Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Executive functions wikipedia , lookup
Effects of sleep deprivation on cognitive performance wikipedia , lookup
Aging brain wikipedia , lookup
Limbic system wikipedia , lookup
Memory consolidation wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Source amnesia wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Emotion and memory wikipedia , lookup
Spatial memory wikipedia , lookup
Prenatal memory wikipedia , lookup
Adaptive memory wikipedia , lookup
Time perception wikipedia , lookup
Effects of alcohol on memory wikipedia , lookup
Exceptional memory wikipedia , lookup
Interference theory wikipedia , lookup
Atkinson–Shiffrin memory model wikipedia , lookup
Memory and aging wikipedia , lookup
Misattribution of memory wikipedia , lookup
Mind-wandering wikipedia , lookup
Collective memory wikipedia , lookup
Childhood memory wikipedia , lookup
State-dependent memory wikipedia , lookup
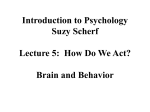
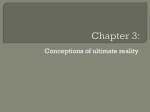
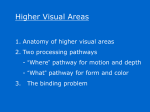
Neuropsychology Copyright 1998 by the American Psychological Association, Inc. 0894-4105»8/$3.00 1998, Vol. 12, No. 1,52-64 Short-Term and Long-Term Memory in Early Temporal Lobe Dysfunction Suzanne Craft Tamara Hershey Washington University Seattle-American Lake Veterans Affairs Medical Center and University of Washington Tracy A. Glauser Sandra Hale Washington University Children's Hospital Medical Center Cincinnati, Ohio Following medial temporal damage, mature humans are impaired in retaining new information over long delays but not short delays. The question of whether a similar dissociation occurs in children was addressed by testing children (ages 7-16) with unilateral temporal lobe epilepsy (TLE) and controls on short- and long-term memory tasks, including a spatial delayed response task (SDR). Early-onset TLE did not affect performance on short delays on SDR, but it did impair performance at the longest delay (60 s), similar to adults with unilateral medial temporal damage. In addition, early-onset TLE affected performance on pattern recall, spatial span, and verbal span with rehearsal interference. No differences were found on story recall or on a response inhibition task. The study of memory systems and their representation in the brain has often focused on identifying dissociable subsystems. Many types of memory distinctions have been proposed on the basis of cognitive, neuropsychological, and neurophysiological evidence, such as semantic-episodic memory (Tulving, Kapur, Craik, Moscovitch, & Houle, 1994X declarative-nondeclarative memory (Squire, 1992), implicit-explicit memory (Schacter, Chiu, & Ochsner, 1993), and short-term-long-term memory (Alvarez, Zola-Morgan, & Squire, 1994). The present study focuses on the distinction between short- and long-term memory following early temporal lobe dysfunction in children. Short-term memory, the ability to represent information internally for brief periods of time, is considered to be a fundamental feature of working memory (Baddeley, 1992; Goldman-Rakic, 1987). This ability is commonly not affected by medial temporal region damage in adult humans and animals. Long-term memory, the ability to store information for later recall, is impaired following damage to or disruption of components of the medial temporal region. A variety of tasks have been used in both animals and humans to demonstrate this distinction, most notably the delayed nonmatch to sample (DNMS), delayed match to sample (DMS), and spatial delayed response (SDR) tasks. These tasks involve the brief presentation of a piece of information followed by a delay. For the DNMS and DMS tasks, objects or colors are generally used; for the SDR task, spatial locations are used. After the delay has ended, participants must recognize or recall the piece of information presented prior to the delay. On such tasks, adult animals and humans with medial temporal damage are able to perform accurately on trials with short delays yet are impaired on trials with longer delays (DNMS: Alvarez et al., 1994; Bachevalier & Mishkin, 1989; Overman, Ormsby, & Mishkin, 1990; Squire, Knowlton, & Musen, 1993; Squire, Zola-Morgan, & Chen, 1988; Zola-Morgan & Squire, 1985; DMS: Aggleton, Nicol, Huston, & Fairbairn, 1988; Prisko, 1963; Sidman, Stoddard, & Mohr, 1968; SDR: Backer Cave & Squire, 1992; Kowalska, 1995; Rains & Milner, 1994; Zola-Morgan & Squire, 1985). In general, delays greater than 15-30 s on these tasks are sensitive to medial temporal damage (Alvarez et al., 1994; Rains & Milner, 1994; Squire et al., 1988), although this may differ across specific task demands, materials, species, and the extent and exact placement of the lesion (Angeli, Murray, & Mishkin, 1993; Eichenbaum, Otto, & Cohen, 1994; Leonard, Amaral, Squire, & Zola-Morgan, 1995; Muri, Rivaud, Timsit, Cornu, & Pierrot-Deseilligny, 1994; Sidman et al., 1968). Tamara Hershey and Sandra Hale, Department of Psychology, Washington University in St. Louis; Suzanne Craft, The Geriatric Research, Education and Clinical Center of the Seattle-American Lake Veterans Affairs Medical Center, and the Department of Psychiatry and Behavioral Sciences, University of Washington; Tracy A. Glauser, Department of Neurology, Children's Hospital Medical Center, Cincinnati, Ohio. This study was conducted in partial fulfillment of the requirements for Tamara Hershey's doctoral degree and was supported in part by a Washington University Dissertation Fellowship. Preliminary results from this study were presented at the Second Annual Meeting of the Cognitive Neuroscience Society held in San Francisco, California, in 1995. We would like to thank the students and teachers at the Governor French Academy and the Pediatric Neurology and Psychology Departments at St. Louis Children's Hospital for their assistance. We also thank the reviewers for their thoughtful and helpful comments. Correspondence concerning this article should be addressed to Tamara Hershey, who is now at Washington University School of Medicine, Department of Psychiatry, 4940 Children's Place, St. Louis, Missouri 63110. Electronic mail may be sent via Internet to [email protected]. 52 MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION Short-term memory, as measured by the SDR task, has been associated with the dorsolateral prefrontal cortex. Following dorsolateral prefrontal damage, performance on the SDR task is impaired on trials with the shortest delay (Bauer & Fuster, 1976; Freedman & Oscar-Berman, 1986; Funahashi, Bruce, & Goldman-Rakic, 1993; Joyce & Robbins, 1991). In addition, studies have demonstrated that cells in the dorsolateral prefrontal cortex fire selectively during the delay period of the SDR task (Funahashi et al., 1993; Goldman-Rakic, 1987). The dorsolateral prefrontal cortex is thought to be responsible for holding spatial information on-line, particularly for short periods of time. Further, inferior frontal cortex has been associated with short-term memory for repeated or unique objects on the DMS task (Fuster, 1990; Wilson, Scalaidhe, & Goldman-Rakic, 1993). Performance on the DNMS task using unique stimuli is unimpaired following prefrontal cortex damage (GoldmanRakic, 1987). It has been proposed that the dorsolateral prefrontal cortex is highly involved in the short-term memory of spatial information, whereas the inferior frontal cortex is involved in the short-term memory of object information (Goldman-Rakic, 1987; Wilson et al., 1993). Thus, shortand long-term spatial and object recognition memory as measured by DMS, but not DNMS, appear to be dissociable following lesions to medial temporal versus dorsolateral or inferior prefrontal cortex (Alvarez et al., 1994; Winocur, 1992). This general pattern has also been reported in adult humans with temporal lobe epilepsy (TLE), a disorder associated with medial temporal dysfunction and neuropathology. Notably, these studies have focused on unilateral TLE, which may make comparisons somewhat difficult with animal work, in which bilateral lesions are generally present. Short-term memory measures (immediate recall, span tasks, consonant or pattern trigram tasks) generally have not revealed consistent differences between left and right temporal lobe epileptics and their normal control groups (Delaney, Prevey & Mattson, 1982; Delaney, Rosen, Mattson, & Novelly, 1980; Lavadas, Umilta, & Provincial!, 1979). If differences have been found, they have occurred at delays of greater than 9 s (Delaney et al., 1982; Prevey et al., 1994) and only with auditory verbal material (Delaney et al., 1982; Samuels, Butters, & Fedio, 1972). After resection of the medial temporal region to treat intractable seizures, longterm memory generally becomes more impaired on clinical memory tasks (Ojemann & Dodrill, 1985; Wechsler, 1987). One recent study has addressed the impact of medial temporal excisions in seizure patients on tasks similar to those used in animal studies, such as DMS and SDR. Among other interesting results, Owen et al. (Owen, Sahakian, Semple, Polkey, & Robbins, 1995) found that patients with amygdala-hippocampal excision were impaired on the longest delay of the DMS task (12 s), with relatively normal