Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Optogenetics wikipedia , lookup
Synaptogenesis wikipedia , lookup
Embodied language processing wikipedia , lookup
Axon guidance wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Synaptic gating wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neuroanatomy wikipedia , lookup
Anatomy of the cerebellum wikipedia , lookup
Development of the nervous system wikipedia , lookup
Evoked potential wikipedia , lookup
Central pattern generator wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Microneurography wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Proprioception wikipedia , lookup
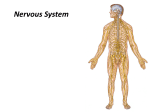
Spinal Cord
Runs through the vertebral canal
Extends from foramen magnum to
second lumbar vertebra
Regions
Cervical
Thoracic
Lumbar
Sacral
Coccygeal
Gives rise to 31 pairs of spinal nerves
All are mixed nerves
Spinal cord Enlargements
Cervical enlargement: supplies
upper limbs
Lumbo -sacral enlargement:
supplies lower limbs
Conus medullaris- tapered inferior
end
Ends between L1 and L2
Spinal Segments & Roots
Spinal segment
C8, T12, L5, S5, Cx1
Anterior (Ventral) Root
Posterior (Dorsal) Root
Dorsal Root (Spinal) Ganglion
Root - Rootlets
Spinal Segments
Importance of the
spinal segments
Coverings of Spinal cord
Dura mater: outermost layer;
continuous with epineurium of the
spinal nerves
Arachnoid mater: thin and web
like
Pia mater: bound tightly to
surface
Ligamentum Denticulatum
Cordotomy
Forms the filum terminale
anchors spinal cord to coccyx
Spaces
Epidural: external to the dura
Anesthestics injected here
Epidural Anesthesia
Subdural space: serous fluid
Subarachnoid: between pia and
arachnoid
Filled with CSF
Coverings of Spinal cord cont…
Lumbar Puncture
Lumbar Puncture – lumbar (terminal) cistern
Spinal Cord
White Matter
Anterior Funiculus (Anterior White Column)
Posterior Funiculus (Posterior White Column)
Lateral Funiculus (Lateral White Column)
Gray Matter
Anterior Horn ------------
motor
Posterior Horn -------------- sensory
Lateral Horn -----------------autonomic (sympathetic)
Gray Commissure -------- anterior and posterior
Cord Organization
Principles of Cord Organization
1) Longitudinal Arrangement
Fibers (White Matter) ------------ White Column
Cell Groups (Gray Matter) ------- Gray Column
2) Transverse Arrangement
Afferent & Efferent Fibers
Crossing (Commissural and Decussating) Fibers
3) Somatotopical Arrangement
Clinical Case
A 58-year-old woman complains of falls, imbalance,
and numbness and tingling in her hands and legs.
There is also some incoordination of hand use and
she has difficulty manipulating small items such as
knitting . She is unable to play the piano now since
she cannot position her fingers correctly on the piano
keys. She thinks the strength in her arms and legs is
adequate. Symptoms started with very slight tingling
sensations, which she noticed about a years ago.
The falls and difficulty walking have been present for
about 2 months.
Clinical Case Cont…
Higher order cognitive functions are intact
according to her husband. Her vision is normal.
On examination, the patient shows normal
mental status. Strength seems essentially normal
throughout.
Sensation, particularly to vibration and joint
position, is severely diminished in the distal
upper and lower limbs (arms, legs, hands, and
feet). Tendon reflexes are normal in the arms, but
somewhat brisk in the legs at the knees and
ankles.
Clinical Case Cont…
Gait is moderately ataxic and she has to reach out for
support by touching the walls of the hallway at
times. Fine movements of the fingers are performed
poorly, even though finger and wrist strength seems
normal
Somatosensory Pathway(Dorsal Colum)
Somatosensory Pathway
Posterior column pathway
carries sensation of highly
localized touch, pressure,
vibration.
Posterior column pathway
includes:
Fasciculus cuneatus tract
Fasciculus gracilus tract Carries fine touch,
pressure, vibration,
sterognosis and conscious
Proprioceptive sensations.
Dorsal Colum tracts
dorsal
cloumn
pathway
Dorsal Colum Lesion
Left
spinal cord injury
dorsal column
pathway
Loss of sense of:
•touch
•proprioception
•vibration
in left leg
Dorsal Colum Lesions
Sensory ataxia
Patient staggers; cannot
perceive position or
movement of legs
Visual clues help
movement
Rombergism
Assessment of Dorsal Colum
Anterolateral system
The Anterolateral Pathway
Provides sensations of
“crude” touch, pressure,
pain, and temperature
Ascend within the anterior
or lateral spinothalamic
tracts:
What is Pain?
