Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Limbic system wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Human brain wikipedia , lookup
National Institute of Neurological Disorders and Stroke wikipedia , lookup
Artificial general intelligence wikipedia , lookup
Neurophilosophy wikipedia , lookup
Neurolinguistics wikipedia , lookup
Selfish brain theory wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Brain Rules wikipedia , lookup
Neuroinformatics wikipedia , lookup
Brain morphometry wikipedia , lookup
Impact of health on intelligence wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neuroeconomics wikipedia , lookup
Neuroanatomy wikipedia , lookup
Aging brain wikipedia , lookup
Neurotechnology wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Neurogenomics wikipedia , lookup
Neuroplasticity wikipedia , lookup
Metastability in the brain wikipedia , lookup
History of neuroimaging wikipedia , lookup
Neuropsychology wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
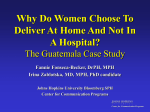
Hopkins THE NEWSLETTER O F T H E J O H N S H O P K I N S D E PA RT M E N T O F P S Y C H I AT RY A N D B E H AV I O R A L S C I E N C E S sprin g 2 0 1 5 Koko Ishizuka, right, together with research program manager Yukiko Lema, center, and research assistant Cecilia Higgs, is tapping the unique characteristics of olfactory neurons to study dynamic changes in patients with neuropsychiatric disorders. A Whiff of Psychiatric Disorder M uch like other stealth diseases—think pancreatic and liver cancers, for example—schizophrenia is notorious for seeming to arrive only in fullblown severity. And just as oncology researchers have been seeking biomarkers that signal the presence of neoplasms at a stage when they’re most easily halted, Johns Hopkins psychiatrist Koko Ishizuka and colleagues are on the trail of clues to the earliest workings of the pathology of major mental disorders—long before patients become captives of their symptoms. The challenge has been to find a true window into the brain in action. Although several lines of evidence indicate that disturbances during neurodevelopment play a role in the etiology of schizophrenia and other major mental disorders, it hasn’t been possible to “see” brain-associated molecular activity as it’s occurring. Just as a publicity photo for a film can’t capture the experience of viewing the actual movie, neither blood cells, induced pluripotent stem cells nor autopsied brains provide a useful way to correlate neuronal changes with dynamic changes in patients’ mood, drive and cognition. What does offer that capability, says Ishizuka, is the nose. The olfactory epithelium, she explains, is not only a unique part of the central nervous system that regenerates continuously throughout life, it’s a source of easily accessible neurons that originate from the two olfactory bulbs just above the nasal septum. Using cultured olfactory cells, her research group is able to measure molecular changes that may reflect those in the brain. “We are looking in these neuronal cells,” says Ishizuka, “for molecular markers of phosphorylation of a protein called DISC1.” Her team originally reported that the phosphorylation is a key switch for neuronal maturation and have since found that the phosphorylation level was altered in cells from patients with schizophrenia and some mood disorders. Furthermore, the phosphorylation level was correlated with brain structure and cognitive function, indicating that the phosphorylation may be used as a predictive marker for such clinical phenotypes, after its validation with a larger cohort. Ishizuka’s team is also looking for potential biomarkers to detect the effects of drug treatment in patients with bipolar disorder. Combining the nasal biopsy with a sophisticated microscopy technique called laser-capture microdissection, which they used to extract olfactory neurons from a larger biopsy sample, they are comparing results from a nasal biopsy before and six weeks after lithium treatment in patients, and results from nasal biopsies between similar time points in control subjects who received no lithium. “In the control subjects, the biomarker should be virtually unchanged from the first to the second biopsy,” says Ishizuka. “However, in lithiumtreated patients, the changes in biomarker expression should differ markedly, a likely