Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Haemodynamic response wikipedia , lookup
Human brain wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Neuropsychology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Time perception wikipedia , lookup
Biology of depression wikipedia , lookup
Dual consciousness wikipedia , lookup
Affective neuroscience wikipedia , lookup
Neurolinguistics wikipedia , lookup
Neuroeconomics wikipedia , lookup
Neurophilosophy wikipedia , lookup
Persistent vegetative state wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Metastability in the brain wikipedia , lookup
Neuroesthetics wikipedia , lookup
Aging brain wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
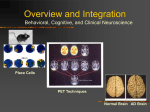
Functional magnetic resonance imaging wikipedia , lookup
Embodied language processing wikipedia , lookup
Neuroplasticity wikipedia , lookup
Emotional lateralization wikipedia , lookup
University of Kentucky UKnowledge University of Kentucky Master's Theses Graduate School 2004 CEREBRAL ACTIVATION DURING THERMAL STIMULATION OF BURNING MOUTH DISORDER PATIENTS: AN f MRI STUDY Romulo J.C. Albuquerque University of Kentucky, [email protected] Recommended Citation Albuquerque, Romulo J.C., "CEREBRAL ACTIVATION DURING THERMAL STIMULATION OF BURNING MOUTH DISORDER PATIENTS: AN fMRI STUDY" (2004). University of Kentucky Master's Theses. Paper 238. http://uknowledge.uky.edu/gradschool_theses/238 This Thesis is brought to you for free and open access by the Graduate School at UKnowledge. It has been accepted for inclusion in University of Kentucky Master's Theses by an authorized administrator of UKnowledge. For more information, please contact [email protected]. ABSTRACT OF THESIS CEREBRAL ACTIVATION DURING THERMAL STIMULATION OF BURNING MOUTH DISORDER PATIENTS: AN fMRI STUDY Functional magnetic resonance imaging (fMRI) has been widely used to study cortical and subcortical mechanisms related to pain. The pathophysiology of burning mouth disorder (BMD) is not clearly understood. Central neuropathic mechanisms are thought to be main players in BMD. This study aimed to compare the location and extension of brain activation following thermal stimulation of the trigeminal nerve with fMRI blood oxygenation level dependent (BOLD) signal. This study included 8 female patients with BMD and 8 matched pain-free volunteers. Qualitative and quantitative differences in brain activation patterns between the two study groups were demonstrated. There were differences in the activation maps regarding the location of activation, with patients displaying greater BOLD signal changes in the right anterior cingulate cortex (ACC BA 32/24) and bilateral precuneus (p<0.005). The control group showed larger BOLD signal changes in the bilateral thalamus, right middle frontal gyrus, right pre-central gyrus, left lingual gyrus and cerebellum (p<0.005). It was also demonstrated that patients had far less volumetric activation throughout the entire brain compared to the control group. These data are discussed in light of recent findings suggesting brain hypofunction as a key player in chronic neuropathic pain conditions. KEYWORDS: Burning Mouth Disorder, Functional Magnetic Resonance Imaging, Brain Activation, Trigeminal Thermal Stimulation, Thalamic Hypofunction Romulo J.C. Albuquerque, DDS July 27, 2004 CEREBRAL ACTIVATION DURING THERMAL STIMULATION OF BURNING MOUTH DISORDER PATIENTS: AN fMRI STUDY By Romulo Jose Cunha Albuquerque Reny de Leeuw, DDS, PhD Director of Thesis Karen Novak, DDS, MS, PhD Director of Graduate Studies RULES FOR THE USE OF THESIS Unpublished theses submitted for the Master’s degree and deposited in the University of Kentucky Library are as a rule open for inspection, but are to be used only with due regard to the rights of the authors. Bibliographical references may be noted, but quotations or summaries of parts may be published only with permission of the authors, and with the usual scholarly acknowledgments. Extensive copying or publication of the thesis in whole or in part also requires the consent of the Dean of the Graduate School of the University of Kentucky. A library that borrows this thesis for use by its patrons is expected to secure the signature of each user. THESIS Romulo Jose Cunha Albuquerque The Graduate School University of Kentucky 2004 CEREBRAL ACTIVATION DURING THERMAL STIMULATION OF BURNING MOUTH DISORDER PATIENTS: AN fMRI STUDY ______________________________________ THESIS ______________________________________ A thesis submitted in partial fulfillment of the requirements for the degree of Masters of Science at the University of Kentucky By Romulo Jose Cunha Albuquerque Lexington, Kentucky Director: Dr. Reny de Leeuw, Professor of Dentistry Lexington, Kentucky 2004 Copyright © 2004, Romulo J.C. Albuquerque ACKNOWLEDGMENTS The following thesis, while an individual work, benefited from the insights and direction of several people. First, my Thesis Committee, Dr. Reny de Leeuw (Thesis Chair), Dr. Jeffrey Okeson and Dr. Charles Carlson, exemplifies the high quality scholarship to which I aspire. In addition, Anders Andersen and Craig Miller provided timely and instructive comments and evaluation for the development of this work. My fellow residents, staff from the Orofacial Pain Center and staff from the Magnetic Resonance Imaging and Spectroscopy Center (Agnes Bognar, Nancy Bailey and David Powell) were indispensable part for the accomplishment of this research. I would like to thank the Orofacial Pain Center and the Magnetic Resonance Imaging and Spectroscopy Center for having funded this study. In particular, I would like to acknowledge my patients and volunteers for their willingness to take part in this study. Their role is indisputably vital to the advances that science has undergone throughout its history. For my part, I would like to thank Dr. Jeffrey Okeson for having given me the opportunity to embark this intellectual journey at the Orofacial Pain Center. I would also like to thank my family, who back in Brazil has supported me by all means through this academic process. Above all, this work would not have been possible if it was not for my wife Lisandra Garcia. She was my harbor when storms came through. She was my friend, my family, my “everything”. I dedicate this thesis to her. iii TABLE OF CONTENTS Acknowledgments……………………………………………………………………..………..iii Table of Contents……………………………………………………………………………….iv List of Tables……………………………………………………………………………..……..vi List of Figures………………………………………………………………………..…………vii List of Files……………………………………………………………………………………..viii 1. Introduction……………………………………………………………………….…………..1 2. Purpose of the Study……………………………………………………………….………..3 3. Review of the Literature……………………………………………………………………..4 3.1. Technical Foundation of Functional Neuroimaging Methods: an Emphasis on fMRI……………………………………………………………………………...……4 3.2. PET vs. fMRI…………………………………………………………………..……5 3.3. Functional Neuroanatomy of Pain…………………………………………..……5 3.4. Common Supraspinal Sites Depicted by Neuroimaging Pain Studies…….....7 3.5. Functional Neuroimaging in Chronic Pain………………………………….….15 3.6. Functional Brain Imaging in Orofacial Pain………………………………...….17 3.7. Burning Mouth Disorder………………………………………………………….22 3.8. Hypothesis……………………………………………………………………...…27 4. Materials and Methods…………………………………………………………………..…29 4.1. Study Design…………………………………………………………………...…29 4.2. Study Population…………………………………………………………….……29 4.3. Subject Recruitment Method………………………………………………..…..30 4.4. Research Procedures……………………………………………………………31 4.5. Statistical Analysis……………………………………………………………….34 iv 5. Results………………………………………………………………………………….……37 5.1. Demographics and Psychophysical Tests………………………………..……37 5.2. Functional MRI Data Analysis……………………………………………..……40 6. Discussion………………………………………………………………………………...…46 6.1. Qualitative Differences in Brain Activation Between Patients and Controls……………………………………………………………………………...….47 6.2. Quantitative Differences in Brain Activation Between Patients and Controls……………………………………………………………………………...….50 6.3. Future Research Directions…………………………………………………..…54 6.4. Study Limitations………………………………………………………………....55 7. Summary………………………………………………………………………………….…57 References…………………………………………………………………………….…….…58 Vita………………………………………………………………………………………………71 v LIST OF TABLES Table 1. Detailed description of the patient population ………………………………...…38 Table 2. Comparison between patients with BMD (n=8) and controls (n=8) regarding the psychophysical data…………………………………………………………………………...39 Table 3. Comparison between patients with BMD (n=8) and controls (n=8) regarding the SCL-90 subscales…………………………………………………………………………..…39 Table 4. Comparison between patients with BMD (n=8) and controls (n=8) regarding the BDI and STAI scores………………………………………………………………………….40 Table 5. Areas of differential activation between BMD patients (n=8) and pain-free volunteers (n=8)…………………………………………………………………………….….44 Table 6. Location and size of the detected clusters of activity in the patient group…….44 Table 7. Location and size of the detected clusters of activity in the control group…….45 vi LIST OF FIGURES Figure 1. Magnetic resonance image of the left anterior cingulate cortex located by the Talairach coordinates (x,y,z)=(5[L],27[A],23[S])…............................................................8 Figure 2. Schematic representation of the anterior cingulate cortex and its subdivisions. ………………………………………………………………………………………………...…..9 Figure 3. Magnetic resonance image of the left insular cortex located by the Talairach coordinates (x,y,z)=(34[L],0[A],4[S])…………………………………………………………11 Figure 4. Magnetic resonance image of the left thalamus located by the Talairach coordinates (x,y,z)=(9[L],15[P],9[S])…………………………………………………………13 Figure 5. Magnetic resonance image of the left dorsolateral prefrontal cortex located by the Talairach coordinates (x,y,z)=(42[L],8[A],29[S])……………………………………….14 Figure 6. Thermal stimulation paradigm (in degrees Celsius)……..……………………..33 Figure 7. Activation map of the BMD group (n=8)………………………………………….41 Figure 8. Activation map of the control group (n=8)………………………………….…….41 Figure 9. Activation map of the comparison between BMD group (n=8) and control group (n=8)……………………………………………………………………………………..42 vii LIST OF FIGURES File 1. ………………………………………………………………………….. fMRI_BMD.pdf viii 1. Introduction Extensive attention has been given to the understanding of the mechanisms involved in nociception, pain modulation and perception by researchers and clinicians around the world. At the present time, however, the implications of the central nervous system (CNS), especially supra-spinal mechanisms, in chronic pain conditions, pain perception and modulation processes are poorly understood. Most of our knowledge is derived from either extrapolations from animal model studies [1, 2] or case reports from patients who had different types of injuries, neuropathies, or surgical procedures involving the CNS [3, 4] [5, 6]. The use of positron emission tomography (PET) and the recent development of functional magnetic resonance imaging (fMRI) have added objective knowledge of pain processing and have clarified some of the features and implications of the CNS in the complex pain modulation networks. The neural circuits of pain are far beyond a simple nociceptive input barrage arising from the periphery to the CNS. Rather, pain processing networks are under the influence of several modulating factors that will be elaborated below. Further, the neural circuits of pain have different dimensions and aspects as proposed by Melzack [7] in the pain “neuromatrix”. These circuits comprise a widely distributed neural network that includes parallel somatosensory, limbic and thalamocortical components that enable the sensory-discriminative, affective-motivational and evaluative-cognitive dimensions of pain experience. Functional MRI studies have been performed since Belliveau and colleagues published the first paper in 1991. [8] A series of different central processing mechanisms have been explored with functional MRI techniques, such as attention and 1 cognition, [9],[10] language, [11] memory, learning, vision processing, auditory perception, [12] cerebellum neurophysiology, [13] and sensory and motor functions. Functional MRI has also been used in neurosurgical planning and for implantation of electrodes within different brain structures for the treatment of neuropathic pain conditions. [14] A variety of functional neuroimaging studies have been conducted to clarify the role of neural structures and cortical regions implicated in the pain “neuromatrix”. Creative, elegant and well-planned research has been designed to explore the “neuromatrix” associated with acute pain models (chemical, thermal and mechanical stimuli) and clinical pain conditions, such as migraines, [15] cluster headaches [16-19], neuropathic pain [20-22] and phantom limb pain. [23] These studies have greatly improved our understanding about the role of many CNS structures in the underlying mechanisms of the above mentioned clinical pain entities. Other orofacial pain disorders, have not yet been the focus of extensive neuroimaging studies. Orofacial pain disorders comprise a variety of acute and chronic pain conditions that include, but are not limited to temporomandibular joint disorders, masticatory myofascial pain, trigeminal neuralgia and continuous neuropathic pains, including burning mouth disorder (BMD). Some of these disorders do not respond to peripheral interventions and it is likely that CNS mechanisms are primarily involved in their etiologies. [24] Brain-imaging studies are a powerful tool for exploring and understanding more of the features of the complex central network of pain in the orofacial region as well as exploring the likely pathophysiology of chronic orofacial pain conditions, such as BMD. Copyright © 2004, Romulo J.C. Albuquerque 2 2. Purpose of the Study Functional MRI studies investigating stimulation of the trigeminal nerve are scarce. To date, chronic orofacial pain conditions have not been investigated under the spectrum of fMRI. This study intends to investigate differences in location and extent of activation of brain regions involved in the sensory-discriminative and emotional-affective components of trigeminal pain processing between patients with BMD and age-matched pain-free volunteers. Copyright © 2004, Romulo J.C. Albuquerque 3 3. Review of the Literature 3.1. Technical Foundation of Functional Neuroimaging Methods: an Emphasis on fMRI Brain-imaging studies rely on the ability of techniques, such as positron emission tomography (PET) and functional magnetic resonance imaging (fMRI), to detect “activity” within the central nervous system. This activity is presumably related to glucose metabolism (PET) and blood perfusion changes (fMRI) most likely associated with neuronal firing [25] [8]. The respective imaging techniques do not directly measure neuronal activity, but translate changes in regional blood flow and blood oxygenation levels associated with such activity into detectable signals. The most common way of detecting brain activity with fMRI is by measuring relative changes in oxyhemoglobin and deoxyhemoglobin levels. Thus, blood oxygenation level dependent (BOLD) signals are measured in and around the microvasculature of active centers in the CNS. More specifically, oxygenated hemoglobin circulates through the brain capillary network and has magnetic susceptibility similar to the surrounding tissues. When activated, neurons extract oxygen from the capillaries, distending the venous vessels and causing oxygenated blood perfusion and relative dilution and reduction of deoxyhemoglobin concentration.