“An unpleasant sensory & emotional experience
associated with actual or potential tissue damage,
or described in terms of such damage” –
Subjective sensation
Pain Perceptions – based on expectations, past
experience, anxiety, suggestions
Affective – one’s emotional factors that can
affect pain experience
Behavioral – how one expresses or controls
pain
Cognitive – one’s beliefs (attitudes) about pain
Pain Pathway
Physiological response produced by activation of
specific types of nerve fibers Aδand C fibres that
carry noxious sensory information
bradykinin, serotonin, prostaglandins, cytokines,
are released from damaged tissue and can
stimulate nociceptors directly.
Experienced because of nociceptors being
sensitive to extreme mechanical, thermal, &
chemical energy.
Composed of a variety of discomforts
One of the body’s defense mechanism (warns the
brain that tissues may be in jeopardy)
Where Does Pain Come
From?
Cutaneous Pain – sharp, bright, burning; can
have a fast or slow onset
Deep Somatic Pain – stems from tendons,
muscles, joints, periosteum, & b. vessels
Visceral Pain – originates from internal
organs; diffused @ 1st & later may be localized
(i.e. appendicitis)
Psychogenic Pain – individual feels pain but
cause is emotional rather than physical
Anterolateral System (Pain &Temp)
spinothalamic pathway
Left
spinal cord injury
Loss of sense of:
•Touch
•Pain
•Warmth/cold
in right leg
Spinothalamic Tracts
Located lateral and ventral to
the ventral horn
Carry impulses concerned
with pain and thermal
sensations (lateral tract) and
also non- discriminative touch
and pressure (medial tract)
Fibers of the two tracts are
intermingled to some extent
In brain stem, constitute the
spinal lemniscus
Fibers are highly somatotopically arranged, with those
for the lower limb lying most
superficially and those for the
upper limb lying deeply
Lateral Spinothalamic Tract
Carries impulses concerned
with pain and thermal
sensations.
Axons of 1st order neurons
terminate in the dorsal horn
Axons of 2nd order neuron
(mostly in the nucleus
proprius), decussate within one
segment of their origin, by
passing through the ventral
white commissure & terminate
on 3rd order neurons in ventral
posterior nucleus of the
thalamus
Thalamic neurons project to
the somatosensory cortex
Anterior Spinothalamic Tract
Carries impulses concerned
with non- discriminative touch
and pressure
Axons of 1st order neurons
enter cord terminate in the
dorsal horn
Axons of 2nd order neuron
(mostly in the nucleus proprius)
may ascend several segments
before crossing to opposite
side by passing through the
ventral white commissure &
terminate on 3rd order neurons
in ventral posterior nucleus of
the thalamus
Thalamic neurons project to the
somatosensory cortex
Spino-reticulo-thalamic System
The system represents an additional route by which
dull, aching pain is transmitted to a conscious level
Some 2nd order neurons terminate in the reticular
formation of the brain stem, mainly within the
medulla
Reticulothalamic fibers ascend to intralaminar nuclei
of thalamus, which in turn activate the cerebral
cortex
Pain Control Theories
Gate Control Theory
Endogenous Opiates Theory
Phantom Pain
Refferd Pain
Gate Control Theory
Melzack & Wall, 1965
Substantia Gelatinosa (SG) in dorsal horn of
spinal cord acts as a ‘gate’
SG cells of Lamina II act as a inhibitory neurons
and inhibit “T” cells of lamina IV
Larger diameter afferent fibers of touch excite
both SG and T cells, Therefore afferent signals of
pain sensation from T cells is blocked by
stimulation of inhibitory SG cells.
Small diameter afferent fibers excite T cells and
Inhibit SG cells Therefore Gate is kept
Descending Pain Inhibition
Descending Pain Modulation (Descending Pain Control
Mechanism)
Periaqueductal Gray Area (PGA) – release enkephalins
Nucleus Raphe Magnus (NRM) – release serotonin
The release of these neurotransmitters inhibit ascending
neurons
Stimulation of the PGA in the midbrain & NRM in the
pons & medulla causes analgesia.
