Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Multielectrode array wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Aging brain wikipedia , lookup
Haemodynamic response wikipedia , lookup
Sex differences in intelligence wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Biology and sexual orientation wikipedia , lookup
Development of the nervous system wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Nervous system network models wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuroeconomics wikipedia , lookup
Metastability in the brain wikipedia , lookup
Optogenetics wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Neuroanatomy wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Channelrhodopsin wikipedia , lookup
Causes of transsexuality wikipedia , lookup
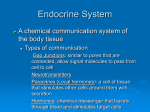
Ruth Wood, 1/21/16 NEUROENDOCRINE SYSTEMS & THE HYPOTHALAMUS "People tend to stay away from the hypothalamus. Most brain scientists (including myself until recently) prefer the sunny expanses of the cerebral cortex to the dark, claustrophobic regions at the base of the brain. They think of the hypothalamus- though they would never admit this to you- as haunted by animal spirits and the ghosts of primal urges. They suspect that it houses, not the usual shiny hardware of cognition, but some witches' brew of slimy, pulsating neurons adrift in a broth of mind-altering chemicals. Let us descend to this underworld." Simon LeVay, The Sexual Brain, 1993 Reading: Kandel: Chapter 47 (hypothalamus), Chapter 58 (sex differences) Beery AK, Zucker I. Sex bias in neuroscience and biomedical research. Neurosci Biobehav Rev. 2011 Jan;35(3):565-72. 1. Organization and neural connections of the hypothalamus. • Hypothalamus: The hypothalamus is part of the diencephalon, the caudal portion of the forebrain. As the name implies, it sits below the thalamus, flanking the third ventricle, and directly above the pituitary gland. Proximity to the pituitary reflects the role of the hypothalamus as an essential link between the nervous and endocrine systems. Through activity of hypothalamic neuroendocrine neurons, the brain communicates with the endocrine system. In turn, the hypothalamus has receptors for many hormones, thereby permitting the endocrine system to communicate with the brain. • Pituitary: The pituitary is composed of two lobes consisting of glandular and neural tissue, derived from the oral ectoderm and neuroectoderm, respectively. The anterior pituitary arises from Rathke’s pouch, an evagination of the oral ectoderm. The posterior pituitary is neural ectoderm, a downward extension of the diencephalon. The posterior pituitary remains connected to the hypothalamus via a thin stalk of neural tissue, while the larger anterior pituitary wraps around the rostral face of the posterior pituitary. The pituitary is encased within a bony socket, the sella turcica. Dorsally, the pituitary is bounded by the optic chiasm and the median eminence, a thin strip of hypothalamic tissue at the base of the third ventricle. Because the pituitary is surrounded by bone except at the dorsal surface, pituitary tumors may cause vision disturbances and hypothalamic damage as they press against the overlying brain. • Neuroendocrine neurons: Neuroendocrine neurons resemble other neurons of the central nervous system. They are often multipolar cells with branching dendrites. Stimulation is by synaptic input from afferent neurons. Like other neurons, neuroendocrine neurons release chemical signals from vesicles in boutons at the end of a long axon. However, unlike typical neurons, the axon terminals of neuroendocrine neurons are in close proximity to capillaries. Transmitters released at the axon terminals enter the capillary lumen. Most neuroendocrine neurons release their products near capillaries at the base of the hypothalamus, the median eminence. The median eminence is one of the circumventricular organs, sites along the ventricles where the blood-brain barrier is weak, allowing for communication between the blood and the brain. Neuroendocrine neurons release releasing hormones from synaptic vesicles stored in axon terminals. Releasing hormones diffuse into blood vessels which travel down the pituitary stalk to the anterior pituitary, where they trigger release of pituitary hormones. Hormones from the anterior pituitary are trophic: they stimulate activity at their target glands. Neuroendocrine secretions from the hypothalamus are releasing hormones because they stimulate release of trophic hormones from the pituitary. Rather than being the "master gland" , the pituitary is an amplifier for signals from the hypothalamus. • Hypothalamo-hypophyseal portal vasculature: A portal system has two capillary beds arranged in