[25] Oxygenated hemoglobin and deoxyhemoglobin have diamagnetic and paramagnetic properties, respectively. They serve as a type of endogenous image contrast. When the relative concentration of oxyhemoglobin and deoxyhemoglobin change, the signal of the T2* weighted MRI changes as well. The local physiological changes result in increased magnetic signal and create a brighter image in the area of activation. [26] Maps of brain activation are developed by extensive processing and 4 statistical analysis of the acquired images. Statistical correlations between the BOLD signal and the desired study stimuli are then calculated for each voxel of the brain image throughout the experiment time. In summary, neural activity has been linked to physiological changes in the local microvasculature that are detectable with imaging techniques such as fMRI [8, 27]. 3.2. PET vs. fMRI When compared to PET imaging, functional MRI renders a series of advantages, as described by Peyron et al. (2000) [28] For instance, functional MRI has superior temporal and spatial resolution; there is no need for radioactive image contrast as is needed for PET, and no injection is required. Further, in fMRI, individual subject data may be analyzed, in contrast to PET studies, where images require pooling in order to achieve interpretable results. Functional MRI also has some disadvantages when compared to PET. Pulsating artifacts impede a detailed visualization of brainstem and thalamic activation. In addition, fMRI is limited to comparisons of cerebral neuronal activation with resting states (baseline activity); and it is therefore unable to portray possible certain neuronal events related to, for example, chronic pain states.[28] Notwithstanding the differences presented between the two techniques, results from both imaging techniques are generally comparable [29]. 3.3. Functional Neuroanatomy of Pain In order to comprehend the most common findings of fMRI studies, it is important to review some of the functional neuroanatomy of the pain-processing network. The 5 conduction of information to the CNS (afferent conduction) is performed by different types of neurons: the first-order neurons that conduct the input from the periphery into the spinal cord; the second-order neurons, which travel along the spinothalamic pathway ascending to the higher centers (thalamus, cortex) of the CNS; and the third/fourth-order (interneurons) neurons, which carry impulses through a multi-synaptic path to the thalamus, reticular formation, other parts of the brainstem and other brain structures, such as the cerebellum, superior colliculus, pontine parabrachial nucleus and periaqueductal gray matter. [30] Nociceptive input is just one of the many different types of afferent signaling barrages (sensory pathways) ascending to the CNS and it will be the main focus of our discussion in this section. The nociceptive conduction process involves two main pathways: the lateral and the medial pain system. The lateral pain system, also called the neospinothalamic tract mainly relays information to the ventral posterior lateral nucleus, ventral posterior medial nucleus and ventral posterior inferior nucleus of the thalamus. The lateral thalamic nuclei project to the primary (SI) and secondary (SII) somatosensory cortices and are thought to be implicated in mediating the sensory-discriminative aspect of the pain experience. When the stimulus travels through the lateral pain system, contralateral activation of the brain is expected [31, 32]. The medial pain system, or paleospinothalamic tract, mainly involves medial thalamic structures, such as the ventral part of the ventral medial nucleus, the ventrocaudal part of the medial dorsal nucleus, the parafascicular nucleus and the contralateral nucleus. The medial thalamic nuclei send information to the insula and anterior cingulate cortex (ACC) and comprise primarily the affective-motivational portion 6 of the pain experience. The medial pain system possesses spinothalamic and spinoreticular projections to various brainstem nuclei and the limbic structures. [33] From the limbic system the nociceptive stimulus is conducted to both right and left cerebral cortices, expressing most likely, a bilateral activation. A word of caution is in place here because there are several additional cortico-cortical connections that may also be important in pain pathways.[31] Thus dichotomizing the pain pathways into a lateral and medial system is much too simplistic. . 3.4. Common Supraspinal Sites Depicted by Neuroimaging Pain Studies Different brain regions have shown activation during acute painful stimulation, in terms of functional neural imaging. The meaning of such activation is the center of extensive debate. In this section, the most commonly activated brain structures are described and the functional relevance of these findings is discussed. 3.4.A. Anterior Cingulate Cortex (ACC) The ACC is one of the most commonly investigated brain structures. It is located above the corpus callosum (Figure 1), and is one of the many components of the brain hemispheres’ medial wall. In recent studies, the ACC has been divided into two main components, based on the cytoarchitecture, organization and function. The two components are the anterior or rostral portion (aACC), also called the perigenual cingulate, and the posterior or caudal portion (pACC). The pACC is subdivided into a dorsal portion and a ventral portion, which is also called the midcingulate region (Figure 2).[34] [35] 7 Fig 1. Magnetic resonance image of the left anterior cingulate cortex located by the Talairach coordinates (x,y,z)=(5[L],27[A],23[S]). The ACC has been directly and indirectly related to the neural circuitry of pain. There have been reports of ACC involvement in pain, anticipation of pain, [9] anxiety, [36] attention and motor responses. [37] It has been suggested that the rostral portion of the ACC (perigenual cortex) subserves the affective reaction to pain. In other words, activity in the rostral ACC is directly related to the unpleasantness of the stimuli, [38],[6, 31, 39]. Apparently this region of the cingulate cortex also plays an important role in processing anxiety [36] [40]. Based on experimental studies in healthy subjects, activity within the ventral portion of the pACC (midcingulate cortex) has been linked to thermal painful stimuli. Recent evidence supports the hypothesis that the midcingulate cortex possesses pain intensity encoding properties. [41] [42] They demonstrated that the midcingulate cortex was activated by painful stimuli only and that the amount of activation was proportional to the intensity of the painful stimulation. Pain-related motor responses have been related to activity in the dorsal subdivision of the pACC. [34] 8 Fig. 2 Schematic representation of the anterior cingulate cortex and its subdivisions. In blue = anterior portion of the ACC (perigenual cingulate), in red and green = posterior portion of the ACC (red = midcingulate cortex) The ACC appears to exert a significant role in the pain modulatory system.[10] Functional MRI data have shown that the anticipation of a painful stimulus resulted not only in activation of the ACC, but also in higher pain ratings that were similar to actual painful stimuli. [9] Another study showed that distraction from a painful stimulus also activated ACC neurons, and this correlated with a decrease in the reported pain intensity. [34] These results suggest that the ACC modulatory influence can be either inhibitory or excitatory in nature. The current literature suggests that the ACC is a major CNS player in chronic neuropathic pain conditions. Increased activation of the midcingulate cortex has been observed in some neuropathic conditions, [21], or after capsaicin application [43] Due to conflicting data in the reports on neuropathic pain conditions, Peyron [28] suggested 9 that the level at which the deafferentation occurs (peripheral or central) may influence the activity in the midcingulate cortex. This was based on the fact that decreased activity in the midcingulate cortex has been shown to occur when an allodynic region is stimulated in patients who suffered medullary infarcts. On the other hand, increased activity within the midcingulate was demonstrated following stimulation of an allodynic area secondary to peripheral nerve lesion. [44] Taken together, the functional meaning of ACC activity upon experimental stimulation can be very puzzling, since it is very likely that this structure possesses a variety of functions within the CNS.[45] More detailed investigations are warranted to further elucidate what the true functional roles of this cortical zone are. 3.4.B. Primary (SI) and Secondary (SII) Somatosensory Cortex The primary somatosensory cortex (SI) is located in the postcentral gyrus and receives somatosensory input from the ventral posterolateral and ventral posteromedial nuclei of the thalamus. The secondary somatosensory cortex (SII) is positioned immediately posterior to the SI and constitutes one of the functional components of the parietal lobe of the brain. Both SI and SII are limited inferiorly by the Sylvian fissure which separates the temporal from the parietal lobe in this specific region. [46] Despite the fact that activation within the SI and SII has been correlated to painful stimulation, [47], [48] the functional significance of activation of either region remains to be elucidated. It has been suggested that both regions (SI and SII) are related to encoding spatial, temporal and intensity aspects of noxious input, [49] [ Bornhovd, 2002 #384],[50] [Peyron, 2000 #60] however, neither one of the somatosensory cortices are solely 10 involved in the interpretation of noxious input because they are activated by innocuous sensory stimulation as well. [51] 3.4.C. Insula The insular cortex lies deep beneath the lateral cerebral fissure (Figure 3) and it is divided into two different components: anterior and posterior. [46] The posterior portion of the insula is localized in close proximity to the SII, which is why many PET studies could not differentiate between activation in the SII and posterior portion of the insular cortex. [52] The insula has been implicated in both affective and sensory- discriminative aspects of the pain experience. [6], [31], [48] Careful investigation of the insular cortex using fMRI indicates that the posterior portion appears to be involved in the sensory-discriminative dimension of the pain experience. [37] In addition, it has been described as the thermosensory cortex because of its ability to encode thermal stimulus intensity. [53] The anterior portion of the insula seems to be a component of the affective-motivational aspect of the pain neuromatrix. Activity within this region may be affected by attention towards the painful stimuli. [37] Fig. 3. Magnetic resonance image of the left insular cortex located by the Talairach coordinates (x,y,z)=(34[L],0[A],4[S]) 11 3.4.D. Thalamus The thalamus is a component of the diencephalon (Figure 4). Previously, it has been described as a relay station located between the spinal cord and the cortex [33, 54]. The thalamus is an important relay station for both the medial and lateral pain system. With respect to the pain experience, the roles of three thalamic regions have been described. The posterior nuclei are involved in conduction and processing of painful stimuli, the ventral posterior nuclei are thought to participate in the localization process of the pain stimulation and the medial nuclei are implicated in the affectiveaversive nature of the painful stimuli. [55] Recent advances in spatial resolution with fMRI have made it possible to evaluate the function of the thalamus in a more detailed manner. [56] For instance, thalamic activation has been demonstrated during acute phasic heat stimulation. [48, 57] The thalamus possesses a great number of interconnections and inhibitory synaptic networks. Therefore, bilateral activation of the thalamus may not only reflect a sensory response, but could be related to the arousal reaction induced by the painful stimuli as well. [28] Thalamus hypoactivity has been linked to chronic pain conditions [20, 58]. The facts that thalamic stimulation can produce analgesia and that thalamic stimulating devices have been shown to reduce pain in some neuropathic pain states [59] reinforce the premise that decreased thalamic activity may be one of the pathophysiological markers for chronic pain. [60] Taken together, these data suggest the thalamus is a dynamic CNS structure that relates to the sensory-discriminative and affectivemotivational dimensions of the pain experience. It is also very likely that activity in the thalamus is compromised in chronic neuropathic pain conditions. 12 Fig. 4. Magnetic resonance image of the left thalamus located by the Talairach coordinates (x,y,z)=(9[L],15[P],9[S]) 3.4.E. Prefrontal Cortex The prefrontal cortex is the most anterior portion of the frontal lobe (Figure 5) and comprises Brodmann areas 9 and 10. The prefrontal cortex has several connections to other brain structures, such as the dorsomedial nucleus of the thalamus, other cerebral lobes and the hypothalamus [61]. The prefrontal cortex presumably plays a crucial role in memory retrieval [62] and attention processing in normal individuals, when they experience an experimentally induced noxious stimulus [41, 49]. Apparently, the prefrontal cortex is activated by painful heat application, but the amount of activation does not increase with increased stimulus intensity (on- and off-response). [41, 49] Clearly, pain intensity encoding is not a task of the prefrontal cortex. 13 Fig 5 Magnetic resonance image of the left dorsolateral prefrontal cortex located by the Talairach coordinates (x,y,z)=(42[L],8[A],29[S]) Prefrontal cortex functioning has been investigated in chronic pain patients. Apkarian et al [22] reported that in the sympathetically maintained pain state, subjects display prefrontal hyperactivity in response to painful stimuli that could be reversed after pain blockade. Hsieh et al. [21] also found increased activity in parietal and prefrontal cortices in chronic neuropathic pain patients. Hence, the prefrontal cortex may play an important role in the pathophysiology of some chronic pain conditions. 