the papers with appropriate study design o Pool the results (if appropriate, conduct meta-analysis) Perform a critical appraisal (with guidance) in Session 2 119 - Critical Appraisal of a Systematic Review will involve considering: o Was there a well formulated question? (i.e. PICOT) o Was there appropriate inclusion and exclusion criteria? o Was the literature search comprehensive? o Was the validity of the studies included appraised appropriately? o Is there heterogeneity of results? If so, has this been explored / explained? Understand the following concepts and their effects on validity of a Systematic Review - publication bias and heterogeneity - Publication Bias refers to bias towards publishing only significant results and not publishing nonsignificant results (this tends to bias towards suggesting an intervention is significant when it truly is not significant) o This means that the Systematic Review literature search may not include the results of all research conducted, and hence any analysis / interpretation will be misleading (generally towards suggesting a statistically significant difference when there actually is no statistically significant difference) Heterogeneity refers to differences in results across different trials (this may indicate differences in samples, intervention (e.g. dosage), measurements, timeframes, etc.) o Tests for heterogeneity (e.g. Ch squared, F-test) have low power, so whilst a positive test will indicate heterogeneity, a negative test cannot be interpreted as being due to a lack of heterogeneity as it may be due to the lack of power in the test o Significant heterogeneity will make it difficult to conduct statistical analysis (i.e. metaanalysis) on these studies given the wide differences - NEUROINFECTION Describe the major clinical and pathophysiological features of CNS infections with an emphasis on meningitis, encephalitis and CNS abscess - There are two key dimensions for considering how / why a person contracts a neuroinfection o Nature of the organism o Nature of the patient (e.g. immunosuppressed, genetically susceptible, etc.) The three major neuroinfection patterns are: o Meningitis o Encephalitis o Focal Infections (e.g. Abscess) o Note: Understanding the particular pattern of neuroinfection will assist in identifying the underlying cause (as only particular organisms can cause each of the three neuroinfection patterns) Acute Pyogenic Meningitis will involve purulent exudates forming in the Sub-Arachnoid space o Depending on the causative organism, the exudates will either form on the base or the top of the brain o CSF will also be cloudy in the event of Acute Pyogenic Meningitis, but will be clear in the event of Aseptic (i.e. Viral) Meningitis Complications of Meningitis is the formation of fibrous tissue in the Sub-Arachnoid space that blocks / restricts the Foramen of Magendie and Foramina of Luschka (which results in Hydrocephalus) o Blockage of the Sub-Arachnoid space can also occlude blood vessels in the region resulting in Stroke o Blockage of the Sub-Arachnoid space can also compress Cranial Nerve through this area (e.g. deafness is a common complication of Meningitis) Patients with Mumps and Measles commonly will also contract Aseptic (i.e. Viral) Meningitis Chronic Meningitis may result from Tuberculosis, whereby the granulomas in the brain burst resulting in the Meningitis Gardeners can commonly contract Cryptococcus Fungal infections (as pigeon faeces contains Cryptococcus), which can result in a Fungal Meningoencephalitis - - - - 120 - - - Encephalitis will typically target particular cells in the CNS (i.e. Neuron vs. Microglia vs. Oligodendrocytes, etc.) Herpes Simplex Encephalitis commonly will attack / destroy (via necrosis) the Medial Temporal Lobe bilaterally o Treatment should be IMMEDIATELY provided with Acyclovir o Earlier treatment will minimise damage to the brain (and hence minimise the long-term deficit) Cytomegalovirus will result in infected cells significantly increasing in size o This virus will affect both the Nucleus and the Cytoplasm of the cell HIV Encephalitis will involve the formation of multinucleated giant cells Antibodies against NMDA Receptors can result in an ‘Anti-NMDA Receptor Encephalitis’ o Therefore, not all Encephalitis will result due to an infection! Presence of ‘Negri bodies’ in the Hippocampus or Cerebellum is pathognomonic for Rabies Amoeba can potentially enter the CNS and cause Cerebral Amebiasis (i.e. a form of meningoencephalitis) Cerebral Malaria will result in congestion of the small blood vessels of the brain o This can be visualised via Fundoscopy, as the small vessels of the Retina will be congested The presence of Eosinophils in the brain during Meningitis / Encephalitis suggests a parasitic cause of the disease (e.g. Malaria, Hyatid Cysts, etc.) Brain Abscess will have a well-demarcated border with a firm, fibrous border / capsule (as the body attempts to wall off the abscess) o The abscess will have the four layers of Pus, Macrophages, Granulation Tissue and Reactive Glia Sub-Dural Empyema can result from a parasinal infection spreading posteriorly into the Sub-Dural Space o These can be difficult to identify on a CT Scan! (it is much easier to identify on a MRI Scan) Describes the routes and barriers to infection within the CNS - Infections of the brain are uncommon due to the presence of a Blood-Brain Barrier and the different physical layers protecting the CNS (e.g. Dura Mater) o However, Haematogenous spread is still the most common cause of neuroinfections (though this requires overcoming the Blood-Brain Barrier [e.g. via use of transporters]) o Other routes from which an infection can spread to the CNS include from: Contiguous / adjacent areas (e.g. Paranasal Sinuses, Middle Ear, etc.) PNS towards the CNS (e.g. Herpes Zoster) Direct trauma / entry of the infection into the CNS CASE CONFERENCE – STROKE Describe the clinical signs and symptoms associated with stroke - - Clinical signs and symptoms include: o Facial weakness o Arm / leg weakness (typically hemiparesis) o Speech difficulty Change in side of hemiparesis (e.g. left to right) suggests an occlusion of the Basilar Artery Describe management principles of stroke - Early management of stroke can have a great influence on brain survival and outcome (Time = Brain!) o Aim to reestablish perfusion as soon as possible via thrombolysis for ischaemic stroke However, do NOT administer Thrombolysis after ~4.5 hours as there is a heightened risk that re-entry of blood to the ischemic area after this time may result in a haemorrhage that will cause additional damage to the brain 121 o - - - Study has shown patients who receive clot retrieval AND Thrombolysis have superior reperfusion and outcomes compared to patients who receive Thrombolysis only Other management principles in the acute-stroke setting include: o Prevent hyperglycaemia (as associated with poor outcomes) o Lower temperature (as high temperature associated with poor outcomes) o Do NOT reduce blood pressure after ischaemic stroke (unless it reaches dangerous levels) as this will reduce brain perfusion In contrast, if there is a haemorrhagic stroke, aim to reduce systolic BP < 160mmHg, as this will minimise the risk of re-bleeding o Review swallowing status and prevent aspiration o Review / prevent DVT and bed sores from lack of movement Patients may develop epilepsy / seizure activity following a Stroke (due to the interference with the brain neural activity) o As such, these patients may require treatment with Anti-Epileptic Drugs Prevention of stroke will involve treatment of CVD risk factors (e.g. hypertension, smoking, dyslipidaemia, diabetes, etc.), reduction of any heavy alcohol intake, usage of Statins (unless there is history of haemorrhage), usage of Anti-Platelet agents, CASE CONFERENCE – EXERCISES IN CRITICAL THINKING AND DIAGN OSIS IN CLINICAL NEUROLOGY – PART I Complete exercises in critical thinking and diagnosis in clinical neurology - Occlusion of the Great Radicular Artery of Adamkiewicz will result in an Anterior Spinal Artery Syndrome o This is a longitudinal syndrome where there is an infarction extending longitudinally along the spinal cord o The clinical symptoms of this lesion will be aligned to a LMN lesion, with the lesion actually in the spinal cord (in the ventral 2/3 of the spinal cord, including the Ventral White Commissure) There will be a bilateral loss of motor function and pain / temperature sensation below the lesion Furthermore, there will loss of tone and reflexes below the lesion, without any Plantar responses (akin to LMN lesion) Note: This is different to Spinal Shock, as the reflexes will NOT return with time if the spinal cord has infracted ‘Watershed Regions’ are areas in the body that receive blood supply from the most distal branches of two large arteries, and are at particular risk of ischaemia during hypotension (as it is the regions farthest away from collateral bloody supply) o There are two key watershed regions within the Spinal Cord at the: Anterior Spinal Artery between T7 and T9 (i.e. location of Great Radicular Artery of Adamkiewicz); and Cervical / Upper Thoracic Region (T1 to T4) Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) can present at as a Mononeuritis Multiplex o This is believed to be an auto-immune disease whereby the immune cells incorrectly attack the nerves in the body. o As a result, the affected nerves fail to respond or respond only weakly to stimuli, causing numbing, tingling, pain, progressive muscle weakness, loss of deep tendon reflexes (areflexia), fatigue, and abnormal sensations Initial functional deficits will be asymmetric However, as the disease progresses, deficits becomes more confluent and symmetrical, making it difficult to differentiate from a polyneuropathy o The likelihood of progression of the disease is high (though it can vary between having chronic progression vs. a relapsing and remitting course) - - 122 o - CIDP can be treated effectively with