Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Brain Rules wikipedia , lookup
Brain morphometry wikipedia , lookup
Cognitive neuroscience wikipedia , lookup
Neuroplasticity wikipedia , lookup
Blood–brain barrier wikipedia , lookup
Neurophilosophy wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Subventricular zone wikipedia , lookup
Neurolinguistics wikipedia , lookup
Neuroesthetics wikipedia , lookup
Endocannabinoid system wikipedia , lookup
History of neuroimaging wikipedia , lookup
Neuropsychology wikipedia , lookup
Aging brain wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Metastability in the brain wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Neuroanatomy wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Haemodynamic response wikipedia , lookup
Signal transduction wikipedia , lookup
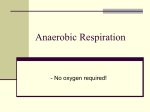
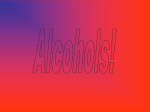
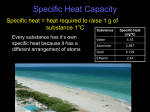
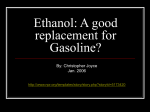
Inmunol3/2006 copia 13/12/06 16:38 Página 188 Revisión Inmunología Vol. 25 / Núm 3/ Julio-Septiembre 2006: 188-200 Alcohol and neuroinflammation: Involvement of astroglial cells and TLR4/IL-1RI receptors A.M. Blanco, C, Guerri Unidad de Patología Celular, Centro de Investigación Príncipe Felipe (CIPF), Valencia, Spain. ALCOHOL Y NEUROINFLAMACIÓN: PAPEL DE LAS CÉLULAS ASTROGLIALES Y DE LOS RECEPTORES TLR4/IL-1RI. Recibido: 200 Junio 2006 Aceptado: 26 Septiembre 2006 RESUMEN La expresión de mediadores inflamatorios y citocinas están implicadas en la patogénesis de diversas enfermedades neurodegenerativas. Una característica importante de la neuroinflamación es la activación de las células gliales, especialmente microglia y astroglia, que producen citocinas, compuestos pro-inflamatorios y tóxicos, desencadenando una respuesta inflamatoria y daño cerebral. Estudios recientes sugieren que los receptores TLRs (Toll-like), junto a las células gliales desempeñan un papel relevante en la respuesta inmune del sistema nervioso central (SNC), y una alteración en la regulación de dicha respuesta puede causar neurodegeneración. El abuso de alcohol y el alcoholismo inducen daño cerebral y, en algunos casos causan neurodegeneración. Los procesos neuropatológicos implicados en estos efectos no están totalmente esclarecidos. Evidencias recientes sugieren que el etanol es capaz de activar a las células gliales y de inducir procesos inflamatorios en el cerebro que pueden conducir a muerte neural. Estas evidencias demuestran que el etanol favorece la activación de vías de señalización intracelular (IKK, MAPKs) y factores de transcripción (NF-κB, AP-1) que conllevan a la producción de citocinas y de mediadores inflamatorios (iNOS, NO, COX-2) en cerebro y en células astrogliales. La respuesta inflamatoria inducida por el etanol parece estar mediada por una activación de los receptores TLR4/IL-1RI, ya que cuando se bloquea su función, se eliminan los efectos del etanol sobre la inducción de mediadores inflamatorios y muerte celular. Aunque los mecanismos que subyacen a la activación de estos receptores se desconoce, proponemos que el etanol a través de su interacción con los lípidos de membrana, podría facilitar el reclutamiento de los receptores TLR4 e IL-1RI en los microdominios de membrana (lipid rafts), conllevando a un aumento en su respuesta y señalización. En conclusión, aunque se requieren más trabajos para evaluar el mecanismo de la activación de los TLR4/IL-1RI por el etanol, en esta revisión se presentan estudios que apoyan la idea de que un aumento en la respuesta innata inmune a través de los receptores TLR4/IL-1RI, podría participar en el daño cerebral asociado al consumo de alcohol. PALABRAS CLAVE: Etanol / Daño cerebral / Inflamación / Células gliales / Receptor Toll-Like. 188 ABSTRACT Inflammatory mediators and cytokine expression are implicated in the pathogenesis of several neurodegenerative diseases. The hallmark of brain inflammation is the activation of glial cells, especially microglia and astroglia, which produce a variety of pro-inflammatory and toxic compounds that can induce brain damage. Recent developments in our understanding of neurodegeneration implicate glial cells and Toll-like receptors (TLRs) as vital players in the immune response within the central nervous system, and that deregulation of this response plays an important role in brain injury and neurodegeneration. Alcohol abuse and alcoholism induce brain damage, and in some cases, neurodegeneration. The neuropathologic processes underlying these effects remain poorly understood. Recent data demonstrate that ethanol promotes inflammatory processes in the brain and in glial cells by upregulating cytokines and inflammatory mediators (iNOS, NO, COX-2), and by activating signalling pathways (IKK, MAPKs) and transcriptional factors (NF-κB, AP-1) implicated in inflammatory injury. TLR4 and IL1RI are involved in the signalling of ethanol-induced inflammatory response, since blocking these receptors abolishes the production of ethanolinduced inflammatory mediators and cell death in astrocytes. Although the mechanisms involved in the ethanol-induced activation of TLR4/IL1RI receptors are unknown, we propose that ethanol can facilitate TLR4/IL1RI recruitment into lipid raft microdomains through its interaction with membrane lipids, leading to the activation and signalling of these receptors. In summary, although further work is needed to evaluate this hypothesis, this review presents evidences supporting the notion that the activation of innate immune system and TLR4/IL-1RI by ethanol triggers inflammatory mediators in the brain and causes brain damage. KEY WORDS: Ethanol / Brain injuries / Inflammation / Glial cells / TollLike Receptor. Inmunol3/2006 copia 13/12/06 16:38 Página 189 INMUNOLOGÍA ROLE OF INFLAMMATION IN BRAIN DAMAGE Inflammation is an important host defence response