Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Blood–brain barrier wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
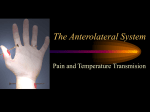
Haemodynamic response wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Neuroeconomics wikipedia , lookup
Selfish brain theory wikipedia , lookup
Time perception wikipedia , lookup
Human brain wikipedia , lookup
Neuroinformatics wikipedia , lookup
State-dependent memory wikipedia , lookup
Brain morphometry wikipedia , lookup
Neurolinguistics wikipedia , lookup
Neurophilosophy wikipedia , lookup
Emotional lateralization wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuroanatomy wikipedia , lookup
Neurotechnology wikipedia , lookup
Neuroesthetics wikipedia , lookup
Limbic system wikipedia , lookup
Brain Rules wikipedia , lookup
Neuropsychology wikipedia , lookup
Aging brain wikipedia , lookup
Metastability in the brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
ESSAY TOPICS ON CNS 1. Functional neuroanatomy of pain Reference Usunoff, K.G., Popratiloff, A., Schmitt, O., Wree, A. Functional Neuroanatomy of Pain Series: Advances in Anatomy, Embryology and Cell Biology, Vol. 184, 2006. Introduction.- Functional neuroanatomy of the pain system.- Primary afferent neuron.Distribution of nociceptor peripheral endings.- Termination in the spinal cord and spinal trigeminal nucleus.- Ascending pathways of the spinal cord and of the STN.- Dorsal column nuclei and nociception.- Cerebellum and nociception.- Cortices involved in pain perception and thalamocortical projection.- Descending modulatory pathways.- Neuropathic pain.Central changes consequent to peripheral nerve injury.- The role of glial cells.Neuropathology of herpes zoster (HZ) and of postherpetic neuralgia (PHN).- Diabetic neuropathic pain.- Cancer neuropathic pain.- Central neuropathic pain 2. Neuroanatomy of the pain system and of the pathways that modulate pain. Reference Willis WD, Westlund KN. Department of Anatomy & Neurosciences, University of Texas Medical Branch, Galveston 77555-1069, USA. Abstract We review many of the recent findings concerning mechanisms and pathways for pain and its modulation, emphasizing sensitization and the modulation of nociceptors and of dorsal horn nociceptive neurons. We describe the organization of several ascending nociceptive pathways, including the spinothalamic, spinomesencephalic, spinoreticular, spinolimbic, spinocervical, and postsynaptic dorsal column pathways in some detail and discuss nociceptive processing in the thalamus and cerebral cortex. Structures involved in the descending analgesia systems, including the periaqueductal gray, locus ceruleus, and parabrachial area, nucleus raphe magnus, reticular formation, anterior pretectal nucleus, thalamus and cerebral cortex, and several components of the limbic system are described and the pathways and neurotransmitters utilized are mentioned. Finally, we speculate on possible fruitful lines of research that might lead to improvements in therapy for pain. 3. The Compassionate Brain: Humans Detect Intensity of Pain from Another's Face Reference Miiamaaria V. Saarela, Yevhen Hlushchuk, Amanda C. de C. Williams, Martin Schürmann, Eija Kalso and Riitta Hari. Abstract Understanding another person's experience draws on "mirroring systems," brain circuitries shared by the subject's own actions/feelings and by similar states observed in others. Lately, also the experience of pain has been shown to activate partly the same brain areas in the subjects‘ own and in the observer's brain. Recent studies show remarkable overlap between brain areas activated when a subject undergoes painful sensory stimulation and when he/she observes others suffering from pain. Using functional magnetic resonance imaging, we show that not only the presence of pain but also the intensity of the observed pain is encoded in the observer's brain—as occurs during the observer's own pain experience. When subjects observed pain from the faces of chronic pain patients, activations in bilateral anterior insula (AI), left anterior cingulate cortex, and left inferior parietal lobe in the observer's brain correlated with their estimates of the intensity of observed pain. Furthermore, the strengths of activation in the left AI and left inferior frontal gyrus during observation of intensified pain correlated with subjects’ self-rated empathy. These findings imply that the intersubjective representation of pain in the human brain is more detailed than has been previously thought. 4. Somatotopic Activation in the Human Trigeminal Pain Pathway Reference Alex F. M. DaSilva, Lino Becerra, Nikos Makris, Andrew M. Strassman, R. Gilberto Gonzalez, Nina Geatrakis, and David Borsook. The Journal of Neuroscience, September 15, 2002, 22(18):8183-8192 Abstract Functional magnetic resonance imaging was used to image pain-associated activity in three levels of the neuraxis: the medullary dorsal horn, thalamus, and primary somatosensory cortex. In nine subjects, noxious thermal stimuli (46°C) were applied to the facial skin at sites within the three divisions of the trigeminal nerve (V1, V2, and V3) and also to the ipsilateral thumb. Anatomical and functional data were acquired to capture activation across the spinothalamocortical pathway in each individual. Significant activation was observed in the ipsilateral spinal trigeminal nucleus within the medulla and lower pons in response to at least one of the three facial stimuli in all applicable data sets. Activation from the three facial stimulation sites exhibited a somatotopic organization along the longitudinal (rostrocaudal) axis of the brain stem that was consistent with the classically described "onion skin" pattern of sensory deficits observed in patients after trigeminal tractotomy. In the thalamus, activation was observed in the contralateral side involving the ventroposteromedial and dorsomedial nuclei after stimulation of the face and in the ventroposterolateral and dorsomedial nuclei after stimulation of the thumb. Activation in the primary somatosensory cortex displayed a laminar sequence that resembled the trigeminal nucleus, with V2 more rostral, V1 caudal, and V3 medial, abutting the region of cortical activation observed for the thumb. These results represent the first simultaneous imaging of pain-associated activation at three levels of the neuraxis in individual subjects. This approach will be useful for exploring central correlates of plasticity in models of experimental and clinical pain. 5. Memory, language, and other brain abilities Brain memory 1. Brain memory 2. How to improve brain memory 3. Brain memory types o Conscious cognitive processes Instantaneous memory Specialized memory Linguistic Visual Emotional o The persistence of brain memory Short-term memory Medium-term memory Long-term memory Vital memory o Reliability of the memory information system o Data integrity 4. Human brain memory o Automatic memory and directed memory o Pre-established logic blocks or structures o Memorise only what it is not logic 5. Evolutionary genetics and neuroscience o Brain memory inheritance o The simple complementary effect o Genetic foundation and the origin of language 6. Emotions and brain The amygdala and allies Reference: www: thebrain.mcgill.ca Abstract The amygdala is an almond-shaped structure in the brain; its name comes from the Greek word for “almond”. As with most other brain structures, you actually have two amygdalae (shown in red in the drawing here). Each amygdala is located close to the hippocampus, in the frontal portion of the temporal lobe. Your amygdalae are essential to your ability to feel certain emotions and to perceive them in other people. This includes fear and the many changes that it causes in the body. If you are being followed at night by a suspect-looking individual and your heart is pounding, chances are that your amygdalae are very active! In certain studies, researchers have directly stimulated the amygdalae of patients who were undergoing brain surgery, and asked them to report their impressions. The subjective experience that these patients reported most often was one of imminent danger and fear. In studies of the very small number of patients who have had had only their amygdala destroyed (as the result of a stroke, for example), they recognized the facial expressions of every emotion except fear. In fact, the amygdala seems to modulate all of our reactions to events that are very important for our survival. Events that warn us of imminent danger are therefore very important stimuli for the amygdala, but so are events that signal the presence of food, sexual partners, rivals, children in distress, and so on. That is why the amygdala has so many connections with several other structures in the brain.