performance on shorter delays and a simultaneous matching condition. On a spatial recognition task, participants were shown a list of spatial locations and then given two-choice recognition trials 3-72 s later. Patients with amygdalahippocampal excisions performed significantly worse than controls on this task. However, the data were not analyzed 53 according to delay, so it is difficult to know if performance was spared for trials with short delays. Notably, left and right excision patients performed similarly on both of these tasks. Research on the neural representation of short- and long-term memory in developing animals and humans has been less extensively reported. Bachevalier (1990) and Mahut and Moss (1984) found that damage to the medial temporal region in young monkeys produces long-term memory impairment as measured by the DNMS task, similar to results in adult monkeys. There have also been several reports of childhood bilateral or unilateral medial temporal damage that has led to dense amnesia (Ostergaard, 1987; Tonsgard, Harwicke, & Levine, 1987; Wood, Brown, & Felton, 1989). However, the neuropsychological evaluations of these children have been limited at best, and no careful analyses of short- and long-term memory have been conducted. In contrast, case studies of unilateral or bilateral temporal lobe agenesis have reported no apparent memory deficits, although, again, testing was limited (Karvounis, Chiu, Parsa, & Gilbert, 1970; Lang, Lehrl, & Huk, 1981). A number of studies on TLE have addressed similar developmental questions hi adults (Saykin, Gur, Sussman, O'Conner, & Gur, 1989; Saykin et al., 1992; Wishart, Warmflash, Barr, & Schaul, 1995) and children (Cohen, 1992; Fedio & Mirsky, 1969; Jambaque, Dellatolas, Dulac, Ponsot, & Signoret, 1993). These studies have generally documented that unilateral TLE patients with early-onset seizures or an early insult, such as febrile seizures, have more severe memory deficits (Saykin et al., 1989; Saykin et al., 1992; Wishart et al., 1995) and more overt hippocampal damage (McMillan, Powell, Janota, & Polkey, 1987; Trenerry et al., 1993; Zaidel, Esiri, & Oxbury, 1993; Mathern, Pretorius, & Babb, 1995). In addition, one study by Saykin et al. (1989) found that TLE patients with early onset of seizures were impaired on both immediate and delayed recall conditions of traditional memory tasks. However, tasks such as DMS and SDR have not been used to examine the effects of earlyversus late-onset TLE on short- and long-term memory. Further, only one study (Fedio & Mirsky, 1969) has examhied short- and long-term memory in children with TLE. They found no difference between left temporal, right temporal, and normal control children on span measures. However, on supraspan tasks (a presumed long-term memory task), the left temporal group performed worse on the verbal task and the right temporal group performed worse on the visual-spatial task. Unfortunately, there was a significant difference in severity of disease between the two TLE groups. Thus, it is somewhat unclear whether disruption of the medial temporal system during development impairs or spares short-term memory performance in immature animals or humans as measured by delayed response or delayed recognition tasks. Given that memory systems and their neural mechanisms undergo profound changes in both capacity and organization during all stages of development (Chugani, Phelps, & Mazziotta, 1987; Flavell, 1977; Huttenlocher, 1990; Janowsky, 1992; Kail, 1979), it is possible that the representation of short- and long-term memory changes across development. Medial temporal damage early in life 54 HERSHEY, CRAFT, GLAUSER, AND HALE has been reported to produce deficits traditionally associated with prefrontal dysfunction, whereas the same damage later in life does not. Bachevalier (1994) has reported that early, bilateral medial temporal damage in monkeys produces emotional and social dysfunction as well as deficits in learning and memory. She attributes this pattern to the possibility that early medial temporal damage stimulates reorganization of closely associated areas, such as the prefrontal cortex. Another study on humans with TLE reported that early-onset left TLE (LTLE) is associated with significantly more perseverative responses on the Wisconsin Card Sorting Test (generally sensitive to prefrontal dysfunction) than late-onset TLE. Right TLE (RTLE) was associated with mild impairment regardless of age of onset (Strauss, Hunter, & Wada, 1993). Further, Bilder et al. (1995) have found strong correlations between anterior hippocampal volumes and executive functions, such as planning skills and response inhibition, in schizophrenics. They speculate that early damage to the anterior hippocampus disrupts connections to the prefrontal cortex, affecting the entire frontolimbic system. The short-term memory system, another prefrontally mediated skill, may also be affected by early medial temporal damage. Short-term spatial memory appears to rely heavily on dorsolateral prefrontal cortex in adulthood and across development. The dorsolateral prefrontal cortex is reciprocally connected to the medial temporal region and the inferior parietal cortex, and the medial temporal region receives projections from the inferior parietal cortex. All three areas are activated during spatial delayed response tasks (Friedman & Goldman-Rakic, 1991; Goldman-Rakic, 1987; Goldman-Rakic, Selemon, & Schwartz, 1984). The medial temporal region and prefrontal cortex appear to be responsible for the mnemonic aspects of the SDR task, whereas the inferior parietal region appears to be responsible for initial nonmnemonic spatial processing (Goldman-Rakic, 1987). GoldmanRakic (1987) has hypothesized that the hippocampal and prefrontal regions coordinate the management of memory demands, with the prefrontal cortex responsible for shortdelay memory processing and the hippocampal region responsible for longer term or larger capacity memory processing. Short-term object recognition memory, as measured by die DMS task, is also supported by the reciprocally connected areas of medial temporal and inferior frontal cortex (Fuster, 1990; Mishkin & Murray, 1994). It is possible that the relationship between medial temporal and prefrontal regions and their mnemonic responsibilities may change across development. Because the medial temporal region develops relatively earlier than prefrontal cortex, it may be responsible for short-term memory early in development. As the prefrontal cortex develops, it may be able to take over shorter term and less demanding memory tasks, leaving more difficult and demanding tasks for medial temporal processing. Early damage to the medial temporal system could interrupt this transfer of functional specificity and could thus affect short-term memory functioning. Therefore, we predict that children with early-onset TLE would show deficits on SDR and DMS tasks at short delays, demonstrating less sparing for short-term memory. More traditional measures of human short- and long-term memory (e.g., immediate and delayed recall of complex information, span tasks) do not have animal analogues and so are difficult to compare to SDR and DMS. However, based on the idea of reduced short-term memory following early medial temporal damage, we also predicted that children with early-onset TLE would perform poorly on immediate recall trials and span tasks compared to controls. Method Participants Participants consisted of 15 children with LTLE (10 males, 5 females; 12 right-handed, 3 left-handed) and 13 children with RTLE (8 males, 5 females; all right-handed). These children were recruited from the Pediatric Neurology Clinics at St. Louis Children's Hospital and Children's Hospital Medical Center in Cincinnati, Ohio. The children had no other medical diagnosis with central nervous system effects; no evidence of mental retardation; and no previous neurosurgery, head injury, or stroke. All children with epilepsy had undergone BEG for localization of their seizures within 2 years prior to testing, and, in most cases (26/28), they also had magnetic resonance imaging (MRI). Of the 26 scans, 7 had abnormal MRI readings ipsilateral to their epileptic foci (4 scans showed distinct medial temporal atrophy ipsilateral to their epileptic foci, 1 showed anterior temporal atrophy, 1 showed lateral ventricle enlargement, and 1 had poor myelination throughout). All other scans were judged to be within normal limits. Seizures were identified as unilateral, unifocal complex partial seizures emanating from the temporal lobe by a pediatric neurologist based on seizure descriptions, observations, and EEG. It was not possible to determine the precise location of patients' seizure foci within the temporal lobe from these techniques, as both lateral and medial temporal foci can lead to similar seizures and medial temporal atrophy (Ebersole & Pacia, 1996). See Tables 1 and 2 for additional group information. TLE groups were statistically equivalent on every variable measured that related to severity of the seizure disorder (duration, age of onset, age at first risk factor for seizures, seizures within the month prior to testing, seizures within the last year, and number of