3.4.F. Other Brain Regions Several studies demonstrated activation of other brain structures such as the inferior parietal cortex, cerebellum and amygdala during painful stimuli. These brain areas were not always consistently activated and the functional significance of their activation within the pain neuromatrix is even less understood than the previously discussed brain structures. [31, 43] [41, 63] 14 3.5. Functional Neuroimaging in Chronic Pain As previously mentioned, there are few neuroimaging studies of chronic pain conditions. In this section, these studies are discussed in a more detailed manner, since they are important to the development of the present study’s hypothesis. Iadorola et al. [20] studied 5 patients with chronic neuropathic pain with oxygen15 water bolus PET. Four of these patients had pain confined to one lower limb and one patient had ophthalmic post-herpetic neuralgia. The authors found that, in patients, thalamic activity on the side receiving input from the symptomatic limb was decreased compared to activity on the side receiving input from the asymptomatic limb and compared to activity generated in control subjects. The decrease in thalamic activity was most robust in anterior dorsal and posterior ventral regions. Earlier, Di Piero [58] who studied 5 cancer pain patients with PET found contralateral decrease in thalamic activity as well, and also found this in posterior and anterior nuclei. Di Piero [58] and Iadorola [20] suggested that decreased thalamic activity may be a clinical feature common to a wide variety of chronic pain disorders. It has been postulated that these changes in thalamic activity may lead to a loss of central inhibition. Using fMRI, Apkarian et al. (2001) studied 7 subjects with unilateral sympathetically maintained pain limited to one hand before and after the SMP was suppressed by sympathetic blockade. [22] In the clinical pain state, the subjects showed increased prefrontal activity, and decreased parietal cortical and contralateral thalamic activity in response to an additional painful stimulus. These activation patterns were reversed after pain was eliminated by a sympathetic block (bupivacaine 0.2%).The authors concluded that the altered activation patterns within the prefrontal and parietal 15 cortex and the thalamus may play a crucial role in the pathophysiology of sympathetically maintained pains. A similar study was previously done by Hsieh et al. [21] who studied 8 chronic neuropathic pain patients before and after regional nerve block with PET. During the clinical pain status, they found increased activity in bilateral insula, parietal and prefrontal cortices and posterior cingulate and right anterior cingulate (BA24) regions. They also noted decreased activity in the contralateral posterior thalamus. No differences were found in the activity of SI and SII regions as it related to the pain status before and after regional nerve block. These findings suggest that abnormal brain responses may underlie sympathetically maintained pain and that prefrontal/limbic networks may be extensively involved. Gracely et al. [64] conducted an fMRI study whereby 16 fibromyalgia patients were compared to 16 gender and age matched healthy controls. They reported their results in terms of number of activated clusters for each group. For the same subjective experience of pressure induced pain they found 19 regions of increased regional cerebral blood flow in healthy controls and 12 regions of increased regional cerebral blood flow in fibromyalgia patients. There were 7 regions common to both groups. Statistical comparison between the two groups revealed 13 regions with higher activation in the patient group. Their results strengthen the hypothesis that fibromyalgia is a cortical or subcortical pain augmentation disorder. A similar study [65] also found that chronic low back pain and fibromyalgia patients display more extensive common patterns of activation when compared to normal volunteers. Together, these studies also corroborate with the augmented central pain processing theory.[64, 65] 16 In summary, the available neuroimaging studies seem to suggest that alterations in brain activation patterns are consistent findings in chronic pain patients. These alterations have been observed not only when comparing patients to controls, but also when comparing patients during the painful state and a pain-free situation. The ACC, thalamus and prefrontal cortex seem to be areas where these alterations primarily occur. Nonetheless, one has to take into account that the reported studies involve different methods and heterogeneous clinical pain conditions. 3.6. Functional Brain Imaging in Orofacial Pain Craniofacial pain conditions, such as masticatory muscle pain, TMJ pain, dental pain, trigeminal neuralgia, burning mouth disorder and migraines are mediated by the trigeminal nerve (CNV). The CNV possesses unique brainstem mechanisms and nociceptive transmission characteristics. The CNV has a unique somatotopical organization, as it relates to a group of nuclei at the brainstem level: the trigeminal spinal tract nucleus, the main sensory nucleus and the trigeminal motor nucleus.[30] The trigeminal nerve also has distinctive macroscopic anatomical characteristics, such as the intracranial location of the trigeminal nerve ganglion and its relationship to adjacent structures. These peculiar features of the CNV may account for significant differences in the central neural network of trigeminal pain versus pain in the rest of the body. Brain imaging studies have been used to explore the pain “neuromatrix”. However, few studies focused on the central pain network related to activation of the trigeminal nerve. With regard to the CNV, most of the functional brain imaging studies 17 were primarily intended to gain insight in the pathophysiology of headache disorders, such as cluster headache, [16] SUNCT (short lasting neuralgiform headache with conjunctival injection and tearing) [66] and migraine. [67, 68] Thus, so far, the available studies have focused mainly on midbrain, pons and hypothalamic grey activation evoked by input from the ophthalmic nerve branch (CNV1) of the CNV and the possible role of these areas as neurovascular pain generators. Derbyshire et al. (1994) investigated patients with “atypical facial pain” with PET. However, the actual painful and non-painful thermal stimuli were applied on the back of the right hand. They reported an increased regional cerebral blood flow (rCBF) in the ACC and decreased blood flow in the prefrontal cortex and hypothesized that this pattern of activation may compromise central inhibitory influences towards the nociceptive input therefore contributing to the maintenance of the pain condition. [69] Kupers et al. (2000)[59] presented a PET study whereby a single patient suffering from atypical facial pain was successfully treated with a thalamic stimulator. They were able to perform functional imaging of the patient during three different states: before thalamic stimulation (pain state), during and after thalamic stimulation (pain-free states). By comparing the pre- and post-thalamic stimulation status they found that there were significant rCBF increases in the prefrontal and anterior insular cortices, hypothalamus and periaqueductal gray that were related to the presence of pain. Interestingly, there were no significant rCBF changes observed in thalamus, SI, SII and ACC. Significant rCBF decreases were observed in the substantia nigra/red nucleus and in the anterior pulvinar nucleus. The authors discussed their data emphasizing possible differences in the cerebral processing of acute and chronic pain, however their 18 results need to be analyzed with caution since it reflects measurements of a single individual. Thayer and Friedman (2002) commented on the role of such central networks in light of maladaptive behaviors or brain states, which they contributed to dysfunctional inhibitory processes. They argued that dysfunction in CNS regions could lead to “disinhibition”, which would prohibit adaptability to normally innocuous stimuli [70]. More recently, Kupers et al. (2004)[71] have carried out a PET study that investigated the cerebral activation network related to experimental masseter muscle pain and skin hyperesthesia overlying the painful muscle. They reported that painful stimulation of the masseter was related to increased rCBF in the dorsal-posterior insula, ACC, prefrontal cortex, right posterior parietal cortex, brainstem, cavernous sinus and cerebellum. They also found that there were no rCBF changes in the SI and SII, however, mechanical stimulation of the skin overlying the masseter muscle was associated with increased rCBF of the SI face representation. Hyperesthesia was also associated with rCBF increases in the subgenual cingulate and ventroposteromedial and dorsomedial thalamus. Based on their findings they stated that deep muscle pain and superficial cutaneous stimulation may possess a different CNS representation. Differentiation of deep visceral and cutaneous pain in human brains has also been demonstrated by Strigo et al. (2003)[72]. The authors implied that different patterns of activation within insular, SI, motor, and prefrontal cortices may account for the ability to discriminate visceral and cutaneous pain. They also stated that the different emotional, autonomic and motor responses associated with these different sensations may account for the observed different pattern of activation. 19 Functional MRI data of brain activation produced by stimulation of different branches from the CNV, other than V1, are scarce. It is largely unknown whether the CNS network of connections related to trigeminal input is similar to the areas activated by stimulation in other areas of the body, such as the extremities. De Leeuw et al. studied fMRI BOLD changes in different brain regions following acute phasic heat stimulation of the V3 branch in normal subjects, and found that heat stimulation of the trigeminal system resulted in activation of brain regions similar to those reported in studies of peripheral body parts. [73] DaSilva et al. [74] have also explored activation of CNS regions created by thermal stimulation of the trigeminal system in healthy subjects. They focused their analysis on the somatotopic arrangement of the three trigeminal branches in the trigeminal spinal tract nucleus, thalamus and somatosensory cortex. Contralateral activation of ventroposteromedial thalamic nucleus was observed after CNV stimulation, as opposed to contralateral ventroposterolateral nucleus activity displayed when the thumb was stimulated. They also reported that SI activation pattern was similar to the trigeminal spinal tract nucleus laminar organization (V2 rostral, V1 caudal and V3 medial) and that this activity pattern in SI was not the same as the one created by the stimulation of the ipsilateral thumb. Iannetti et al. [75] investigated the representation of the different divisions of the trigeminal nerve within SI and SII in humans using non-painful mechanical tactile stimulation. They mechanically stimulated the ophthalmic and mandibular trigeminal branches of 14 healthy individuals and encountered contralateral activation of SI and SII that largely overlapped. They also found that while V3 stimulation activated the contralateral somatosensory cortices alone, V1 stimulation provoked activation in the 20 ipsilateral and contralateral sides of SI and SII. This study illustrated some of the distinct cortical representations inherent to the trigeminal nerve. It is important to notice that these authors were only investigating tactile cortical representation of the trigeminal nerve and not pain. Functional MRI has also been used to locate and identify brainstem and cervical spinal cord nuclei that are related to cranial nerves sensory and motor pathways. In an fMRI study, Komisaruk et al. [76] used cross-correlation analysis of regional blood oxygen level-dependent (BOLD) signal intensity during specific motor and sensory procedures such as brushing the face, left- and right eye movement, smiling and lip puckering, pushing the tongue against the hard palate, swallowing, tasting a sweetsour-salty-bitter mixture, finger tapping and tongue movement and trapezius muscle activation. They were able to locate the brainstem trigeminal main sensory nucleus among other cranial nerves nuclei. Painful stimulation was not investigated in this study. In summary, data from the above mentioned studies suggest that in orofacial chronic pain states (atypical facial pain) it seems like the finding of a dysfunctional brain network is also observed. The thalamus, prefrontal cortex and ACC appear to be the major players in such dysfunction. During thermal acute pain stimulation it is possible that the trigeminal nerve possesses unique thalamic transmission pathways with activation of the ventroposteriormedial nucleus instead of the ventroposteriorlateral nucleus. 21 3.7. Burning Mouth Disorder Burning mouth disorder (BMD) is defined as an idiopathic, constant, most commonly bilateral, burning sensation involving intra-oral soft tissues (tongue, lips and oral mucosa).[77, 78] According to epidemiological studies its prevalence in the general adult population is estimated to be between 1 and 3% [79, 80]. In the United States more than 1 million people suffer from BMD. [81] Clinical studies indicate that postmenopausal females are more frequently affected by BMD [82]. For a complete review of BMD epidemiology and clinical characteristics refer to Fraikin et al. [83], Grushka et al. [78], Scala et al. [84] and Rhodus et al. [85] It has been proposed that a distinction should be made between BMD and oral burning. Whereas the term burning mouth disorder refers to an idiopathic burning of the intra-oral tissues, the term oral burning has been suggested to imply that the burning sensation is secondary to certain pathological states. These pathological states include diabetes mellitus [79, 86], xerostomic drugs, nutritional deficiencies, salivary gland pathology, mucosal pathology (candidiasis, lichen planus, geographic tongue), gastric esophageal reflux and parafunctional habits. Rhodus et al. [85, 87] suggest that the treatment of oral burning complaints should aim at identification and management of possible contributing/precipitating factors as the ones listed above. After ruling out any contributing factors, or in the absence of a positive response of the burning complaint to management of these contributing factors, one should consider the possibility of an idiopathic condition and therefore name it, more appropriately, BMD. Other authors have proposed the classification of burning mouth syndrome as being either primary or 22 secondary in light of its relationship to the same etiological issues mentioned above. [84] The lack of consensus with regard to a clear definition of what is generally called BMD makes it extremely difficult to review and interpret the results of studies about this condition. A good illustration of such difficulties is the fact that some authors [88, 89] believe that dysgeusia and xerostomia are concomitant findings and symptoms of what they call burning mouth syndrome. Alternatively, other researchers believe that these factors may have a causal relationship with the complaint of burning in the oral cavity. This relationship, however, is not well understood and can only be established by longterm studies that evaluate for instance, whether pain reduction or elimination has any impact on the dysgeusia and xerostomia or vice-versa. The view that BMD is primarily a psychogenic disorder has lost support as a result of recent studies.[90] It is a common observation that depression and anxiety disorder are very frequently reported by patients with chronic pain conditions.