Endogenous opioid peptides - endorphins &
enkephalins
Referred Pain?
Dermatomal rule
Convergence
Facilitation
Case ….
An 85-year-old man is being evaluated for gait
difficulties. On examination it is found that joint
proprioception is absent in his toes. People with
impaired position sense will usually fall if they stand
with their feet together and do which of the
following?
Flex the neck
Extend their arms in front of them
Flex the knees
Turn the head
Close their eyes
Clinical Case
A 45 year old woman complained of pain in her right breast
and progressive weakness of her right lower limb for a period
of two months, she contacted her Family physician, Her
Family physician referred her to a neurologist.
The neurologic evaluation revealed weakness in the right
lower limb. This was associated with spasticity (increased
tone), hyperreflexia (increased deep tendon reflexes) at the
knee and ankle, which also demonstrated clonus.
On the right side there was loss of two-point discrimination,
touch ,vibratory sense and proprioception at levels below the
hip. The left side showed a loss of pain and temperature
sensation below dermatome T-7.
Clinical Case Of Spinal Cord cont..
MRI of a patient indicated to have an extramedullary
tumor expanding from the dorsal roots at spinal cord
levels T-5,6.
Based on the symptoms and clinical findings what is
your diagnosis ?
Grey Matter Of Spinal cord
White Matter
Anterior Funiculus (Anterior White Column)
Posterior Funiculus (Posterior White Column)
Lateral Funiculus (Lateral White Column)
Gray Matter
Anterior Horn -----------motor
Posterior Horn -------------- sensory
Lateral Horn ----------------- autonomic
(sympathetic)
Gray Commissure -------- anterior and posterior
Principles of Cord Organization
1) Longitudinal Arrangement
Fibers (White Matter) ------------- White Column
Cell Groups (Gray Matter) ------- Gray Column
2) Transverse Arrangement
Afferent & Efferent Fibers
Crossing (Commissural and Decussating) Fibers
3) Somatotopical Arrangement
Principles of Cord Organization
Lamina of Rexed
Lamina I ---------- posteromarginal nucleus
Lamina II ---------- substantia gelatinosa of Rolando
Lamina III, IV ----- nucleus proprius
Lamina V, VI
Lamina VII --------- intermediate gray
intermediolateral cell column (ILM)
Clarke’s column (Nucleus dorsalis)
intermediomedial cell column (IMM)
Lamina VIII
Lamina IX ---------- anterior horn (motor) cell
Lamina X ----------- gray commissure
Alpha Motor Neurons
Motor Unit
Motor End Plate
Phasic
Tonic
Muscle Spindle
Motor Pathways
CNS issues motor commands in response to information
provided by sensory systems, sent by the somatic nervous
system (SNS) and the autonomic nervous system (ANS)
Conscious and subconscious motor commands control
skeletal muscles by traveling over 3 integrated motor
pathways
The corticospinal pathway – voluntary control of motor activity
Corticobulbar tracts
Corticospinal tracts
The medial and lateral pathways – modify or direct skeletal
muscle contractions by stimulating, facilitating, or inhibiting
lower motor neurons
Motor Pathways
• Contain a sequence of TWO
neurons from the cerebral
cortex or brain stem to the
muscles
• Upper motor neuron : has cell
body in the cerebral cortex or
brain stem, axon decussates
before terminating on the
lower motor neuron
• Lower motor neuron: has cell
body in the ventral horn of the
spinal cord, axon runs in the
ipsilateral ventral root of the
spinal nerve and supply the
muscle.