generalized seizures in lifetime) and medication (number of medications, and number of hours between last dose of medication and testing start time). These results indicate that our two TLE groups were well matched on these clinical variables. However, there was a high level of variance in the number of seizures in the Table 1 Means and Standard Deviations of Demographic Variables by Group Normal control (n = 19) Left temporal (n = IS) Right temporal (n = 13) Variable M SD M SD M SD Age Grade Parents' average years ofeducation Information Block Design 11.53 5.32 2.7 2.4 11.24 5.00 2.6 2.5 11.16 5.17 2.4 2.2 13.71 12.68 10.79 2.2 2.6 3.6 13.93 10.00* 8.73 2.4 3.2 4.1 13.27 8.62* 8.77 2.0 2.1 2.5 *p < .05, a significant difference from the normal control group. MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION Table 2 55 Measures Means and Standard Deviations of Clinical Variables by Epilepsy Group Left temporal Wechsler Intelligence Scale for Children—3rd Edition Right temporal Variable M SD M Age of onset Age at first risk factor Duration of seizure disorder Months since last seizure Hours since last medication dose Number of medications Number of seizures in last month 5.6 2.7 2.9 3.0 5.7 3.5 3.7 2.9 5.8 11.3 3.9 9.9 5.5 18.4 4.9 25.9 SD b 2.7" 1.1 1.2 0.6 3.8 0.9 1.8 0.5 0.0 0.0 0.5 1.2 "n = 13. "re - 11. year prior to testing in the LTLE group due to one outlier.1 Analyses were computed both with and without this participant, and no differences were obtained in any of the results. All analyses reported here included this participant. As expected, duration and age of onset were significantly inversely correlated with each other within both LTLE (r = -.75, p < .01) and RTLE (r = -.88, p < .01) groups. Due to these strong correlations, any effects of age of onset must be considered to be partly due to effects of duration. Duration and age at time of testing were correlated (LTLE: r = +.65,p < .01; RTLE: r = +.67, p = .01). See Table 2 for means and standard deviations. A normal comparison (NC) group consisted of 19 participants, who were matched on the basis of age, sex, and parents' years of education (11 males, 8 females; 18 right-handed, 1 left-handed). Children in the NC group had no history of brain injury, stroke, or epilepsy, were not on any medications, and did not have any other medical diagnoses with central nervous system effects. These children were recruited from local private and parochial schools and from the community. NC and epilepsy participants were between the ages of 7 and 16. For all children, a parent gave written informed consent prior to their participation. Mean age at time of testing and mean years of education for mother and father were statistically equivalent across all three groups. Three mothers in the NC group and one mother in the LTLE group reported only their educational level, due to the fathers' absence from the home and lack of knowledge regarding the fathers' present level of education and occupation. To reflect the educational level of each child's household more accurately, a mean parents' years of education variable was calculated. For households with two parents, an average years of education was calculated. For households with only the mother, the mother's years of education was used for the mean parents' years of education. This variable was not significantly different between the groups. See Table 1 for means and standard deviations. Procedure Children with epilepsy were tested at St. Louis Children's Hospital or Children's Hospital Medical Center in Cincinnati, Ohio. NC children were tested either at St. Louis Children's Hospital or at their school. All tasks (with the exception of the WISC-III subtests) were developed with two equivalent versions, because some participants were tested twice for the purposes of another study. Only the first session is reported here. The two versions were counterbalanced across groups. (WISC-III; Wechsler, 1991) Two subtests (Information, Block Design) were given as a measure of general cognitive functioning. Performance on these tests provided an estimate of each child's basic verbal and spatial functioning as compared to an age-matched normative group. SDR This task was used to measure participants' spatial memory across short and long delays. It involves the ability to hold spatial information in memory for a brief or extended amount of time and to update that information repeatedly. The basic components of this task were adapted for use in humans by Luciana et al. (Luciana, Depue, Arbisi, & Leon, 1992). This methodology was used with some modification for our purposes. Participants were required to focus on a central fixation point on a computer screen, While they remained fixated, a cue appeared in one of 32 possible locations at a 4.5-in. (10.8 cm) radius from a central fixation point for 150 ms, a duration too brief for any eye movements to occur. The fixation cross then turned gray for a delay period of either 2 s, 30 s, or 60 s. During the delay, participants were required to fixate on the center cross while they listened to a tape on which a voice spoke letters at the rate of one per second. They were instructed to say "yes" out loud whenever a letter A was heard. The experimenter monitored the children's eye movements and verbally cued the children to fixate on the cross whenever they appeared to move their eyes. After the delay, the fixation cue turned black, and they were asked to point to the place on the computer screen where they remembered seeing the cue. The experimenter then moved the cursor with a mouse to the point where the children were pointing and recorded that location. Responses were measured in X and Y coordinates and compared to the actual location of the cue. Thirty-two experimental trials were presented, eight trials at each delay, plus eight trials with no mnemonic load. On these "cue-present" trials, the cue was present during the delay and response phase. This set of trials allowed some indication of the children' pointing accuracy. Mean error (distance from target) was calculated for each child for each type of trial (2 s, 30 s, 60 s, cue-present). DMS A DMS task was used to measure pattern recognition memory across short and long delays. The general task specifications were derived from Diamond (1990), but different stimuli were used to make this a more challenging task. In this task, participants were seated in front of the computer screen. A trial consisted of the following: A line drawing appeared in the center of the computer screen for 2 s. Participants were instructed to study the drawing. These drawings were abstract, geometrical figures that were matched for major figural components and thus required effort to distinguish. Unique drawings were used on each trial. The drawing disappeared and a central fixation point remained on the screen for varying delays (2 s, 30 s, 60 s). During the delay, participants were lr This child had over a thousand seizures in the year preceding her participation in this study. However, most of these seizures were in the first half of the year. After changing medications, she achieved excellent seizure control and had no seizures in the few months preceding her testing session. 56 HERSHEY, CRAFT, GLAUSER, AND HALE instructed to listen to a tape and say "yes" whenever they heard a letter A. When the fixation point disappeared, two drawings appeared, one left of center and one right of center. One of these was the drawing that appeared just prior in the trial. The participants were instructed to press the computer key corresponding to the old drawing (the left key or the right key). Three practice trials were given. The experimental segment consisted of 8 trials at each delay period for a total of 24 trials. Total number of errors and median response time were calculated for each participant for each delay condition (2 s, 30 s, 60 s). Story Recall Task The story recall task was used to test verbal declarative memory. Immediate and delayed recall trials in free recall formats were given. Participants heard two brief narratives containing 18 informational bits each. They were then asked to recall as much of each story as possible immediately after hearing each paragraph (immediate recall) and following a 25 to 30-min delay (delayed recall). Credit was given for each informational bit recalled verbatim and half credit was given for accurate paraphrases. Confabulations (recalling information clearly not related to the story) were also recorded. Total verbatim, paraphrase, and confabulation scores were calculated for immediate and delayed recall conditions. The paragraph recall task has been used extensively in previous investigations on memory (Craft, Zallen, & Baker, 1992; Newcomer, Craft, Hershey, Askins, & Bardgett, 1994) and is a well-validated declarative memory task (Squire, Shimamura, & Graf, 1987). Pattern Recall Task The pattern recall task was used to test visual declarative memory. Immediate and delayed recall trials were administered. Children were presented with a page consisting of three separate patterns constructed of four dark-colored blocks each on a 3 X 3 matrix (12 colored blocks out of 27 total blocks). They were instructed to study the patterns for later