Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Perivascular space wikipedia , lookup
Central pattern generator wikipedia , lookup
Microneurography wikipedia , lookup
Alzheimer's disease wikipedia , lookup
Time perception wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Environmental enrichment wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Neuroeconomics wikipedia , lookup
Aging brain wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Embodied language processing wikipedia , lookup
Anatomy of the cerebellum wikipedia , lookup
Muscle memory wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Synaptic gating wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Parkinson's disease wikipedia , lookup
Cerebral cortex wikipedia , lookup
Substantia nigra wikipedia , lookup
Motor cortex wikipedia , lookup
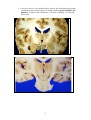
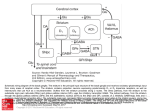
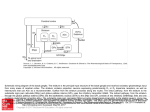
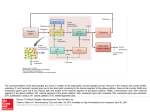
Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. Marcjh 8, 2011 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 THE BASAL GANGLIA Objectives: 1. What are the main manifestations of Basal Ganglia disease? 2. Be able to contrast signs and symptoms of: • Basal Ganglia Disease • Cerebellar Disease • Corticospinal Tract Disease = Upper motor neuron • Motor Neuron Disease = Lower Motor neuron 3. Identify the structures involved in: • Huntington's Disease • Parkinson's Disease I. Introduction A. General features of the basal ganglia, one of our 3 major motor control centers: 1. Involved in motor, cognitive and affective tasks 2. Do not project directly to targets below the midbrain 3. Act mainly on the premotor cortex via the thalamus, similar to cerebellum. B. What Do the Basal Ganglia Do? 1. We are beginning to understand that there are more than 3 different loops or parallel circuits and functions (motor, cognitive and affective) all influenced by a dopaminergic mesencephalic system. 2. The only one we will focus on is the motor loop. Motor pattern generators permit voluntary movements to take place in what seems like an automatic manor. 3. Normally the BG are the “brakes” on the voluntary motor system. 4. Selectively facilitate some movements and inhibit others, and/or compare commands for movement from the precentral motor cortex with proprioceptive feedback from the movement in progress. 5. Play a role in initiating internally generated movements C. Definitions 1. Basal ganglia a. Corpus striatum 1. Caudate \ = the striatum 2. Putamen / 3. Globus pallidus = the pallidum b. Though technically not part of the basal ganglia, the subthalamic nucleus and substantia nigra are presented with the basal ganglia because of their connections and involvement in disease. 1 2. Lenticular nucleus is an old descriptive term for the lens-shaped gray matter just lateral to the internal capsule; it includes both the globus pallidus and putamen. Another term is lentiform, even more confusing. Avoid using either term. 2 From The Digital Anatomist Interactive Brain Syllabus. John Sundsten and Kate Mulligan, Univ. Washington School of Medicine. 1998 © Source: Kandel? 3 II. Connections of Basal Ganglia A. The caudate and putamen are a single entity that is divided by the anterior limb of the internal capsule. Both have similar connections, cell types and neurotransmitters. There is evidence that the caudate is more involved in cognitive functions and the putamen more with motor functions B. Striatal Afferents 1. From the Cerebral CORTEX: Corticostriate afferents Nearly every region of the cerebral cortex sends axons to the ipsilateral caudate and putamen. See diagram by Dr. Voron next page (a. Visual cortex projects to the tail of the caudate and cells there respond to complex patterned visual stimuli.) b. Frontal cortex projects to the head of the caudate; therefore, this part of the caudate responds to environmental stimuli that are important in preparing for movement. 2. From the SUBSTANTIA NIGRA: Nigrostriatal afferents. These neurons use dopamine as their neurotransmitter. See diagram by Dr. Voron next page C. Striatal Efferents – Globus Pallidus. See diagram by Dr. Voron next page D. Efferents to Thalamus: The Globus Pallidus – 1. Pallidothalamic axons terminate in thalamic nuclei. In different region from the axons coming from the cerebellum. Myelin stained section through thalamus and BG, Stensaas E. The Thalamic nuclei project to the premotor and supplementary cortex in front of the precentral gyrus. 4 F. The premotor and supplementary motor cortex is a region important in planning movements. 1. Premotor cortex is the part of area 6 on the lateral surface of the hemisphere in front of the precentral gyrus. 2. Supplementary motor cortex is the part of area 6 on the medial surface of the hemisphere. . 3. These areas then project to area 4 (the precentral gyrus), primary motor cortex and hence to the corticospinal tract. III. Striatal Motor Functions The striatum is thought to link sensory cues to motor behavior integrating nearly all the activity occurring in the cortex. 1. Many connections (subthalamus and globus pallidus, substantia © Stephen C. Voron, M.D., reciprocal 2004 nigra and striatum). Excitatory (Glu): 2. A role in initiating internally generated movements like associated movement when walking. Cortex, Subth Nuc, VL Thal 3. Interplay of inhibition and excitation results in normal motor behavior. Inhibitory (GABA): Interruption of either the Direct or Indirect pathways results in decrease or increase in movement. We call these diseases: Movement disorders GPe, Gpi/(SNr) which usually occur at rest. Striatum, Both inhibitory and excitatory: SNc: dopamine Striatum interneurons: ACh Indirect pathway Inhibits extraneous movement Direct pathway Facilitates intentional movement Excitatory (Glu): Cortex, Subth Nuc, VL Thal Inhibitory (GABA): Striatum, GPe, Gpi/(SNr) 5 IV. Basal Ganglia Diseases-Often called Involuntary Movement Disorders. There may be an increase or a decrease in movements depending on the disease and structures involved. A. Involuntary movements during wakefulness. In general there are POSITIVE (hyperkinetic) signs such as rigidity, chorea, athetosis, resting tremor, etc. In addition there are NEGATIVE (hypokinetic) sympto ms such as akinesia, bradykinesia, masked face, decreased blinking, loss of associated movements, difficulty planning movements. B. Basal ganglia disease is relatively common and results from release (or disinhibition), Suzanne Stensaas© C. Parkinson's disease was the first example of a neurological disorder with a molecular basis. It is a slowly progressive disorder characterized by bradykinesia (trouble initiating movement), festinating gait, resting tremor, lead pipe or cogwheel rigidity, and masked facies. . 1. Substantia nigra (pars compacta) contains pigmented dopaminergic neurons that project to the striatum; the dopamine has the general effect of facilitating movement. 2. In Parkinson's disease, >70% of dopaminergic neurons in the substantia nigra die. There is also neuronal loss in other monoaminecontaining nuclei, but the nigrostriatal dopamine loss is considered most important for the movement disorder. This loss in turn affects the direct pathway 3. L-DOPA therapy increases dopamine and provides significant improvement in movement in many patients. 6 D. Huntington's disease is an autosomal dominant disorder (CAG repeat) resulting in degeneration of cholinergic and inhibitory GABAergic neurons in the striatum and cerebral cortex, probably via glutamate-mediated excitotoxic mechanisms. Huntington's Disease usually includes choreoathetosis, dementia, and death within 10-20 years of the onset of symptoms. No specific treatment is available. Disease is often diagnosed after reproductive years reached and offspring produced. 7