series. For the hypothalamo-hypophyseal portal system, the median eminence is supplied by the superior hypophyseal artery, which branches to form the 1˚ capillaries of the median eminence. These converge to form the portal veins, which travel down the rostral surface of the pituitary stalk. When they reach the anterior pituitary, the portal veins fan out to form 2˚ capillaries. Why is the anterior pituitary supplied by a portal system? Releasing hormones are produced in very small quantities, and often have a short half-life in blood. The portal system provides an efficient means to deliver releasing hormones to the anterior pituitary in sufficient quantity. Because hormones from the anterior pituitary have a much longer half-life, and are released in larger amounts, the anterior pituitary functions as an amplifier for the hypothalamus. 2. Neuroendocrine systems regulated by the hypothalamus, and their key functions • Parvicellular neurons and the anterior pituitary: The anterior pituitary releases 6 hormones from 5 different cell types. Release of anterior pituitary hormones is controlled by releasing hormones from parvicellular neuroendocrine neurons in the hypothalamus. Cell bodies of neuroendocrine neurons are scattered in various hypothalamic nuclei. These neurons extend their axons to the median eminence. TARGET Thyroid Adrenal Growth Gonad Gonad Breast PITUITARY HORMONE Thyroid-stimulating hormone (TSH) Adrenocorticotropic hormone (ACTH) Growth hormone (GH) Follicle-stimulating hormone (FSH) Luteinizing hormone (LH) Prolactin HYPOTHALAMIC SECRETION Thyrotropin-releasing hormone (TRH) Corticotropin-releasing hormone (CRH) Growth hormone-releasing hormone (GHRH) Gonadotropin-releasing hormone (GnRH) Gonadotropin-releasing hormone (GnRH) Dopamine (inhibitory) • Magnocellular neurons & the Posterior Pituitary: The posterior pituitary releases two hormones: oxytocin and vasopressin (anti-diuretic hormone, ADH). Both oxytocin and vasopressin are nonapeptides. The neurons that make oxytocin and vasopressin are large magnocellular neurons, with cell bodies in the paraventricular (PVN) and supraoptic (SON) nuclei of the hypothalamus. Oxytocin is made primarily in the paraventricular nucleus, while the supraoptic nucleus synthesizes mostly vasopressin. These magnocellular neurons project caudally to the posterior pituitary. Their axons form the pituitary stalk, with the axon terminals in the neurohypophysis. Although the posterior pituitary is neural tissue, it does not contain neuronal cell bodies. Cells within the posterior pituitary are pituicytes. These are glial cells similar to astrocytes. The posterior pituitary is supplied by small arteries, which branch into fenestrated capillaries. The blood-brain barrier is absent. Vasopressin promotes water retention. It is released in response to increases in plasma osmolarity (also stress and hypovolemia). Alcohol inhibits vasopressin, thereby functioning as a diuretic. Vasopressin acts on the kidney to facilitate reabsorption of water from the urinary filtrate. Diabetes insipidus is caused by lack of vasopressin. Oxytocin is important during parturition and lactation. At parturition, oxytocin causes contraction of the myometrium to expel the fetus and placenta. During lactation, oxytocin is essential for milk release (but not milk synthesis) to move milk towards the nipple in response to suckling. Oxytocin also acts centrally as a neurotransmitter to promote pair-bonding and social interaction. 3. Behaviors and homeostatic regulatory mechanisms under hypothalamic control • Hypothalamic anatomy: Unlike the organized laminar structure of cortex or cerebellum, the hypothalamus consists of paired clusters of neurons, termed "nuclei", on either side of the third ventricle. Hypothalamic nuclei are heavily interconnected, and are interspersed with diffuse fiber bundles. From rostral to caudal, the hypothalamus can be divided into 4 regions: preoptic, anterior, tuberal, and mammillary. The preoptic region sits just rostral to the optic chiasm. Developmentally, it is part of the telencephalon, but is structurally and functionally similar to the hypothalamus. The anterior region extends from the level of the optic chiasm to the beginning of the median eminence. The tuberal region is particularly important for ingestive behavior. In a mediolateral plane, the hypothalamus can be divided into 3 zones: periventricular, medial and lateral. The periventricular zone is a thin strip of tissue adjacent to the 3rd ventricle. Most of the principal hypothalamic nuclei are in the medial zone. The lateral zone (lateral to the fornix) has sparse and indistinct nuclei, with fibers en passant. • Function: It has been said that the hypothalamus controls the 4 Fs: fighting, fleeing, feeding