Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Neuroanatomy wikipedia , lookup
Development of the nervous system wikipedia , lookup
Lateralization of brain function wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Environmental enrichment wikipedia , lookup
Dual consciousness wikipedia , lookup
Embodied language processing wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuroplasticity wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Time perception wikipedia , lookup
Emotional lateralization wikipedia , lookup
Metastability in the brain wikipedia , lookup
Muscle memory wikipedia , lookup
Human brain wikipedia , lookup
Central pattern generator wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Aging brain wikipedia , lookup
Basal ganglia wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
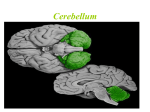
“ЗАТВЕРДЖЕНО” на методичній нараді кафедри нервових хвороб, психіатрії та медичної психології “______” _______________ 2008 р. Протокол № _____ Зав. кафедри нервових хвороб, психіатрії та медичної психології професор В.М. Пашковський METHODOLOGICAL INSTRUCTION №4 THEME: Cerebellum. Syndromes of it’s lesion. Modul 1. General neurology Сontents modul 1. introduction. symptoms of motor and sensory disturbanses Subject: Nervous deseases Year 4 Medical faculty Hours 2 Author of methodological instructions PhD, MD Zhukovskyi O.O. Chernivtsy 2008 1. Scientific and methodological substantiation of the theme. The cerebellum is a reflexional organ of coordination of movements, equilibrium and muscular tone. The functional of cerebellum and its pathology deserves notice of clinicians and contributors. The pathology of coordination system is observed at inflammatory, degenerative, hereditary processes and tumors. There are many links of cerebellum with different parts of the nervous system, which cause a lesion of the coordination system in various pathological processes. That’s why every doctor has to know the signs of lesion of coordination system. Correct and well-timed diagnostic – condition and warranty of rational therapy. 2. Aim: students should be able to determine independently lesion signs of cerebellum and its pathways, to localize the pathological process (focus) on different topical levels. Students should be able to formulate and to explain the topical diagnosis. Students must know: 1. Anatomical structures and function of the cerebellum and its pathways. 2. The function of the cerebellum: a) function of the worm; b) function of the hemisphere. 3. Clinical signs of cerebellar ataxia. 4. Classification of ataxias. 5. The signs of lesion of cerebellum and its pathway on different levels: - lesion of hemispheres; - lesion of worm; - lesion of the red nucleus; - lesion of cortex of frontal lobes of brain; - lesion of Pons. Students should be able to: 1. Collect the patient’s complaints (changes of gait and movements, posture, speech and handwriting, instability during walking) and to analyze them. 2. Examine patient’s neurological status: find out the symptoms of cerebellum’s lesion: giddiness, instability at standing and walking, clumsy discrepancy of purposeful movements, tremor of extremities at execution of exact movements, deterioration of vision, change of speech etc. 3. To carry out tests on synergy and coordination, change of speech, letter, muscles tone. 4. Make a conclusion about presence of pathology of cerebellar function. 5. To determine level of a lesion of the cerebellum. Make the topical diagnosis. Student should gain practical skills: 1. To indicate nystagmus; 2. To indicate scanning speech; 3. To check muscular hypotonia; 4. To check intention tremor; 5. To indicate dysmetria; 6. To find the impairment of equilibrium and gait; 7. To study asynergia; 8. To indicate macrographia; 9. To check adiadochokinesia; 10. To make difference between static and dynamic ataxia. 3. Educational aim. To indicate that the primary function of the cerebellum is to detect and correct errors in movement. Errors are detected by comparing movement commands from the cerebral cortex with movement-produced somatosensory feedback from the spinal cord and information about balance from the vestibular receptors in the inner ear. Errors are corrected by affecting the planning, timing, and coordination of muscular contractions. 4. Integration (basic level). Subjects Gained skills Anatomy Knowledge of anatomy structures of the cerebellum and its pathways: anatomy of cerebellum; the pathways of lower, middle and upper legs of cerebellum; the pathways of cerebellum’ correction. Histology Hystological structure of cerebellum and its pathways Physiology Knowledge of function of the cerebellum: the function of the worm, the function of the hemisphere. The cerebellum is located beneath the brain and overlies the dorsal aspect of the pons and medulla. It contains several functionally independent lobes covered by transversely oriented folia. The primary function of the cerebellum is to detect and correct errors in movement. Errors are detected by comparing movement commands from the cerebral cortex with movement-produced somatosensory feedback from the spinal cord and information about balance from the vestibular receptors in the inner ear. Errors are corrected by affecting the