Corticosteroids (unlike the Acute version of the disease [also known as Guillain-Barre Syndrome] where Corticosteroids will have a detrimental impact) Other treatment can include IVIG or Chemotherapy (both of which reduce the level of activity of the immune system, and hence reduce the level of immunopathology) Note: AIDP / Guillain-Barre Syndrome are often associated with URTI and diarrhoea / GIT issues (as well as preceding triggering infection) Multiple Sclerosis usually affects the CNS, so a neuropathy only affecting the PNS is unlikely to be Multiple Sclerosis Lead toxicity can lead to neuropathy, although the neuropathy will only affect motor function (and NOT sensory function) o Similarly, Inclusion Body Myositis (an inflammatory muscle wasting disease) will only affect motor function (and NOT sensory function) BRAIN TUMOURS Identify main features of brain tumours including clinical presentation and diagnosis - Brain Tumours are different from other tumours as they have a greater propensity to progress to more malignant, higher grade tumours over time (rather than remaining stable at the same grade) o Prognosis of tumour will depend on the grading of the tumour (i.e. level of differentiation of cells) Brain Tumours very rarely metastasise (although other tumours will commonly metastasise to the brain) Presence of a brain tumour one on side of the brain can shift the brain to the contralateral side as well as herniation downwards (i.e. coning!) o The brain tumour will also result in an increase in intracranial pressure Raised intracranial pressure due to brain tumours can result in headache, nausea, CNVI palsy, Papilloedema, Epilepsy, Coma and / or Homonymous Hemianopia MRI with Contrast will clearly identify the presence of a brain tumour o In contrast, a CT Scan without Contrast may not clearly identify the presence of brain tumour New blood vessels developed from brain tumours will initially NOT possess the tight junctions needed to maintain the blood-brain barrier o As a result, there may be oedema present surrounding the tumour o This oedema can be identified clearly using Gadolinium Contrast CT Scans (as Gadolinium does NOT normally cross the Blood-Brain-Barrier) - - Describe the main types of primary tumours and metastatic brain tumours - The type of brain tumour will vary depending on the particular location within the brain ~20% of childhood tumours are brain tumours (compared to ~1-2% of adult tumours being brain tumours) o ~70% of the childhood brain tumours will arise in the Posterior Fossa / near the Cerebellum, compared to only ~30% of adult brain tumours o Note: Posterior Fossa tumours will result in an earlier increase in intracranial pressure, which can trigger earlier vomiting This earlier generation of symptoms can result in the brain tumours being identified earlier (and hence treated when the tumour is smaller) Risk factors for brain tumour include age and exposure to radiation of the head (e.g. due to X-Ray or CT Scan) Brain cells that have higher turnover are more likely to develop into Brain Tumours o As a result, Microglia, Astrocyte, Ependyma and Oligodendrocyte Tumours are more common (i.e. Glioma, Glioblastoma, Astrocytoma, etc.) o In contrast, Neuronal Brain Tumours are uncommon - 123 - - - - - Astrocytomas and Oligodendrocytomas will progress relatively slowly and patients can survive for longer periods with this type of brain tumour o In contrast, Glioblastomas are much more dangerous and will result in death relatively sooner Different Glioblastomas can have different molecular pathways / mutations, which will have an impact in the future as the trend towards molecular-specific therapies continue Large Glioblastomas are likely to have spread beyond the obvious lesion throughout the cerebral cortex o As a result, excision of the Glioblastoma lesion will not be curative and instead only have the advantage of relieving intracranial pressure Meningiomas may have a ‘spiral-like’ appearance under the microscope o They will also be very evident in CT Scans with Contrast, as Meningiomas are supplied by the External Carotid Artery (which does not have a blood-brain barrier) and so the contrast will enter the Meningioma itself Acoustic Neuroma are common brain tumours that will result in progressive unilateral deafness o Note: These tumours are actually a Schwann Cell tumour from the Vestibular Nerve (rather than being a Neural tumour from the Cochlear Nerve as the name would have suggested) Secondary Metastases in the Brain will be visible as a circular tumour in the brain that commonly lodge in the junction between the Grey and White Matter o The prognosis for Secondary Metastases to the Brain is very poor! Describe the different types of brain swelling and the causes and consequences of elevated intracranial pressure - Cytotoxic Oedema involves an increase in the size of the cells (i.e. swelling of the cells), whilst Vasogenic Oedema involves opening of the blood-brain barrier resulting in water entering the cranium / brain o Oedema can also occur due to the failure of the Na+/K+ pumps, resulting in increased Na+ ion concentrations in the brain (which attracts additional water into the brain) Brain tumours will result in increased intracranial pressure due to: o The mass-occupying effect of the tumour o Venous congestion (which occurs due to the brain tumour) o Blockage of CSF outflow (resulting in hydrocephalus); and o Swelling of the Brain The brain is able to adapt to a small increase in cranium volume without an increase in intracranial pressure as the intracranial blood vessels will compress in response o However, there is a limit after which any further increases in cranium volume will result in exponential increases in intracranial pressure (as the brain is no longer able to adapt to the increases in volume) Elevated intracranial pressure will result in headache, nausea, CNVI palsy, Papilloedema, Epilepsy, Coma and / or Homonymous Hemianopia o Headache is worse in morning (due to lying supine through the night, which increases intracranial pressure) o Nausea occurs as there is pressure against the areas in the Brainstem that trigger nausea o Coma can occur as there is pressure against the areas in the Brainstem that are responsible for consciousness - - - IMPACT OF BLINDNESS Describe the effect of severe visual impairment on the activities and functional status of individuals and their families - ‘Low Vision’ is defined as vision < 6/18 in both eyes with corrected vision (i.e. after glasses) o Legal blindness is defined as vision < 6/60 in both eyes with corrected vision (i.e. after glasses) Severe visual impairment will affect the opportunities and choices available to people - 124 - o They will not be able to drive if their vision (with correction) is <6/12 in NSW o There will be limitation to the future career choices available People with severe visual impairment will require significant support from their families in their dayto-day life o This can potentially cause problems in family dynamics if there is one person for whom so much care is dedicated (as other people may feel left out) Describe impact of blindness - Discrimination and prejudice against visually impaired people is unfortunately extremely common o Visually impaired people are not given the same opportunities and suffer from the bigotry of low expectations o Whilst the presence of anti-discrimination laws has reduced some of the discrimination, visually impaired people are still discriminated against Technological advancements has significantly increased the opportunities available for visually impaired people Visually impaired / blind people have the same intellectual / cognitive ability as other people o However, other people will commonly treat visually impaired / blind people differently upon finding out about their disability (despite them having the same intellectual / cognitive ability) o It is important to treat visually impaired / blind people as normal people, rather than acting condescendingly - Describe services available to help people of all ages who have visual disability - There are a range of services available via Low Vision Australia for the visually impaired, including: o Clinic-based low vision services (e.g. Optometrist, Orthoptist, Occupational Therapist) o Children’s Services o Orientation and Mobility (e.g. visual scanning techniques, training in mobility aids, etc.) o Employment (e.g. job finding, workplace modification) o Adaptive Technology and Training (e.g. large print and speech in computers) o National Information and Library (i.e. information that can be read / listened by the visually impaired) o Equipment Solution (i.e. sell and demonstrate equipment, trial equipment) o Deaf-Blind Services (e.g. Braille education, individual assessment / advice) o Recreation and Support (e.g. adaptive activities [e.g. Blind Cricket], community social groups, etc.) These services will assist visually impaired people to optimise their independence and quality of life Low Vision Aids are also available to correct / improve visual loss / deficit o Magnification is usually employed to assist these vision problems o Most devices are supplied for near tasks or stationary distance requirements o Telescopes and Binoculars can be employed for distance vision. o Consumer devices such as iPads and iPhones are useful Low Vision Aids o Note: It is important to review the use of the devices provided 2-3 months after supply to ensure the device is working as intended and there is no misunderstanding on how to use the device - Describe means by which to involve family, the community and agencies for the blind and government agencies in the process of rehabilitation of children blind from birth or an adult blind patient - Children’s Services from Low Vision Australia provides training and resources for families to help children, from birth to school leaving age, who are blind or vision impaired o They develop programs that are tailored to individual needs to facilitate each