to injury, tissue ischemia, autoimmune responses or infections and it often elicits a generalized sequence of events known as the acute phase response, which can limit the proliferation of invading pathogens. However, while local and generalized inflammatory responses offer clear benefits in infectious states, sustained or inappropriate inflammation can cause numerous diseases including inflammatory bowel disease, rheumatoid arthritis and psoriasis. Inflammation is also an important component of the damage caused by autoimmune diseases, and fundamentally contributes to diseases such as cancer, diabetes and cardiovascular diseases(1, 2). The central nervous system (CNS) was considered as an immune privileged organ, which was not susceptible to inflammation or immune activation, and was thought to be largely unaffected by systematic inflammatory and immune responses. This point of view has changed drastically during the last decade. It is now accepted that the brain coordinates and regulates many aspects of the host defence response, which may explain the behavioural responses to diseases such as fatigue and depression, and how the psychological state influences susceptibility to disease and recovery(3). Furthermore, emerging evidence indicates that inflammation represents a potential pathogenic factor in many CNS diseases, including chronic neurodegenerative diseases, such as Parkinson´s disease(4), Alzheimer´s disease(5), Creutzfeldt-Jacob disease(6), and more recently in some psychiatric disorders such as depression, anxiety and schizophrenia(3). In these diseases, inflammation is atypical and occurs in the absence of leukocyte over infiltration(7). There is no doubt that the brain differs significantly from other tissues in its response to infection or central inflammation. One evident example in this response is leukocyte recruitment, which is rapid in systemic organs, but modest and delayed in the brain. However, the brain exhibits key features of inflammation and in response to acute insults, and the resident cellular elements, including glial cells, release inflammatory mediators within minutes or hours in response to acute insults(3). Glial cells, particularly microglia and astrocytes, are responsible for the immune functions within the brain, and they play roles in inflammatory response. Microglia, the macrophages of brain parenchyma, are in a downregulated state as compared with other tissue macrophages in the healthy brain. However, they are rapidly stimulated in response to injury or infection, and their morphology changes and acquires an array of functions, including phagocytosis, up-regulation of cell-surface molecules and the production and secretion of inflammatory mediators(8). A.M. BLANCO, C. GUERRI In addition to microglia, astrocytes are also important in the immune response, contributing to the establishment and maintenance of the blood-brain barrier (BBB)(9) and modulating the migration of monocytes and lymphocytes across the BBB(10). Astrocytes also respond vigorously to brain injury and seem to play an important role in the fine tuning of brain inflammation(11). Indeed, injury to CNS damage is inevitably accompanied by astrocytic hypertrophy, proliferation, and altered gene expression, a process commonly referred to as reactive astrogliosis(12) which is associated with inflammation(13). Depending on the disease context, however, astrogliosis can be seen as either a positive event that promotes neuronal and glial survival via the production of neurotrophins and growth factors, or as a negative influence on regeneration via the inhibition of neuronal and glial growth and migration. The diffuse nature of reactive astrogliosis in the CNS suggests a role either for soluble mediators, such as cytokines, and/or the presence of an integrated astrocyte-to-astrocyte syncytium that enables the transfer of information across extended distances. The cytokines for which the evidence is most compelling in the initiation and modulation of reactive gliosis include IL-1-β, TNF-α, IFN-γ, and TGF-β. Glial cells express receptors for all these cytokines, and each one appears to fulfil a different functional role in the astrocyte response(14). Stimulation of astrocytes in response to a neuropathologic process triggers the activation of an innate immune response (see below), leading to the production of inflammatory cytokines and free radicals, as well as to the expression of major histocompatibility complex II molecules(15). This functional reprogramming may be essential for maintaining homeostasis and the local regulation of inflammatory and immune responses(16). Among the cytokines, IL-1-β has been considered an important mediator of inflammatory responses in the CNS. It has been implicated in a number of neurodegenerative conditions, including Alzheimer´s disease(17), and it is vastly produced under conditions of brain damage, disease, or stress(18). Although the mechanisms of these effects are unclear, IL-1 is initially released by glial cells, acting on astrocytes and microglia to induce the production of additional cytokines and growth factors, thereby promoting inflammatory activity in the brain(19, 20). Indeed, IL-1 promotes glial scaring or astrogliosis when directly injected into the CNS, thus suggesting a potential role of IL-1 in mediating astrocytic hypertrophy upon neuronal damage(21). Finally, although extensive data suggest that inflammation contributes to the development of many CNS diseases, controversy regarding whether neuroinflammation and glial (microglial and astroglial) activation are beneficial or 189 Inmunol3/2006 copia 13/12/06 16:38 Página 190 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS detrimental remains. Indeed, many mediators produced as a result of microglial and astroglial activation have a dual role; they can be neuroprotective as well as neurotoxic, and