UMN
LMN
Descending Spinal Tracts
Originate from the cerebral cortex & brain
stem
Concerned with:
Control of movements
Muscle tone
Spinal reflexes & equilibrium
Modulation of sensory transmission to
higher centers
Spinal autonomic functions
The motor pathways are
divided into two groups
Direct pathways
(voluntary motion
pathways) - the
pyramidal tracts
Indirect pathways
(postural pathways),
essentially all others the extrapyramidal
pathways
Direct (Pyramidal) System
Regulates fast and fine (skilled) movements
Originate in the pyramidal neurons in the
precentral gyri,
Impulses are sent through the corticospinal
tracts and synapse in the anterior horn
Stimulation of anterior horn neurons activates
skeletal muscles
Part of the direct pathway, called corticobulbar
tracts, innervates cranial nerve nuclei
Indirect (Extrapyramidal) System
Complex and multisynaptic pathways
The system includes:
• Rubrospinal tracts: control flexor muscles
• Vestibulospinal tracts: maintain balance and
posture
• Tectospinal tracts: mediate head neck, and eye
movement
• Reticulospinal tracts
Descending Spinal Tracts
Pyramidal
Corticospinal
Extrapyramidal
Rubrospinal
Tectospinal
Vestibulospinal
Olivospinal
Reticulospinal
Descending
Autonomic Fibers
Corticospinal Tracts
Concerned with voluntary,
discrete, skilled
movements, especially
those of distal parts of the
limbs (fractionated
movements)
Innervate the contralateral
side of the spinal cord
Provide rapid direct
method for controlling
skeletal muscle
Origin: motor and sensory
cortices
Axons pass through corona
radiata, internal capsule, crus
cerebri and pyramid of
medulla oblongata
In the caudal medulla about
75-90% of the fibers
decussate and form the
lateral corticospinal tract
Rest of the fibers remain
ipsilateral and form anterior
corticospinal tract. They
also decussate before
termination
Distribution:
55% terminate at
cervical region
20% at thoracic
25% at lumbosacral
level
Termination: Ventral horn
neurons (mostly through
interneurons, a few fibers
terminate directly)
Corticobulbar tracts end
at the motor nuclei of CNs
of the contralateral side
Rubrospinal Tract
Controls the tone of limb
flexor muscles, being
excitatory to motor neurons
of these muscles
Origin: Red nucleus
Axons course ventromedially, cross in ventral
tegmental decussation,
descend in spinal cord
ventral to the lateral
corticospinal tract
Cortico-rubro-spinal pathway
(Extrapyramidal)
Tectospinal Tract
Mediates reflex movements of
the head and neck in response
to visual stimuli
Origin: Superior colliculus
Axons course ventro-medially
around the periaqueductal gray
matter, cross in dorsal
tegmental decussation,
descend in spinal cord near the
ventral median fissure,
terminate mainly in cervical
segments
Cortico-tecto-spinal pathway
(Extrapyramidal)
Vestibulospinal Tracts
Lateral Vestibulospinal
Tracts
Origin: lateral vestibular
(Deiter’s) nucleus
Axons descend ipsilaterally in
the ventral funiculus
Terminate on ventral horn
cells throughout the length of
spinal cord
Has excitatory influences
upon extensor motor neurons,
control extensor muscle tone
in the antigravity maintenance
of posture
Case ..
Following an automobile accident, an eighteen year
old male was hospitalized for several weeks. A
neurological exam at that time revealed the
following:
1. Complete loss of conscious proprioception in the
right lower limb.
2. Babinski sign on the right.
3. Inability to detect pain and temperature sensation
on the medial side of the antecubital fossa
(medialepicondyle) on both upper limbs.
4. Inability to detect pain and temperature at the apex
of the left axilla, in all the intercostal spaces on the
left, and in the left lower limb.
5. The patient could feel a gentle squeezing of both
thumbs, right and left middle fingers, and the left
little finger.
6. No sensation to squeezing could be detected in the
right little finger.
Ipsilateral paralysis below the lesion. Paralysis is
the "Upper Motor Neuron" or spastic type; there is
spasticity, slow (disuse) muscle atrophy, hypertonia,
ankle clonus and a positive Babinski sign. Superficial
reflexes, e.g., the abdominal and cremasteric are lost.
Spastic paralysis is attributed to interruption of the
lateral corticospinal tract and the accompanying lateral
reticulospinal tract. Loss of these upper motor neurons
deprives the anterior horn cells, i.e., lower motor
neurons, of the impulses which generate contraction of
skeletal muscle, hence, weakness (paresis) or paralysis.
Hypertonia and hyperreflexia appear to result from loss
of the inhibitory effects of these two descending motor
pathways on the stretch reflexes, leaving them
hyperexcitable to segmental muscle afferents
It may be possible to also demonstrate a "Lower
Motor Neuron Syndrome" or flaccid paralysis
ipsilaterally at the level of the lesion. If the anterior
horn cells supplying the skeletal muscles are injured
at the level of the lesion then these muscles are
denervated. This paralysis is of the flaccid type;
muscles undergo rapid atrophy due to loss of the
trophic influence of the nerves as well as disuse.