child's development, access to education and independence 125 o - They offer advice on a range of aspects including daily living skills such as dressing and eating with cutlery o They assist teachers in the students school to ensure they have access to the curriculum o They offer programs in adaptive technology and independence skills Low Vision Australia also run a range of other programs that can assist the rehabilitation of adult blind patients Describe the effects of visual impairment on quality of life - Poor vision will inhibit / prevent healthy ageing and increase the risk of falls, hip fracture and depression Visual impairment will impact upon quality of life through the limitation of career opportunities and the increased challenges of social interaction Remember the importance of treating the patient rather than just the disease!!! o Visually impaired / blind people may suffer from depression / mental health issues following their diagnosis of vision impairment, so it’s critical to treat these mental health issues o Even after adapting to their vision impairment, these patients may go through peaks and troughs in their mood due to the loss of vision impairment, so it is important to continually focus on the person’s mental well-being - Interview a visually impaired patient in order to understand coping mechanisms and skills needed by those with visual impairment and their families - Blind / visually-impaired patients are commonly highly sensitive to glare, which is why these people typically wear dark-glasses at all times Visually impaired patient suffer significant discrimination, which can adversely affect their mental health o It is important that appropriate mental health care and support is provided for these patients as they overcome these challenges - CASE CONFERENCE – EXERCISES IN CRITICAL THINKING AND DIAGN OSIS IN CLINICAL NEUROLOGY – PART II Complete exercises in critical thinking and diagnosis in clinical neurology - An increasing proportion of Strokes in the past ~50 years are due to Ischaemic Strokes (compared to Haemorrhagic Strokes) due to changes of lifestyle factors and treatment options for hypertension o Treatment of hypertension has reduced the incidence of haemorrhagic strokes o Increased cholesterol intake increases risk of Ischaemic Stroke - - CASE I Movement of eyeball laterally, but not upwards or medially suggest a lesion of the Occulomotor Nerve (CNIII) o Loss of light reflex directly or consensually for one eye will also indicate a lesion of the Occulomotor Nerve (CNIII) Ptosis can be caused by loss of innervation of the Levator Palpebral Superior (via the Occulomotor Nerve [CNIII]) o Partial Ptosis can also occur due to loss of sympathetic innervation of the eye (which will also result in constriction of the Pupil) o Other possible causes of Ptosis include: Myaesthenia Gravis (such that Ptosis will worse at the end of the day due to fatigability of the Levator Palpebral Superior) Mitochondrial Myopathies (congenitally inherited) Trauma Senility (the Ptosis will be so severe that it can result in functional blindness) 126 - - - - - - - - - Congenital Ptosis Pupil dilation can occur due to loss of Parasympathetic Innervation of the Sphincter Pupillae o This can occur due to a lesion along the nerve path (Occulomotor Nerve [CNIII]) or at the relevant nucleus in the brainstem (Edinger-Westphal Nucleus) Lower facial muscle paralysis (excluding forehead) occurs due to an Upper Motor Neuron lesion of the Facial Nerve (CNVII) o There is no forehead / upper facial muscle paralysis from an Upper Motor Neuron lesion of the Facial Nerve (CNVII) as there is bilateral innervation of the forehead / upper facial muscles o Alternatively, another mechanism may be there are multiple higher motor centres innervating the upper facial muscles, so the lesion of one motor centre (or pathway from this centre) will not result in total loss of upper facial muscles Right Upper and Lower Limb Paralysis can occur due to a lesion of the Left Corticospinal Tract above the Pyramids (i.e. before it has crossed) o This lesion is likely NOT in the Cortex if there is ipsilateral (rather than contralateral) lesion of the eye o Instead, the lesion is likely near the Midbrain given the potential lesion of the EdingerWestphal Nucleus (which is in the Midbrain) Normal Sensory Examination indicates there is no lesion of the posterolateral regions of the Brainstem (which is the location of the Sensory Nuclei within the Brainstem) Lesions in the CNS may appear like a Peripheral Lesions if there is damage to the axons from the CNS Nuclei (rather than damage to the nuclei itself) o For example, damage to the Axons of the Occulomotor Nerve (CNIII) The lesion for this patient is likely in the Left Cerebral Peduncle in the Midbrain (given the presence of the Left Corticospinal Tract damage above the Pyramids [resulting in Right Upper and Lower Limb weakness and Right Lower Facial Muscle Weakness] and Left Occulomotor Nerve lesion) o This is called Weber’s Syndrome, which occurs due to occlusion of the Midbrain Paramedian Branches of the Basilar Artery The pattern of Head and Neck involvement on one side of the body and Upper / Lower Limb involvement on the other side of the body can ONLY occur due to a lesion in the Brainstem o In contrast, lesion in the Cortex will result in unilateral signs / symptoms on the contralateral side of the body CASE II Impairment of light touch, pinprick, joint position and vibration on the left side of the face and body suggests a lesion above the Brainstem (i.e. Thalamus or Cortex) o Unlikely to have a pathology that only affects all the nociceptors, muscle spindles or peripheral nerves on one side of the body o Not possible to have spinal cord lesion (as will affect contralateral pain and temperature, and will NOT affect facial sensation) o Facial weakness of the same side of the body as lower / upper limb weakness suggest the lesion is above the Brainstem Left-sided weakness (including upper and lower limb weakness), mild weakness of the left lower face and slurred speech suggest a lesion above the Brainstem (i.e. Thalamus or Cortex) o Unlikely to have a pathology that only affects all the muscles or peripheral nerves on one side of the body o Not possible to have spinal cord lesion (as will NOT affect facial sensation) Lesion of the Internal Capsule is likely to cause the above mild contralateral motor and sensory weakness (as this region of the brain is packed with both motor and sensory nerve fibres) o This may occur due to occlusion of the blood supply to this area (via a haemorrhage or thrombus) (i.e. Lenticulostriate Arteries) o The presence of a normal CT Scan of the Brain ~4 days after the onset of symptoms suggests this is NOT a haemorrhage or tumour (as this would be easily visible on a CT Scan), but rather than infarction (as CT Scans have a low sensitivity to detect infarctions) 127 o - - - - Note: These deficits are unlikely to be caused by a Middle Cerebral Artery Stroke, as a stroke that affects such large areas of the Cortex would produce much more severe deficits (rather than only mild weakness) CASE III Homonymous Left Superior Quadrantanopia will occur due to a lesion in the Right Temporal Lobe (i.e. Meyer’s Loop) or further posterior in the Visual Cortex o The Right Temporal Lobe / Meyer’s Loop will be supplied by the Right Middle Cerebral Artery, whilst the Visual Cortex (i.e. Occipital Lobe) will be supplied by the Right Posterior Cerebral Artery Right Arm and Face weakness suggest a lesion in the lateral Left Primary Motor Cortex (i.e. PreCentral Gyrus) o This region of the brain is supplied by the Left Middle Cerebral Artery and / or Left Posterior Cerebral Artery o Furthermore, difficulty speaking suggests a lesion in Broca’s Region (i.e. anterior to the Primary Motor Cortex at the Inferior Frontal Gyrus) o Therefore, the lesion is likely to located in the Cortex at the Left Frontal Lobe Note: If there was no speech symptoms, this lesion may have been located in the Internal Capsule or further down the descending Corticospinal Tract Right Homonymous Hemianopia and Profound Amnesia suggest a lesion of the Left Temporal Lobe and the Hippocampus o This region of the brain is supplied by the Middle Cerebral Artery and Posterior Cerebral Artery respectively This patient is likely to have Infective Endocarditis (as they recently had a dental extraction and a history of rheumatic fever) resulting in a series of microemboli in the brain causing multiple lesions DEMYELINATING DISEASES Describe the main features of demyelinating disorders (both central [primary and secondary demyelination] and peripheral) - Myelin Disorders can be classified according to: o Primary Demyelination – this refers to attack of the Myelin initially, followed subsequently by attack of the Axon o Secondary Demyelination – this refers to the destruction of the Axon followed by the macrophages consuming the leftover myelin o Note: Dysmyelination refers to abnormal formation of Myelin Multiple Sclerosis is an autoimmune disease of the CNS resulting in the destruction of myelin o There is a clinical threshold below which inflammation / MS lesions can occur without causing clinical signs / symptoms Axonal damage may be ongoing / continuing throughout this period even if there are no clinical signs / symptoms o Common symptoms of MS include blurred vision (due to Optic Neuritis), diplopia, numbness, ataxia (due to Cerebellar lesions) and UTIs (due to the need of urinary catheters) Lhermitte’s Sign (i.e. electric sensation that runs down the back and limbs that is elicited by neck flexion) and Uthoff’s Sign (i.e. increased severity of symptoms in heat) are very suggestive of Multiple Sclerosis o MRI Scan can identify both new, acute lesions as well as older lesions of MS This is useful for the diagnosis of Multiple Sclerosis, as it can show separate lesions separated by time ( as well as separated by space) o Oligoclonal Bands in the CSF indicate the presence of IgG in