[91, 92] Eli et al. [93] have demonstrated that despite of their elevated psychological profile, BMD symptoms may not be correlated with stressful life events. In fact, Carlson et al. did not observe any significant clinical elevations on any of the SCL-90R subscales, including depression, anxiety, and somatization in a sample of 33 BMD patients. Great controversies still exist about the psychogenic factors and how they relate to BMD. Interestingly, several studies indicate that the psychological profile abnormalities may relate to the patients’s poor coping skills regarding their pain condition. [94, 95] The pathophysiology of BMD is largely unexplained. Yet several reports in the literature suggest that BMD is likely a neuropathic pain condition. The first line of 23 evidence supporting this hypothesis comes from the clinical trials that demonstrate therapeutic effects of anti-epileptic agents, such as clonazepam [96-98] for BMD. Secondly, sensory abnormalities have been shown to exist in patients suffering from BMD. Svensson et al.[99] stimulated the intra- and peri-oral tissues with an argon laser and showed that thermal sensory thresholds were higher in BMD patients. They also reported that stimulation at sensory threshold levels frequently created a faint pinprick sensation in patients while normal subjects only described a perception of warmth. Ito et al. [100] have also found higher thermal pain thresholds in patients with BMD. Grushka et al. [101] did not observe differences in thermal pain thresholds but they reported that patients with BMD had decreased pain tolerance to thermal stimulation. Gao et al. [102] showed abnormal sensory function in patients with BMD following electrical stimulation of the tongue. All of these studies share the opinion that BMD is very likely a neuropathic pain condition as it may represent abnormal transduction and/or processing of input arising from the trigeminal afferent fibers to the CNS. Nevertheless, to date there is still a great deal of controversy regarding the likelihood that BMD is a neuropathic disorder. Moreover, some authors appear to implicate peripheral neuropathic pathophysiological mechanisms [88, 89, 102-107], while others believe that central neuropathic mechanisms are main players in BMD.[108-112] The upcoming section will discuss the studies implicating peripheral and central mechanisms in more details. Proponents of a peripheral pathophysiology Grushka et al. [88] suggested that BMD may be related to selective damage to the chorda tympani and glossopharyngeal nerves (sensation of taste). They 24 hypothesized that this deafferentation may result in a loss of inhibition to pain that ultimately leads to BMD. Nagler and Hershkovich [89] performed a taste and salivary analysis in BMD patients and normal controls. They observed sialometrical and sialochemical discrepancies between the control and the patient groups. In light of their findings, they proposed that an oral neuropathy or neurologic transduction interruption secondary to salivary compositional changes might be an etiological factor in BMD. Gao et al. [102] demonstrated increased trigeminal nerve sensitivity and alterations in neural transmission within the peripheral nervous system. Lauritano et al. [103] demonstrated the existence of subclinical polyneuropathy in 50% of patients with BMD. In particular, they detected a loss of function in small diameter nervous fibers. Histological examination of tongue mucosa revealed a moderate atrophy in 70% patients. Heckman et al. [104] also demonstrated disturbances in oral mucosal blood flow in patients with BMD that would support the peripheral pathophysiology hypothesis. Additional support for this hypothesis comes from clinical trials supporting the use of alpha-lipolic acid for burning mouth disorder. Alpha-lipolic acid is a potent antioxidant mitochondrial coenzyme that has shown to posses neuroprotective function. The use of alpha lipolic acid is though to increase the levels of intracellular glutathione and eliminate free radicals possibly produced by the altered peripheral nerve fibers. [105, 106, 113] Proponents of a central pathophysiology Central nervous system mechanisms involved in the pathophysiology of BMD have been carefully investigated by a group of researchers from Finland. These authors provided preliminary data implicating the CNS in the pathophysiology of BMD. Jaaskelainen et al. [108] showed that BMD patients displayed blink reflex abnormalities. 25 They hypothesized that the abnormal reflexes could be due to a decreased dopaminergic inhibition mediated by the basal ganglia and their connection to the facial motor nuclei. To further test their hypothesis, they performed a fluorodopa-PET study in 10 BMD patients and 14 normal volunteers. [109] They demonstrated that BMD patients had a dysfunction of the nigrostriatal dopaminergic system which confirmed their neurophysiologic observations. These investigators also compared 10 BMD patients with 11 healthy volunteers to explore differences in the striatal dopamine D1 and D2 receptors with PET. This study revealed a bilateral decrease in the D1/D2 ratio in the putamen. According to the authors, this possibly reflects a decline in endogenous dopamine levels in BMD patients.[111] Similar results were observed by the same researchers in patients with atypical facial pain. [110] Hence, the authors discussed the contention that disruption of the nigrostriatal dopaminergic system may primarily affect the regulation of nociception of the trigeminal system and cause a loss of sensory inhibition. These findings are in agreement with experimental data suggesting a role for the basal ganglia in the various dimensions of the pain experience.[114] Based on their preliminary results, the above mentioned group of authors developed a more robust investigation with 52 BMD patients. For this larger trial, they used quantitative sensory tests (QST) and blink reflex recordings to investigate the neural mechanisms of BMD related pain. Abnormal findings, such as, increased excitability of the blink reflex and abnormal sensory thresholds (warm allodynia or hypoesthesia) were recorded in the great majority of patients. The authors felt that their data strengthened the hypothesis that BMD disorder is a neuropathic condition and very likely a combination involving a 26 peripheral neurogenic mechanism(s) and an increased excitability of higher centers within the CNS.[112] In summary, the available literature suggests that BMD is a neuropathic entity with peripheral and central neural pathophysiology. It is important to recognize that these mechanisms need further elucidation. The only available neuroimaging data to date comes from one PET study implicating basal ganglia nuclei in the pathophysiology of BMD.[109] It is not known whether other CNS sites are also implicated in pathophysiology of BMD. Functional MRI studies of BMD are an unexplored field of investigation. In general, fMRI studies have provided a significant improvement in the understanding of pain-related CNS functioning and appear to be a promising modality for the investigation of disorders in which CNS mechanisms are potentially involved. 3.8. Hypothesis Since we believe that BMD is in fact a painful neuropathy with substantial involvement of the CNS in its pathophysiology, we hypothesize to demonstrate increased BOLD signal intensity as well as larger clusters of activity within the ACC, and decreased BOLD signal intensity and smaller clusters of activity involving the thalamus in BMD as compared to the normal volunteers. In other words, we expect to demonstrate that BMD patients have similar brain activation patterns to those observed in previous neuroimaging studies pertaining patients with chronic neuropathic pain conditions. These studies demonstrated somewhat consistent altered patterns of brain 27 activation that are likely related to the chronic neuropathic pain condition.[115], [116], [21], [20], . [58] [59]. Copyright © 2004, Romulo J.C. Albuquerque 28 4. Materials and Methods 4.1. Study Design: The study is a block design fMRI study, consisting of eight female patients with burning mouth disorder (BMD) and a control group of eight normal subjects. 4.2. Study Population: Participants were eight right-handed female patients, who were diagnosed with burning mouth disorder and eight right-handed control subjects matched by gender, age and menstrual status. The age matching procedure consisted of recruiting subjects within a maximum of five years age difference. The criteria for diagnosis of BMD were an at least 3 months old history of an idiopathic burning sensation of the intraoral soft tissues. All patients were previously screened for a variety of disorders that may account for burning of the intra-oral soft tissues. Exclusion criteria included patients with candidiasis, nutritional deficiencies, salivary flow disturbances, lichen planus or geographic tongue. Patients who were taking xerostomic medications and angiotensin converting enzyme (ACE) inhibitors were excluded, if a positive relationship was clinically established between the use of the drug and the intra-oral burning. [87] [87] We chose 8 subjects in each group because, as a general rule, results in fMRI studies do not seem to improve beyond 10 to 12 subjects. With 10 subjects, the variance and heterogeneity of subjects (the noise) increases faster than the additional signal. Activation maps from a previous study [73] with nine subjects showed regions that were activated with t values ranging from t= 3.7 to t=6.62 at sites of peak activation. These values correspond approximately to p values < .0001 and the activations were in regions where an effect was predicted (thalamus, insula, PFC, ACC, SI). Becerra and 29 co-workers [48] studied two groups of eight subjects who underwent identical stimulation protocol to evaluate reliability and consistency. They found no significant differences in activation between the two groups. Furthermore, the power of fMRI studies not only depends on the number of subjects, but also on the number of measurements during each scan. Each scanning session includes 128 consecutive MRI signal measurements in which the signal intensity is recorded for each volumetric (3.5mmX3.5mmX3mm) space of the brain over time. Female patients were chosen as the study population to decrease the amount of variability in fMRI signaling within the subjects. It is not well known how gender might affect fMRI signal. It is also noteworthy that BMD is significantly more prevalent in females with a male/female ratio of 6:1[79] [80] [78]. We chose to include only right-handed persons to reduce further potential heterogeneity of the sample. In general, left-handed people seem to have a less pronounced cerebral functional and anatomical asymmetry than right-handed people. [117, 118],[119] 4.3. Subject Recruitment Method: The patients were recruited from the Orofacial Pain Center of the University of Kentucky. Participants had to be native speakers of American English, have pain for more than 3 months and have burning pain levels above or equal to 3/10 where “0” represents no burning pain and “10” represents the most extreme burning pain. Patients with present neurological, psychological and chronic pain conditions, other than the burning mouth disorder were excluded. The patients were asked to discontinue any medications that could potentially affect brain function, such as anti-depressants, 30 anticonvulsants, antipsychotics and analgesics for at least 4 half-lives prior to the scanning session. All patients were instructed to withdraw from caffeine on the day of the scanning session. Patients who felt that they could not discontinue their medications or caffeine were excluded from the study. The normal volunteers (control group) were recruited by flyers that were posted throughout public areas of the University of Kentucky campus. All participants were paid US$ 50.00 for their participation. This study was approved by the Office of Research Integrity from the University of Kentucky. 4.4. Research Procedures: 4.4.A. Pre-fMRI Assessments 4.4.A.1. Psychometrics. Patients and normal volunteers completed a battery of psychometric questionnaires, consisting of the Symptom Check List-90 (SCL-90R), Beck Depression Inventory (BDI) and the State-Trait Anxiety Inventory (STAI). The SCL-90R is a 90-item self report questionnaire that yields nine symptom dimensions and 3 global indices of functioning. It is a measure of current symptom status. It has reliability coefficients ranging from r's=0.77-0.90 for the symptom dimensions. Measures of psychological status included the somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety and paranoid ideation subscales of the SCL-90R. Average scores for each subscale were obtained according to instructions outlined in the scoring manual. [120] The BDI [121] is a 21-item self report questionnaire that measures cognitive, affective, somatic and vegetative symptoms of depression. The BDI has shown strong internal consistency (α between .81 and 88) and is widely used in clinical and non-clinical samples [122, 123] The STAI [124] is a 40-item self 31 report questionnaire that measures state and trait anxiety using a 4-point scale ranging from “almost always” to “almost never”. This instrument also has shown good internal consistency (α between .90 and .93). 4.4.A.2. Thermal Thresholds and Stimulus Protocol Subjects were pre-exposed to the thermal stimuli sequence used in the fMRI session. First, pain thresholds were determined with the method of limits. [125] Threshold measurements were taken with a Peltier thermode (30 x 30 mm), which was positioned on the skin overlying the right masseter. When necessary, the stimulus temperature for heat pain was adjusted, so that the participant rated the painful stimulus at least “3 out of 10”, but not higher than “8 out of 10” where “0” meant no pain and “10” represented the worst imaginable pain. This was done to assure that the test protocol elicited pain, but not to an extent that would incur movement of the participant. The baseline adaptation temperature was set at 32°C in accordance with several previous publications. The thermal test sequence, as used in the scanner, started with a 35second period of a 32°C baseline temperature, followed by a 35-second period of warm (39.5°C) non-painful stimulation. After these non-painful temperatures, pulses of painful heat (47-49°C) were delivered during a 35-second period. After a sequence of painful stimuli, the thermode was brought back to adaptation temperature (32°C) for 35 seconds (Figure 6). Four of these sequences of baseline, warm and painful stimulation formed a complete thermal cycle. The stimulus temperatures were well below the limits of potentially tissue damaging temperature ranges. The patients were also instructed to grade on a scale from 0 to 10 how much burning they were experiencing (present burning index - PBI) right before engaging in the MRI scanning session. 