and... reproduction. This statement is memorable, but not entirely accurate. A more comprehensive summary of the major functions of the hypothalamus is: Social behavior Aggression Sexual behavior Maternal behavior Ingestive behavior Feeding Drinking Homeostatic mechanisms Circadian rhythms Thermoregulation Stress Medial preoptic area (MPOA): MPOA coordinates sexual and parental behavior with reproductive function. GnRH neurons at the base of the preoptic region stimulate gonadal function in males and females. In turn, the MPOA has receptors for gonadal hormones (testosterone in males, estrogen and progesterone in females). By themselves, hormones don't cause behavior. Instead, hormones enhance the salience of sensory information. In MPOA, gonadal hormones promote response to social cues from conspecifics related to sexual and parental behavior. MPOA receives sensory input from the olfactory, visual and somatosensory systems. All these sensory inputs facilitate social behavior. MPOA also receives projections from the amygdala which contributes to the emotional components of social behavior. In addition to humoral output via neuroendocrine GnRH neurons, MPOA projects to other hypothalamic nuclei, and to midbrain circuits for motivation and reward. This accounts for the rewarding aspects of both sexual and parental behavior. Periventricular nucleus (PeVN): PeVN is a thin strip of tissue immediately rostral to the 3rd ventricle. It contributes to the sensation of thirst. Increases in blood osmolarity and decreases in blood volume are sensed in the hindbrain, and this information is relayed to the PeVN. Lesions of this brain area reduce the desire to drink. Anterior hypothalamic area (AHA): AHA is important for aggressive behavior in much the same way that MPOA regulates sexual behavior. AHA and MPOA have similar neural (amygdala, sensory systems) and humoral inputs (testosterone receptors). Neurons in AHA and MPOA are also involved in body temperature regulation as a 'heat-loss center'. When the temperature of the blood increases, temperature-sensitive neurons in AHA and MPOA initiate heat-loss mechanisms: sweating, peripheral vasodilation. Body temperature is responsive to hormones from the thyroid and gonad, and from infectious agents to initiate fever. Lesions in AHA/MPOA cause hyperthermia. Paraventricular and supraoptic nuclei (PVN, SON): Their names describe their locations: adjacent to the 3rd ventricle (PVN), and above the optic tract (SON). PVN and SON have magnocellular neuroendocrine neurons that project to the posterior pituitary (see above). PVN also has parvicellular neuroendocrine neurons that regulate anterior pituitary secretion. PVN plays an important role in the response to chronic stress via CRH neurons which control secretion of cortisol from the adrenal cortex. TRH neurons in PVN stimulate the thyroid. Suprachiasmatic nucleus (SCN): SCN sits directly over the optic chiasm. It is the brain's master oscillator, where it regulates rhythms, particularly circadian rhythms. SCN receives retinal input to entrain endogenous rhythms of activity with the external environment. In turn, SCN controls rhythmicity throughout the body through secretion of melatonin from the pineal gland. Melatonin is released only in the dark. Ventromedial nucleus (VMH): VMH is considered to be a 'satiety center' in the brain. Lesions of VMH dramatically increase food intake. By contrast, the lateral hypothalamus stimulates food intake. VMH receives input about metabolic state from the arcuate nucleus. In addition, VMH is important for female sexual behavior in many animals, while MPOA is central for male sexual behavior. VMH has many estrogen receptors, and receives somatosensory information from the pudendal area. Arcuate nucleus (ARC): ARC lies immediately adjacent to the median eminence. It is particularly responsive to humoral signals about hunger, satiety and metabolism, including leptin, insulin, glucose and fat. ARC has neuroendocrine neurons that regulate prolactin and growth hormone secretion from the anterior pituitary. Dopamine neurons in ARC inhibit prolactin secretion. GHRH neurons stimulate growth hormone. Posterior nucleus (PN): PN is part of the mammillary region, and is involved in body temperature regulation, but opposite to the 'heat-loss' center in AHA/MPOA. PN is a heat-gain center activated by lower-than-normal blood temperature. Activation of PN induces shivering, piloerection, and peripheral vasoconstriction. Lesions to PN cause hypothermia. Outputs of PN project to spinal sympathetic neurons. 