the CSF (which occurs due to the Multiple Sclerosis) Multiple Sclerosis lesions commonly occur in the Paraventricular regions, Grey Matter / White Matter Junction, Optic Chiasm, Brain Stem and Spinal Cord o These lesions will appear macroscopically as well-defined, grey, firm plaques in white matter - - 128 o - - - - - - - - Note: Lesions to the Brainstem are visible on the outside, as the White Matter is located on the outside of the Brainstem (rather than being within the Brainstem) MS may be identifiable microscopically by the presence of significant quantities of lymphocytes surrounding the blood vessel (which suggests the presence of immune system pathology of MS) o Other microscopic features include presence of ‘punched out’ lesions around small veins, myelin debris in macrophages and disappearance of Oligodendrocytes Initially, MS will mainly result in the loss of myelin with the relative maintenance / retention of Axons o However, Axonal Loss will eventually also occur in MS, as the Axons cannot survive in the long-term without the Myelin Sheath o There is a high incidence of acute axonal loss in lesions during active myelin destruction, and a low level of continuous axonal loss in chronic plaques There appears to be some genetic risk associated with MS, although this is polygenetic as no single gene has been found to be associated with MS Environmental risk factors for MS include: o Vitamin D deficiency o Epstein Barr Virus (EBV) (as may mimick myelin proteins) o Smoking o Obesity o Excess sodium intake (per mouse studies) Study showed Retina attracted inflammatory cells despite the lack of myelin in the Retina o This suggest the inflammation is NOT triggered by the Myelin Sheath o Instead, Endothelial injury may be the primary event triggered inflammatory cell entry There may be more than one antigen relevant in MS that triggers and perpetuates the inflammatory process o However, the antigen that initiates the inflammation may be different to the antigen that perpetuates the inflammation o Possible antigens include myelin-basic protein, myelin-associated glycoprotein, EBV, Herpes Virus Type 6, etc. Remyelination can occur initially in MS from Oligodendrocyte Precusor Cells o However, this remylination cannot compensate / counter all the myelin damage inflicted, resulting in progressive loss of myelin o Research into future treatments for MS include considering how to stimulate this remyelination process There are several alternatives proposed to the autoimmune hypothesis of MS such as: o Apoptosis Pathway – Apoptosis of Oligodendrocytes has been seen in fresh MS lesions (rather than inflammation) , which may suggest a different signalling pathway o Locus Coeruleus Hypothesis – this suggested that these neurons absorbed toxicants from the bloodstream and consequently reduce the level of Noradrenaline released Noradrenaline is an anti-inflammatory agent, so this uptake of toxicants may result in the increased inflammation in Multiple Sclerosis o Venous Outflow Impairment – Latest view is that this theory is incorrect and that venous outflow impairment does NOT cause Multiple Sclerosis Other Demyelination disorders include: o Central Pontine Myelinolysis This Demyelination of the Pons may occur following rapid changes in Na+ levels This can affect the myelin is other parts of the body in addition to the Pons Common trigger for this condition is rapid correction of hyponatremia (i.e. infusion of Na+ following hyponatremia) o Acute Disseminated Encephalomyelitis (ADEM) This is a rare autoimmune disease that cause causes destruction of Myelin Common triggers include vaccination or viral infection This condition usually occurs in children and is marked by high fever o Neuromyelitis Optica This is an inflammatory disorder that will involve demyelination over long segments of the Optic Nerve and Spinal Cord This occurs due to a circulating antibody to Aquaporin 4 (AQP4) 129 The Aquaporin 4 receptors on Astrocytes are attacked by these antibodies, which result in death of these Astrocytes Death of the Astrocytes will result in the death of Oligodendrocytes (which rely on the Astrocytes for survival), which then results in the destruction of Myelin MUSCLE WEAKNESS Describe major diseases that cause muscles weakness, their mechanisms and clinical features - Secondary tumours are extremely rare in muscles (despite the significant vascular supply to muscles) Motor Neuron / Nerve will determine the type of the Muscle Fibre that it innervates (i.e. Type 1 / slow vs. Type 2 / fast) Type 1 / Slow Muscle Fibres require oxygen for metabolism (i.e. aerobic) whilst Type 2 / Fast Muscle Fibres do not require oxygen for metabolism (i.e. anaerobic) o Type 1 Fibres are slow-twitch fibres, red in colour and consists of fats o Type 2 / Fast Muscle Fibres will be lost following disuse (e.g. bed-ridden patient) Proximal Weakness typically results from a muscle disease, whilst Distal Weakness typically results from a nerve disease (i.e. neuropathy) Muscle diseases are typically progressive / insidious in onset, but can be detected via the Creatine Kinase investigation / test o Muscle Disease will generally involve abnormal levels of Creatine Kinase o Muscle Disease can also be identified via Nerve Conduction Studies (which can be used to distinguish between a nerve or muscle problem) o Muscle Biopsy is another technique that can be used to identify the presence of muscle disease Diabetes and alcohol consumption commonly will result in Peripheral Neuropathies Loss / destruction of motor neuron may result in the remaining adjacent motor neurons innervating the muscle fibres originally innervated by the destroyed motor neuron o However, the precision of movement on the re-innervated muscle fibre will be lower (i.e. clumsier movement) Myaesthenia Gravis is a disease of the neuromuscular junction that involves a reduction in the density of Acetylcholine Receptors on the Post-Synaptic Membrane (as the Acetylcholine Receptors are broken down by autoantibodies) o Lambert-Eaton Myaesthenic Syndrome (LEMS) is another neuromuscular junction disease that involves autoantibodies against the voltage-gated Ca2+ channels on the pre-synaptic membrane, and is common in cancer patients (i.e. this is usually a paraneoplastic process) Duchenne Muscular Dystrophy is a progressive disorder with genetic inheritance (X-linked) that involves abnormal Dystrophin Protein o Dystrophin Protein connects the cytoskeleton of muscle fibre to the surrounding extracellular matrix through the cell membrane o Histology will involve the replacement of muscle fibres with fat and connective tissue, as well as an increase in the size of remaining muscle fibres (i.e. hypertrophy) o Note: Whilst this disease commonly affects males, it theoretically can also affect females too (if both X chromosomes have the relevant mutation) Necrosis of muscle fibre and invasion of the muscle fibre by macrophages will occur in Polymyositis o This is characterised by symmetric proximal muscle involvement o Treatment with Corticosteroids will commonly cure the symptoms of Polymyositis Dermatomyositis will be a autoimmune disorder that will affect the skin and muscle o Peripheral Muscle Fibres of the Fascicle will atrophy (i.e. Perifascicular), whilst Central Muscle Fibres of the Fascicle will remain normal o There is commonly a reddish / purplish rash of the upper eyelids associated with periorbital oedema, and typically affects the proximal muscles initially o ~20-25% of patients with Dermatomyositis have an underlying cancer Inclusion Body Myositis is a progressive disease commonly affecting flexors of upper limbs and extensors of lower limbs - - - - - - - - 130 o - - - - Histology will reveal the presence of vacuoles (i.e. empty, bubble-like spaces) and clumps of cellular materials (inclusion bodies) within muscle fibres o Cholesterol lowering agents (e.g. Stains) are believed to trigger this disease in some people Macrophagic Myofasciitis may be triggered by the Aluminium contained within Vaccines (and will be localised to the site of vaccination) o There will be sheets of macrophages in striated muscle and inconspicuous muscle fibre damage (due to the presence of aluminium) o This disease can initially appear like Polymyositis under histology and can commonly be misdiagnosed Mitochondrial Myopathies will involve abnormal mitochondria and commonly can be inherited from the person’s mother (i.e. maternal inheritance) o Cholesterol lowering agents (e.g. Stains) are also believed to trigger this disease in some people McArdle Disease is a metabolic disorder (more specifically a glycogen storage disease) caused by deficiency of Myophosphorylase and will commonly result in significant exercise intolerance with muscle pain, early fatigue and myoglobin in the urine (due to muscle breakdown) Binge drinking of alcohol may produce ‘Alcohol Myopathy, which is an acute toxic syndrome of Rhabdomyolysis (i.e. breakdown of muscle tissue that leads to the release of muscle fibre contents into the blood) with accompanying myoglobinuria, which may lead to renal failure CASE CONFERENCE – EXERCISES IN CRITICAL THINKING AND DIAGN OSIS IN CLINICAL NEUROLOGY – PART III - - - - - Complete exercises in critical thinking and diagnosis in clinical neurology CASE I Facial Nerve (CNVII) Palsy will NOT cause Ptosis (as these patients cannot close their eyes, rather than their eyelids) Diplopia that cannot be explained via Cranial Nerve palsy / Cranial Nuclei lesion may be due to one of the ‘3T’s’: o Thyroid Disease o Thiamine Deficiency o Tensilon Test (i.e. Myaesthenia Gravis indicated by use of Tensilon [short-term Acetylcholinesterase Inhibitor]) Cover Tests will enable determination of which eye is resulting in a diplopia o Covering the affected eye will result in the peripheral / outer-most image (i.e. false image) disappearing o Typically, the direction where the diplopia is more severe is the direction in which one of the eyes are having problems moving If the patient has a