may participate in long-term repair and recovery. The complex interplay and balance between diverse mediators and environmental factors may ultimately determine the outcome of acute CNS injury and the initiation and progression of inflammatory brain damage. A deeper knowledge of the mechanisms underlying the glial response may lead to the identification of potential therapies that will selectively encourage repair in the injured brain. INNATE IMMUNITY IN THE CNS: ROLE OF TRL4/ IL-1RI SIGNALLING The immune system is subdivided into two interactive branches, namely, the innate (cellular) and adaptive (humoral) immune systems. Both systems have been shown to participate in infectious and autoimmune responses in the CNS. In general, innate immunity represents the first line of defence against pathogens and does not require prior exposure to foreign antigens to be triggered. Cell types that make up the innate immune system include macrophages, neutrophils, dendritic cells, natural killer cells, and microglia and perivascular macrophages in the CNS. In contrast, the induction of adaptive immunity requires signals provided by the innate immune system to facilitate the expansion of antigen-specific T and B lymphocytes, which are important for antibody production and the formation of long-lived memory cells. Unlike adaptive immunity, in which a vast number of potential antigens can be recognized by T and B cells because of random gene rearrangements of their specific antigen receptors, innate immune system cells must recognize their cognate antigens by virtue of a predetermined subset of germ line-encoded receptors. As a result of this limited receptor expression, cells of the innate immune system may not be able to recognize every possible antigen; but may instead focus on a few highly conserved structures expressed by large groups of microorganisms. These conserved structural motifs are referred to as pathogen-associated molecular patterns (PAMPs), and the receptors of the innate immune system that recognize these molecules are known as the «Toll-like receptors» (TLRs). At present, eleven TLRs have been identified in humans, while 13 can be found in the mouse genome. TLRs 1-9 are conserved between both species and they all share a common cytosolic TIR domain (see below)(22). Among these receptors, TLR4 was the first human TLR to be identified. It interacts with lipopolysaccharide (LPS), a major component of the gram-negative bacterial cell wall. This interaction and the subsequent signalling response of TLR4 has been extensively studied(22). 190 VOL. 25 NUM. 3/ 2006 Interestingly, the stimulation of TLRs triggers proinflammatory signalling pathways similar to those activated by IL-1-β. TLRs have been shown to be a member of a large superfamily that includes the interleukin-1 receptors (IL1Rs)(23, 24). TLRs and IL-1Rs have a conserved region of ~ 200 amino acids in their cytoplasmic tails, which is known as the Toll/IL-1R (TIR) domain(24-27). By contrast, the extracellular regions of TLRs and IL-1Rs differ markedly(28). Activation of IL-1R and TLRs shares downstream signalling molecules, which culminate in the activation of nuclear factor-κ B (NFκB), a transcription factor that regulates the expression of a wide array of genes involved in immune responses. IL-1R and TLRs also signal through the mitogen-activated protein kinases (MAPKs), such as extracellular signal-regulated kinase (ERK), p38 and c-jun N-terminal kinase (JNK)(29). A diagram depicting the major steps involved in TLR4 and IL-1RI signalling pathways is presented in Figure 1. The activation of TLR4 and IL-1RI triggers the association of MyD88 (myeloid differentiation primary-response protein 88)(30), which in turn recruits IRAK-4 (IL-1 associated kinase4)(31) thereby allowing the association of IRAK-1(32). IRAK4 is activated during the formation of this complex (complex I), leading to the hyperphosphorylation of IRAK-1, which then induces the interaction of TRAF6 (tumour necrosis factor receptor-associated factor 6) with complex I(33). The association IRAK-4-IRAK-1-TRAF6 causes some conformational change in one or more of these factors, leading to their disengagement from the receptor complex. Complex I interacts at the membrane level with another preformed complex consisting of TAK-1 (transforming growth factor-α-activated kinase-1), TAB-1 (TAK-binding protein) and TAB-2(34) forming a second complex or complex II. This interaction induces phosphorylation of TAB-2 and TAK-1, which then translocate together with TRAF6 and TAB-1 to the cytosol. TAK-1 is subsequently activated in the cytoplasm, leading to the activation of the Iκ-B-α-kinase complex (IKK). The phosphorylation of Iκ-B-α leads to its degradation, the release of NF-κB and the activation of NFκB-dependent genes, such as IL-1-β, TNF-α, IL-6, COX-2, iNOS(35). Biochemical evidence also indicates that the activation of complex II triggers the stimulation of p42/p44 ERK, p38 and JNK(23), which in turn regulate the nuclear activation of the transcriptional factors NF-κB and AP-1 (activator protein1)(36). Notably, because NF-κB and AP-1 binding sites have been found in the promoters of many genes that are induced during inflammation, it has been claimed that the large number of specific receptors of the innate immune system exerts their manifold gene activations principally through the MAP kinase and the IKK-NF-κB pathways(22, 24, 37). Inmunol3/2006 copia 13/12/06 16:38 Página 191 INMUNOLOGÍA A.M. BLANCO, C. GUERRI Figure 1. TLR4 and IL-1RI signalling pathways. Activation of TLR4 and IL-1RI by their ligands, LPS and IL-1-β share downstream signalling molecules (MyD88, Traf-6, IRAKs) forming complex I, that activates complex II formation (Traf-6, IRAKs, TAB-1, -2 and TAK-1), which culminates in the activation of MAPKs and transcriptional factors (NF-κB and AP-1), and regulates the expression of target