4. Sex differences in brain and behavior • Genetic sex: Genetic sex is determined at fertilization. In mammals, genetic females are homogametic (XX), while genetic males are heterogametic (XY). Under normal circumstances, genetic sex (XX or XY) determines phenotypic sex (male or female). When this process does not proceed normally, this gives rise to Disorders of Sexual Development (DSDs). • Phenotypic sex: Phenotypic sex encompasses the sexually-dimorphic characteristics that we express as male or female. If all sexually-dimorphic traits were specified individually in the genetic code, this would be unwieldy. Instead, the Y chromosome in males induces the early gonad to develop into a testis, which produces the male hormone testosterone that signals development of a masculine phenotype throughout the body. If no Y chromosome is present, the early gonad becomes an ovary. Although the developing ovary is relatively quiescent, development of a female phenotype does not require a similar stimulatory signal because the female is the default phenotype. Again, DSDs may arise when these processes go awry. Sex is a biologic definition that distinguishes male and female; gender is the sense of one's own self as a man or woman. As such, gender represents a combination of biologic and cultural factors. And ultimately, each of us defines our own gender. Accordingly, the distinction of male or female sex applies to all animals, but only humans can be said to have gender. • Gonadal steroid hormones: Gonadal steroid hormones are relatively long-lasting lipophilic signals derived from cholesterol that are produced in the gonads. Thus, in addition to producing gametes (oocytes and sperm), the ovaries and testes are also endocrine glands. Whether a particular cell responds to gonadal steroid hormones depends upon whether the cell has receptors for that hormone. Steroid hormone receptors are intracellular proteins that are widely distributed throughout the body, and in specific regions of the brain. • Males: Androgens are produced by the testes, and confer masculine characteristics. Testosterone is the principal androgen. Testosterone secretion during the 2nd trimester of fetal development is responsible for initial differentiation towards a male phenotype. In childhood, the testes are essentially inactive. However, testosterone production resumes at puberty. After reaching peak levels in the 20s, testosterone production declines slowly. • Females: The ovaries produce estrogens and progestagens, of which estradiol and progesterone are the most abundant. The ovaries remain quiescent throughout prenatal development and childhood. At puberty, the ovaries begin to produce estradiol and progesterone in a regular monthly pattern. At menopause, the ovary is depleted of hormoneproducing cells, and the blood levels of estradiol and progesterone fall to undetectable levels. Thus, males and females differ in the types of steroid hormones (androgens vs estrogens & progestagens), the pattern of hormone secretion (continuous in males vs cyclic in females) and the persistence of hormone production with aging (present in males vs absent in females). The changing pattern of estradiol and progesterone throughout the monthly menstrual cycle presents a particular challenge for research, since it is difficult to control for the different hormone levels among female research subjects. Historically, this concern has slowed the progress of research using women as study subjects. 5. Organizational vs activational effects of steroids Steroid hormone production has different effects depending on the stage of development. These can be divided into organizational vs activational effects. • Organization: Exposure to steroid hormones during early development produces permanent changes that persist even when the hormones are no longer present. These are known as organizational effects. These can include the acquisition of masculine characteristics (masculinization), as well as the suppression of feminine characteristics (defeminization). For example, the male genitalia differentiate prenatally under the influence of testosterone. Although testosterone is no longer present at birth or in childhood, the penis and scrotum persist. • Activation: Activational effects of steroid hormones are relatively transient actions during adulthood. In adult men, testosterone increases libido. However, as testosterone levels decline in older men, libido may also be diminished. Often, the organizational effects of steroids during development determine and interact with the activational effects in adulthood. For example, monthly menses in women represents the combination of organizational effects (development of a uterus) and activational effects (cyclic secretion of estradiol and progesterone). Because he lacks a uterus, reproducing the same pattern of hormones in a man would not induce menstruation. • Anatomical sex differences in the brain: Most of our information regarding