Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Haemodynamic response wikipedia , lookup
Start School Later movement wikipedia , lookup
Neural oscillation wikipedia , lookup
Axon guidance wikipedia , lookup
Neuroanatomy wikipedia , lookup
Synaptogenesis wikipedia , lookup
Metastability in the brain wikipedia , lookup
Synaptic gating wikipedia , lookup
Neuroeconomics wikipedia , lookup
Activity-dependent plasticity wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Aging brain wikipedia , lookup
NMDA receptor wikipedia , lookup
Biology of depression wikipedia , lookup
Optogenetics wikipedia , lookup
Neurotransmitter wikipedia , lookup
Spike-and-wave wikipedia , lookup
Signal transduction wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Restless legs syndrome wikipedia , lookup
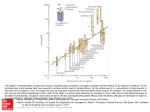
18 HISTAMINE AND RESTLESS LEGS SYNDROME (RLS) By Regina Patrick, RPSGT H istamine is a compound derived from the amino acid histidine and is found in virtually all body tissues. Excessive amounts of histamine in the respiratory tract, which occurs in some people during the hay fever/pollen season, can result in a runny or stuffy nose, wheezing and sneezing. Antihistamine drugs are used to relieve these symptoms. Some people with seasonal allergies who also have the sleep disorder restless legs syndrome note that antihistamines worsen their leg movements. Histamine may play a role in movement, which could explain the worsening of leg movements during sleep with antihistamine use in people with restless legs syndrome (RLS). HISTAMINE & HISTAMINE RECEPTORS In the brain, histamine acts as an excitatory neurotransmitter and plays a role in wakefulness and in the transition between sleep and wakefulness; in the stomach it stimulates gastric secretion; and in the lungs, it plays a role in airway constriction. These varied functions result from the activation of four types of histamine receptors (labeled H1, H2, H3 and H4). H1 receptors modulate neuronal firing in the brain. H2 receptors primarily play a role in stimulating gastric secretion. H3 receptors inhibit the release of histamine from histaminergic neurons and may modulate the release of other neurotransmitters in other types of neurons. H4 receptors were discovered in 2001;1 scientists have not fully determined their function. A high density of H3 receptors exists on the striatum of the brain. The striatum is a group of specialized cells located near the thalamus that is part of the basal ganglia (several groups of cells at the base of the brain). It plays a role in movement. The striatum contains neurons that are GABAergic (i.e., releasing the neuroinhibitor gamma-aminobutyric acid), dopaminergic (i.e., releasing the excitatory neurotransmitter dopamine), and glutamatergic (i.e., releasing the excitatory neurotransmitter glutamate). The striatal H3 receptors are found on the terminals of GABAergic, dopaminergic and glutamatergic neurons. The presence of H3 receptors on dopaminergic and glutamatergic neurons appears to play a role in inhibiting the release of dopamine and glutamate from their respective neurons. Two types of dopamine receptors – D1 and D2 – lie in close proximity to the histamine receptors in the striatum, which may allow for interactions between these receptors. Scientists are unsure if the interaction between histamine and dopamine receptors is antagonistic (i.e., blocking) or agonistic (i.e., activating). However, some research suggests that it may be antagonistic. Carla Ferrada and associates found that activation of the H3 receptors may modulate dopamine receptor activity.2 These researchers subcutaneously injected mice with reserpine (which depletes dopamine stores from a neuron) to block the activity of all striatal dopamine receptors. After treatment with reserpine, the researchers injected the mice with drugs that specifically blocked H3 receptor activity, D1 receptor activity, or D2 receptor activity; and with drugs that specifically activated these receptors. The researchers used the locomotor activity of the mice as a measure of dopaminergic activation. Increased locomotor activity indicated increased dopaminergic activation. Since the animals were previously treated with reserpine, locomotor activity from dopamine receptor activation was considered an exogenous effect of the drug rather than an endogenous effect. They found that when the H3 receptor activity was blocked and either the D1 or D2 receptors were activated, the locomotor activity of the mice increased from its baseline level. When the H3 receptor was activated and either the D1 or D2 receptor was activated, the locomotor activity of the mice decreased from its baseline level; however, the decrease was greater with activation of the D2 receptors. When they blocked H3 receptor activity but simultaneously activated the D1 and D2 receptors, the activity level of the mice increased to approximately twice that of when either dopamine receptor was activated alone. Since locomotor activity shows a greater increase with the absence of H3 input, Ferrada and colleagues concluded that histaminergic receptors may modulate the activity of dopaminergic receptors in the striatum. Changes in the striatum, such as a loss of neurons in the tissue, have been noted in other movement disorders such as Parkinson’s disease.3 Since RLS is a movement disorder, some scientists have suspected that the striatum also may be involved in this disorder. Studies are beginning to confirm this hypothesis.4,5 Animal studies reveal that histamine levels in the brain are higher during wake than during sleep. Regina Patrick, RPSGT Regina Patrick, RPSGT, has been in the sleep field for 22 years and works as a sleep technologist at St. Vincent Mercy Sleep Disorders Center in Toledo, Ohio. LINKING HISTAMINE TO RLS RLS involves creepy, crawly, uncomfortable leg sensations that usually manifest in the evening or at night, often when a person is sitting quietly or lying down in bed. The sensations are only momentarily relieved by massaging the legs, rubbing them against the bedsheets, stretching, walking or other activity. Often