genes in immune response and cell death. The aforementioned signalling pathways suggest that stimulation with either IL-1 or LPS could lead to the transcriptional induction of common sets of genes that encode pro-inflammatory proteins such as chemokines, cytokines, proteases and metabolic enzymes, like inducible nitric oxide synthase (iNOS) and ciclooxygenase-2 (COX2)(36). Indeed, iNOS and COX-2 are important components of the post-lesion inflammatory cascade in various types of brain damage(38-40). Finally, significant advance in recent years has led us to understand the role of the innate immune response in the CNS and the involvement of TLRs as vital players in this orchestrated response in the brain. In the brain and spinal cord, the expression of TLRs in glial cells has been documented and this expression is increased during neuroinflammation events(41). Recent evidences also indicate that a chronic activation of the innate immune response and signalling may lead to neuronal cell loss and may be involved in neurodegeneration(42). The innate immune response in the CNS is necessary to resolve potential pathogenic conditions, and although the transient upregulation of inflammatory events in the brain may not lead to cell death(43), overactivation of innate immunity may lead to neurodegeneration(42). Indeed, cell damage and apoptosis occur concomitantly as a result of the stimulation of signalling pathways and inflammatory mediators associated with TLR4/IL-1RI, which in turn, induce a highly inflammatory response in the CNS under conditions of damage, disease, or stress(44). ETHANOL AND INNATE IMMUNE SYSTEM Clinical and experimental studies revealed that ethanol intake affects both the immune and inflammatory systems(45), resulting in specific defects in the cellular components of the innate immune responses to bacterial and viral pathogens(46, 47). Ethanol is known to alter cytokine levels in a variety of tissues including lung, liver and brain. However, the regulation of the immune response by ethanol is complex and depends on dose, duration of ethanol treatment (acute vs. chronic) 191 Inmunol3/2006 copia 13/12/06 16:38 Página 192 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS and the type of cell and pathogen(48). Acute ethanol treatment impairs immune functions, interfering with the inflammatory response and increasing the host susceptibility to a variety of infections, such as bacterial pneumonia(49). Accordingly, ethanol suppresses the TLR3(50) and TLR4(51) response in monocytes or macrophages in vitro, decreasing the synthesis and secretion of numerous cytokines(52). Conversely, chronic ethanol consumption is associated with elevated serum levels of proinflammatory cytokines(53, 54), and the activation of some of these cytokines, such as IL-1-β and TNF-α and their signalling transduction response(55) is involved in ethanol-induced liver damage(56). Increasing evidence demonstrate that the activation of the innate immune response plays a crucial role in the development of alcoholic liver disease(57). The gastrointestinal tract seems to be the initial target of ethanol, leading to an activation of the innate immune response. Alcohol consumption is associated with the impaired barrier function of the intestinal mucosa in patients with various stages of alcoholic liver injury(58), increasing the plasma levels of endotoxins such as lipopolysaccharide (LPS) (a component of gramnegative bacterial cell wall). Increased exposure to LPS is an important contributor to the activation of the innate immune response in the liver. In addition, chronic ethanol also exacerbates the response of Kupffer cells to LPS, resulting in an increased production of inflammatory cytokines(57). Recent studies have identified a number of intermediates in the TLR-4 signalling cascade that are affected by chronic ethanol, including an increased expression of CD14, as well as enhanced activation of NF-κB and the MAPK family members, p44/p42 ERK and p38(57). The importance of TLR4 in the development of alcohol liver diseases is exemplified by the decrease in hepatic damage in mice that have a natural mutation and lack a functional TLR4(59). ETHANOL AND BRAIN DAMAGE: ROLE OF THE INFLAMMATORY MEDIATORS The brain is one of the major target organs for ethanol actions, and heavy alcohol consumption results in significant alterations of the brain structure, physiology and function. Alcoholics have reduced brain weight compared with nondrinking controls(60), and the degree of brain atrophy correlates with the rate and amount of alcohol consumed over a lifetime. The reduction in brain weight and volume has been attributed to a loss of white matter, which occurs primarily in the frontal lobe and is specifically susceptible to alcohol-related brain damage(61, 62). Furthermore, neuronal loss has also been documented in specific regions of the cerebral cortex, hippocampus and cerebellum from alcoholic brains(62, 63). 192 VOL. 25 NUM. 3/ 2006 Current neuroimaging studies also indicate that chronic alcohol use induces important changes in brain morphology, such as cortical and subcortical atrophy, and confirms that frontal lobe structures are specifically vulnerable to the effects of ethanol with shrinkage in this area, largely owing to a loss of white matter(64). The mechanisms involved in white matter loss remain unclear, although glial impairments in conjunction with astrocytic loss and death have been reported in the prefrontal cortex and hippocampus from human alcoholic brains(65-68). Changes in myelination might also occur during chronic alcoholism, since both glial fibrillary acidic protein (GFAP) gene expression (a marker of astrocytes) and myelinassociated genes were down-regulated in the brain of alcoholics(69, 70). A recent report demonstrates that astrocytes promote myelination in response to electrical impulses(71), suggesting