indication of drug efficacy.” Results of these studies, says Akira Sawa, director of the Johns Hopkins Schizophrenia Center, could be applied clinically in as little as five years for making timely diagnoses of major mental disorders and for studying treatment responses with existing therapies—drug and behavioral—and perhaps even for testing new ones. “We believe that by combining a biomarker with imaging studies and clinical evaluation,” says Ishizuka, “we’ll have a powerful set of tools for making an accurate, early diagnosis of schizophrenia and other mood disorders.” n Sachiko Kuno and Ryuji Ueno Innovation Professorship Psychiatrist Akira Sawa has been awarded the Sachiko Kuno and Ryuji Ueno Innovation Professorship, an honor that is intended to cultivate the leadership necessary to reduce the social stigma and to improve the care of schizophrenia globally. The professorship is endowed by the S&R Foundation, begun by Sachiko Kuno and Ryuji Ueno to support individuals who are interested in furthering international collaboration in the arts, sciences or social entrepreneurship. As director of the Johns Hopkins Schizophrenia Center, Sawa oversees a number of programs structured to provide the most comprehensive, coordinated care for patients. Research, education and outreach are integral components of the programs. With this professorship, Sawa likens his role to that of an orchestra conductor, who does not directly make music, but by coaching and coordinating the musicians contributes to the orchestra’s beautiful sounds. “I am proud and feel lucky that I am surrounded by many great team members,” says Sawa. “My job for them is neither as a clinician nor a researcher, but a supporter who helps them toward one common goal— improved outcomes for patients with schizophrenia.” ideas at work Johns Hopkins Psychiatry Goes POC-IT Size I n a patient with diabetes whose glycemic control is not improving despite intensification of glucose-lowering therapy, should the clinician suspect a depressive disorder? Is it OK to prescribe clonazepam for panic attacks in a patient with a history of substance abuse? Answers to questions such as these—and hundreds of others—are now available at the tap of a finger, thanks to the resourcefulness of four Johns Hopkins psychiatry residents and the many colleagues they corralled to create an evidence-based clinical decision support tool that brings vital information to clinicians at the point of care. Called the Johns Hopkins POC-IT Guide for Psychiatry, it’s available on the Web and mobile devices, and contains over 160 interconnected sections about psychiatric illness, psychiatric medications, psychiatric emergency care, appropriate referrals and much more. The brainchild of Paul Kim, Paul Nestadt, Matthew Peters and Traci Speed, the guide was conceived originally as a resource for primary care physicians and mental health professionals such as psychologists and social workers. Primary care physicians prescribe three-quarters of the antidepressant medications in the U.S. and many antianxiety medications. The idea of the guide quickly won the support of Department Director J. Raymond DePaulo and Joe Bienvenu, who heads both the Johns Hopkins Anxiety Disorders Clinic and the Psychiatry Residents’ Outpatient Continuity Clinic. Serving as the guide’s co-editors-in-chief, DePaulo and Bienvenu helped the residents and nearly 150 department collaborators get the product written, edited and produced in a matter of two short years. Equally important to launching the guide was the technical know-how of the Johns Hopkins POC-IT Center, which also offers similar guides on antibiotics, HIV and diabetes. In October 2014, the guide was launched at the annual meeting of the American Association of Family Physicians, where it was well received. Paul Kim, Paul Nestadt, Traci Speed and Matthew Peters envisioned the POC-IT Guide over coffee. All are planning academic careers in their respective specialty areas: Kim in neuroscience research, Nestadt in anxiety disorders, Speed in mood disorders and Peters in neurocognitive disorders. “We learned a lot from the doctors there about what they wanted to know about most,” says Bienvenu. The guide, which incorporates their feedback, debuted to psychiatric colleagues in May 2015 at the American Psychiatric Association Annual meeting. “It is an added benefit that