diplopia when they look to the right and cover tests suggest the right eye did not move fully, this suggests a problem with the Right Lateral Rectus Muscle (which is innervated by Abducens Nerve [CNVI]) o Weakness of eye closure suggests a lesion / problem with the Facial Nerve (CNVII) o Left Ptosis without Meiosis suggests a lesion of the Occulomotor Nerve (CNIII) The widespread involvement of multiple cranial nerves is unlikely unless there is a widespread intracranial infection (e.g. Chronic Meningitis [due to TB, Cryptococcus, Carcinoma]) o However, such infections are likely to result in systemic symptoms too Lack of sensory abnormalities indicate either a process that will never affect sensation (e.g. myopathy, neuromuscular junction problem), or alternatively will affect sensation in the near-future Myaesthenia Gravis is an autoimmune disease where autoantibodies will block Acetylcholine Receptors on the post-synaptic membrane o This will inhibit receipt of Acetylcholine at the post-synaptic membrane, resulting in failure of the post-synaptic muscle from contracting (i.e. muscle weakness) o This is likely to exhibit as affecting multiple different muscles rather than a single muscle only 131 o - - - - - - - - Treatment can involve inhibition of the Acetylcholinesterase, which results in an increase in Acetylcholine in the Synaptic Cleft (which increases the likelihood of Acetylcholine interacting with the post-synaptic membrane) o Other treatments that are also possible are a Thymectomy (if these patients also have an enlarged Thymus) Ocular Myaesthenia Gravis is more common / visible given the fine control needed for the eye muscles compared to other muscles (and so slight changes to the Neuromuscular Junction in the Ocular Muscles will be more sensitive) o Therefore, Myaesthenia Gravis disease is more manifest in the eyes compared to the rest of the body Hallmark of Myaesthenia Gravis is fatigability (i.e. worsening muscle weakness following repeated activity o As a result, symptoms are commonly worse later in the day compared to the morning o This occurs as repeated activity will consume the Acetylcholine in the Synaptic Cleft, thus increasing the severity of the blockage of the Acetylcholine Receptors (as there is a lack of Acetylcholine to bind to the remaining Acetylcholine Receptors) Investigations used to assess Myaesthenia Gravis include autoantibody assay, Jitter test and Nerve Conduction Studies CASE II Patients with Parkinson’s Disease have a life expectancy of ~20 years post-diagnosis Utilisation behaviour involves patients grabbing objects in view and starting the 'appropriate' behaviour associated with it at an 'inappropriate' time o Utilisation behaviour patients have difficulty resisting the impulse to operate or manipulate objects which are in their visual field and within reach Grasp, Palmomental, Pout and Rooting Reflexes and Upgoing Plantar responses are Primitive Reflexes Pre-Frontal Lobe is associated with influence over expression, perseverance and distractibility o This area of the brain will typically inhibit Primitive Reflexes too (so a lesion in this area will result in presence of Primitive Reflexes) o Damage to this area of the brain will also result in Utilisation behaviours Remember to provide a clinical vignette / history when requesting an investigation! o This will assist the Radiologist is identifying the required area to focus upon (and prevent unnecessary imaging /investigations) Parkinson’s Disease will generally involve the triad of Tremor, Rigidity and Bradykinesia o The absence of one of these signs is a red-flag that the underlying condition is actually NOT Parkinson’s Disease o Failure to respond to Parkinson’s Disease therapy within ~3 months is another red-flag to suggest that the underlying condition is actually NOT Parkinson’s Disease Parkinson’s Disease will also typically be asymmetric rather than being symmetric Parkinson’s Disease patients typically do NOT have abnormal brain imaging Slowly-developing Hydrocephalus may result in signs / symptoms of Parkinson’s Disease o Therefore, Frontal Meningioma resulting a slowly-developing Hydrocephalus may initially exhibit as a patient with Parkinson’s Disease, but then will deteriorate further due to increased damage to the Pre-Frontal Lobe CLINICAL PATHOLOGY OF MOVEMENT DISORDERS Recognise and describe the phenomenology associated with Movement Disorders including tics, tremor, parkinsonism, chorea, ataxia and dystonia - ‘Movement Disorders’ is an extremely broad term referring to a range of underlying conditions o Many movement disorders will also involve other non-movement symptoms (e.g. cognitive changes / decline) Key terminology to understand in the context of Movement Disorders are: o Ballistic Chorea – this refers to fast, rapid, ‘flinging’ movements o Athetosis Chorea – this refers to slower, writhing movements - 132 o o o o o o o o o o o Tremor – this is characterised by involuntary, alternating movements in a predictable, rhythmic manner (i.e. same frequency and same amplitude) Dyskinesia – this refers to involuntary muscle movements Bradykinesia – this refers to slow movements Akinesia – this refers to loss of movement Ataxia – this refers to lack of voluntary coordination of muscle movements Tic – this refers to a sudden, single movement that is repetitive / stereotyped (i.e. predictable) This may be triggered / elicited by increasing stress This can be voluntarily suppressed for a short period, but this voluntary suppression will make patients uncomfortable Dystonia – this refers to sustained, involuntary co-contractions of antagonist muscles causing twisting and repetitive movements / postures This can sometimes be relieved via a sensory trick referred to as ‘Geste Antagoniste’ This involves a physical gesture (such as touching your chin) which may serve to temporarily interrupt dystonic symptoms Examples of Dystonia include Torticollis, Writer’s Cramp, etc. Note: Repetitive actions are more likely to be associated with Dystonia (e.g. Writer’s Cramp, Musician’s Cramp) Rigidity – this refers to constant increased muscle tone Spasticity – this refers to increased muscle tone following increased velocity of the muscle Intention Tremor – this refers to tremor when approaching the endpoint of a deliberate and visually guided movement Dysdiadokinesia – this refers to impairment of the ability to perform rapid, alternating movements Understanding of the common patterns of diseases, their symptoms, diagnosis and management - Parkinson’s Disease arising from a mutation of a single gene (e.g. AR/AD PARK 1-12) is rare (<5% of patients) and more likely to have an atypical presentation (e.g. younger onset, strong family history, etc.) Motor symptoms of Parkinson’s Disease can be treated with Dopamine replacement / stimulation o However, the non-motor symptoms (e.g. dementia, falls, hallucinations) are not reduced by Dopamine replacement / stimulation o Furthermore, the underlying progression of Parkinson’s Disease will continue irrespective of Dopaminergic Neurons Pathology of Parkinson’s Disease will commence in the Caudal Brainstem and progress rostrally over time o This may explain why constipation and poor mood may be a precursor to the diagnosis of Parkinson’s Disease (which generally occurs upon motor symptoms), as these functions are controlled in the Caudal Brainstem o Progression to the Midbrain (i.e. Substantia Nigra / Dopaminergic Neurons) will trigger the motor symptoms of Parkinson’s Disease o Further progression to the Cortex will trigger the non-motor symptoms (e.g. dementia, hallucinations) of Parkinson’s Disease Parkinson’s Disease may result in the loss of paralysis during REM Sleep, resulting in acting out dreams o This ‘acting out’ during REM Sleep will occur during synucleinopathies (e.g. Parkinson’s Disease, Lewy Body Dementia, Multi-System Atrophy) o Note: Patients presenting with ‘Acting Out’ of REM Sleep only have an 80% probability of developing Parkinson’s Disease in the next ~15 years Parkinson’s Disease patients will have a Resting Tremor that will disappear on conscious action o In contrast, Essential Tremor will not be present at rest, but will appear upon conscious action o Essential Tremor is a condition that commonly occurs either due to genetic inheritance and is more likely to affect adolescents / younger people - - - - 133 - - - - ~50% of Essential Tremor patients will have a reduction in tremor following alcohol consumption L-Dopa (i.e. Levodopa) is taken up by Dopaminergic Neurons, within which it is converted to Dopamine o The Dopamine produced is stored in vesicles and then secreted from the pre-synaptic membrane o As Parkinson’s Disease progresses, the number of Dopaminergic Neurons decrease resulting in insufficient Dopamine production (resulting in ‘OFF’ phenomenon / akinesia) Furthermore, more of the L-Dopa is now absorbed by Serotonergic Neurons, which convert L-Dopa to Dopamine However, these Serotonergic Neurons do not store Dopamine in vesicles and instead releases the Dopamine immediately This results in a wave of excessive Dopamine, which can trigger Dyskinesia Note: The net effect of the loss of Dopaminergic Neurons is to narrow the therapeutic window for L-Dopa The loss of Dopaminergic Neurons (and hence the narrowing of the Therapeutic Window) is not related to the length of Levodopa therapy but rather the duration of the Parkinson’s Disease (and so there is no benefit from delaying therapy with Levodopa) Anti-psychotics may result in the appearance of Parkinsonian features (given anti-psychotics may be Dopamine antagonists) Multi System Atrophy (MSA) is a Parkinsonian Syndrome that involves abnormal depositions of Alphasynuclein throughout the Brainstem and / or Basal Ganglia o This condition is associated with REM Sleep Disorders, Autonomic Dysfunction, difficulties swallowing, difficulty breathing and Cerebellar deficits (e.g. ataxia, short-shuffling gait, dysarthria, etc.) o Axial T2 Hypersensitivity MRI of the Pons will