an RLS sufferer feels compelled to move the legs around, hence the name “restless legs syndrome.” These A2Zzz 18.2 | June 2009 19 uncomfortable sensations typically subside soon before the onset of sleep or with the onset of sleep. Reports of antihistamine-induced RLS began to appear in the medical literature in the late 1980s to early 1990s. For example in 1989, Korean researcher In-Ho Paik and colleagues reported the sudden development of RLS in three patients taking mianserin, a serotonin-antagonist antidepressant drug that also has antihistamine activity.6 The RLS symptoms ended once the patients stopped taking the drug. In 1993 O’Sullivan and Greenberg related the case of a female patient who developed RLS symptoms and oral dyskinesia (i.e., uncontrolled mouth movements) after taking the H2 antagonist drug cimetidine for 10 years to treat esophageal reflux.7 She described the leg sensations as feeling “like nerves being pulled apart.” Despite such reports, scientists remain unsure of the extent to which antihistamine drugs either may be inducing RLS or may be unmasking dysfunctional histaminergic activation in people with RLS. Recently, a team of Johns Hopkins researchers investigated the activation of histaminergic pathways in the brain of 12 individuals with RLS.8 The subjects were given either the antihistamine medication diphenhydramine, or as a control they were given a non-histamine sedative to induce drowsiness, which is a common effect of antihistamine use. They found that the RLS subjects who had taken the antihistamine drug had three to four times more leg activity than the subjects who had taken the sedative. In another aspect of their study, the researchers microscopically examined the autopsied brains of RLS sufferers. They found that in 83 percent of the subjects, the substantia nigra (i.e., a thin layer of pigmented cells in the brainstem that is thought to play a role in movement) had an increased amount of H3 receptors. They believe that the increased presence of H3 receptors in the substantia nigra may lead to increased stimulation of histaminergic pathways, resulting in increased leg movements in RLS sufferers. In the brain, the histaminergic neural pathway originates in the tuberomammillary nucleus of the hypothalamus. The tuberomammillary nucleus is a group of cells that play a role in locomotion and in the regulation of sleep and wakefulness. From the tuberomammillary nucleus, the neurons project to the thalamus, the suprachiasmatic nucleus, the basal ganglia, the hypothalamus and the brainstem. Animal studies reveal that histamine levels in the brain are higher during wake than during sleep. For example, German researchers Nora Sittig and Helga Davidowa found that tuberomammillary nucleus cells in rat subjects released histamine during the dark period (i.e., the animal’s wake phase) but decreased their production during the light period (i.e., the animal’s sleep phase).9 The tuberomammillary nucleus’ connections with the suprachiasmatic nucleus may play a role in the cells’ cyclical release of histamine on a circadian rhythm. CLINCAL RELEVANCE An estimated 12 million Americans are affected by RLS.10 Lifestyle changes such as avoiding the stimulant effects of caffeine, tobacco and alcohol before bedtime helps reduce symptoms in some people. Nutritional deficiencies in iron, folate or magnesium may play a factor in some cases of RLS. Supplementation of these nutrients helps to reduce the uncomfort- able nocturnal leg movements in some people with RLS. If these do not work, drug therapy may offer relief. Drug treatment for RLS currently involves the use of dopamine agonists (e.g., ropinirole, pramipexole), benzodiazepines (e.g., clonazepam), anticonvulsants (e.g., gabapentin) and opioids (e.g., hydrocodone). However, some patients report difficulties with side effects (e.g., nausea, dizziness, daytime sleepiness). Therefore, therapeutic modulation of histaminergic pathways may offer another option for treating this disorder. However, studies have yet to determine if altering H3 receptor activity modulates dopamine receptor activity and reduces nocturnal leg movements in RLS. For now, scientists are focusing on understanding the exact role of histamine in RLS. References 1. Nguyen T, Shapiro DA, George SR, et al. Discovery of a novel member of the histamine receptor family. Mol Pharmacol. 2001 Mar; 59(3):427–433. 2. Ferrada C, Ferre S, Casado V, et al. Interactions between histamine H3 and dopamine D2 receptors and the implications for striatal function. Neuropharmacology. 2008 Aug;55(2):190-7. Epub 2008 May 16. 3. Berg D, Godau J, Walter U. Transcranial sonography in movement disorders. Lancet Neurol. 2008 Nov;7(11):1044-55. 4. Thomas C. Wetter TC, Eisensehr I, Claudia Trenkwalder C. Functional neuroimaging studies in restless legs syndrome. Sleep Med. 2004 Jul;5(4):401-6. 5. Godau J, Wevers AK, Gaenslen A, et al. Sonographic abnormalities of brainstem structures in restless legs syndrome. Sleep Med. 2008 Oct;9(7):782-9. Epub 2007 Nov 19. 6. Paik IH, Lee C, Choi BM, et al. Mianserininduced restless legs syndrome. Br J Psychiatry. 1989 Sep;155:415-7. 7. O’Sullivan RL, Greenberg DB. H2 antagonists, restless leg syndrome, and movement disorders. Psychosomatics. 1993 Nov-Dec;34(6):530-2. 8. Johns Hopkins University. Press Release: Histaminergic clinical and autopsy abnormalities in restless legs syndrome. Washington, DC: Washington Convention Center; 2008 Nov 15-19; Program #143.13, Poster #U7. Available online at: http://www.hopkinsmedicine.org/ Press_releases/2008/11_14_08.html. Accessed March 30, 2009. 9. Sittig N, Davidowa H. Histamine reduces firing and bursting of anterior and intralaminar thalamic neurons and activates striatal cells in anesthetized rats. Behav Brain Res. 2001 Oct 15;124(2):137-43. 10. National Institutes of Health (NIH). National Institute of Neurological Disorders and Stroke (NINDS). Restless Legs Syndrome Fact Sheet. 2001 Apr. NIH Publication No. 01-4847. Available online at: http://www.ninds. nih.gov/disorders/restless_legs/detail_restless_legs.htm. Accessed March 30, 2009. A2Zzz 18.2 | June 2009