32 Figure 6 Thermal stimulation paradigm (in degrees Celsius) 4.4.B. Functional MRI Session Protocol After the participants had completed the pre-fMRI test sequence described above, they were guided to the MRI scanner (1.5 Tesla vision system, Siemens, Munich, Germany). The fMRI session allowed for the collection of three-dimensional MPRAGE structural images for co-registration of fMRI data with anatomy, that enabled the transformation to standardized stereotaxic coordinates [61]. Functional MRI data were collected from 44 contiguous 3 (mm) thick axial slices beginning at the level of the inferior portion of the cerebellum and yielding whole-brain coverage. A gradient echo EPI sequence with TE= 45 (ms), TR= 4.0 (s), and FA=90o was used for functional imaging. The in-plane resolution was 3.5 (mm) x 3.5 (mm) with an image size of 64 x 64 pixels for a field of view of 228 (mm). Magnetic field homogeneity, particularly at the base of the brain, was carefully optimized using the field mapping and correction facilities of the VISION system (MAPSHIM). Following the anatomy scan, the fMRI session for each participant involved two complete thermal cycles in which stimulation 33 was delivered to the left side of the face in a blocked design with alternating epochs of baseline, warm, and noxious heat. Immediately after the fMRI session, patients were asked to grade the pain levels elicited by the thermal painful stimulation on their face on a scale from “0” (no pain) to “10” (most extreme pain). Our goal was to produce a similar subjective experience of pain in both groups. 4.5. Statistical Analysis 4.5.A. Psychometric and Demographic Data Analysis In order to detect possible significant differences between the patients and individuals from the control group regarding the psychometric tests and demographic information we performed an independent sample t-tests. It is important to note that the primary objective of this study was to investigate differences in brain activation patterns with fMRI and not to investigate psychometric or demographic differences. However, if present, observed discrepancies would need to be taken into account in the interpretation of our results 4.5.B. Functional MRI Data Analysis The statistical analysis was carried out with the Analysis of Functional Neuroimaging Software (AFNI). The functional images were corrected for motion artifacts with automated motion correction software (MATLAB and SPM99). [126]. The three-dimensional MPRAGE structural images were transformed into Talairach coordinates on an individual basis using AFNI Software. The anterior commissure (AC), posterior commissure (PC) as well as two midsagittal points were used to align the individual brains at the AC-PC plane. Other landmarks, such as most anterior, posterior, 34 superior, inferior and lateral points of the brain were also used in the Talairach transformation process. The EPI sequences consisted of 128 full brain images that were acquired in a timely manner. This means that every four seconds a full brain functional image was obtained. The 128 time points of the EPI sequences were then correlated with a time course box car reference function (.1D files). The reference profiles were designed appropriately so as to set up contrasts for the separate comparison of baseline temperature vs. warm temperature, baseline temperature vs. pain temperature and warm temperature vs. pain temperature. Thus, activation maps were calculated on a voxel-by-voxel basis for each of the three pairings of stimulus conditions in a particular run. Statistical parametric maps based on the mean fractional signal change and sample variance within each run were transformed and resampled by cubic spline interpolation as isotropic 2 mm voxels in the standard stereotaxic space of Talairach and Tournoux [61] using the AFNI software package [127] and spatially smoothed in MATLAB 5 (The MathWorks, Natick, MA) using an isotropic Gaussian spatial filter with sigma equal to 3 millimeters. Functional data were then merged across runs and across participants using the 3dmerge AFNI auxiliary software to generate average group activation maps for each pairing of stimulus conditions. Activation maps were created for each study group (patients and control subjects). Comparisons between the warm (39.5 oC) versus painful heat (47-49 oC) status were used for the construction of the statistical maps in each group. This is because the aim of the study is to compare supra-spinal mechanisms as it relates to painful stimulation in BMD patients versus normal individuals. We believe that by comparing warm to painful heat we construct 35 brain activation maps that relate to painful stimulation alone and not to the processing of a warm stimulus or a temperature change. It is also important mentioning that this research method is a block design fMRI study. As such, painful heat stimulation was always preceded by warm stimulation. Maps of the difference in activation between patient and control groups were created using an AFNI auxiliary program 3dttest, which allows for the execution of independent samples t-tests on a voxel-by-voxel basis for the two sets of fMRI three-dimensional data sets. A cluster analysis for each of the two groups was performed with the use of 3Dcluster and 3dclust AFNI auxiliary software. The cluster analysis allowed us to measure the total volume of activation throughout the entire brain. Clusters of activity of at least 1000 µl of volume and connectivity radius of 2mm were shown in the maps. The Talairach coordinates for the center of mass and the location of each cluster were recorded and used for comparison between the two groups. For didactic purposes the differences regarding the magnitude of fractional signal changes throughout different areas of the brain (3dttest) were reported as qualitative differences and the difference in the amount of total brain activation (cluster analysis) were regarded as quantitative differences. Copyright © 2004, Romulo J.C. Albuquerque 36 5. Results 5.1. Demographics and Psychophysical Tests This study included eight BMD female patients (mean age 49.1 ± 10.1) and eight pain-free female volunteers (mean age 50.3 ± 12.3) matched with regard to age, and menstrual or menopausal status. Six out of the eight patients were post-menopausal and two patients still had a regular menstrual cycle. The two patients and two controls with a regular menstrual cycle underwent MRI scanning during the low estrogen phase, two days following the onset of menses. There were no significant differences between the two groups regarding age (p=.845). The BMD patients reported a mean present burning index of 4.3 ± 2.1 on a scale from “0” (no burning) to “10” (most extreme burning). The mean duration of the BMD was 60.5 ± 38.4 months. A detailed description of the patient population is shown in Table 1. There were no significant differences between the two groups related to thermal pain thresholds, the pre-fMRI pain rating, the test temperature applied during the fMRI session, and the post fMRI pain rating. The pain ratings were measured on a scale from “0” (no pain) to “10” (most extreme pain)(Table 2). The psychometric tests revealed significant differences between the two groups regarding the SCL-90 subscales for somatization, interpersonal sensitivity and anxiety. The other SCL-90 subscales did not differ between groups (Table 3). There were no differences in the BDI and STAI (Table 4). 37 Table 1. Detailed description of the patient population Pain Location Age PBI Duration Patient # of Pain [yrs.] [months] Tongue 41 60 7 1 and Palate Gingival and 4 71 120 2 Buccal Mucosa Gingiva and 3 47 60 3 Buccal Mucosa Tongue 49 36 8 4 and Palate Gingiva and 3 42 36 5 Buccal Mucosa Tongue and 3 55 118 6 Buccal Mucosa Tongue and 3 40 24 7 Buccal Mucosa Tongue 48 30 3 8 and Palate 49.1 Mean 48 4.3 (10.1) (SD) Menstrual Status HRT PM No PM No PM No PM No PM Yes PM No Regular No Regular No - - PBI = present burning index on a scale (0-10); HRT = hormone replacement therapy; SD = standard deviation; PM = post-menopausal 38 Table 2. Comparison between patients with Burning Mouth Disorder (n=8) and controls (n=8) regarding the psychophysical data. Controls Psychophysical Patients Mean Mean tt-value p-value Measures t-scores ± SD Scores ± SD Thermal Pain 45.4 ± 4.8 47.4 ± 2.6 -1.04 .322 Threshold (oC) Test Temperature 47.6 ± .9 48.1 ± .8 -1.14 .273 Applied During the fMRI Session (oC) Pre-fMRI Pain 5.6 ± 1.9 5.3 ± 1.7 .43 .677 Rating (0-10) Post fMRI Pain 7.1 ± 1.4 5.8 ± 1.8 1.75 .101 Rating (0-10) SD = standard deviation Table 3. Comparison between patients with Burning Mouth Disorder (n=8) and controls (n=8) regarding the SCL-90 subscales SCL-90R Patients Mean Controls Mean t-value p-value Subscales t-scores ± SD t-scores ± SD 61.6 ± 13.2 47.1 ± 13.1 2.21 Somatization .044 Obsessive 64.3 ± 10.5 53.3 ± 12.1 1.86 .083 Compulsive Interpersonal 60.0 ± 10.6 49.9 ± 7.7 2.19 .046 Sensitivity 58.3 ± 10.1 52.6 ± 10.5 1.05 .313 Depression 59.9 ± 8.7 48.0 ± 10.7 2.41 Anxiety .030 52.5 ± 9.6 52.0 ± 14.0 0.08 .935 Hostility 51.9 ± 9.8 46.9 ± 8.1 1.11 .285 Phobic Anxiety Paranoid 55.3 ± 10.8 46.3 ± 8.1 1.89 .080 Ideations 56.4 ± 11.8 53.5 ± 10.4 .517 .613 Pscychoticism SD = standard deviation 39 Table 4. Comparison between patients with Burning Mouth Disorder (n=8) and controls (n=8) regarding the BDI and STAI scores Controls Patients Test-Scores Mean Scores Mean Scores t-value p-value ± SD ± SD 12.5 ± 13.1 7.4 ± 7.1 .98 .346 BDI 40.6 ± 13.7 29.8 ± 10.6 1.78 .097 State Anxiety 43.0 ± 13.3 37.3 ± 12.8 .88 .392 Trait Anxiety BDI = Beck Depression Inventory; STAI = State Trait Anxiety Inventory; SD = standard deviation 5.2. Functional MRI Data Analysis 5.2.A. Individual Group Analysis Statistical maps were constructed and analyzed for the BMD group and the control group individually. Voxels in which significant differences in the fractional signal change were observed (Z=3.0; p< 0.005) are shown in figure 7 for the BMD and figure 8 for the control subjects. The maps display activation in areas that include the ACC (BA32/24), the right and left pre-central gyrus, the right post-central gyrus, the right and left thalamus, the right insula, the right medial frontal gyrus, the right middle frontal gyrus, the right and the left inferior parietal lobule, right and left precuneus and cerebellum. The left lingual gyrus and the left posterior cingulate gyrus were activated in volunteers but not in patients. 40 Figure 7. Activation map of the BMD group (n=8) BMD Group (Warm vs. Pain) Cerebellum Thalamus Precuneus Post-central Gyrus Insula ACC (BA24/32) Pre-central gyrus Figure 8. Activation map of the control group (n=8) Control Group (Warm vs. Pain) Cerebellum Lingual Gyrus Thalamus Post-central Gyrus Insula ACC (BA24/32) Pre-central gyrus 41 5.2.B. Between Group Analyses 5.2.B.1. Qualitative Differences Statistical comparison (t-test) between the BMD and control group’s activation maps revealed significant differences in the ACC (BA32/24) and bilateral thalamus. In addition, we detected differences in the following areas: left lingual gyrus, left precuneus, right precuneus, right middle frontal gyrus, right pre-central gyrus and right inferior semilunar lobule of the cerebellum. The activation maps corresponding to the above mentioned differences are presented in figure 9. The ACC (BA32/24) and the right and left precuneus showed greater fractional signal change in patients than normal volunteers. In the remaining areas where a significant difference was detected there was less pronounced fractional signal change in patients than in controls (Table 5). Figure 9. Activation map of the comparison between BMD group (n=8) and control group (n=8) BMD Group vs. Control Group BMD > Control Control > BMD Cerebellum Lingual Gyrus Thalamus Precuneus ACC (BA24/32) Middle Frontal Gyrus Pre-central gyrus 42 5.2.B.2. Quantitative Differences As a general measurement of brain activation, we calculated the total volume of activation for each group of subjects (BMD and controls) using a cluster size threshold of 1000 µl (approximately 27 voxels) and voxel connectivity radius of 2mm. This analysis revealed that the BMD group (24432 µl) displayed less volumetric brain activity when compared to the control group (92528 µl). To better categorize this discrepancy in the amount of activation between the two groups we also compared the two groups taking into account the total number of separate clusters above the 1000 µl threshold in each group. The BMD group cluster analysis revealed 4 large clusters of activity while the control group had 10 clusters. Tables 6 and 7 display the Talairach coordinate for the center of mass as well as the size of each of the detected clusters in the BMD group and control group respectively. It is important to notice that the total volume of activation displayed in Tables 6 and 7 will be slightly smaller than the total volume of activation reported above. This is because during inspection of the statistical maps we detected a large cluster of activity embracing three distinct brain regions in the statistical maps of the control group. This large cluster in reality represented three separate clusters connected by a small number of voxels. We decided to erode the data in order to separate these three clusters. For a fair comparison the activation maps of both groups were eroded. This was done by eliminating the voxels of activity that were marginal to the main large initial cluster. By comparing the location of the center of mass from the patient group versus the control group we observed that the location of 3 clusters were common to both patients and controls. The common activation areas were: right insula, right medial frontal gyrus and right inferior parietal lobule. A large cluster involving the 43 cingulate gyrus/BA32 was found exclusively in the patient group. Clusters located at the right cerebellum, right anterior cingulate gyrus/BA 10, left cerebellar tonsil, right and left thalamus, right inferior frontal gyrus and right middle frontal gyrus were unique to the control group. Table 5. Areas of differential activation between BMD patients (n=8) and pain-free volunteers (n=8). Mean Fractional Talairach Coordinate Signal Change Anatomical Location z-score (mm) (%) x y z BMD Control R ACC BA32/24 2.5 23.5 31.5 .23† .04 -3.029 L Thalamic Medial Dorsal -13.5 -20.5 11.5 .10 .31† 3.024 Nucleus R Thalamic Medial Dorsal 8.5 -17.5 11.5 .18 .33* 2.044 Nucleus R Middle Frontal Gyrus 37.5 23.5 31.5 -.02 .17* 2.527 R Pre-central Gyrus 36.5 3.5 36.5 .02 .16 * 2.143 L Lingual Gyrus -18.5 -64.5 0.5 -.05 .32* 2.267 L Precuneus -20.5 -65.5 19.5 .37* .02 -2.022 R Precuneus 9.5 -68.5 19.5 .15‡ -.26 -4.479 R Cerebellar Inferior 5.5 -67.5 -34.5 -.06 .44† 3.283 Semilunar Lobule BMD = burning mouth disorder; R = right side ; L = left side ; BA = Brodmann area ; * p<0.05 ; † p<0.005; ‡ p<0.001 Table 6. Location and size of the detected clusters of activity in the patient group Cluster Talairach Cluster # Anatomical Location volume coordinates (µl) x y z 1 4.1 24.3 30.7 R Cingulate Gyrus / BA 32 2344 2 43.2 8.2 4.6 R Insula* 2232 3 1.2 -3.9 53.2 R Medial Frontal Gyrus* 1744 4 37.4 -39.6 44.9 R Inferior Parietal Lobule* 1264 R = right side; L = left side; BA = Brodmann area; * = areas activated in both patients and controls 44 Table 7. Location and size of the detected clusters of activity in the control group Talairach Cluster coordinates Cluster # Anatomical Location volume (µl) x y z 1 14.4 -58.1 -26.8 R Cerebellum 10344 R Anterior Cingulate Gyrus / 2 4.8 53.1 -0.4 5024 BA 10 3 -26.2 -50.1 -32.1 L Cerebellar Tonsil 3512 4 -12.9 -17.5 13.6 L Thalamus 2344 5 28.3 3.4 12.4 R Insula * 2080 6 0.2 37.7 30.2 R Medial Frontal Gyrus* 1928 7 9.7 -13.5 12.4 R Thalamus 1912 8 40 3.1 32 R Inferior Frontal Gyrus 1800 9 33.1 30.7 29.8 R Middle Frontal Gyrus 1096 10 50.2 -41.9 31.5 R Inferior Parietal Lobule* 1000 R = right side; L = left side; BA = Brodmann area; * = areas activated in both patients and controls Copyright © 2004, Romulo J.C. Albuquerque 45 6. Discussion To the best of our knowledge, the present report is the only fMRI study with BMD patients. This study demonstrated significant brain activation (p<0.005) in both BMD patients and normal controls in pain related areas following thermal noxious stimulation. The activation pattern was similar to that found in earlier fMRI studies involving painful thermal stimulation of non-trigeminal [37, 39, 48, 63] and trigeminal sites [73]. The same activation pattern has also been observed with painful heat stimulation of the nondominant arm in PET studies [52, 128]. The activated brain regions have been implicated in the processing of different dimensions of the pain experience. Both groups displayed significant changes in BOLD signal (p<0.005) at the SI and thalamus. These two structures are likely related to the sensory-discriminative aspect of the pain experience. We also observed significant (p<0.005) activation in the cingulate gyrus. This structure is thought to be mediating the affective-motivational portion of pain. Activation was further observed in the cerebellum, inferior parietal lobule, frontal gyrus and pre-central gyrus. These regions are associated with the motor response to painful stimulation. Finally, there was activation in the insula and frontal gyrus, both of which are implicated in the processing of pain related memories.