differentiation of the hypothalamus and regulation of sexually dimorphic behavior comes from animal studies. However, analogous structures have been found in the human. In humans and animals, there are sexually dimorphic nuclei in the hypothalamus. These nuclei are ~ 2x as large in males as in females. Animal studies suggest that there is a critical period during early development when steroid exposure increases the size of the sexually dimorphic nuclei. If there is no steroid hormone in the brain during this early period, the nuclei remain permanently smaller (female). Interestingly, in most cases, estrogen is responsible for masculinization of the brain, via local aromatization from testosterone. Although there are numerous examples of sexual differentiation in behavior and brain function, as well as sexually dimorphic nuclei, it has been difficult to link particular sexually dimorphic brain regions to specific behaviors. The photos at top show the sexuallydimorphic nucleus of the preoptic area (SDN-POA) in rats. Left: normal male. Center: normal female. Right: female treated with testosterone at birth • Sex differences in behavior: How different are we? As applied to sex differences in behavior, the debate on Nature vs Nurture continues. However, there is increasing recognition in the scientific community that aspects of sexual and non-sexual behavior appear to be determined before birth, presumably due to prenatal steroids (that is, Nature not Nurture). A 2008 study compared toy preferences (plushies vs trucks) in male and female rhesus monkeys (at right). Sex differences in monkey toy preferences were remarkably similar to those of human children. On the other hand, a 2007 study (below) used eye-tracking to evaluate sex differences and effects of oral contraceptives on how men and women view sexual stimuli (pornographic photos). Men spent more time looking at female faces. Naturally-cycling women (NC females) spent more time looking at genitals, while women on oral contraceptives (OC females) spent a higher proportion of time looking at contexual elements of the pictures. However, the overall patterns of viewing were similar. 6. Sex-related and hormone-sensitive disorders in research and medicine Sex differences in disease can include differences between males and females in the incidence of a particular disease, the presenting symptoms, the clinical course, and the response to therapy. • Childhood: When a sex-related disease presents in childhood, it is reasonable to expect an organizational effect of hormones. This is not to say that testosterone (or its absence) causes the disorder per se, but that the hormonal environment during development conveys susceptibility to this disorder. Examples include autism and ADHD, which both show increased incidence in boys. • Puberty: Other sex-related diseases may present around the time of puberty (schizophrenia, substance abuse disorders in males; depression, anxiety and eating disorders in females). These diseases may represent activational effects of hormones, with or without an underlying organizational effect. Cultural and peer influences also play a significant role in this age group. • Adulthood: Some sex-related diseases in women are exacerbated by the fluctuating levels of estradiol and progesterone across the menstrual cycle. In particular, the decline in steroid hormones at menses can precipitate premenstrual syndrome, migraines, and seizures (catamenial epilepsy) in susceptible women. • Aging: As men and women age, additional sex-related diseases emerge. While steroid hormone production decreases in both sexes, women have a marked drop in estradiol and progesterone at menopause. The loss of potentially protective effects of estrogen can increase disease incidence in post-menopausal women. Examples of sex-related neurologic diseases in older adults include Alzheimer’s disease in women, and Parkinson’s Disease in men. In some cases, sex-differences in risk factors such as diet and exercise contribute to disease. 7. Implications for research When considering research and evidence-based medicine ask: • Is there gender bias inherent in the hypothesis of a study? • Is the inclusion or exclusion of women as participants in a study appropriate? • Does data analysis properly identify results by sex? • Can findings from studies that exclude particular groups such as women, children, or particular races, be generalized and applied to those groups? In recent years, clinical research studies have increased the numbers of women as human subjects. This has not happened in basic science research using cells and animals. In May of 2014, the NIH announced a new policy that basic science research must incorporate plans to balance male and female research subjects.