recall. After the children viewed the page for 10 s, it was removed from sight. The children then were asked to reproduce the three patterns and their locations on the page on another piece of paper with three blank 3 x 3 matrices. After a 25 to 30-min delay, participants were asked to recall the patterns once more. On all recall trials, 1 point was given for each correctly placed block in a pattern, A total correct score was calculated for immediate and delayed recall conditions. This total correct score was reduced by 1 point for every extra block beyond 12 that the child marked. Performance on this task has shown to be sensitive to changes in memory functioning in a previous study (Craft et al., 1992). Verbal Span Verbal span was administered as described in Hale et al. (Hale, Myerson, Rhee, Weiss, & Abrams, 1996) and is consistent with Baddeley's model of verbal short-term memory (Baddeley, 1992). This task was used as a measure of verbal short-term memory with and without an interference condition. The interference condition served to place a higher load on the working memory system. Without interference. Participants observed a series of digits that appeared one at a time inside a 4 X 4 matrix on the left side of the screen. Each digit appeared for 2 s with a 1-s intertrial interval. When an empty matrix appeared at the end of the series, participants had to recall the series of numbers in the same order that they appeared. The series began with one digit and could potentially end with a series of nine digits. Two trials were given at each series length. If the children correctly recalled one or both trials at a given series length, they advanced to the next series length. If both trials were failed at a given length, the task ended, and 1 point was given for every correct response. With interference. This version was similar to the previous version except that participants also had to name the colors in which the digits appeared. Digits were one of three colors: red, white, or blue. Participants were familiarized with the colors before beginning any trials. As each digit appeared, participants were required to name the color of the digit. When the blank matrix appeared, they were instructed to recall the series of digits that preceded it. Response scoring and the discontinuation criteria were as stated previously. Spatial Span Spatial span was administered as described in Hale et al. (1996) and is consistent with Baddeley's model of spatial short-term memory (Baddeley, 1992). This task was used as a measure of spatial short-term memory with and without an interference condition. The interference condition served to place a higher load on the working memory system. Without interference. Participants were seated in front of a computer on which they were shown a series of Xs in different locations within a 4 X 4 matrix, one at a time. Each X appeared for 2 s with an intertrial interval of 1 s. When a blank matrix appeared, participants were required to mark on the computer screen where the Xs in the previous series had appeared. There was a limited time in which they could recall the series. The series began with one X and could potentially end with a series of nine Xs. Two trials were given at each series length. If participants correctly recalled one or both trials at a given series length, they advanced to the next series length. If both trials were failed at a given length, the task ended, and 1 point was given for every correct response. With interference. The basic structure of this task was similar to spatial span without interference except that the Xs appeared in one of three colors (red, white, or blue). Participants were instructed to identify which color each X was drawn in by pointing to a palette of the three possible colors to the right of the matrix. When the empty matrix appeared, participants were required to mark the locations in which the Xs in the series appeared. Response scoring and discontinuation criteria were as stated previously. Response Inhibition Task The Stroop Color and Word Test has been shown to be sensitive to frontal lobe dysfunction and requires response inhibition (Ferret, 1974). The standard version of this task involves reading words. Because our participants varied in reading ability due to their age, we developed a task that involves response inhibition but does not require word reading. In this task, participants were first shown a 2 X 2-in. ( 5 X 5 cm) block of color (either red, blue, or green) against a black background, which appeared randomly in one of four quadrants on a computer screen, and they were asked to name the color (alone condition). Voice onset time was recorded by a voice key interfaced with the computer, and participants' verbal responses were recorded on the computer after every trial by an experimenter. Thirty trials, 10 of each color, were given. Then participants were shown the same size block of color outlined in black in the center of a larger ( 5 X 5 in., 9.5 X 9.5 cm) block of color, again appearing randomly in one of four quadrants of the computer screen. Participants were again asked to name the color of the small block (the block in the middle). Sixty trials were given. 57 MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION On half of the trials, both blocks were the same color (congruent condition); on the other half of the trials, the blocks were different colors (discongruent condition), requiring the children to inhibit their response to the larger, more prominent color. Reaction time and accuracy were recorded and compared between conditions. Results Memory Measures SDR Task A repeated measures general linear models analysis was conducted on SDR error scores (millimeters between the target and the response) with group (NC, LTLE, RTLE) as the independent variable and delay (cue-present, 2 s, 30 s, 60 s) as the repeated measure. A significant main effect was obtained for delay, F(2,44) = 117.72, p< .01, as well as an effect of group, F(2, 44) = 3.32, p = .05. In addition, a significant interaction between group and delay was obtained, F(6,44) = 4.44, p < .01. Repeated measures general linear models analyses were also carried out on pairs of groups (NC and LTLE, NC and RTLE, LTLE and RTLE). These analyses revealed that the interaction between group and delay was present when comparing NC and LTLE, F(3, 32) = 7.76, p < .01, and NC and RTLE, F(3, 30) = 6.34, p < .01, but not when comparing the two epilepsy groups. Finally, separate general linear models analyses was conducted on all groups at each delay condition. There were strong group effects at the 60-s delay only, F (2,44) = 5.87, p < .01. Bonferroni corrected post hoc comparisons were conducted that revealed that the RTLE and the LTLE groups performed significantly worse than the normal controls at the 60-s delay (see Figure 1). No group had any apparent 60 -, 50 - • Normal Control • Left Temporal A Right Temporal 40- 30 - 20 - 10 - Table 3 Means and Standard Deviations ofDMS Error Rates by Group Normal control (« = 19) Left temporal (n = 14) Right temporal (« = 13) Delay M SD M SD M SD 2s 30s 60s .07 .05 .01 .11 .06 .04 .14 .09 .11 .16 .12 .11 .09 .09 .07 .15 .13 .13 Note. DMS = delayed match to sample. difficulty with the sensory or perceptual aspects of the task, demonstrated by their accurate performance at the cuepresent condition. In addition, age of onset was not associated with performance at any delay for the two epilepsy groups. DMS A repeated measures general linear models analysis was conducted on DMS error rates (ratio of number of incorrect responses to total number of trials in that condition) with group (NC, LTLE, RTLE) as the independent variable and delay (2 s, 30 s, 60 s) as the repeated measure. There was no significant main effect of delay, but there was a main effect of group, F(2,44) = 3.45, p < .05. The interaction between group and delay was not significant. Inspection of the data revealed that one LTLE participant performed at chance levels (50%), which was much worse than the other participants. When this participant's data were removed from the analysis, the main effect of group was no longer present (p = .09). See Table 3 for means and standard deviations of these corrected data. As can be seen from these data, the DMS task was insensitive to group differences most likely due to ceiling effects. To examine the relationship of age to the rate of ceiling performance, a median split on age was performed for each group. On average, 28% of younger participants and 34% of older participants achieved ceiling performance across conditions, indicating that age was not the predominant reason for ceiling level performance. A repeated measures general linear models analysis was also conducted on DMS response times with group (NC, LTLE, RTLE) as the independent variable and delay (2 s, 30 s, 60 s) as the repeated measure. There was a significant main effect of delay, F(2, 88) = 39.06, p < .001 (response times increased across delay conditions), but the main effect of group and the interaction between group and delay were not significant. Story Recall Cue-present 2 30 60 Delays (seconds) Figure 1. Spatial delayed response: Mean error scores and standard errors for each group at each delay. Asterisks denote a significant difference from the normal control group. Data from immediate and delayed recall trials were analyzed using a repeated measures general linear models analysis with group (NC, LTLE, RTLE) as the independent variable and delay (immediate, delayed recall) as the repeated measure. The dependent measure was the number of verbatim points plus paraphrase points obtained at recall. 