that alterations and cell death in astrocytes could cause deficits and loss of myelin in alcoholics. Alcohol-related neuronal loss has been also documented in specific regions of the cerebral cortex, hippocampus and cerebellum(62). Experimental evidence also demonstrates that alcohol is toxic for neural cells in culture(72-75) and that acute intoxication can cause brain damage and even neurodegeneration in some cases(76, 77). Indeed, neural damage and neurodegeneration have been demonstrated in short-term binge drinking animal models, leading to neuronal loss in specific brain regions including, olfactory and forebrain corticolimbic association areas, entorhinal and pirirhinal cortex and hippocampus, brain areas involved in many aspects of learning and spatial memory(77). These results suggest that a drinking pattern, specifically binge drinking in which high blood and brain alcohol levels are achieved, is an important factor in the ethanol-induced neuropathology, and that alcoholic neurodegeneration could occur primarily as a result of binge drinking episodes(76-78). The neuropathological processes underlying the effects of ethanol on neural damage are largely unknown, although several mechanisms and concurring factors have been proposed to contribute to neurodegeneration. Among the mechanisms proposed include: the participation of excitotoxic events and nitric oxide generation(79), the involvement of glial swelling and brain edema(78), and the production of free radicals causing oxidative stress(80). The latter mechanism includes the ability of ethanol to enhance free radical species by inducing the cytochrome P450 2E1 (CYP2E1)(81), which leads to the generation of hydroxyethyl radicals(82), reactive oxygen species (ROS)(83) and the activation of NF-κB(80). Interestingly, the induction of both CYP2E1 and ROS was also noted in astrocytes exposed to ethanol(81), suggesting that glial activation might contribute to the induction of free radical species by ethanol in the brain. Inmunol3/2006 copia 13/12/06 16:38 Página 193 INMUNOLOGÍA Recent findings also suggest the involvement of inflammation in alcohol-induced brain damage. These studies demonstrate that chronic ethanol treatment not only increases the levels of cytokines (IL-1-β, TNF-α) and inflammatory mediators (iNOS and COX-2) in the rat's brain and in cultured astrocytes, but also activates signalling pathways that are classically associated with inflammation (MAPKs, NF-κB, AP-1, see below). Notably these inflammatory events are associated with an increase in cell death(75). This suggests that activation of glial cells by ethanol might trigger the production of toxic compounds, such as ROS or nitric oxide(73), inflammatory cytokines and glutamate, which might contribute to ethanolinduced brain damage, similar to what occurs in several brain disorders and neurodegenerative diseases(4, 5, 84). The evidence indicating the presence of ethanol-induced inflammatory mediators in the brain originates from several studies mainly performed in neural cells in culture. These studies demonstrate that ethanol influences the expression of iNOS and COX-2 in both the brain and neural cells exposed to ethanol(75). It is known that both enzymes are induced only in response to different stimuli including stress, inflammation or neural damage(38-40). Ethanol is known to influence NO production and iNOS expression in a number of cellular systems, and in the presence or absence of additional stimuli, such as cytokines or LPS. For example, ethanol enhances the cytokine-induced iNOS gene and protein expression in C6 glioma cells, in immortalized astrocytes(85, 86), in BBB cells(87) and in embryonic cortical neurons(88). Stimulation of NO production and iNOS expression also occurs as a direct effect of ethanol, as demonstrated in brain homogenates from the guinea pig model of prenatal ethanol exposure(89), in brain lysates from chronic-alcohol fed rats(75) and in cerebral pial cultures(90). In fact, the induction of iNOS can occur in astrocytes upon 30 min treatment with ethanol(73). Up-regulation of COX-2 expression has also been observed in the rat’s brain after acute (91) and chronic ethanol administration(75, 91, 92), as well as in ethanol-exposed astrocytes(73, 93). Interestingly, the study by Luo et al (2001)(93), demonstrated that ethanol selectively increased COX-2 levels in astrocytes, but not in neurons. However, a clearer demonstration that ethanol induces COX-2 in astrocytes is seen in a recent study showing a fast induction of COX-2 upon 30 min of ethanol treatment(73). This study also demonstrates that the activation of NF-κB is critical for the ethanol-induced up-regulation of iNOS and COX-2 in astrocytes, since inhibition of NF-κB activity either by pyrrolidine dithiocarbamate (PDTC) or BAY 11-7082 suppresses the induction of iNOS and COX2, suggesting a transcriptional regulation of these inflammatory mediators by NF-κB(73). A.M. BLANCO, C. GUERRI ETHANOL ACTIVATES SIGNALLING PATHWAYS AND TRANSCRIPTION FACTORS INVOLVED IN INFLAMMATORY BRAIN DAMAGE Stimulation of the innate immune system triggers the activation of NF-κB (see Figure 1) and the induction of numerous immune and inflammatory response genes(94) encoding cytokines, chemokines, enzymes (iNOS and COX2)(95-97) and adhesion molecules. Several in vitro and in vivo studies clearly demonstrate that both acute and chronic ethanol treatments cause the activation of NF-κB. Short-term ethanol treatment (25-100 mM) has been shown to induce NF-κB DNA binding in human astroglial cells(98), similarly to long-term ethanol–treated rat astrocytes(75). Chronic ethanol treatment also induces activation of NF-κB in liver(99), brain(100) and in the cerebral cortex of ethanol-fed rats(75). In the last study the stimulation of NF-κB was accompanied by a significant decrease in the cytoplasmic levels of IκB-α, and by elevated