indicate a ‘Hot-Cross Bun’ sign (i.e. there is a cross on axial images through the Pons, representing selective degeneration of the Pontocerebellar Tracts) Progressive Supra-nuclear Palsy (PSP) is a Parkinsonian Syndrome that may involve lack of pursuit eye movements and Parkinsonian Signs (e.g. short shuffling gait, lack of arm swing, lack of facial expression) o These patients though will have Vestibular-Ocular Eye Movements present (which indicates nerves and muscles to eyes must be working effectively) o This condition is a Diffuse Tauopathy throughout the Brainstem, Striatum, Cerebellum and / or Cortex o Axial MRI will indicate the ‘Mickey Mouse’ sign (i.e. Cerebral Peduncles and Midbrain are shaped like Mickey Mouse’s head and ears) this occurs due to selective atrophy of the Midbrain Tegmentum, with relative sparing of the Midbrain Tectum and Cerebral Peduncles o Mid-Sagittal MRI of the Brainstem will indicate the ‘Hummingbird’ sign (i.e. Pons is the breast of the Hummingbird, Midbrain is the Head of the Hummingbird and with a beak extending anteriorly towards the Optic Chiasm) this occurs due to selective atrophy of the Midbrain Tegmentum o Note: These patients do NOT have a REM Sleep Disorders or Hallucinations (in contrast to MSA and Parkinson’s Disease Presence of Neuropsychiatric and Parkinsonian symptoms may suggest Wilson’s Disease o This autosomal recessive disease affects younger people (<20 years) and involves excessive deposition of Copper in the Brain and Liver o This disease can be treated /cured if diagnosed early (via copper chelation and / or liver transplant), so it’s critical to be able to diagnose this condition before it’s too late! o Axial MRI of Midbrain will indicate the ‘Panda Sign’ (i.e. Red Nucleus are the Eyes, Substantia Nigra the Ears and Superior Colliculus the Nose of the Panda) COMMUNITY IMPACT OF NEURODEGENERATIVE DI SEASE IN THE ELDERLY 134 Describe effects of neurodegenerative disorders at a population level, using Parkinson's Disease and Alzheimer's Diseases as the principal examples - Neurodegenerative Diseases are progressive diseases resulting in nervous system dysfunction The increasing prevalence of these disease poses a significant financial burden on society o Estimated total financial cost (including lost productivity) of PD was $775million in 2011 ~42% of main carers of Dementia patients are spouses / partners, whilst ~44% of main carers are children of Dementia patients o ~40% of Family Carers of Dementia patients become depressed, particularly during the last few months of the life of the Dementia patient o This is significantly higher than the rates of depression for Family Carers of patients with other illnesses (e.g. cancer) o This may be due to the prolonged nature of care for Dementia (given the progressive nature of the disease) as well as the distress / difficulty of caring for a Dementia patient (e.g. compared to a cognitively able cancer patient) o Note: There is an expected shortage of ~150,000 carers by 2029 for Dementia patients - Describe the increasing prevalence of neurodegenerative diseases in an ageing population and their increasingly prominent role in the community and the health care system - Prevalence on neurodegenerative disease increased with increasing age (~780/100,000 people >55 for PD and ~1,800/100,000 for Dementia) o >80% of people with PD are >65 years of age o Increased ageing of population is expected to result in a significant increase in the prevalence of these neurodegenerative diseases Incidence of neurodegenerative disease showed significant correlation with each other neurodegenerative diseases and strokes Given median time from onset to death of ~12.2 years in PD and between ~3-7 years for Dementia, the number of people living with PD and Dementia is rapidly increasing o This has societal and health care system implications given these people may become highneed patients (e.g. higher health care costs, greater need for assisted living, greater need for carers, etc.) - Describe treatment developments in neurodegenerative disorders from a patient's perspective, and contrast this with research evidence supporting those treatments - There is no cure or disease modifying treatment for neurodegenerative disease, so treatment is focused on symptom control / relief o Levodopa (i.e. Dopamine precursor) remains the most effective treatment for PD o However, long-term Levodopa is associated with adverse side-effects such as dyskinesia and ‘wearing off’ phenomenon o Alternatively, Dopamine Agonists can be used, but these have a different set of side-effects (e.g. hypotension, nausea, vomiting, hallucination) Management for neurodegenerative diseases needs to be individualised due to the variability of symptoms o Aim to reduce stress levels, as this intensified symptoms and counteracts the benefits of medications o Remember to consider and treat depression and anxiety, as these are common mood disorders in patients with neurodegenerative diseases - Describe difficulties in diagnosing Parkinson’s disease (PD) - No antemortem diagnostic test is available for Parkinson’s Disease o Diagnosis is performed based on clinical features, but this cannot be confirmed until the post-mortem 135 o Challenge with this approach is that diagnostic criteria / practices (i.e. at least two out of three of bradykinesia, resting tremor and rigidity) have changed over time, which makes comparison of diagnostic data over time difficult Describe dementia and list the diagnostic criteria for Alzheimer's Disease (AD) - Dementia is a progressive, irreversible syndrome of impaired memory, cognition / intellectual function, personality and behaviour resulting in significant impairment of function o This is the second leading cause of disease burden and the leading cause of disability in Australians >65 years There are a range of different causes of Dementia including: o Alzheimer’s Disease o Vascular Dementia o Frontotemporal Dementia o Dementia with Lewy Bodies o Mixed Dementia o Parkinson’s Disease with Dementia Diagnostic criteria for Dementia is that there is cognitive or behavioural symptoms that: o Interfere with the ability to function at work or usual activities o Represents a decline from previous level o Are not explained by Delirium or Major Psychiatric Disorder o Note: Cognitive and behavioural symptoms must involve at least 2 of the following domains Memory Reasoning Visuospatial abilities Language Behaviour / personality Diagnostic Criteria for Alzheimer’s Disease involves: o Meeting the criteria for Dementia o Insidious onset (months to years) o No prominent features of other types of Dementia o Most prominent and initial cognitive deficit is either: Memory (Amnestic Presentation) Language, Visuospatial, Executive Dysfunction (Non-Amnestic Presentation) - - - Describe risk factors and protective factors for AD - Risk factors for AD include: o Elderly age o Down Syndrome o Family History of AD o Genetic mutations (e.g. Apo E4 allele, PS1/PS2/APP gene mutations) o Smoking o Low Cognitive Activity o Low Physical Activity o Depression o Metabolic factors (Obesity, Hypertension, T2DM) Protective factors for AD include: o Physical exercise o Mental exercise o Strong social networks o Mediterranean diet plus curries - MOTOR NEURONE DISEASES 136 Describe the main clinical and pathophysiologic features of common neurodegenerative disorders, including motor neurone disease and Huntington's disease - Amyotrophic Lateral Sclerosis (ALS) is also known as Motor Neuron Disease (MND) o ALS is the common term used in the US, whilst MND is the common term used in Commonwealth countries Degeneration of the Upper Motor Neurons will result in degeneration of the Corticospinal Tract in the Spinal Cord (which is located in the posterolateral aspect of the Spinal Cord [and hence the term ALS]) ALS will involve degeneration of BOTH the Upper and Lower Motor Neurons (as well as the Bulbar Region) o It is unknown if there is a direction of the progression of disease (i.e. Upper to Lower vs. Lower to Upper vs. Neither) There has been recent speculation that ALS will progress from Upper Motor Neurons to Lower Motor Neurones o Degeneration of Lower Motor Neuron ONLY is referred to as ‘Progressive Muscular Atrophy’ o Degeneration of Upper Motor Neuron ONLY is referred to as ‘Primary Lateral Sclerosis’ Muscles will atrophy following death of their innervating Motor Neurons Ventral / Anterior Spinal Roots in ALS will become atrophied due to the loss of the Motor Neurons in the Spinal Cord o This is particularly evident when comparing the atrophied Ventral / Anterior Spinal Roots to the normal Dorsal / Posterior Spinal Roots Upper Motor Neurons (i.e. Betz Cells) will die during ALS, in addition to the Lower Motor Neurons in the Ventral Horn o Death of these cells will NOT trigger inflammation ALS has a relatively rapid progression, such that median survival is ~3 years from first symptoms There are multiple ‘ALS Mimic Syndromes’ that need to be differentiated / considered when making a diagnosis of ALS o The diagnosis of ALS can be a diagnosis of exclusion o Be very careful of the diagnosis of ALS, as this is effectively a ‘death sentence’ (vs. ALS Mimic Syndromes, which can be treated) Death from ALS commonly occurs from failure of Respiratory Muscles European populations appear to have a higher incidence / prevalence of ALS (although this may be due to more effective diagnostic procedures in European countries) TDP-43 is normally present in the Nucleus, but will leave the nucleus and enter the cytoplasm in patients with ALS o Patients with TDP-43 may be on a spectrum of disease spanning from ALS to Frontotemporal Lobar Degeneration (i.e. Frontotemporal Dementia) (or both conditions!) It is hypothesised that there is a genetic pre-disposition for ALS that will be triggered by cell damage with time and environmental exposures (e.g. infection, toxins, , pesticides, herbicides, diesel fumes, etc.) to ultimately cause the disease o Genetic mutations