psychiatry residents and medical students also find the guide useful,” says Speed. Far from being a one-and-done project, the guide will be completely updated biannually and also if a hot topic emerges. “We will follow the model of our Division of Infectious Diseases,” Bienvenu says, “which quickly updates the ABX POC-IT Guide when there’s a new outbreak, like Ebola. We want the psychiatry guide to supplement the knowledge of both new and experienced physicians in all patient settings.” n The Johns Hopkins POC-IT Guide for Psychiatry is available on all major Web browsers and for many smartphones and tablets. To learn more, scan the code or visit bit.ly/HopkinsPsychiatryPOCIT. “It takes a village to do this kind of work,” says Joe Bienvenu, co-editor-in-chief of the Johns Hopkins POC-IT Guide for Psychiatry. The electronically available guide is equivalent to about 400 pages of the type of hard-copy pocket guide Bienvenu remembers lugging around during his medical training. image gallery Effects of Serotonin Degeneration on Emotion and Memory Networks Frederick Barrett, Haris Sair, Gwenn Smith and colleagues are using multimodal brain imaging to study how degeneration of the serotonin system affects brain function in patients with mild cognitive impairment (MCI). To do so, they measured serotonin system degeneration by imaging serotonin transporter binding with positron emission tomography (PET), and cortical and limbic brain circuits with functional magnetic resonance (fMR) imaging. In the images at left, the grey spheres are superimposed on the brain images in the fusiform gyrus (FG) of the temporo-parietal cortex that is affected in MCI. Serotonin transporter loss in the cell bodies of origin of the serotonin projections (dorsal raphe nucleus) leads to decreased communication between the FG and cortical regions including superior frontal gyrus (SFG), supramarginal gyrus (SMG) and premotor cortex (blue spheres), and a compensatory increase in communication between the fusiform gyrus and limbic regions including entorhinal cortex (ERC), subgenual anterior cingulate cortex (sgACC) and laterobasal amygdala (red spheres). These data, say the researchers, suggest that in MCI, serotonin degeneration is associated with alterations of the intrinsic organization of cortical and limbic structures involved in memory and emotional processing. The project is a collaboration between Johns Hopkins’ Division of Geriatric Psychiatry and Neuropsychiatry, the Biological Psychiatry Research Unit, and the Department of Radiology and Radiological Science. n traumatic brain injury This PET scan shows increased binding of a protein (represented in yellow), known to indicate brain injury, in the brain of a former NFL football player compared to a healthy male of similar age. The player sustained sports-related traumatic brain injury and belatedly reports impaired brain function. Johns Hopkins researchers introduced this neuroimaging approach for showing changes in the brain that could be related to sports-related brain trauma. Can a Protein Indicate Brain Injury in Older NFL Players? M ost of us who play or watch football have seen players get hurt. Some injuries are mild. Some can be career ending. But what about those that aren’t immediately visible? Today, researchers and the sports industry are looking at whether sports-related traumatic brain injury can launch progressive brain pathologies whose symptoms may go undetected for years. To help shed light on that question and open doors to treatments, cures and new ways of protecting the brain from the initial traumatic injury, researchers from the Johns Hopkins Department of Psychiatry and Behavioral Sciences and the Department of Radiology and Radiological Sciences are testing a new imaging approach for spotting signs of sports-related traumatic brain injury in former NFL football players. In their study published in the February 2015 issue of the journal Neurobiology of Disease, psychiatrist Jennifer Coughlin and colleagues enrolled retired NFL players, ages 57 to 74, who were recruited to the study by the NFL Players Association and by word of mouth. In both the players and normal aged-matched controls, the researchers used positron emission tomography (PET) to detect binding of a radiolabel to a known indicator of brain injury and repair called translocator protein. Results showed