levels of cytokines, as well as COX-2 and iNOS(75). These findings suggest that NF-κB is activated in response to challenge by both acute and chronic ethanol, although the mechanism involved remains unclear. The activity of NF-κB is controlled at multiple levels, most notably by the regulation of its subcellular localization. NF-κB is retained in the cytoplasm in resting cells, and it is transported to the nucleus in response to a diverse range of stimuli(101, 102), where it binds specifically to κB enhancer elements of DNA and alters the expression of a great number of proinflammatory genes(35). Following stimulation, the duration of NF-κB activation may be transient or persistent, depending on the cellular stimulus and cell type. The temporal profile is of considerable clinical relevance because whereas rapid induction of NF-κB is beneficial for immune response to infection or injury, long-term activation has been demonstrated to be associated with chronic inflammatory diseases, such as multiple sclerosis. Notably, chronic ethanol treatment triggers sustained activation of NF-κB in the rat’s brain and in astrocytes in culture, and this event is associated with elevated levels of inflammatory mediators, IL-1-β and TNF-α(75). Likewise, a recent study demonstrated that NFκB is sustained in astrocytes in response to stimulation with IL-1-β(103), suggesting that elevated levels of IL-1 could mediate the persistent activation of NF-κB observed in both astrocytes and in the brain of alcohol-fed rats, and might contribute to a prolonged induction of inflammatory mediators and ethanol-induced damage in the brain. Furthermore, despite the fact that the induction of NFκB is directly regulated by IKK, there is evidence demonstrating that IKKs themselves are also activated through phosphorylation by an upstream kinase(s). Candidates 193 Inmunol3/2006 copia 13/12/06 16:38 Página 194 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS for this kinase include NF-κB-inducing kinase (NIK) and mitogen-activated protein kinase (MAPK) pathways (p44/p42 ERK, JNK and p38)(104-106) (see Figure 1). Cumulative data demonstrates the participation of the MAPKs pathway in inflammation processes(107). Moreover, the stimulation of this pathway, apart from activating NF-κB, can also trigger the activator protein-1 (AP-1) transcriptional activity. The AP-1 family is dependent on its phosphorylation by MAPK or MAPK-activated kinases(108), resulting in the transcriptional activation of genes of the jun and fos-family or in the activation at the protein level. Ethanol withdrawal hyperactivity is associated with the expression of the early genes c-fos and c-jun(109), with transient selective increases in the DNAbinding activity of immediate early genes (IEGs)-encoded AP-1 in the brain(110, 111). Notably, chronic ethanol treatment increases the MAPKs and AP-1 expression in liver, brain and astrocytes(57, 75), and these effects are associated with inflammation and cell damage. Finally, although the activation of MAPKs can mediate the inflammation and release of neurotoxic molecules, it is obvious that the activation of MAPK under certain circumstances may be beneficial for the plasticity of the CNS. Nevertheless, based on the few in vivo and in vitro studies available to date, the MAPKs, which mediate the activation of glial cells by ethanol with neurotoxic consequences, represent promising targets for the pharmacotherapy for acute brain insults and neuroinflammatory injury induced by ethanol. Finally, neural injury and cell death have been associated with many neurological and neuroinflammatory disorders(112), and several reports demonstrate that one of the mechanisms implicated in ethanol-induced neurotoxicity is the promotion of apoptosis. Our recent studies suggest a role for inflammation in ethanol-induced cell death in brain and in astrocytes: we found that ethanol-induced activation of MAPKs, NF-κB, AP-1 were associated with increased apoptosis in the brain and in astrocytes(74, 75). Furthermore, we were able to prevent ethanol-induced apoptosis in astrocytes by blocking the receptors TLR4 and IL-1RI(74) (see below), suggesting the involvement of the innate immune response in the ethanolinduced astrocytic death. Finally, although apoptosis occurs in neurodegenerative disorders(113, 114), we cannot exclude the possibility that ethanol also causes necrotic cell death since it has been suggested that necrosis often triggers a prominent inflammatory reaction, while apoptosis results in the uneventful removal of dying cells, with little or no inflammation 115). Figure 2 illustrates the cascade of events by which ethanol induces glial activation through the stimulation of intracellular signalling pathways, and triggers the production of inflammatory mediators and toxic compounds that could 194 VOL. 25 NUM. 3/ 2006 exacerbate an inflammatory response leading to astrocytic and neural death. INVOLVEMENT OF TLR4/IL-1RI IN ETHANOLINDUCED INFLAMMATORY RESPONSE IN ASTROCYTES As already discussed, stimulation of TLRs triggers the initial innate immune response, which ultimately leads to inflammatory gene expression and the clearance of infectious agents(24), although an excessive production of inflammatory molecules contributes to the pathogenesis of inflammatory diseases(42). Ethanol is known to affect the innate immune response in several organ systems(45, 57). Nevertheless, very little is known about the potential action of ethanol on the CNS immune system, as well as the participation of inflammation in alcohol-induced brain damage. The CNS exhibits well-organized innate immune reactions. In response to injury(116, 117) and infections(43, 118), glial cells are capable of mounting a quick and effective response to control an infection until cells of the peripheral adaptive immune system can be recruited (119, 120). Microglia and astrocytes