planning, timing, and coordination of muscular contractions during movement. The basal ganglia and cerebellum are important sub-cortical motor centers that function in parallel to help control movement. Because neither structure projects directly onto lower motor neurons, their influence in motor control is indirect. Both structures form subcortical feedback loops by receiving input from the cortex and projecting back to the cortex via the thalamus. However, these feedback loops have important functional differences. First, the basal ganglia project to the supplementary motor and prefrontal areas while the cerebellum projects to the premotor and primary motor areas. Second, the basal ganglia receive input from wider areas of the cerebral cortex than the cerebellum. Third, the basal ganglia receive no direct somatic input from the spinal cord while the cerebellum receives many direct projections from the spinal cord relaying movement-produced changes in sensory feedback. Fourth, the basal ganglia's sole access to lower motor neurons is via the cortex while the cerebellum has other more direct connections via the vestibular nuclei, reticular nuclei, and red nucleus. As the differences in projections would suggest, the cerebellum seems to be involved in the regulation of specific parameters of movement while the basal ganglia are thought to be involved in more complex aspects of motor planning. The cerebellum acts as a comparator of movement intention (as reflected in cortical output) with movement results (as reflected in the sensory consequences of movement). The cerebellum is responsible for controlling the timing, coordination of synergists, and background tone of a movement. The basal ganglia are responsible for initiating and scaling internally generated movements. Unlike the cerebellum with its primary role in motor control, the basal ganglia also participate in cognitive and limbic-related control systems. The cerebellum lesions make the syndrome of cerebellar ataxia. The signs of this syndrome are: a) nystagmus b) scanning speech c) muscular hypotonia d) intention tremor e) dysmetria f) impairment of equilibrium and gait g) asynergia h) macrographia i) adiadochokinesia. Lesion of warm. Static ataxia, trunk ataxia, “drunken gait”, hypotonia in extremities. At the given stage it is important to be able to differ such kinds of ataxia as: a) cerebellar (static or dynamic) b) frontal c) vestibular d) sensitive e) hysterical f) mixed Lesion of hemispheres of a cerebellum. Objectively: (+) of finger-nose and heel-knee tests, test on a diadochokinesis, index test, test “parsleys”, Ojyhovski test, (+) Babinski test on an asynergia of a trunk, (+) test on hypermetric of movements, (+) a manual Doynikov’s phenomenon. Lesion of a frontal lobe, cortex of a brain. All disturbances will be on the opposite party: an astasia, abasia, the ataxia will be on the opposite part. Lesion in the Pons Varoliy’s. The ataxia will be on the same party. Self assessment: 1. What are the signs of cerebellum worm lesion? 2. Where and what are observed at lesion of the right frontal lobe? 3. Where and what are observed at lesion of the right red nucleus? 4. The patient has cerebellar ataxia on right extremities. The lesion of what structures can cause such signs? 5. Name decussating of the cerebellar correction pathway. 6. Enumerate main functions of the cerebellum. 7. Name main functions of the cerebellum. 8. There are adiadochokinesis on right, intention tremor during the finger-nose test on the right. Where is the focus? 9. What is the name of the second neuron of the cerebellar correction pathway? 10.How much pairs of legs has cerebellum? 11.What is the function of cerebellum worm? 12.What is the function of cerebellum hemispheres? 13.Name the types of cerebellar ataxia? 14.Name the efferent path of the lower cerebellar leg? Tests 1. Lesion of the worm of cerebellum causes the appearance of ataxia: a) dynamic; b) vestubular; c) static; d) sensitive; e) frontal. 2. What test lets examine static ataxia? a) Shwabach’s; b) Ozhekhovsky; c) Romberg’s; d) Stuart-Holmes’s; e) Shilder’s. 3. Where is the focus of lesion when the patient has astasia-abasia? a) Occipital lobe; b) Frontal lobe; c) Temporal lobe; d) Upper parietal lobe; e) Lower parietal lobe. Real-life situations: 1. Patient has a tumor of the worm of a cerebellum. Describe clinical signs of worm lesion? 2. Describe the dicussation of specific ways of the cerebellar amendment? 3. List the basic functions of a cerebellum. References: 1. Basic Neurology. Second Edition. John Gilroy, M.D. Pergamon press. McGraw Hill international editions, medical series. – 1990. 2. Clinical examinations in neurology /Mayo clinic and Mayo foundation. – 4th edition. –W.B.Saunders Company, Philadelphia, London, Toronto. – 1976. 3. McKeough, D.Michael. The coloring review of neuroscience /D.Michael McKeough/ - 2nd ed. – 1995. 4. Neurology for the house officer. – 3th edition. – howard L.Weiner, MD and Lawrence P. Levitt, MD, - Williams&Wilkins. – Baltimore. – London. – 1980. 5. Neurology in lectures. Shkrobot S.I., Hara I.I. Ternopil. – 2008. 6. Van Allen’s Pictorial Manual of Neurologic Tests. – Robert L. Rodnitzky. 3th edition. – Year Book Medical Publishers, inc.Chicago London Boca Raton. - 1981.