[28, 48, 129] The activation of these brain regions in our study population indicates that our thermal stimulus protocol is a reliable technique of thermal stimulation for the trigeminal nerve during fMRI acquisition as demonstrated by de Leeuw (2001).[73] In both groups the activation of the post-central gyrus (SI) occurred in the vicinity of the area that represents the face.[74] 46 The primary objective of this study was to demonstrate differences in the location and extension of activation between BMD patients and normal volunteers. We demonstrated that BMD patients process thermal painful stimulation quantitatively and qualitatively different than normal pain-free age and gender matched control subjects. It is worth mentioning that there were no differences in the subjective experience of pain, or in the temperatures used to create such experience. For this reason, brain activation discrepancies found in this study cannot be explained in terms of the subjective experience of pain but may reflect true functional disparities between the two groups. On the other hand, our small group size may have precluded us to find true differences with regard to these variables. In order to characterize these differences, we chose to analyze the data in terms of the magnitude of fractional BOLD signal change on a voxelto-voxel basis, as well as in terms of the total volume of brain activation at a threshold of 1000µl. 6.1. Qualitative Differences in Brain Activation Between Patient and Controls In terms of the locations of significant brain activation, we were able to show that the BMD patients had greater BOLD signal change in the right ACC (BA24/32) and bilateral precuneus than did normal controls. ACC hyperactivity has been demonstrated in other neuroimaging studies involving chronic neuropathic pain conditions [16, 19, 21, 22, 69]. It is important to note that there are fundamental differences between this and the above mentioned studies. Firstly, most of these previous studies used PET as their imaging technique. Secondly, the findings of such studies reflect changes in activation from a painful status to a pain-free state in the same group of patients. Our study 47 involves two distinct groups of subjects and explores differences in the processing of transient painful stimuli delivered to the division of the trigeminal nerve that is supposedly mediating the chronic pain condition. Therefore, our data merely suggest that BMD patients have a dysfunctional ACC (BA32/24) while the other studies, in light of their methods, more directly imply that the ACC (BA32/24) plays a role in the pathophysiology of the chronic pain condition. Since the ACC has also been implicated in the processing of anxiety, [34] it may be argued that the difference of activation at the ACC reflects greater anxiety levels in the patient group as shown by the differences on the SCL-90 anxiety subscale between the BMD and normal controls. The effects of psychological variables such as anxiety, somatization and interpersonal sensitivity, which have been shown to be elevated in our patient population, must always be taken into account in brain imaging studies. The precuneus was another area where patients displayed a greater magnitude of activation when compared to the control subjects. Precuneus activation has been linked to a variety of CNS processes. It appears that this region of the brain is a multimodal association area [130] and possesses motor and sensory functions. For example, precuneus activation has been shown during volitional swallowing [131, 132], locomotor-related imagery [133] and painful somatosensory hallucinations. [134] Most importantly, precuneus has been activated during mechanical muscle hyperesthesia in the orofacial region [71]. It is possible that precuneus hyperexcitability is implicated in the pathophysiology of BMD, however due to its dynamic functional characteristics it is very difficult to determine its exact role with the presently available data. 48 The thalamus was found to be differently activated in patients as compared to controls. Generally, thalamic responses to painful stimuli reflect discriminative and attentional networks of pain processing mechanisms.[28] This study revealed that control subjects had significantly greater bilateral BOLD signal changes in the thalamus than BMD patients This implies that the thalamus in BMD patients may be hypoactive. The area of activity within the thalamus appeared to involve the dorsal medial nucleus as well as the ventral lateral nucleus of the thalamus. However spatial smoothing of fMRI data makes it extremely difficult to draw accurate conclusions about the activation of such small regions of the brain. The finding of thalamic hypoactivity is in agreement with other neuroimaging studies that demonstrated thalamic hypofunction in patients suffering from chronic pain conditions.[20-22, 64] Thalamic hypoactivity is unlikely related to acute pain states, because thalamic hyperactivity has been demonstrated during acute pain conditions such as angina pectoris [135], cluster headache[17] and dental pain.[115]. Neuroimaging studies have shown significant increases in thalamic activity following procedures that led to cessation of chronic pain. These procedures include cordotomy for cancer pain [58], anesthetic blocks [21] and motor cortex stimulation for neuropathic pain [136]. Therefore, in chronic pain conditions, it is hypothesized that thalamic hypofunction is very likely a result of persistent, spontaneous chronic pain input. The idea that a hypofunctional thalamus may be directly related to the pathophysiology of neuropathic pain is supported by studies in which thalamic stimulation provides pain relief [59, 60, 137]. Kupers et al. reported a case of a patient with chronic orofacial neuropathic pain that was successfully treated by thalamic stimulation. They showed with PET that following thalamic stimulation and 49 subsequent pain relief, there was an increase in rCBF in areas of the brainstem that are often linked with descending inhibition of pain, such as the periaqueductal gray matter. Consequently, it is thought that the hypofunctional thalamus does not allow for adequate descending inhibition during chronic pain states. The present findings indicate this may be the case for BMD as well. This research showed that the control group also had significantly greater BOLD signal increases in the right middle frontal gyrus, right pre-central gyrus, right cerebellar inferior semilunar lobule and left lingual gyrus as compared to the BMD group. The right middle frontal gyrus is the supplementary motor area (SMA) and it has shown to be activated in other functional neuroimaging studies of pain [49, 138, 139]. Presumably, the SMA is involved in the planning and readiness for a withdrawal response secondary to pain.[128] The pre-central gyrus is the primary motor cortex and it has also displayed rCBF changes during painful stimulation. The activation of this area is primarily related to volunteer motor activities; however, in neuroimaging pain studies it is postulated that its activation may also reflects withdrawal reaction or movement refrain [28]. Activation of the cerebellum has been described in neurofunctional studies of pain.[17, 37, 43, 65, 71, 72, 138, 140] It is hypothesized that the cerebellum is involved in motor planning, as well as in the cognitive, affective and nociceptive processing of pain. Recent evidence reinforces the premise that the cerebellum is in fact involved in pain intensity encoding. [141] Despite the similar subjective experience between the two groups the control group displayed greater activation in areas responsible for the processing of motor response, for instance cerebellum, SMA and pre-central gyrus. Interestingly, stimulation of motor cortex has been shown to relieve neuropathic pain.[136] Given the diminished 50 response in BMD patients compared to controls, it could be postulated that these cortical areas, primarily involved in motor function, also play a significant role in descending inhibitory processes. The lingual gyrus is part of the visual cortex; it is located within the occipital lobe. Its function has been linked to the visual perception of motion [142, 143]; it has been implicated in semantic language processing [144] and it has also been reported as a site of processing aversive visual stimuli [145, 146]. In the present study, activation of the lingual gyrus in the absence of a specific visual task is interesting. The relationship between the lingual gyrus and pain processing is not understood. In summary, this study showed significant qualitative differences in brain activation patterns between BMD and normal controls. These differences are likely related to a dysfunctional brain network present in BMD patients. These findings will be the foundation for the development of a working hypothesis regarding BMD pathophysiology. 6.2. Quantitative Differences in Brain Activation Between Patient and Controls In terms of extent of brain activation, the present study showed that normal volunteers had greater total volume of brain activation in response to the painful stimulation than BMD patients. Additionally, our cluster analysis (size threshold of 1000µl) revealed that volunteers were able to activate more brain regions than did BMD patients. Whereas only four clusters of activation were detected in patients, 10 were detected in the normal volunteers. While a similar analysis methodology was used in a 51 neuroimaging study with fibromyalgia patients, contrasting results were found. [64] The study reported that fibromyalgia patients showed a greater number of activated brain areas than controls. The authors discussed their data in terms of cortical and subcortical augmentation of pain processing in fibromyalgia patients. The increased number of activated brain regions found by Gracely et al. may be related to several factors. Firstly, they used the same stimulus intensity for all participants. Since fibromyalgia patients have lower pressure pain threshold they produced different subjective pain ratings between patients and volunteers. In our study we were able to create the same subjective pain experience with equal stimulus intensities. Secondly, our study used thermal stimulation of the trigeminal nerve, while they used mechanical stimulation (pressure) to the left thumb nail. Thirdly, the difference between our study and Gracely et al.’s may be secondary to the fact that fibromyalgia is a widespread pain and not a focal and localized condition such as BMD. Our findings of diminished number of clusters and total volumetric activity coupled with the previously mentioned qualitative discrepancies in BMD patients as compared to normal controls may be interpreted as representing impaired brain network connectivity dynamics essential for inhibitory control. Thayer and Friedmann (2002) [70] reported that the behavior of living systems may be defined as a self-organizing dynamic system. Moreover, they suggested that inhibitory processes allow these systems to efficiently function in the face of changing environmental demands. They also mention that the process of sensitization does not always imply overall hyperactivity but it may be defined as a loss of inhibitory neural processes leading to maladaptive activation of fewer brain pathways. Our findings imply that BMD patients process acute thermal stimulation less dynamically than do normals. 52 Our theory is that patients with BMD have a diminished inhibitory control of sensory experiences and as a consequence of such they may be more likely to experience intraoral proprioceptive information as burning pain. This theory of overall brain hypofunction in BMD is supported by other studies where hypoactivity of the nigrostriatal dopaminergic system was documented in BMD patients.[109, 111] It is possible that, because of the multiple connections that exist between thalamus and the basal ganglia, the thalamic hypofunction shown in BMD patients is primarily responsible for the hypoactivity of the nigrostriatal dopaminergic system. It is also possible that the hypofunctional thalamus is playing a crucial role in diminishing brain connectivity dynamics. Hypofunction of the thalamus has been described in other chronic neuropathic pain conditions and it may not be an exclusive feature of BMD.[21, 58] In summary, these findings suggest quantitative differences in brain function between patients with BMD and normal volunteers. These results support the development of a working hypothesis that BMD may be a consequence of diminished brain dynamics that lead to the perception of burning in the intra-oral tissues. In fact, the hypothesis of overall brain hypofunction is an alternative explanation for why systematic literature reviews describe cognitive behavioral therapy among the most efficacious treatment modalities for BMD.