express TLR2, TLR4, TLR5 and TLR9(41, 121, 122), respond functionally with cytokine and chemokine production(121, 122), and are capable of contributing to an inflammatory environment in the CNS(15, 123) following a variety of infectious or inflammatory insults(124). Our recent studies demonstrate that astrocytes respond to ethanol, by secreting cytokines and other inflammatory mediators(73, 75), and by contributing to an inflammatory environment in the brain of alcohol-fed animals(75). These effects seem to be mediated by the ethanol-induced activation of TLR4/IL-1RI in astrocytes (74). In fact, we recently demonstrated that ethanol, at physiological relevant concentrations (10 mM or 50mM), is capable of inducing a rapid activation of the TLR4/IL-1RI signal-transduction pathways(74) in a similar manner to the situation when cells are stimulated with LPS and IL-1-β(125-128). Thus, we observed a rapid phosphorylation (within 10 min) of IRAK, p44/p42 ERK, SAPK/JNK and p38 MAPK, upon ethanol stimulation. In addition, a subsequent downstream activation of the transcription factors NF-κB and AP-1, as well as the upregulation of iNOS and COX-2 were noted after a 30-min ethanol treatment. We also found a time lag between the maximal COX-2 and iNOS expression and the increase in cell death, observed at 3 h of ethanol treatment(74). Consistent with the hypothesis that ethanol mediates inflammatory events by activating TLR4/IL-1RI, we showed that both the ethanol-induced inflammatory mediators and the cell death in astrocytes were abolished by blocking the activation of these receptors with neutralizing antibodies(74). These results Inmunol3/2006 copia 13/12/06 16:38 Página 195 INMUNOLOGÍA A.M. BLANCO, C. GUERRI Figure 2. Potential mechanisms of ethanol-induced brain damage. Ethanol triggers signalling inflammatory responses and the production of inflammatory mediators and toxic compounds by activating TLR4 and IL-1RI in glial cells, and this could exacerbate the inflammatory response leading to brain damage by astrocytic and neural death. support the notion that ethanol-induced inflammatory mediators in the brain are mediated via activation of glial TLR4/IL-1RI signalling pathways. At present, it is not clear how ethanol might interact with TLR4/IL-1RI to either activate or inhibit their signalling response, which depends on the cell type and ethanol concentration. It is well established that ethanol interacts with membrane lipids and influences the function of membrane proteins(129). A plausible explanation is that ethanol can either facilitate or disrupt the recruitment of these receptors, depending on the ethanol concentration and the physicochemical characteristics of the cell membrane. A high ethanol concentration can perturb membrane lipid microdomains, such as lipid rafts, resulting in disruption of the receptor function. On the contrary, low ethanol concentrations might facilitate the aggregation and interaction of proteins within the membrane, thus allowing their activation and signalling through the lipid rafts. We suggest a schematic model of low and high concentrations of ethanol effects on lipid rafts and the signal transduction of TLR4 and IL-1RI (Figure 3). Lipid rafts are cholesterol/sphingomyelin-enriched membrane microdomains, which are involved in the recruitment of molecules with signal transduction capabilities(130, 131), and are now recognized as important sites for initial immune cell activation. The presence of TLR2 and TLR4 within lipid rafts and their subsequent clustering in response to LPS(132, 133) support their role in the innate immune response(132135). Indeed, disruption of lipid rafts leads to an inhibition of TLR internalization and signalling(132). High concentrations of ethanol appear to interfere with lipid raft clustering, leading to the suppression of TLR4 signalling in murine macrophages(51, 136). However, low concentrations of ethanol might promote receptor recruitment into lipid rafts, leading to dimerization and signalling. Furthermore, as several studies have demonstrated that ethanol suppresses both cytokine-induced expression of iNOS(85, 86) and LPS-induced NO production(137) in glial cells, ethanol may possibly interfere with the recruitment of TLRs into the lipid rafts in the presence of other stimuli (e.g. LPS, cytokines), leading to an inhibitory, rather than an additive effect on the TLR signalling transduction. 195 Inmunol3/2006 copia 13/12/06 16:38 Página 196 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS VOL. 25 NUM. 3/ 2006 Figure 3. Suggested model by which ethanol mediates activation of TLR4/IL-1RI through its interactions with lipid rafts. We hypothesize that low concentrations of ethanol (10-50 mM) might facilitate TLR4 and IL-1RI aggregation and their recruitment into lipid rafts, leading to the activation of their signal transduction. On the contrary, high ethanol concentration can perturb membrane lipids, including lipid rafts, and result in a disruption of the receptors function and signalling. AcP= Accessory protein. Finally, since lipid rafts are considered important for TLRs signalling, it should be expected that the levels of ethanol intake would cause distinct alterations in the membrane lipid composition and subsequently, affect the response of TLRs in different ways. Indeed, while acute ethanol treatment down-regulates the production of proinflammatory cytokines induced by LPS in human monocytes(138, 139), chronic ethanol treatment (7 days in vitro), results in augmentation of LPS-induced TNF-α(48). To summarize, although ethanol effects on TLR4/IL1RI are complex, data suggest that TLR4/IL-1RI are targets of ethanol-induced inflammatory damage in many organs, including the brain. CONCLUSIONS Results of studies reviewed in this article indicate that ethanol consumption activates a wide range of inflammatory mediators and signalling pathways