that radiolabel binding was higher in players than in controls. Of the 12 brain regions studied, three—the right and left supramarginal cortex and the right side amygdala— showed significantly elevated radiolabel binding in the football players compared to the controls. Coughlin emphasizes that this was a pilot study to test whether their approach is valid for studying brain injury. “Only nine players were studied,” she says, “which means that the number is too small to rule out other factors that might cause similar symptoms,” such as smoking, drug and alcohol use, and family history of dementia. “We hope to recruit more participants and partner with our colleagues around the country who will join us in using this and related PET scan techniques to look for brain events in football players,” Coughlin adds. “That may be the best way to provide enough data to reach more solid conclusions so we can eventually better guide players who suffer concussions.” The research was supported by several funders including the National Institutes of Health, the NFL Charities and the GE/NFL Head Health Challenge. All want to know whether (and if so, how) repetitive hits to the head can trigger a biological pathway in the brain and cognitive, mood and behavioral impairments. n We hope to be able to draw a correlation between biological markers of brain injury and the latent memory deficits that some retired players experience, and to lay out a timeline that could help explain the pathobiology of the injury. —Jennifer Coughlin paper trail save the date A smattering of the psychiatry and behavioral sciences research and thinking underway at Johns Hopkins Structural imaging in late-life depression: association with mood and cognitive responses to antidepressant treatment. Christopher Marano, Clifford Workman, Christopher Lyman, Cynthia Munro, Michael Kraut, Gwenn Smith: Am J Geriatr Psychiatry 2015;23:4-12 Assessment and management of behavioral and psychological symptoms of dementia. Helen Kales, Laura Gitlin, Constantine Lyketsos: BMJ 2015;350:h369 Cocaine dependent individuals discount future rewards more than future losses for both cocaine and monetary outcomes. Johnson MW, Bruner NR, Johnson PS: Addict Behav 2015;40:132-136 Delirium diagnosis methodology used in research: a survey-based study. Fourth Annual Schizophrenia Symposium Fall 2015 A day to hear about the latest in schizophrenia research and clinical care Johns Hopkins School of Medicine Baltimore, MD Karin Neufeld, Archana Nelliot, Sharon K. Inouye, E. Wesley Ely, O. Joseph Bienvenu, Hochang Lee, Dale Needham: Am J Geriatr Psychiatry 2014;22(12):1513-1521 Watch for details here: bit.ly/JHSchizophrenia2015 Neuropsychiatric disturbances associated with traumatic brain injury: a practical approach to evaluation and management. Vani Rao, Vassilis Koliatsos, Faizi Ahmed, Constantine Lyketsos, Kathleen Kortte: Semin Neurol 2015;35:64-82 Hopkins This newsletter is published for the Department of Psychiatry and Behavioral Sciences by Johns Hopkins Medicine Marketing and Communications. 901 South Bond Street, Suite 550 Baltimore, MD 21231 Some of the research in this newsletter has corporate ties. For full disclosure information, call the Office of Policy Coordination at 410-223-1608. To make a gift, contact Jessica Preiss Lunken, Director of Development Johns Hopkins Department of Psychiatry and Behavioral Sciences Fund for Johns Hopkins Medicine 550 North Broadway, Suite 914 Baltimore, MD 21205 Non-Profit Org. U.S. Postage PAID Permit No. 5415 Baltimore, MD Department of Psychiatry and Behavioral Sciences J. Raymond DePaulo Jr., M.D. Director Marketing and Communications Dalal Haldeman, Ph.D., M.B.A. Senior Vice President Elaine Richman, Writer Mary Ann Ayd, Managing Editor Lori Kirkpatrick, Designer Keith Weller, Photography ©2015 The Johns Hopkins University and The Johns Hopkins Health System Corporation If you no longer wish to receive this newsletter, please email [email protected] Check our departmental website for more news: www.hopkinsmedicine.org/psychiatry Hopkins T H E NE W S L ET T ER S prin g 2 0 1 5 O F T H E J O H N S H O P K I N S D E PA R T M E N T O F P S Y C H I AT RY A N D B E H AV I O R A L S C I E N C E S A Whiff of Pyschiatric Disorder PAGE 1 Johns Hopkins Psychiatry Goes POC-IT Size PAGE 2 Can a Protein Indicate Brain Injury in Older NFL Players? PAGE 3