[147, 148] Based on our findings, we might postulate that cognitive behavioral therapy promotes brain dynamics leading to relief of the burning sensation. It has been shown with PET and fMRI that cognitive behavioral therapy and relaxation techniques are capable of changing brain activation patterns as well as sympathetic activity [149, 150] The cognitive engagement that comes as a consequence of cognitive behavioral therapy and relaxation may stimulate critical regions of the brain, such as the 53 cerebellum [150] just enough to re-establish inhibitory processes that have not been functioning adequately. It is very difficult to draw conclusions regarding differences in specific areas of the brain and how they may relate to the pathophysiology of BMD. Despite the fact that we found areas that were differentially activated, trying to assign a specific function to a defined area of the human brain is very difficult as the brain involves multiple interacting structures. The processing of sensory information by the CNS is very dynamic; and it is possibly very different from individual to individual. It is important to note that our data support our hypothesis that BMD patients would display brain activation patterns that are similar to those reported in patients with chronic neuropathic pain (hypofunctional thalamus, hyperfunctional ACC (BA24/32)). We also postulate that brain areas primarily involved in motor tasks may be important for the descending inhibitory system and may be playing a key role in the pathophysiology of BMD. So, the question becomes how can one behaviorally “activate” the thalamus and other CNS sites so it can do their behavioral inhibitory work? This should be the focus of future investigations in this newly emerging field. 6.3 Future Research Directions Future studies should investigate if the same fMRI paradigm reveals similar patterns of brain activation in other focal chronic neuropathic pain conditions in the orofacial region, for example, continuous neuropathic pain. Similar studies with musculo-skeletal chronic pain conditions, for instance masticatory muscle pain disorders, would also be warranted. These studies may help determine if the activation 54 patterns described above are unique features of BMD, other focal neuropathic pain conditions, or just any chronic orofacial pain state. Future studies should also investigate the effects that cognitive behavioral therapy, diaphragmatic breathing and other behavioral strategies have in brain activation patterns. Special attention should be given to how these behavioral techniques modulate thalamic activity. Our working hypothesis of a hypofunctional brain in BMD patients and the current evidence that cognitive behavioral therapy is an effective treatment for this condition[147, 148] lead us to believe that these behavioral approaches could potentially correct the maladaptive changes in brain function. In light of its invasiveness, thalamic and other CNS stimulators may not be the primary focus of investigation for BMD. However, studies involving such devices would certainly help clarifying the implications of brain hypofunction in BMD. Thalamic stimulators have been used in the treatment of neuropathic pain conditions [59, 151] Stimulation of thalamus and other CNS sites (motor cortex, spinal cord) [14, 136, 152] increased activity in the different brain regions and significantly decreased persistent neuropathic pain conditions. Finally, studies on the role of primarily motor function related brain areas in the descending inhibition processes are also warranted. 6.4. Study Limitations The small sample size and consequent diminished statistical power put in question the reliability of our psychophysical data (potential for type II error). In terms of fMRI statistical analysis our sample size appears to be adequate. It would have been better if we had recruited a larger number of patients with BMD from which 55 psychophysical data could be collected. After collection of psychophysical data, a smaller sample of these patients could be randomly assigned to undergo fMRI scanning. This alternative design would provide us more power regarding our psychophysical conclusions. It is important mentioning that our psychophysical data analysis was in agreement with other larger studies with BMD patients.[101, 153] Another point that needs to be taken into account, as a limitation of this study, is that there was potential bias in the selection of patients. Patients who were taking medications that interfered with brain functioning, such as, antidepressants or benzodiazepines; and who were unable to discontinue such medication were excluded from this study. It is possible that only patients with milder cases of BMD were included in our patient sample. The large age range of our patient population and normal volunteer group could have serious implications in our fMRI data analysis. It is well known that the brain atrophies with age.[154] This could account for a large variability in brain anatomical features and may have influenced our data in a negative way during the normalization process and construction of three dimensional statistical maps. The tight matching criteria of our study should have made this issue less problematic. Copyright © 2004, Romulo J.C. Albuquerque 56 7. Summary To the best of our knowledge, the present study is the only fMRI study concerning BMD. This research’s results showed that BMD patients possess different patterns of brain activation compared to normal volunteers, as it relates to an acute thermal stimulation of the trigeminal nerve. These differences were qualitative and quantitative It was demonstrated that BMD patients have brain activation patterns similar to those reported in other neuropathic pain conditions.. When compared to volunteers, patients with BMD showed greater BOLD signal changes in the ACC BA32/24 and bilateral precuneus; and diminished BOLD signal changes in the bilateral thalamus, right middle frontal gyrus, right pre-central gyrus, left lingual gyrus and cerebellum. It was also demonstrated that patients with BMD displayed far less volumetric activation throughout the entire brain compared to the control group. This study’s findings strengthen the theory of a central neuropathic mechanism for BMD and have led to the development of a theory regarding the pathophysiology of BMD as it relates to an overall hypofunctional and less dynamic brain. Copyright © 2004, Romulo J.C. Albuquerque 57 References 1. Dong, W.K., et al., Nociceptive responses of trigeminal neurons in SII-7b cortex of awake monkeys. Brain Res, 1989. 484(1-2): p. 314-24. 2. Ossipov, M.H., et al., Mediation of spinal nerve injury induced tactile allodynia by descending facilitatory pathways in the dorsolateral funiculus in rats. Neurosci Lett, 2000. 290(2): p. 129-32. 3. Head, H. and G. Holmes, Sensory disturbances from cerebral lesions. Brain, 1911. 34: p. 102-254. 4. Lahuerta, J., et al., Percutaneous cervical cordotomy: a review of 181 operations on 146 patients with a study on the location of "pain fibers" in the C-2 spinal cord segment of 29 cases. J Neurosurg, 1994. 80: p. 975-985. 5. Pender, M.P., Neurology. 4: Multiple sclerosis. Med J Aust, 2000. 172(11): p. 556-62. 6. Treede, R.D., et al., Cortical representation of pain: functional characterization of nociceptive areas near the lateral sulcus. Pain, 2000. 87(2): p. 113-9. 7. Melzack, R., From the gate to the neuromatrix. Pain, 1999. Suppl 6: p. S121-6. 8. Belliveau, J.W., et al., Functional mapping of the human visual cortex by magnetic resonance imaging. Science, 1991. 254(5032): p. 716-9. 9. Porro, C.A., et al., Does anticipation of pain affect cortical nociceptive systems? J Neurosci, 2002. 22(8): p. 3206-14. 10. Bantick, S.J., et al., Imaging how attention modulates pain in humans using functional MRI. Brain, 2002. 125(Pt 2): p. 310-9. 11. Kim, K.H., et al., Distinct cortical areas associated with native and second languages. Nature, 1997. 388(6638): p. 171-4. 12. Binder, J.R., et al., Functional magnetic resonance imaging of human auditory cortex. Ann Neurol, 1994. 35(6): p. 662-72. 58 13. Desmond, J.E., et al., Lobular patterns of cerebellar activation in verbal workingmemory and finger-tapping tasks as revealed by functional MRI. J Neurosci, 1997. 17(24): p. 9675-85. 14. Roux, F.E., et al., Chronic motor cortex stimulation for phantom limb pain: a functional magnetic resonance imaging study: technical case report. Neurosurgery, 2001. 48(3): p. 681-7. 15. Cao, Y., et al., Functional MRI-BOLD of visually triggered headache in patients with migraine. Arch Neurol, 1999. 56(5): p. 548-54. 16. May, A. and P.J. Goadsby, Cluster headache: imaging and other developments. Curr Opin Neurol, 1998. 11(3): p. 199-203. 17. May, A., et al., Experimental cranial pain elicited by capsaicin: a PET study. Pain, 1998. 74(1): p. 61-6. 18. Goadsby, P.J., A. Bahra, and A. May, Mechanisms of cluster headache. Cephalalgia, 1999. 19 Suppl 23: p. 19-21; discussion 21-3. 19. Hsieh, J.C., J. Hannerz, and M. Ingvar, Right-lateralised central processing for pain of nitroglycerin-induced cluster headache. Pain, 1996. 67(1): p. 59-68. 20. Iadarola, M.J., et al., Unilateral decrease in thalamic activity observed with positron emission tomography in patients with chronic neuropathic pain. Pain, 1995. 63(1): p. 55-64. 21. Hsieh, J.C., et al., Central representation of chronic ongoing neuropathic pain studied by positron emission tomography. Pain, 1995. 63(2): p. 225-36. 22. Apkarian, A.V., et al., Prefrontal cortical hyperactivity in patients with sympathetically mediated chronic pain. Neurosci Lett, 2001. 311(3): p. 193-7. 23. Lotze, M., et al., Phantom movements and pain. An fMRI study in upper limb amputees. Brain, 2001. 124(Pt 11): p. 2268-77. 24. Coderre, T.J., et al., Contribution of central neuroplasticity to pathological pain: review of clinical and experimental evidence. Pain, 1993. 52(3): p. 259-85. 25. Kwong, K.K., et al., Dynamic magnetic resonance imaging of human brain activity during primary sensory stimulation. Proc Natl Acad Sci U S A, 1992. 89(12): p. 5675-9. 59 26. Pike, G.B. and R. Hoge, D., Functional Magnetic Resonance Imaging: Technical Aspects, in Pain Imaging. Progress in pain research and management., K.L. Casey and M.C. Bushnell, Editors. 2000, IASP Press: Seattle. p. 157-194. 27. Ogawa, S., et al., Brain magnetic resonance imaging with contrast dependent on blood oxygenation. Proc Natl Acad Sci U S A, 1990. 87(24): p. 9868-72. 28. Peyron, R., B. Laurent, and L. Garcia Larrea, Functional imaging of brain responses to pain. A review and meta-analysis (2000). Neurophysiol Clin, 2000. 30(5): p. 263-88. 29. Coull, J.T. and A.C. Nobre, Where and when to pay attention: the neural systems for directing attention to spatial locations and to time intervals as revealed by both PET and fMRI. J Neurosci, 1998. 18(18): p. 7426-35. 30. Sessle, B.J., Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive transmission and neuroplasticity, and their clinical correlates. Crit Rev Oral Biol Med, 2000. 11(1): p. 57-91. 31. Treede, R.D., et al., The cortical representation of pain. Pain, 1999. 79(2-3): p. 105-11. 32. Rome, H.P. and J.D. Rome, Limbically Augmented Pain Syndrome (LAPS): Kindling, Corticolimbic Sensitization, and the Convergence of Affective and Sensory Symptoms in Chronic Pain Disorders ; Pain Medicine, Mar2000, Vol. 1 Issue 1, p7, 17p. Pain Medicine, 2000. 1(1): p. 7-17. 33. Ingvar, M. and J.C. Hsieh, The image of pain, in Textbook of Pain, P.D. Wall and R. Melzack, Editors. 1999, Churchill Livingstone: London. p. 215-232. 34. Kwan, C.L., et al., An fMRI study of the anterior cingulate cortex and surrounding medial wall activations evoked by noxious cutaneous heat and cold stimuli. Pain, 2000. 85(3): p. 359-74. 35. Derbyshire, S.W., Exploring the pain "neuromatrix". Curr Rev Pain, 2000. 4(6): p. 467-77. 36. Ploghaus, A., et al., Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J Neurosci, 2001. 21(24): p. 9896-903. 37. Brooks, J.C., et al., fMRI of thermal pain: effects of stimulus laterality and attention. Neuroimage, 2002. 15(2): p. 293-301. 60 38. Craig, A.D., et al., Functional imaging of an illusion of pain. Nature, 1996. 384(6606): p. 258-60. 39. Gelnar, P.A., et al., A comparative fMRI study of cortical representations for thermal painful, vibrotactile, and motor performance tasks. Neuroimage, 1999. 10(4): p. 460-82. 40. Whalen, P.J., et al., The emotional counting Stroop paradigm: a functional magnetic resonance imaging probe of the anterior cingulate affective division. Biol Psychiatry, 1998. 44(12): p. 1219-28. 41. Bornhovd, K., et al., Painful stimuli evoked different stimulus-reponse functions in the amygdala, prefrontal, insula and somatosensory cortex: a single-trial fMRI study. Brain, 2002. 125: p. 1326-1336. 42. Buchel, C., et al., Dissociable neural responses related to pain intensity, stimulus intensity, and stimulus awareness within the anterior cingulate cortex: a parametric single-trial laser functional magnetic resonance imaging study. J Neurosci, 2002. 22(3): p. 970-6. 43. Iadarola, M.J., et al., Neural activation during acute capsaicin-evoked pain and allodynia assessed with PET. Brain, 1998. 121(Pt 5): p. 931-47. 44. Peyron, R., et al., Allodynia after lateral-medullary (Wallenberg) infarct. A Positron Emission Tomography (PET) study. Brain, 1998. 121: p. 345-56. 45. Price, D., Psychological and Neural Mechanisms of the Affective Dimension of Pain. Science, 2000. 288: p. 1769-1772. 46. Waxman, S.G., Cerebral Hemispheres / Telencephalon, in Correlative Neuroanatomy, S.G. Waxman, Editor. 2000, McGraw-Hill. p. 135-152. 47. Baron, R., et al., Brain processing of capsaicin-induced secondary hyperalgesia: a functional MRI study. Neurology, 1999. 53(3): p. 548-57. 48. Becerra, L.R., et al., Human brain activation under controlled thermal stimulation and habituation to noxious heat: an fMRI study. Magn Reson Med, 1999. 41(5): p. 1044-57. 49. Coghill, R.C., et al., Pain intensity processing within the human brain: a bilateral, distributed mechanism. J Neurophysiol, 1999. 82: p. 1934-1943. 61 50. Dong, W.K., et al., Somatosensory, multisensory, and task-related neurons in cortical area 7b (PF) of unanesthetized monkeys. J Neurophysiol, 1994. 72(2): p. 542-64. 51. Chen, J.-I., et al., Differentiating Noxious- and Innocuous-Related Activation of Human Somatosensory Cortices Using Temporal Analysis of fMRI. J Neurophysiol, 2002. 88: p. 464-74. 52. Casey, K.L., et al., Comparison of human cerebral activation patterns during cutaneous warmth, heat pain and deep cold pain. J Neurophysiol, 1996. 76: p. 571-81. 53. Craig, A.D., et al., Thermosensory activation of insular cortex. Nature Neurosc., 2000. 3: p. 184-9. 54. Okeson, J.P., The neural anatomy of pain, in Bell's Orofacial Pains, J.P. Okeson, Editor. 1995, Quintessence: Carol Stream. p. 13-44. 55. Albe-Fessard, D., et al., Diencephalic mechanisms of pain sensation. Brain Res Rev, 1985. 9: p. 217-296. 56. Davis, K.D., et al., Functional MRI study of thalamic and cortical activations evoked by cutaneous heat, cold, and tactile stimuli. J Neurophysiol, 1998. 80(3): p. 1533-46. 57. Davis, K.D., et al., Event-related fMRI of pain: entering a new era in imaging pain. Neuroreport, 1998. 9(13): p. 3019-23. 58. DiPiero, V., et al., Chronic pain: a PET study of the central effects of percutaneous high cervical cordotomy. Pain, 1991. 46: p. 9-12. 59. Kupers, R.C., J.M. Gybels, and A. Gjedde, Positron emission tomography study of a chronic pain patient successfully treated with somatosensory thalamic stimulation. Pain, 2000. 87(3): p. 295-302. 