58 HERSHEY, CRAFT, GLAUSER, AND HALE A significant effect of delay, F(2, 44) = 30.15, p < .01 (immediate recall greater than delayed recall) was obtained, but the effect of group and the interaction were not significant (see Figure 2). Confabulation errors were also analyzed with the same repeated measures analysis as described previously. This analysis revealed a significant effect of delay on number of confabulations during recall, F(l, 44) = 9.64, p < .05, with more confabulatory responses present in delayed recall than in immediate recall. No effect of group or interaction between group and delay was obtained. Pattern Recall Data from immediate and delayed recall trials were analyzed using a repeated measures general linear models analysis with group (NC, LTLE, RTLE) as the independent variable and delay (immediate and delayed recall) as the repeated variable. The dependent measure was the number of correctly placed boxes (out of 12) with a penalty of 1 point for every extra box (above 12) that was marked. This type of error occurred equally frequently across groups. Analyses were conducted on both penalized and unpenalized scores; the results were the same. The results reported here are for the penalized scores. A significant main effect for group, F(2, 44) = 4.52, p < .05, was obtained, but the main effect for delay was not significant. The interaction between group and delay was borderline significant, F(2, 44) = 3.13, p = .05. Repeated measures general linear models analyses were carried out on pairs of groups (NC and LTLE, NC and RTLE, LTLE and RTLE). These analyses revealed that the interaction between group and delay was present when comparing the normal control group against the LTLE group, F(l,32) = 5.11,p< .05, but not when comparing the NC against the RTLE groups or when comparing two epilepsy groups against each 30 _, 25 - 20 - 15 - 10 - Normal Control 11 E 10 5 1 9 * 8- y 7- . E 6 - Normal Control Left Temporal Z Right Temporal Immediate Recall Delayed Recall Figure 3. Pattern recall: Mean number of correctly recalled pattern elements and standard errors for each group at immediate and delayed recall conditions. Asterisks denote a significant difference from the normal control group. other. Finally, general linear models analyses were conducted on all groups on each condition separately. Strong group effects were found for the immediate recall condition only, F(2, 44) = 5.83, p < .01. Post hoc Bonferroni corrected t tests were conducted on immediate recall scores that revealed that both epilepsy groups scored significantly lower than the NC group on immediate recall (see Figure 3). Verbal Span A repeated measures general linear models analysis was performed on verbal span scores with group (NC, LTLE, RTLE) as the independent variable and condition (without interference, with interference) as the repeated measure. This analysis revealed a significant effect of condition, F(l, 44) = 41.26, p < .01 (with interference < without interference), and group, F(2, 44) = 4.14, p < .05. The interaction between group and condition was nonsignificant. Bonferroni corrected post hoc comparisons between pairs of groups revealed that the RTLE group performed significantly worse than the NC group on the with interference condition. The LTLE group was impaired relative to the NC group at a trend level on the with interference condition (p = .07; see Table 4). Left Temporal Right Temporal Spatial Span 5 - Immediate Recall Delayed Recall Figure 2. Story recall: Mean bits recalled and standard errors for each group at immediate and delayed recall conditions. A repeated measures general linear models analysis was performed on spatial span scores with group (NC, LTLE, RTLE) as the independent variable and condition (without interference, with interference) as the repeated measure. The analysis revealed a significant effect of condition, F(2,44) = 127.90, p < .01 (with interference < without interference; see Table 4), but no effect of group. However, due to the 59 MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION Table 4 Means and Standard Deviations of Span Task Performance by Group Task Verbal span No interference Interference Spatial span No interference Interference Normal control (n = 19) Left temporal (" = 15) Right temporal (n = 13) M SD M SD M SD 10.8 9.4 2.3 2.5 10.1 7.8** 2.1 2.3 9.3 6.3* 2.7 3.3 10.3 6.6 3.2 4.1 7.7** 4.3** 2.7 2.7 8.5*** 4.9*** 3.5 3.5 *p < .05, a significant difference from the normal control group. **p < .07, different from normal control group, trend level. ***/> < .09, different from normal control group when outlier is removed, trend level. effects in the verbal span task, and the apparently lower performance of the epilepsy groups compared to controls in this task, exploratory comparisons were performed between each epilepsy group and the control group. For the left temporal group, performance on both conditions was different from controls at a trend level (ps < .07). Although the right temporal group's mean scores were generally equivalent to the left temporal group, their standard deviations were higher. When the data were inspected on a participantby-participant basis, an outlier was discovered. When this participant's data were removed, there was a trend level difference between this revised group and the control group for both conditions (ps < .09). Response Inhibition Task Two participants (1 in the LTLE group and 1 in the RTLE group) had missing data on this task due to technical problems. A repeated measures general linear models analysis was conducted on response inhibition median reaction times with group (NC, LTLE, RTLE) as the independent variable and condition (alone, congruent, discongruent) as the repeated measure. This analysis revealed a significant effect of condition, F(2, 42) = 78.32, p < .01, but no main effect of group and no interaction between group and condition. All conditions were significantly different from each other, with average reaction time increasing across conditions (alone, congruent, discongruent; see Figure 4). A repeated measures general linear models analysis was conducted on accuracy rates with group (NC, LTLE, RTLE) as the independent variable and condition (alone, concordant, discordant) as the repeated measure. This analysis revealed that the main effect of group was not significant, but the main effect for condition was significant, F(2, 42) = 10.27, p < .01. Participants were significantly more accurate in the alone condition as compared to the discongruent condition, and in the congruent condition as compared to the discongruent condition. The difference between the alone and congruent conditions was not significant. The interaction between group and condition was not significant. RTLE) as the independent variable. This analysis revealed a significant effect of group, F(2, 44) = 9.56, p < .01. Post hoc Bonferroni corrected comparisons revealed that the two epilepsy groups scored significantly lower than the NC group but were not significantly different from each other, although the RTLE group had relatively lower scores than the LTLE group (see Table 1). A general linear models analysis was also conducted on Block Design scaled scores with group (NC, LTLE, RTLE) as the independent variable. The main effect of group was not significant (see Table 1). To understand the possible relationship between IQ and performance on memory tasks, we conducted Pearson correlations between Information scaled scores and performance on the conditions of the SDR and pattern recall tasks that demonstrated significant group differences. For all three groups, these correlations were nonsignificant. Clinical Variables Age of onset was also correlated with all task performance variables to determine its effect. None of these 900 -, 800 - 700 - 600 - 500 - 400 - • • A Normal Control Left Temporal Right Temporal 300 0 General Cognitive Measures A general linear models analysis was conducted on Information scaled scores with group (NC, LTLE, and Alone Congruent Discongruent Figure 4. Response inhibition: Median reaction times and standard errors for each group by condition. 