associated with ALS include mutations of the SOD1 genes and Oligogenic Genetic Disorder o Note: There appears to be increased expresses in polio virus receptor in patients with ALS, which may suggest there is an underlying viral cause of ALS! Retrograde transmission from the neuromuscular junction has been proposed as a means via which toxins are transported to the Motor Neurone resulting in death of the Motor Neurone o Genetic differences in dealing with toxins can result in increased susceptibility to these toxins (which increases the risk of ALS) There is some evidence that cell death in ALS and other neurodegenerative diseases occur due to excitotoxicity (resulting from excessive Glutamate synapsing at the post-synaptic receptors) o Alternatively, the presence of Tangled Proteins can interrupt the intracellular machinery resulting in cell death Kennedy Disease is another motor neuron disease that will involve fasciculation and atrophy of the tongue and gynaecomastia o This disease involves a Triplet-repeat disorder within the Androgen receptors - - - - - - - - - 137 - - Spinal Muscular Atrophy (also known as Werdnig-Hoffman Disease) is an autosomal recessive neurodegenerative disease affecting Lower Motor Neurons ONLY o This results from mutation from the Survival Motor Neurone gene o Depending on the type of this disease (which varied based on the presence of other genes), the lifespan of the patient can either be a few years vs. surviving to adulthood Huntington’s Disease can result in both Chorea and Dementia o There will be atrophy of the Striatum and a corresponding enlargement of the Lateral Ventricles o Microscopic view will indicate a reduction in the number of medium-sized spiny neurons (in contrast to the larger neurons which are unchanged) These medium-sized spiny neurons communicate between the Striatum and Global Pallidus o This disease occurs as a result of excessive CAG repeats (i.e. >35 repeats) on Chromosome 4 The number of repeats can potentially increase in successive generations due to mutations in the father’s sperm that carries these genes this worsening / earlier onset in the next generation is referred to as ‘Anticipation’ LEADERS IN THE HISTORY OF MEDICINE TBD - Numerous examples throughout history have illustrated the morally fallible, unethical behaviour present in many exceptional, intelligent and famous Neuroscientists o This highlights the ease of engaging in unethical practices in medicine, and hence the importance of showing leadership to avoid these pitfalls o Furthermore, this highlights that even great doctors can make terrible decisions When a great leader makes a mistake (e.g. Aristotle regarding embryology), it can take hundreds of years to correct this error as people do not wish to contradict / oppose the respected leader Preventing disease is mainly a team-effort rather than due to a brilliant individual (even though there is a tendency to deify the individual) Spread of infectious diseases is dependent on not just the virulence and mode of transmission of the organism / disease, but also the human / societal conditions present (e.g. commerce, war, empire) o There are significant social determinants of illness (e.g. poverty associated with increased illness) o Hence, controlling spread of infectious disease is a communal social achievement, not a medical or individual one Response to Plague involved both excellent public health responses (e.g. quarantine, hiring of ‘Plague’ doctors, destruction of ‘infected’ items) and horrible societal responses (e.g. pogrom burning Jews alive in Strasbourg) o Different communities had different types of responses reflecting their own values Ebola Virus has many similarities to the Black Plague (e.g. high mortality, swift progression, bloody symptoms, foreign origin, blaming sub-groups in society, etc.) o NGOs are working now to train local communities in Africa on infectious control measures to prevent spread of disease and to reduce the fear / ignorance / uncertainty of the Ebola Virus disease - - - DEMENTIA TBD – new in 2015 - Alzheimer’s Disease is the largest cause of Dementia (~85% of all cases of Dementia) Frontotemporal Dementia will results in symptoms focused mainly on behavioural changes o However, other forms of cognition may be retained, so these Frontotemporal Dementia patients may be able to score normally on the MMSE Vascular Dementia arises from a series of the small infarcts (may be due to vascular risk factors such as hypertension, diabetes, etc.) in the brain - 138 o - - - - - - - - This is typically a slowly, progressive dementia rather than having significant step changes in cognition o As a result, it is unclear whether progressive dementia occurs from a series of strokes or other smaller infarcts due to other vascular risk factors Syphilitic Dementia is another form of dementia that will often involve these patients resulting in delusions of grandeur (e.g. patient believes they are the King of Egypt) o HIV is another disease that may ultimately result in Dementia Repeated trauma to the head can potentially result in a form of progressive Dementia (Dementia Pugilistica) CJD (Creutzfeld-Jakob Disease) is a prion disease that can result in Dementia Lewy Body Dementia (LBD) is a form of dementia that will involve fluctuations hour-to-hour and dayto-day in cognition o Visual hallucinations during periods of confusion are also common Vitamin B12 Deficiency and Hypothyroidism can result in Dementia o Similarly, a Frontal Meningioma may trigger symptoms of Dementia Alzheimer’s Disease will result in increased Atrophy of the Brian (incl. loss of weight of the brain) o This can be visualised macroscopically by an enlargement of the size of the sulci o The Ventricles (particularly the Temporal [also known as the Inferior] Horn) will also be enlarged to compensate from the atrophy of the Medial Temporal Lobe / Hippocampus o Note: Small amounts of Brain Atrophy will occur with ageing, but this is exacerbated by Alzheimer’s Disease Neuritic Plaque (also known as Senile Plaque) in Alzheimer’s Disease will involve a circular structure with a periphery of Neuritic Processes surrounding an A-Beta Amyloid Core o There is a clear space / halo between the periphery of Neuritic Processes and the A-Beta Amyloid Core o Note: ‘Congo Red’ is the stain used to identify the presence of Amyloid A-Beta Amyloid will form from the Amyloid Precusor Protein (APP) that is cleaved by the BetaSecretase enzyme o In contrast, cleavage of the APP by the Alpha-Secretase enzyme will NOT result in the formation of an Amyloid protein Evidence suggesting the importance of Amyloid (i.e. A-Beta) protein in Alzheimer’s Disease includes: o Increased prevalence of Alzheimer’s Disease in Down’s Syndrome patients (as the APP is encoded by genes on Chromosome 21) o Familial Alzheimer’s Disease is associated with a gene related to APP o Failure to develop Amyloid Proteins in other forms of Tauopathy Dementias (e.g. Cortical Basal Degeneration, Progressive Supranuclear Palsy) Neurofibrilliary Tangles in Alzheimer’s Disease consist of hyperphosphorylated Tau o These Neurofibrilliary Tangles occur within neurons (and as such are much smaller than the extraneuronal Neuritic Plaques) o Note: Tau has the normal function of stabilising microtubules CSF 14-3-3 protein indicates the presence of rapid brain destruction / degeneration o This protein will be present in CJD as well as other diseases such as rapid Alzheimer’s Disease o CJD will particularly affect the Striatum, as well as other parts of the Cortex o EEG showing Periodic Sharp Wave Complexes is a highly specific sign for CJD o Patients with CJD may appear to have larger white matter tracts within the Cerebellum (i.e. innermost layer) due to the atrophy of the surrounding Cortical Tissue o Patients with CJD will have ‘Spongiform’ vacuoles throughout their Cerebellum Furthermore, there will be no influx of inflammatory cells in these patients This occurs as CJD is NOT a virus or bacteria, but rather a Protein (and hence cannot be destroyed by inflammatory cells) Note: Autoclaving will NOT destroy Prion Cells, so there is a risk of transmission following the re-use of instruments (and so disposable surgical / pathology instruments are now used to avoid this risk) o Note: Pathogenic form of Prion will have increased Beta-sheets 139 PREVENTION IN PSYCHI ATRY Summarise methods of prevention in psychiatry, including: o Opportunities for prevention o Benefits of early intervention o Risk factors and protective factors o Examples of prevention programs - Primary prevention occurs prior to the disease occurring, secondary prevention occurs after the disease has occurred but prior to it causing complications / disability whilst tertiary prevention occurs after complications / disability from disease have arisen o Prevention approaches can be universal, selective (high-risk sub-groups) or indicated (i.e. high-risk individuals with minimal but detectable features of a disorder) Early interventions target people who are displaying the early signs and symptoms of a mental disorder OR are experiencing their first episode of mental disorder o Benefits of early intervention are to minimise / avoid acute episodes of mental illness and provide the best environment for positive mental health for the person o Childhood and adolescence is a critical period for management of mental illness, as many common psychiatric disorders will initially present during childhood and adolescence Early intervention will thus require recognition and diagnosis of these conditions during childhood and adolescence Risk factors for mental illness include: o Parental mental illness o Cold / affectionless parenting o Parental discord o Perinatal problems (this can affect brain development, which can result in increased risk of mental illness later in life) o Adverse life events o Low intelligence (this may be a sign of an underlying problem with brain development, such that these people have an increased risk of mental