60. Rezai, A.R., et al., Thalamic stimulation and functional magnetic resonance imaging: localization of cortical and subcortical activation with implanted electrodes. Technical note. J Neurosurg, 1999. 90(3): p. 583-90. 61. Talairach, J. and P. Tournoux, Co-planar stereotaxic atlas of the human brain. 1988, New York: Thieme. 62 62. Buckner, R.L., Frontally mediated control processes contribute to source memory retrieval. Neuron, 2002. 35(5): p. 817-8. 63. Coghill, R.C., J.G. McHaffie, and Y.F. Yen, Neural correlates of interindividual differences in the subjective experience of pain. Proc Natl Acad Sci U S A, 2003. 100(14): p. 8538-42. 64. Gracely, R.H., et al., Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum, 2002. 46(5): p. 1333-43. 65. Giesecke, T., et al., Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum, 2004. 50(2): p. 613-23. 66. May, A., et al., Functional magnetic resonance imaging in spontaneous attacks of SUNCT: short-lasting neuralgiform headache with conjunctival injection and tearing. Ann Neurol, 1999. 46(5): p. 791-4. 67. Goadsby, P.J., Neuroimaging in headache. Microsc Res Tech, 2001. 53(3): p. 179-87. 68. Knight, Y.E. and P.J. Goadsby, The periaqueductal grey matter modulates trigeminovascular input: a role in migraine? Neuroscience, 2001. 106(4): p. 793800. 69. Derbyshire, S.W., et al., Cerebral responses to pain in patients with atypical facial pain measured by positron emission tomography. J Neurol Neurosurg Psychiatry, 1994. 57(10): p. 1166-72. 70. Thayer, J.F. and B.H. Friedman, Stop that! Inhibition, sensitization, and their neurovisceral concomitants. Scand J Psychol, 2002. 43(2): p. 123-30. 71. Kupers, R.C., P. Svensson, and T.S. Jensen, Central representation of muscle pain and mechanical hyperesthesia in the orofacial region: a positron emission tomography study. Pain, 2004. 108(3): p. 284-93. 72. Strigo, I.A., et al., Differentiation of visceral and cutaneous pain in the human brain. J Neurophysiol, 2003. 89(6): p. 3294-303. 73. de Leeuw, R., et al., Cerebral activation during thermal and emotional challenges: an fMRI study. Pain, 2001. 2:S1: p. 34. 63 74. DaSilva, A.F., et al., Somatotopic activation in the human trigeminal pain pathway. J Neurosci, 2002. 22(18): p. 8183-92. 75. Iannetti, G.D., et al., Representation of different trigeminal divisions within the primary and secondary human somatosensory cortex. Neuroimage, 2003. 19(3): p. 906-12. 76. Komisaruk, B.R., et al., Functional localization of brainstem and cervical spinal cord nuclei in humans with fMRI. AJNR Am J Neuroradiol, 2002. 23(4): p. 60917. 77. Rhodus, N.L., C.R. Carlson, and C.S. Miller, Burning mouth (syndrome) disorder. Quintessence Int, 2003. 34(8): p. 587-93. 78. Grushka, M., J.B. Epstein, and M. Gorsky, Burning mouth syndrome. Am Fam Physician, 2002. 65(4): p. 615-20. 79. Bergdahl, M. and J. Bergdahl, Burning mouth syndrome: prevalence and associated factors. J Oral Pathol Med, 1999. 28(8): p. 350-4. 80. Ship, J.A., et al., Burning mouth syndrome: an update. J Am Dent Assoc, 1995. 126(7): p. 842-53. 81. Lipton, J.A., J.A. Ship, and D. Larach-Robinson, Estimated prevalence and distribution of reported orofacial pain in the United States. J Am Dent Assoc, 1993. 124(10): p. 115-21. 82. Grushka, M., Clinical features of burning mouth syndrome. Oral Surg Oral Med Oral Pathol, 1987. 63(1): p. 30-6. 83. Fraikin, N., et al., [Burning mouth syndrome]. Rev Med Liege, 1999. 54(6): p. 548-52. 84. Scala, A., et al., Update on burning mouth syndrome: overview and patient management. Crit Rev Oral Biol Med, 2003. 14(4): p. 275-91. 85. Rhodus, N.L., C. Carlson, and C.S. Miller, Burning mouth (syndrome) disorder. Quintessence International, 2003. 34(8): p. 587-93. 86. Basker, R.M. and D.M. Main, The cause and management of burning mouth condition. Spec Care Dentist, 1991. 11(3): p. 89-96. 64 87. Rhodus, N.L., et al., Burning mouth syndrome: diagnosis and treatment. Northwest Dent, 2000. 79(3): p. 21-8. 88. Grushka, M., J.B. Epstein, and M. Gorsky, Burning mouth syndrome and other oral sensory disorders: a unifying hypothesis. Pain Res Manag, 2003. 8(3): p. 133-5. 89. Nagler, R.M. and O. Hershkovich, Sialochemical and gustatory analysis in patients with oral sensory complaints. J Pain, 2004. 5(1): p. 56-63. 90. Pokupec-Gruden, J.S., A. Cekic-Arambasin, and V. Gruden, Psychogenic factors in the aetiology of stomatopyrosis. Coll Antropol, 2000. 24 Suppl 1: p. 119-26. 91. Nicholson, B. and S. Verma, Comorbidities in chronic neuropathic pain. Pain Med, 2004. 5 Suppl 1: p. S9-S27. 92. Grzesiak, R.C., Psychologic aspects of chronic orofacial pain, Part II: Patient characteristics. Compendium, 1988. 9(4): p. 282-3, 286-8, 290-1. 93. Eli, I., et al., Antecedents of burning mouth syndrome (glossodynia)--recent life events vs. psychopathologic aspects. J Dent Res, 1994. 73(2): p. 567-72. 94. Jerlang, B.B., Burning mouth syndrome (BMS) and the concept of alexithymia--a preliminary study. J Oral Pathol Med, 1997. 26(6): p. 249-53. 95. Grushka, M., B.J. Sessle, and R. Miller, Pain and personality profiles in burning mouth syndrome. Pain, 1987. 28(2): p. 155-67. 96. Woda, A., et al., A possible therapeutic solution for stomatodynia (burning mouth syndrome). J Orofac Pain, 1998. 12(4): p. 272-8. 97. Gremeau, C., et al., Topical clonazepam in stomatodynia: a randomised placebocontrolled study. Pain, 2004. 108: p. 51-57. 98. Grushka, M., J. Epstein, and A. Mott, An open-label, dose escalation pilot study of the effect of clonazepam in burning mouth syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1998. 86(5): p. 557-61. 99. Svensson, P., et al., Sensory and pain thresholds to orofacial argon laser stimulation in patients with chronic burning mouth syndrome. Clin J Pain, 1993. 9(3): p. 207-15. 65 100. Ito, M., et al., Pain threshold and pain recovery after experimental stimulation in patients with burning mouth syndrome. Psychiatry Clin Neurosci, 2002. 56(2): p. 161-8. 101. Grushka, M., B.J. Sessle, and T.P. Howley, Psychophysical assessment of tactile, pain and thermal sensory functions in burning mouth syndrome. Pain, 1987. 28(2): p. 169-84. 102. Gao, S., Y. Wang, and Z. Wang, Assessment of trigeminal somatosensory evoked potentials in burning mouth syndrome. Chin J Dent Res, 2000. 3(1): p. 40-6. 103. Lauritano, D., et al., [Etiopathogenic, clinical-diagnostic and therapeutic aspects of the burning mouth syndrome. Research and treatment protocols in a patient group]. Minerva Stomatol, 1998. 47(6): p. 239-51. 104. Heckmann, S.M., et al., Oral mucosal blood flow in patients with burning mouth syndrome. Pain, 2001. 90(3): p. 281-6. 105. Femiano, F., et al., Burning mouth syndrome (BMS): controlled open trial of the efficacy of alpha-lipoic acid (thioctic acid) on symptomatology. Oral Dis, 2000. 6(5): p. 274-277. 106. Femiano, F. and C. Scully, Burning mouth syndrome (BMS): double blind controlled study of alpha-lipoic acid (thioctic acid) therapy. J Oral Pathol Med, 2002. 31(5): p. 267-9. 107. Femiano, F., C. Scully, and F. Gombos, Idiopathic dysgeusia; an open trial of alpha lipoic acid (ALA) therapy. Int J Oral Maxillofac Surg, 2002. 31(6): p. 625-8. 108. Jaaskelainen, S.K., H. Forssell, and O. Tenovuo, Abnormalities of the blink reflex in burning mouth syndrome. Pain, 1997. 73(3): p. 455-60. 109. Jaaskelainen, S.K., et al., Role of the dopaminergic system in chronic pain -- a fluorodopa-PET study. Pain, 2001. 90(3): p. 257-60. 110. Hagelberg, N., et al., Altered dopamine D2 receptor binding in atypical facial pain. Pain, 2003. 106(1-2): p. 43-8. 111. Hagelberg, N., et al., Striatal dopamine D1 and D2 receptors in burning mouth syndrome. Pain, 2003. 101(1-2): p. 149-54. 66 112. Forssell, H., et al., Sensory dysfunction in burning mouth syndrome. Pain, 2002. 99(1-2): p. 41-7. 113. Femiano, F., Burning mouth syndrome (BMS): an open trial of comparative efficacy of alpha-lipoic acid (thioctic acid) with other therapies. Minerva Stomatol, 2002. 51(9): p. 405-9. 114. Chudler, E.H. and W.K. Dong, The role of the basal ganglia in nociception and pain. Pain, 1995. 60(1): p. 3-38. 115. Derbyshire, S.W., et al., Cerebral responses to pain in patients suffering acute post-dental extraction pain measured by positron emission tomography (PET). Eur J Pain, 1999. 3(2): p. 103-113. 116. Apkarian, A.V., et al., Cortical responses to thermal pain depend on stimulus size: a functional MRI study. J Neurophysiol, 2000. 83(5): p. 3113-22. 117. Szaflarski, J.P., et al., Language lateralization in left-handed and ambidextrous people: fMRI data. Neurology, 2002. 59(2): p. 238-44. 118. Siebner, H.R., et al., Long-term consequences of switching handedness: a positron emission tomography study on handwriting in "converted" left-handers. J Neurosci, 2002. 22(7): p. 2816-25. 119. Soros, P., et al., Cortical asymmetries of the human somatosensory hand representation in right- and left-handers. Neurosci Lett, 1999. 271(2): p. 89-92. 120. Derogatis, L.R., SCL-90R Manual: Administration, Scoring, & Procedures. 1992, Towson, MD: Clinical Psychometry Research. 121. Beck, A.T. and R. Steer, Beck Depression Inventory Scoring Manual. 1987, New York: The Psychological Corporation. Harcourt Brace Janovich. 122. Beck, A.T., R. Steer, and M.G. Garbin, Pschometric Properties of the Beck Depression Inventory: Twenty-five years later. Clin Psychol Rev, 1988. 9: p. 77100. 123. Kendall, P.C., et al., Issues and recommendations regarding the use of the BDI. Cognitive therapy & Research, 1987. 11: p. 289-299. 124. Spielberger, C.D., et al., Manual for the State-Trait Anxiety Inventory (Form Y). 1983, Palo Alto, CA: Consulting Psychologists Press. 67 125. Yarnitsky, D. and J.L. Ochoa, Studies of heat pain sensation in man: perception thresholds, rate of stimulus rise and reaction time. Pain, 1990. 40(1): p. 85-91. 126. Friston, K.J., et al., Spatial registration and normalization of images. Hum Brain Mapp, 1995. 2: p. 165-189. 127. Cox, R.W., AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Computers and Biomedical Research, 1996. 29: p. 162173. 128. Coghill, R.C., et al., Distributed processing of pain and vibration by the human brain. J Neurosci, 1994. 14(7): p. 4095-108. 129. Talbot, J.D., et al., Multiple representations of pain in human cerebral cortex. Science, 1991. 251(4999): p. 1355-8. 130. Krause, B.J., et al., Episodic retrieval activates the precuneus irrespective of the imagery content of word pair associates. A PET study. Brain, 1999. 122 ( Pt 2): p. 255-63. 131. Kern, M.K., et al., Cerebral cortical representation of reflexive and volitional swallowing in humans. Am J Physiol Gastrointest Liver Physiol, 2001. 280(3): p. G354-60. 132. Kern, M., et al., Swallow-related cerebral cortical activity maps are not specific to deglutition. Am J Physiol Gastrointest Liver Physiol, 2001. 280(4): p. G531-8. 133. Malouin, F., et al., Brain activations during motor imagery of locomotor-related tasks: a PET study. Hum Brain Mapp, 2003. 19(1): p. 47-62. 134. Bar, K.J., et al., Transient activation of a somatosensory area in painful hallucinations shown by fMRI. Neuroreport, 2002. 13(6): p. 805-8. 135. Rosen, S.D., et al., Central nervous pathways mediating angina pectoris. Lancet, 1994. 344(8916): p. 147-50. 136. Garcia-Larrea, L., et al., Positron emission tomography during motor cortex stimulation for pain control. Stereotact Funct Neurosurg, 1997. 68(1-4 Pt 1): p. 141-8. 137. Duncan, G.H., et al., Stimulation of human thalamus for pain relief: possible modulatory circuits revealed by positron emission tomography. J Neurophysiol, 1998. 80(6): p. 3326-30. 68 138. Svensson, P., et al., Cerebral processing of acute skin and muscle pain in humans. J Neurophysiol, 1997. 78(1): p. 450-60. 139. Adler, L.J., et al., Regional brain activity changes associated with fentanyl analgesia elucidated by positron emission tomography. Anesth Analg, 1997. 84(1): p. 120-6. 140. Casey, K.L., et al., Temporal and spatial dynamics of human forebrain activity during heat pain: analysis by positron emission tomography. J Neurophysiol, 2001. 85(2): p. 951-9. 141. Helmchen, C., et al., Differential cerebellar activation related to perceived pain intensity during noxious thermal stimulation in humans: a functional magnetic resonance imaging study. Neurosci Lett, 2003. 335(3): p. 202-6. 142. Astafiev, S.V., et al., Extrastriate body area in human occipital cortex responds to the performance of motor actions. Nat Neurosci, 2004. 7(5): p. 542-8. 143. Santi, A., et al., Perceiving biological motion: dissociating visible speech from walking. J Cogn Neurosci, 2003. 15(6): p. 800-9. 144. Bartha, L., et al., Medial temporal lobe activation during semantic language processing: fMRI findings in healthy left- and right-handers. Brain Res Cogn Brain Res, 2003. 17(2): p. 339-46. 145. Taylor, S.F., et al., The effect of emotional content on visual recognition memory: a PET activation study. Neuroimage, 1998. 8(2): p. 188-97. 146. Knight, D.C., et al., Functional MRI of human Pavlovian fear conditioning: patterns of activation as a function of learning. Neuroreport, 1999. 10(17): p. 3665-70. 147. Zakrzewska, J.M., H. Forssell, and A.M. Glenny, Interventions for the treatment of burning mouth syndrome: a systematic review. J Orofac Pain, 2003. 17(4): p. 293-300. 148. Zakrzewska, J.M., A.M. Glenny, and H. Forssell, Interventions for the treatment of burning mouth syndrome. Cochrane Database Syst Rev, 2001(3): p. CD002779. 149. Paquette, V., et al., "Change the mind and you change the brain": effects of cognitive-behavioral therapy on the neural correlates of spider phobia. Neuroimage, 2003. 18(2): p. 401-9. 69 150. Critchley, H.D., et al., Brain activity during biofeedback relaxation: a functional neuroimaging investigation. Brain, 2001. 124(Pt 5): p. 1003-12. 151. Gybels, J.M. and R. Kupers, Operative neurosurgical techniques, in Management of persistent pain by brain stimulation, H. Schmidek and W.H. Sweet, Editors. 1995, Saunders: Philadelphia. p. 1389-1398. 152. Hautvast, R.W., et al., Spinal cord stimulation in chronic intractable angina pectoris: a randomized, controlled efficacy study. Am Heart J, 1998. 136(6): p. 1114-20. 153. Carlson, C.R., C.S. Miller, and K.I. Reid, Psychosocial profiles of patients with burning mouth syndrome. J Orofac Pain, 2000. 14(1): p. 59-64. 154. Fox, N.C. and J.M. Schott, Imaging cerebral atrophy: normal ageing to Alzheimer's disease. Lancet, 2004. 363(9406): p. 392-4. 70 Vita Bibliographical information Name: Romulo Jose Cunha Albuquerque Date of birth: February 08, 1976 Place of birth: Recife, PE, Brazil Education Fellowship in Orofacial Pain, from July 1, 2000 to June 30, 2001. University of Kentucky College of Dentistry, Lexington, KY, USA. DDS, from February 1996 to October 2000. University of Pernambuco College of Dentistry, Recife, PE,Brazil. Professional positions held Resident (Full-Time) at the Orofacial Pain Center, from July, 2001 to June, 2002. University of Kentucky College of Dentistry, Lexington, KY, USA. Private Practice, from October 2000 to at Recife, PE, Brazil. Fellow Dentist at the Orofacial Pain Center from the University of Pernambuco, from August 1998 to December 2000. College of Dentistry, Recife, PE, Brazil. Volunteer Dentist at the Pediatric Dentistry Department, from June 2000 to January 2001. Santo Amaro Dental Care Unit, Recife, PE, Brazil. Professional affiliations Member of the Kentucky Pain Society 71