60 HERSHEY, CRAFT, GLAUSER, AND HALE correlations were significant for either epilepsy group or for both groups combined. Age at first risk factor was also correlated with task performance variables. These correlations were conducted in an effort to determine if the timing of the first insult to the brain is associated with performance in children with epilepsy. These correlations were not significant. Thus, in this sample, neither age at first insult nor age at first seizure was associated with cognitive functioning. The nonsignificance of these correlations could be affected by our relatively small sample sizes and the wide age ranges. Because age has a strong effect on cognitive functioning, it may overpower any more subtle effects of these clinical variables. Finally, to determine the effect of medication dosage on performance, we correlated total daily dose with select performance variables (SDR, pattern recall, and story recall) for children only on Tegretol (n = 18). None of these correlations was significant. Thus, it is unlikely that medication dosage alone can account for any group differences. Discussion The present study examined the pattern of short- and long-term memory function in children with early-onset TLE with two tasks used extensively in animal work (SDR and DMS) as well as with a supporting battery of clinical and experimental measures. When the data from all tasks are considered (see Table 5), the results can be grouped into three major findings: (a) Children with focal TLE were not impaired on short-delay memory tasks associated with the prefrontal cortex working memory system; their performance was variable on short-term memory tasks with heavier working memory demands, (b) Children with focal TLE were impaired on spatial tasks with high memory loads or long delays, demand characteristics that have been previously associated with the medial temporal memory system (Gabrieli, Keane, & Stebbins, 1993; Squire, 1992). (c) Children with focal TLE were less impaired on comparable verbal medial temporal-related memory tasks. Variably Spared Short-Term Memory The primary hypothesis of this study was that children with early-onset TLE would show short- and long-term memory deficits due to developmental disruption of the medial temporal-prefrontal memory system. On the tasks most closely linked to prefrontal cortex and short-term memory in animals and humans (short-delay conditions on SDR and DMS), this hypothesis was not supported. Childhood TLE did not affect short-term memory performance, but it did affect longer term memory on the SDR task. This pattern is consistent with the performance of adult monkeys and humans with medial temporal damage on spatial delayed response tasks (Backer Cave & Squire, 1992; Kowalska, 1995; Rains & Milner, 1994; Zola-Morgan & Squire, 1985). Ceiling effects on our version of the DMS impeded our ability to detect any effects using this paradigm. Thus, it is unlikely that early temporal lobe dysfunction affects the development of prefrontally mediated short-term memory as measured by these two tasks. However, on the span tasks, a more complex pattern was evident. Children with TLE were unimpaired on simple verbal span (no interference condition) relative to controls, but they were impaired on simple spatial span (trend level significance). All three groups performed better on the verbal span task than on the spatial span task, indicating that manipulating the spatial material was inherently more demanding than manipulating the verbal material. When a dual task (interference condition) was added to the span tasks, the children with TLE performed poorly with both types of material compared to controls. It is possible that the more demanding nature of the spatial span task overloaded the prefrontally mediated short-term memory system, even without an added interference condition. This possibly is consistent with the following discussion of other high-load or long-delay spatial tasks. Spatial Medial Temporal-Related Memory Deficits The SDR task, long-delay condition only, pattern recall task, and spatial span with interference all have heavy demands on the declarative memory system. It is not surprising that participants who have difficulty holding one location on-line for 60 s (as in the SDR task) also have difficulty holding 12 locations on-line for 10-15 s (as in the pattern recall task) or 4 to 5 locations under dual task conditions (spatial span with interference). Gabrieli and Table 5 Summary of Task Performance by Seizure Groups Relative to Controls Left temporal (n = 15) Right temporal (n = 13) SDR DMS Impaired at 60-s delay Impaired at 60-s delay Story recall Pattern recall • — Impaired— immediate recall Impaired— interference condition2 Impaired" Task Verbal span Spatial span Response inhibition Information Block design — — — Impaired—immediate recall Impaired— interference condition Impaired3 — Lower Lower — Note. SDR = spatial delayed response; DMS = delayed match to sample. "Trend level effect. — — MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION 61 colleagues (1993) reported that patients with amnesia due to Consortium, 1995; Novelly et al., 1984). Of the three medial temporal damage performed adequately on a lowload short-term memory task, but they were impaired on a high-load short-term memory task. The researchers speculated that the medial temporal lobe system does play a role in short-term memory tasks, particularly when the information load exceeds what they call "primary memory buffers in frontal and other cortical regions" (p. 1002). Similar ideas published studies on the memory skills of children with TLE, one found the same pattern as adults (Fedio & Mirsky, 1969) and the other two found a similar pattern, although less distinct (Cohen, 1992; Jambaque et al., 1993). However, have also been proposed by Eichenbaum et al. (1994), who stated that the parahippocampal gyrus may play the role of intermediate memory, holding information on-line that the neocortical short-term memory system cannot, either due to delay length or capacity limitations. Based on these speculations, children with TLE would be impaired on short-term memory tasks compared to normal controls, but only under high memory demands. When children are required to hold a large amount of information on-line for later recall, the immature prefrontal memory system's capacity may be overwhelmed. The information would then be held on-line by the medial temporal lobe memory system, which, in the case of children with TLE, is impaired and is thus unable to accurately handle the information. It may be that in the domain of memory, early medial temporal damage does not affect the prefrontal cortex or tasks that can be performed exclusively in that region. However, due to the immaturity of the prefrontal cortex in children, certain memory tasks may not be handled as well or as exclusively by the prefrontal cortex and may rely more on earlier developed and closely connected aspects of the memory system, such as the medial temporal region. Thus, the patterns of impairment on memory tasks that involve both regions are different from those seen in adults with fully developed cortex and dysfunctional medial temporal regions. As these children undergo the development of their prefrontal cortex, we speculate that they would demonstrate less impairment on some of the less demanding "frontal" memory tasks, such as the simple spatial span task. Relatively Intact Verbal Medial Temporal-Related Memory Skills Children with TLE were impaired on verbal span with interference but not on a traditional and well-validated verbal declarative memory task, story recall. Interestingly, many types of focal, developmental injuries to either the left or right hemisphere result in greater impairment on spatial tasks than on verbal tasks (Stiles & Thai, 1993). Thus, it is not surprising that our left and right temporal lobe seizures groups performed equivalently across a wide variety of spatial and verbal tasks. In contrast, many studies of adults with unilateral TLE have supported the idea of the lateralization of material-specific memory deficits. Generally, LTLE is associated with verbal delayed memory deficits, and RTLE is associated with visuospatial delayed memory deficits (Novelly et al., 1984; Ojemann & Dodrill, 1985; Saykin et al., 1989). Differences between unilateral TLE groups on visuospatial memory tasks are generally more difficult to document (Barr, & The Bozeman Epilepsy this first study had significant differences between groups in seizure severity (left temporal more severe than right temporal), the second study had significant differences between groups in age at time of testing (left temporal younger than right temporal), and the third study had one very small group (n = 6) making their results somewhat questionable. It is conceivable that in the first two studies the left temporal groups appeared more unpaired on verbal memory in part due to their greater severity and younger age at time of testing. In addition, children with TLE in our study had lower Information subtest scaled scores than the NCs, although they were still within the average range. The Information subtest is thought to be an estimate of general verbal intelligence and is itself a measure of semantic memory. It could be argued that performance on this test does not reflect a deficit in either area as much as it does a side effect of having a chronic illness, which may cause children to miss school more than their peers. This phenomenon has been noted in children with other types of chronic illnesses (Ryan, 1990). However, it is possible that the significant differences obtained between groups on memory tasks are explained simply by differences in verbal intellectual level or semantic memory, or the differences are exaggerated by the high level of verbal functioning of the NCs rather than reflecting impaired memory