illness / psychosis) Protective factors for mental illness include: o Success / Achievement o Belief in own effectiveness o ‘Easy’ temperament o Sense of humour and optimism o Positive school life (this can compensate for challenges / problems at home) o Good peer relations o Positive relation with a caregiver (e.g. parent, grandparent, mentor / teacher, etc.) o High intelligence Examples of prevention / intervention programs include: o Positive Parenting Program (i.e. Triple P) This is a set of packaged interventions that can applied within communities, and will be applicable at any stage of life of person Appropriate intervention at any of the stages of life can prevent progression on a delinquent pathway with increased age to further delinquent behaviour These interventions have been identified based on prior research, so the value of Triple P is simply to compile these different interventions together into a package Interventions are not complicated but rather cover basic parenting strategies, including teaching parents about causes of behavioural problems, positive encouragement techniques, disciplinary measures (e.g. quiet time), etc. One the key benefits from this program is having a group of parents that are seeking help to come together to share their problems This has led to parents feeling more confident in their parenting, making significant changes in home, etc. Studies have illustrated that Triple P program resulted in significant reduction in negative child behaviour and improved parenting sense of competency - - - - 140 o o Study also illustrated Triple P program at a population level reduced the level of child abuse / injuries Prevention and Early Intervention of Schizophrenia Universal prevention in schizophrenia is difficult, as many of the risk factors are nonmodifiable (e.g. family history, antenatal / perinatal complications, immigration, season of birth) Instead, early intervention is arguably the earliest time for an intervention to be implemented to reduce the prevalence of schizophrenia The challenge with early intervention is how to accurately identify people with prodromal Schizophrenia (or is actually a slightly depressed mood?) and what is the appropriate early intervention to provide (e.g. medication, non-pharmacological, etc.) As a result, a lot of the focus is to reduce the duration of the untreated acute psychosis (i.e. after prodromal phase) Early intervention has been shown to lead to better outcomes for schizophrenia patients (i.e. earlier the treatment following onset of psychosis, the better the outcomes) Children of Parents with Mental Illness Parents with mental illness will not only pass on genes which increase the risk of mental illness, but also create an environment that increases the risk of mental illness in the child (e.g. social isolation, difficulty communicating with children, difficulty teaching children social norms) Preventative intervention programs for these children include Peer Support Programs, Family Interventions, Online Interventions and Bibliotherapy These programs will educate children about mental illness and teach them coping skills / resilience (which reduces probability of mental illness) Note: ‘Bibliotherapy’ involves providing people with literature to teach them about their problems and possible solutions PRACTICAL ANATOMY PRACTICAL 1 – SPINAL CORD AND SPINAL NERVES Recognise the gross anatomical features of the spinal cord (including blood supply), associated nerve roots and meninges - ... Understand the organisation of a 'generic' segment of the spinal cord, including: o Generic features of the grey matter; o Compartmentalisation of the white matter; and o ... ... Disposition of the dorsal and ventral roots, spinal nerves and their primary rami ... Recognise the cross sectional features of cervical, thoracic, lumbar and sacral levels of the spinal cord and significance of the lumbar and cervical enlargements - ... 141 Understand the organization of the spinal grey matter including awareness of Rexed's laminae and the grouping of these into 'dorsal', 'intermediate' and 'ventral' grey - ... Establish awareness of the classification of sensory and motor fibres and understanding of the distribution of different modalities into separate fibre tracts. - ... Know the names and locations of the major ascending (spino-thalamic, dorsal column, spino-cerebellar) and descending (cortico-spinal, rubrospinal, vestibulo-spinal, reticulo-spinal) tracts, and in general terms, their destinations - ... PHYSIOLOGY PRACTICAL 1 – REFLEXES AND CUTANEOUS SENSAT ION Elicit the reflexes usually used in clinical examination and indicate the neuronal pathways involved - ... Perform the standard clinical tests for cutaneous sensation and interpret the observations - ... Indicate the range of normal values for standard motor and sensory tests - ... Measure and calculate the conduction velocity of a myotatic reflex - ... Demonstrate that muscle spindles contribute to the sense of proprioception - ... ANATOMY PRACTICAL 2 – CSF, MENINGES AND VE NTRICLES Know the location of the cerebral ventricles and cerebral aqueduct - ... Know the disposition of the meninges (i.e. dura mater, arachnoid mater, pia mater), their relationship to the brain, the cerebral vasculature and the circulation of the CSF - ... Understand the location and function of the choroid plexus - ... 142 HISTOLOGY PRACTICAL 1 – HISTOLOGY OF BRAIN AND MENINGES Understand the microscopic appearance of brain tissue and the meninges - ... ANATOMY PRACTICAL 3 – NORMAL BRAINSTEM Identify the external features of the brainstem - ... Distinguish sections of medulla oblongata, pons and midbrain at characteristic levels and relate these to the external features - ... Understand the paths taken by the major ascending and descending tracts (identified in 6.01 BCS#1) and recognise associated brainstem nuclei - ... Understand the arterial supply of the brainstem, particularly in relation to the specified ascending and descending tracts, and related nuclei - ... PHYSIOLOGY PRACTICAL 2 – EYE MOVEMENTS Understand the different types of eye movements - ... Understand the anatomical structures involved and the function of each type of movement - ... Understand the use of the electro-oculogram - ... ANATOMY PRACTICAL 4 – CRANIAL NERVES Identify the 12 cranial nerves where they are attached to the base of the brain - ... Identify cranial nuclei within the brainstem in the sections studied previously (6.02 BCS 1) and appreciate that a given nucleus may relate to several cranial nerves - ... 143 Identify the sites where cranial nerves exit the skull. - ... Observe where cranial nerves pierce the dura mater and deduce their intracranial course (where relevant) - ... Identify the more prominent cranial nerves in the face and neck - ... PHARMACOLOGY PRACTICAL 1 – CENTRAL NEUROTRANSMI TTERS Describe the structural components of neurons, which are involved in synaptic transmission - ... List the major chemical neurotransmitters involved in CNS function - ... Explain to steps involved in the synthesis, storage, release and post synaptic actions of these major neurotransmitters - ... ANATOMY PRACTICAL 5 – CORTEX – STRUCTURE AND FUNCTI ON Recognise the division of the cerebrum into lobes (i.e. frontal, temporal, parietal and occipital) - ... Understand what is a ‘gyrus’ and ‘sulcus’ - ... Be aware of cortical lamination and understand the concept of projection, associational and commissural fibres - ... Understand the concept of 'primary', 'secondary' and 'higher-order (association)' cortical areas - ... Be aware of Brodman's Areas - ... Identify primary and secondary visual, somatosensory, motor and auditory areas 144 - ... Understand the concept of 'laterality' and to recognize the main speech and language areas in the brain - ... PHYSIOLOGY PRACTICAL 3 – VISUAL TESTING Determine your own near point and far point - ... Understand and calculate the power of accommodation and the amount of myopia and hyperopia - ... Determine whether you have astigmatism - ... Measure your own visual acuity using a standard clinical test chart - ... Identify colour blindness and the type of defect present - ... Measure the diameter of your area of highest visual acuity and of your blind spot - ... Calculate the diameter of your fovea and optic disc - ... Recognise normal retinal features in fundus photographs - ... ANATOMY PRACTICAL 6 – VISUAL PATHWAYS Identify the anatomical and functional organisation of the central visual pathways from the retina to the cortex (i.e. optic nerve, optic tract, superior colliculus, pretectum, suprachiasmatic nucleus, lateral geniculate nucleus, pulvinar, optic radiation, primary and secondary visual cortex) - ... Describe major signs and symptoms associated with lesions of each region, particularly the different visual cortices - ... 145 ANATOMY PRACTICAL 7 – MOTOR PATHWAYS Identify anatomy of the basal ganglia nuclei (i.e. caudate-putamen, globus pallidus, subthalamus, substantia nigra and pedunculopontine nucleus) - ... Identify normal circuitry and major connections (+neurotransmitters) of the basal ganglia (direct and indirect pathways) - ... Describe suspected functions associated with the basal ganglia and the way in which these nuclei may work in the great scheme of motor control system - ... ANATOMY PRACTICAL 8 – FOREBRAIN STRUCTURES Understand the anatomical organisation of forebrain structures, including the cortex, thalamus, hypothalamus, basal forebrain, hippocampus, amygdala, olfactory areas and basal ganglia - ... Understand the organisation of fibres within the internal capsule - ... ANATOMY PRACTICAL 9 – ANATOMY REVISION Revise anatomy for the Block - ... 146


























































































































































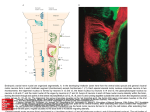






![Nervous Tissue [PPT]](http://s1.studyres.com/store/data/000313628_1-63044c543d97a5d91f1cbdf37558ffd7-150x150.png)