Tone and tendon reflexes are diminished since they
are reflex responses and the injured lower motor
neurons are the "final common pathway" to the
muscle in the stretch reflex, hence, there is no
reflex.
Loss of conscious proprioception, two-point
discrimination and vibratory sense ipsilaterally is due to
interruption of the posterior white columns (fasciculus
gracilis/cuneatus). This is frequently accompanied by a Romberg
sign. A normal individual, standing erect with heels together and
eyes closed, sways only slightly. Stable posture is achieve by
1) a sense of position from the vestibular system,
2) awareness of the position and status of muscles and joints by
conscious proprioception and 3) visual input regarding our position.
Closing the eyes has only slight effect on the normal individual's
stance since the vestibular and conscious proprioception systems
are sufficient. In a patient with an impaired posterior column
conscious proprioception is diminished; when the eyes are closed
loss of both systems renders the patient unstable and they are likely
to sway or fall to the side.
Pain and temperature sensation is lost below the
lesion, on the opposite side beginning about one
dermatomal segment below the level of the lesion. These
sensations are carried by the lateral spinothalamic tract
whose fibers originated on the side opposite the lesion
but which crossed in the anterior white commissure.
Dorsal root afferents carrying pain and temperature
synapse in the dorsal gray; the second order neuron
crosses in the anterior white commissure along an
ascending path for a distance of about one spinal
segment. Because of the oblique ascent of the crossing
fibers in the anterior white commissure, injury of the
spinothalamic tract is not likely to be carrying sensation
from that level.
A careful sensory evaluation may reveal that at the
dermatomal level of the lesion there is a bilateral
loss of pain and temperature sensation. Since the
second order neurons from both sides cross in the
midline below the central canal, a hemisection of
the cord may interrupt the crossing fibers from both
sides and produce this limited bilateral deficit.
Hemisection of Spinalcord
At the level of
lesion
side
Sensory
disturbance
Motor
disturbance
Reflexes
On the same side
Below
On the Opposite
side
Loss of all sensation
Loss of the dorsal
Loss of
1-superfecial sensations column due to
1-pain & temp.
2-deep sensations
damage of gracil &
due to damage of
cunite leading to loss lateral
of
spinothalamic tract.
1. fine touch
2-crude touch due
2. kinesthetic
to damage of
3. vibration
ventral
4. sterognosis
spinothalamic tract.
1-LMNL
UMNL due to
2-paralysis of muscles damage of pyramidal
which its supply arising tract
from damage
Loss of all reflexes
which its centers in
damage segments
On the same side
1-loss of flexor
withdrawal reflex
2-increase crossed
extensor reflex
Above
On the same side
Hyperanasthesia
(Hypersensitivity)
increase sensitivity to
1. pain
2. touch
3. Temp.
Case 2….
• A 55 year old man noticed a weakness of his left hand
and loss of pain in his both arms which was progressing
and causing him mental apathy and he felt he should
visit neurologist .
• On examination he demonstrated bilateral weakness,
atrophy, and fasciculations of the intrinsic muscles of his
hands and shoulders. Upper motor neuron syndrome
signs, i.e., weakness, hypertonia, hyperreflexia, positive
Babinski, were evident in both lower extremities.
Dermatomes C-2 through T-6 demonstrated bilateral
loss of pain and temperature sensation. There was
bilateral impairment of position and vibratory sense
below the hips.
Case 2 cont..
MRI investigation showed a central cavitation at C-2
through T-7 which expanded symmetrically in all
directions.
It involved the anterior white commissure
(spinothalamic fibers) and included portions of the
posterior white columns, lateral white funiculus, and
anterior gray horns.
Syringomyelia
Syringomyelia
the result of central cord cavitation affecting a few segments,
and usually involving the cervical spinal cord
frequently found in Arnold-Chiari malformations affecting the upper
cervical cord and medulla
mainly affects the crossing fibres of the spinothalamic tract as they
decussate in the ventral white commissure => bilateral paintemperature sensory loss over a few segments eg. only
affecting the neck and upper shoulders in a cape-like distribution (or
only affecting the upper limbs) with normal sensation above and
below the affected dermatomes
does not affect the spinothalamic tracts in the early stages => no
initial lower trunk or lower limb pain-temperature sensory loss
does not usually affect the dorsal columns => normal position sense
("dissociative" sensory loss)
may rarely affect the lower motor neurons to the upper limbs early in
the disease course, and may eventually affect the corticospinal tracts