for the epilepsy groups. Several points addressing this possibility can be made. First, the NC group was matched to epilepsy participants on parents' years of education and on gender. Mean parents' years of education was comparable among all groups. We did not match participants on intelligence scores due to the fact that intelligence is considered to be an outcome measure of seizure disorder. Matching according to outcome variables has been criticized for creating inappropriate control groups (Meehl, 1970). Second, there were no significant correlations between Information scaled scores and key variables within each group. Thus, better performance on a verbal intelligence test was not associated with better performance on the spatial memory task for any participant group. Conclusion In conclusion, although the organization of memory systems within the adult brain has received tremendous attention in recent decades, the growth and refinement of these memory systems have been less intensively studied. The present study addressed the separable nature of shortand long-term memory in a population with early temporal lobe dysfunction. The results indicated that early-onset TLE affects short- and long-term memory differently across certain task variables. Short-term memory performance as measured by a spatial delayed response task was not affected in children with TLE, but performance at a longer delay on 62 HERSHEY, CRAFT, GLAUSER, AND HALE the same task was impaired, consistent with findings in adults. Further, although children with both left and right TLE were largely impaired on spatial memory tasks that had high memory loads or long delays, they were relatively unimpaired on comparable verbal tasks. This pattern of impairment differs qualitatively from findings in adults with early or late medial temporal lobe damage in whom sparing of immediate recall, impairment in verbal memory, and some material-specific patterns of impairments are seen. These differences may be due to an interaction between the immaturity of the prefrontal cortex and the dysfunction of the medial temporal region in the mediation of short- and long-term declarative memory. References Aggleton, J. P., Nicol, R. M., Huston, A. E., & Fairbairn, A. F. (1988). The performance of amnesic subjects on tests of experimental amnesia in animals: Delayed matehing-to-sample and concurrent learning. Neuropsychologia, 26(2), 265-272. Alvarez, P., Zola-Morgan, S., & Squire, L. R. (1994). The animal model of human amnesia: Long-term memory impaired and short-term memory intact. Proceedings of the National Academy of Sciences, 91, 5637-5641. Angeli, S. J., Murray, E. A., & Mishkin, M. (1993). Hippocampectomized monkeys can remember one place but not two. Neuropsychologia, 31(W), 1021-1030. Bachevalier, J. (1990). Ontogenetic development of habit and memory formation in primates. In A. Diamond (Ed.), Annals of the New York Academy of Sciences, Vol. 608, The Development and Neural Basis of Higher Cognitive Functions (pp. 457—484). New York: New York Academy of Sciences. Bachevalier, J. (1994). Medial temporal lobe structures and autism: A review of clinical and experimental findings. Neuropsychologia, 32(f>), 627-648. Bachevalier, J., & Mishkin, M. (1989). Mnemonic and neuropathological effects of occluding the posterior cerebral artery in Macaco mulatto. Neuropsychologia, 27(1), 83-105. Backer Cave, C, & Squire, L. R. (1992). Intact verbal and nonverbal short-term memory following damage to the human hippocampus. Hippocampus, 2(2), 151-164. Baddeley, A. (1992). Working memory: The interface between memory and cognition. Journal of Cognitive Neuroscience, 4(3), 281-288. Barr, W. B., & The Bozeman Epilepsy Consortium. (1995). The right temporal lobe and memory: A critical reexamination, Journal of the International Neuropsychological Society, 1, 136. Bauer, R. H., & Fuster, J. M. (1976). Delayed-matching and delayed-response deficit from cooling dorsolateral prefrontal cortex in monkeys. Journal of Comparative and Physiological Psychology, 90(3), 293-302. Bilder, R. M., Bogerts, B., Ashtari, M., Wu, H., Alvir, J. M., Jody, D., Reiter, G., Bell, L., & Lieberman, J. A. (1995). Anterior hippocampal volume reductions predict "frontal lobe" dysfunction in first episode schizophrenia. Schizophrenia Research, 77(1), 47-58. Chugani, H. T., Phelps, M. E., & Mazziotta, J. C. (1987). Positron emission tomography study of human brain functional development. Annals of Neurology, 22, 487^97. Cohen, M. (1992). Auditory/verbal and visual/spatial memory in children with complex partial epilepsy of temporal lobe origin. Brain and Cognition, 20, 315—326. Craft, S., Zallen, G., & Baker, L. D. (1992). Glucose and memory in mild senile dementia of the Alzheimer type'. Journal of Clinical and Experimental Neuropsychology, 14, 253—267. Delaney, R. C., Prevey, M. L., & Mattson, R. H. (1982). Short-term retention with lateralized temporal lobe epilepsy. Cortex, 22, 581-600. Delaney, R. C., Rosen, A. J., Mattson, R. H., & Novelly, R. A. (1980). Memory function in focal epilepsy: A comparison of non-surgical, unilateral temporal lobe and frontal lobe samples. Cortex, 16, 103-117. Diamond, A. (1990). Rate of maturation of the hippocampus and the developmental progression of children's performance on the delayed non-matching to sample and visual paired to comparison tasks. In A. Diamond (Ed.), Annals of the New York Academy of Sciences: Vol. 608, The Development of Neural Basis of Higher Cognitive Functions (pp. 394-433). New York: New York Academy of Sciences. Ebersole, J. S., & Pacia, S. V. (1996). Localization of temporal lobe foci by ictal EEC patterns. Epilepsia, 37(4), 386-399. Eichenbaum, H., Otto, T., & Cohen, N. J. (1994). Two functional components of the hippocampal memory system. Behavioral and Brain Sciences, 17, 449-518. Fedio, P., & Mirsky, A. F. (1969). Selective intellectual deficits in children with temporal lobe or centrencephalic epilepsy. Neuropsychologia, 7, 287-300. Flavell, J. H. (1977). Cognitive development. Englewood Cliffs, NJ: Prentice Hall. Freedman, M., & Oscar-Berman, M. (1986). Bilateral frontal lobe disease and selective delayed response deficits in humans. Behavioral Neuroscience, 100(3), 337-342. Friedman, H. R., & Goldman-Rakic, P. S. (1991). The circuitry of working memory revealed by anatomy and metabolic imaging. In H. S. Levin, H. M. Eisenberg, & A. L. Benton (Eds.), Frontal lobe function and dysfunction (pp. 72-91). New York: Oxford University Press. Funahashi, S., Bruce, C. J., & Goldman-Rakic, P. S. (1993). Dorsolateral prefrontal lesions and oculomotor delayed-response performance: Evidence for mnemonic "scotomas." The Journal of Neuroscience, 13(4), 1479-1497. Fuster, J. M. (1990). Prefrontal cortex and the bridging of temporal gaps in the perception-action cycle. In A. Diamond (Ed.), Annals of the New York Academy of Sciences: Vol. 769, The Development and Neural Basis of Higher Cognitive Functions (pp. 318-336). New York: New York Academy of Sciences. Gabrieli, J. D. E., Keane, M. M., & Stebbins, G. T. (1993). Reduced working memory capacity in patients with global amnesia: Evidence for a limbic/diencephalic contribution to working memory performance. Society for Neuroscience Abstracts, 19, 1002. Goldman-Rakic, P. S. (1987). Circuitry of primate prefrontal cortex and regulation of behavior by representational memory. In J. Mills & V. G. Mountcastle (Eds.), Handbook of physiology: The nervous system (pp. 373^17). Baltimore: Williams & Wilkins. Goldman-Rakic, P. S., Selemon, L. D., & Schwartz, M. L. (1984). Dual pathways connecting the dorsolateral prefrontal cortex with the hippocampal formation and parahippocampal cortex in the rhesus monkey. Neuroscience, 12(3), 719-743. Hale, S., Myerson, J., Rhee, S. H., Weiss, C. S., & Abrams, R. A. (1996). Selective interference with the maintenance of location information in working memory. Neuropsychology, 10(2), 228240. Huttenlocher, P. R. (1990). Morphometric study of human cerebral cortex development. Neuropsychologia, 28(6), 517-527. MEMORY IN EARLY TEMPORAL LOBE DYSFUNCTION Jambaque, I, Dellatolas, G., Dulac, O., Ponsot, G., & Signoret, J. (1993). Verbal and visual memory impairment in children with epilepsy. Neuropsychologia, 31(11), 1321-1337. Janowsky, J. S. (1992). The development and neural basis of memory systems. In M. H. Johnson (Ed.), Brain development and cognition: A reader (pp. 665-678). Oxford, England: Basil Blackwell. Joyce, E., & Robbins, T. W. (1991). Frontal lobe function in Korsakoff and non-Korsakoff alcoholics: Planning and spatial working memory. Neuropsychologia, 29(8), 709-723. Kail, R. (1979). Use of strategies and individual differences in children's memory. Developmental Psychology, 15, 251-255. Karvounis, P. C., Chiu, J. C, Parsa, K., & Gilbert, S. (1970). Agenesis of temporal lobe and arachnoid cyst. New York State Journal of Medicine, 70(18), 2349-2353. Kowalska, D. M. (1995). Effects of hippocampal lesions on spatial delayed responses in dog. Hippocampus, 5, 363-370. Lang, C., Lehrl, S., & Huk, W. (1981). A case of bilateral temporal lobe agenesis. Journal of Neurology, Neurosurgery and Psychiatry, 44, 626-630. Lavadas, E., Umilta, C., & Provincial;, L. (1979). Hemispheredependent cognitive performances in epileptic patients. Epilepsia, 20, 493-502. Leonard, B. W., Amaral, D. G., Squire, L. R., & Zola-Morgan, S. (1995). Transient memory impairment in monkeys with bilateral lesions of the entorhinal cortex. The Journal of Neuroscience, 75(8), 5637-5659. Luciana, M., Depue, R. A., Arbisi, P., & Leon, A. (1992). Facilitation of working memory in humans by a D2 dopamine receptor agonist. Journal of Cognitive Neuroscience, 4(1), 58-68. Mahut, H., & Moss, M. (1984). The monkey and the sea horse. In R. L. Isaacson & K. H. Pribram (Eds.), The hippocampus (Vol. 4, pp. 241-279). New York: Plenum Press. Mathern G. W., Pretorius, J. K., & Babb, T. L. (1995). Influence of the type of initial precipitating injury and at what age it occurs on course and outcome in patients with temporal lobe seizures. Journal of Neurosurgery, 82, 220-227. McMillan, T. M., Powell, G. E., Janota, L, & Polkey, C. E. (1987). Relationships between neuropathology and cognitive functioning in temporal lobectomy patients. Journal of Neurology, Neurosurgery and Psychiatry, SO, 167-176. Meehl, P. (1970). Nuisance variables and the ex post facto design. In M. Radner & S. Winokur (Eds.), Minnesota studies in the philosophy of science (pp. 373—402). Minneapolis: University of Minnesota Press. Mishkin, M., & Murray, E. A. (1994). Stimulus recognition. Current Opinion in Neurobiology, 4, 200-206. Muri, R. M., Rivaud, S., Timsit, S., Cornu, P., & PierrotDeseilligny, C. (1994). The role of the right medial temporal lobe in the control of memory-guided saccades. Experimental Brain Research, 101, 165-168. Newcomer, J. W., Craft, S., Hershey, T, Askins, K., & Bardgett, M. E. (1994). Glucocorticoid-induced impairment in declarative memory performance in adult humans. Journal of Neuroscience, 14(4-), 2047-2053. Novelly, R. A., Augustine, E. A., Mattson, R. H., Glaser, G. H., Williamson, P. D., Spencer, D. D., & Spencer, S. S. (1984). Selective memory improvement and impairment in temporal lobectomy for epilepsy. Annals of Neurology, 15, 64-67. Ojemann, G. A., & Dodrill, C. B. (1985). Verbal memory deficits after left temporal lobectomy for epilepsy: Mechanism and intraoperative prediction. Journal of Neurosurgery, 62, 101-107. 63 Ostergaard, A. L. (1987). Episodic, semantic and procedural memory in a case of amnesia at an early age. Neuropsychologia, 25(2), 341-357. Overman, W. H., Ormsby, G., & Mishkin, M. (1990). Picture recognition versus picture discrimination learning in monkeys with medial temporal removals. Experimental Brain Research, 79, 18-24. Owen, A. M., Sahakian, B. J., Semple, J., Polkey, C. E., & Robbins, T. W. (1995). Visuospatial short-term recognition memory and learning after temporal lobe excisions, frontal lobe excisions or amygdalo-hippocampectomy in man. Neuropsychologia, 33(1), 1-24. Perret, E. (1974). The left frontal lobe of man and the suppression of habitual responses in verbal categorical behavior. Neuropsychologia, 12, 323-330. Prevey, M. L., Delaney, R. C., Mattson, R. H., Cattanach, L., Spencer, S. S., Kim, J. H., & Spencer, D. D. (1994, February). Verbal short-term encoding in temporal lobe epilepsy: Comparison of patients with left temporal lobe lesions versus hippocampal sclerosis. Paper presented at the 22nd Annual Meeting of the International Neuropsychological Meeting, Cincinnati, OH. Prisko, L. (1963). Short-term memory in focal cerebral damage. Unpublished doctoral dissertation, McGill University, Montreal, Canada. Rains, G. D., & Milner, B. (1994). Right-hippocampal contralateralhand effect in the recall of spatial location in the tactual modality. Neuropsychologia, 32(10), 1233-1242. Ryan, C. M. (1990). Neuropsychological consequences and correlates of diabetes in childhood. In C. S. Holmes (Ed.), Neuropsychological and behavioral aspects of diabetes (pp. 58-84). New York: Springer-Verlag. Samuels, I., Butters, N., & Fedio, P. (1972). Short-term memory disorders following temporal removals in humans. Cortex, 8, 283-298. Saykin, A. J., Gur, R. C., Sussman, N. M., O'Conner, M. J., & Our, R. E. (1989). Memory deficits before and after temporal lobectomy: Effect of laterality and age of onset. Brain and Cognition, 9, 191-200. Saykin, A. J., Robinson, L. J., Stafiniak, P., Kester, D. B., Gur, R. C., O'Connor, M. J., & Sperling, M. R. (1992). Neuropsychological changes after anterior temporal lobectomy: Acute effects on memory, language and music. In T. L. Bennet (Ed.), The neuropsychology of epilepsy (pp. 263-290). New York: Plenum Press. Schacter, D. L., Chiu, C. Y, & Ochsner, K. N. (1993). Implicit memory: A selective review. Annual Review of Neuroscience, 16, 159-182. Sidman, M., Stoddard, L. T, & Mohr, J. P. (1968). Some additional quantitative observations of immediate memory in a patient with bilateral hippocampal lesions. Neuropsychologia, 6, 245-254. Squire, L. R. (1992). Memory and the hippocampus: A synthesis from findings with rats, monkeys, and humans. Psychological Review, 99(2), 195-231. Squire, L. R., Knowlton, B., & Musen, G. (1993). The structure and organization of memory. Annual Review of Psychology, 44, 453^95. Squire, L. R., Shimamura, A. P., & Graf, P. (1987). Strength and duration of priming effects in normal subjects and amnestic patients. Neuropsychologia, 25, 195—210. Squire, L. R., Zola-Morgan, S., & Chen, K. S. (1988). Human amnesia and animal models of amnesia: Performance of amnesic patients on tests designed for the monkey. Behavioral Neuroscience, 102(2), 210-221. Stiles, J., & Thai, D. (1993). Linguistic and spatial cognitive development following early focal brain injury. In M. H. 64 HERSHEY, CRAFT, GLAUSER, AND HALE Johnson (Ed.), Brain development and cognition: A reader (pp. 643-664). Oxford, England: Basil Blackwell. Strauss, E., Hunter, M., & Wada, J. (1993). Wisconsin Card Sorting Task: Effects of age of onset of damage and laterality of dysfunction. Journal of Clinical and Experimental Neuropsychology, 75(6), 896-902. Tonsgard, J. H., Harwicke, N., & Levine, S. C. (1987). KluverBucy syndrome in children. Pediatric Neurology, 3(3), 162-165. Trenerry, M. R., Jack, C. R., Ivnik, R. J., Sharbrough, F. W., Cascino, G. D., Hirschom, K. A., Marsh, W. R., Kelly, P. J., & Meyer, F. B. (1993). MRI hippocampal volumes and memory function before and after temporal lobectomy. Neurology, 43, 1800-1805. Tulving, E., Kapur, S., Craik, F. I., Moscovitch, M., & Houle, S. (1994). Hemispheric encoding/retrieval asymmetry in episodic memory: Positron emission tomography findings. Proceedings of the National Academy of Sciences of the United States of America, 91(6), 2016-2020. Wechsler, D. (1987). Wecksler Memory Scale—Revised Manual. San Antonio, TX: Psychological Corp. Wechsler, D. (1991). Wechsler Intelligence Scale for Children (3rd ed.). Cleveland, OH: Psychological Corp. Wilson, F. A. W., Scalaidhe, S. P. O., & Goldman-Rakic, P. S. (1993). Dissociation of object and spatial processing domains in primate prefrontal cortex. Science, 260, 1955-1958. Winocur, G. (1992). The hippocampus and prefrontal cortex in learning and memory: An animal model approach. In L. R. Squire & N. Butters (Eds.), Neuropsychology of memory (pp. 429-439). New York: Guilford Press. Wishart, H. A., Warmflash, V., Barr, W. B., & Schaul, N. (1995, February). A moderating effect of age at seizure onset in childhood on relations between focus site and memory in epilepsy surgery candidates. Paper presented at the 23rd Annual Meeting of the International Neuropsychological Society, Seattle, WA. Wood, F. B., Brown, I. S., & Felton, R. H. (1989). Long-term follow-up of a childhood amnesic syndrome. Brain and Cognition, 10, 76-86. Zaidel, D. W., Esiri, M. M., & Oxbury, J. M. (1993). Regional differentiation of cell densities in the left and right hippocampi of epileptic patients. Journal of Neurology, 240, 322-325. Zola-Morgan, S., & Squire, L. R. (1985). Medial temporal lesions in monkeys impair memory on a variety of tasks sensitive to human amnesia. Behavioral Neuroscience, 99, 22-34. Received February 15, 1996 Revision received April 28, 1997 Accepted May 5, 1997 AMERICAN PSYCHOLOGICAL ASSOCIATION SUBSCRIPTION CLAIMSINFORMATION Today's Date:_ WE provide this form to assist members, institutions, and nonmember individuals with any subscription problems. With the appropriate information we can begin a resolution. If you use the services of an agent, please do NOT duplicate claims through them and directly to us. PLEASE PRINT CLEARLY AND IN INK IF POSSIBLE. PRINT FULL NAME C« KEY NAME OF INSTITUTION MEMBERORCUSTOMEKNUMBER (MAYBE FODM) ON ANYPASTKSIJE LABEL) DATE YOUR ORDER WAS MAILED (OR PHONED) _CHECK -CHARGE CHECIOCARD CLEARED DATE:_ CITY STATE/COUHTRY YOUR NAME AND PHOHE NUMBER TITLE (K potable, send a copy, from and bide, of your cancelled check to htb us in our research of your claim.) ISSUES: MISSING DAMAGED VOLUME OR YEAR NUMBER OR MONTH Thank you. Ottfe a claim is received and rtsobed, delivery of replacement issues routinely takes 4-6 weeks. —_^——. (TO BE FILLED OUT BY APA STAFF) —^^^^—^^^— DATE RECEIVED: ACTION TAKEN: _ STAFF NAME: DATE OF ACTIONt _ INV.NO.&DATE: LABEL NO. &DATEi_ Send this form to AFA Subscription Claims, 750 First Street, ME, Washington, DC 20002-4242 PLEASE DO NOT REMOVE. A PHOTOCOPY MAY BE USED.