in the brain, which are associated with inflammation and the immune response. In particular, the ethanol-induced inflammatory response seems to be related to the activation and signalling of TLR4 196 and IL-1RI, the LPS and IL-1β specific receptors. Further studies are required to understand the mechanisms by which ethanol activates TLR4/IL-1RI, although it is clear that these receptors are targets of ethanol-induced inflammatory damage in astrocytes and the brain. However, there is still much to be understood about the nature of CNS inflammation and the molecular effects of ethanol in the brain before the development of a clinical treatment may be successfully explored. These results contribute to our understanding of the brain injury caused by ethanol, and they may as well lead to the possibility of new treatments and/or intervening strategies to restore the brain damage induced by ethanol. ACKNOWLEDGMENTS The work of the authors is supported by Grants from Ministerio de Educación y Ciencia (SAF 2003-06217 and SAF 2006-02178), Instituto Carlos III, FIS-Red RTA G03/005, Dirección General. Drogodependendecias, GV, and Fundación de Investigación Médica Mutua Madrileña. We wish to thank Marisa March for her assistance in the preparation of the manuscript. Inmunol3/2006 copia 13/12/06 16:38 Página 197 INMUNOLOGÍA DISCLOSURES The authors have no financial conflict of interest. CORRESPONDENCE TO: Dra. Consuelo Guerri Sirera C/ E. P. Avda. Autopista del Saler, 16-3 (junto Oceanográfico) 46013 Valencia (Spain) E-mail: [email protected] REFERENCES 1. Tedgui A, Mallat Z. Cytokines in atherosclerosis: pathogenic and regulatory pathways. Physiol Rev 2006;86:515-581. 2. Dalgleish AG, O'Byrne K. Inflammation and cancer: the role of the immune response and angiogenesis. Cancer Treat Res 2006;130:138. 3. Lucas SM, Rothwell NJ, Gibson RM. The role of inflammation in CNS injury and disease. Br J Pharmacol 2006;147(Suppl 1):S232240. 4. Hunot S, Hirsch EC. Neuroinflammatory processes in Parkinson's disease. Ann Neurol 2003;53 (Suppl 3):S49-58; discussion S58-60. 5. Giovannini MG, Scali C, Prosperi C, Bellucci A, Pepeu G, Casamenti F. Experimental brain inflammation and neurodegeneration as model of Alzheimer's disease: protective effects of selective COX2 inhibitors. Int J Immunopathol Pharmacol 2003;16(2 Suppl):3140. 6. Stoeck K, Bodemer M, Zerr I. Pro- and anti-inflammatory cytokines in the CSF of patients with Creutzfeldt-Jakob disease. J Neuroimmunol 2006;172:175-181. 7. Perry VH, Cunningham C, Boche D. Atypical inflammation in the central nervous system in prion disease. Curr Opin Neurol 2002;15:349354. 8. Hanisch UK. Microglia as a source and target of cytokines. Glia 2002;40:140-155. 9. Prat A, Biernacki K, Wosik K, Antel JP. Glial cell influence on the human blood-brain barrier. Glia 2001;36:145-155. 10. Weiss JM, Berman JW. Astrocyte expression of monocyte chemoattractant protein-1 is differentially regulated by transforming growth factor beta. J Neuroimmunol 1998;91:190-197. 11. Dietrich PY, Walker PR, Saas P. Death receptors on reactive astrocytes: a key role in the fine tuning of brain inflammation? Neurology 2003;60:548-554. 12. Ridet JL, Malhotra SK, Privat A, Gage FH. Reactive astrocytes: cellular and molecular cues to biological function. Trends Neurosci 1997;20:570-577. 13. Little AR, O'Callagha JP. Astrogliosis in the adult and developing CNS: is there a role for proinflammatory cytokines? Neurotoxicology 2001;22:607-618. 14. John GR, Lee SC, Song X, Rivieccio M, Brosnan CF. IL-1-regulated responses in astrocytes: relevance to injury and recovery. Glia 2005;49:161-176. 15. Dong Y, Benveniste EN. Immune function of astrocytes. Glia 2001;36:180-190. 16. Benveniste EN. Cytokine actions in the central nervous system. Cytokine Growth Factor Rev 1998;9:259-275. A.M. BLANCO, C. GUERRI 17. Mrak RE, Griffin WS. Potential inflammatory biomarkers in Alzheimer's disease. J Alzheimers Dis 2005;8:369-375. 18. Patel HC, Boutin H, Allan SM. Interleukin-1 in the brain: mechanisms of action in acute neurodegeneration. Ann N Y Acad Sci 2003;992:3947. 19. Merrill JE, Benveniste EN. Cytokines in inflammatory brain lesions: helpful and harmful. Trends Neurosci 1996;19:331-338. 20. Benveniste EN. Cytokines: influence on glial cell gene expression and function. Chem Immunol 1992;52:106-153. 21. John GR, Chen L, Rivieccio MA, Melendez-Vasquez CV, Hartley A, Brosnan CF. Interleukin-1beta induces a reactive astroglial phenotype via deactivation of the Rho GTPase-Rock axis. J Neurosci 2004;24:2837-2845. 22. Dunne A, O'Neill LA. The interleukin-1 receptor/Toll-like receptor superfamily: signal transduction during inflammation and host defense. Sci STKE 2003;2003(171):3-17. 23. O'Neill LA, Dinarello CA. The IL-1 receptor/toll-like receptor superfamily: crucial receptors for inflammation and host defense. Immunol Today 2000;21:206-209. 24. Akira S, Takeda K. Toll-like receptor signalling. Nat Rev Immunol 2004;4:499-511. 25. Kurt-Jones EA, Popova L, Kwinn L, Haynes LM, Jones LP, Tripp RA, et al. Pattern recognition receptors TLR4 and CD14 mediate response to respiratory syncytial virus. Nat Immunol 2000;1:398401. 26. O'Neill L. The Toll/interleukin-1 receptor domain: a molecular switch for inflammation and host defence. Biochem Soc Trans 2000;28: 557-563. 27. Takeda K, Kaisho T, Akira S. Toll-like receptors. Annu Rev Immunol 2003;21:335-376. 28. Takeda K, Akira S. TLR signaling pathways. Semin Immunol 2004;16:3-9. 29. Yang Y, Zhou H, Li W, Zhou M, Zeng Z, Xiong W, et al. Lipopolysaccharide (LPS) regulates TLR4 signal transduction in nasopharynx epithelial cell line 5-8F via NFκB and MAPKs signaling pathways. Mol Immunol 2006. May 2 (in press, available on line). 30. Wesche H, Henzel WJ, Shillinglaw W, Li S, Cao Z. MyD88: an adapter that recruits IRAK to the IL-1 receptor complex. Immunity 1997;7:837-847. 31. Li S, Strelow A, Fontana EJ, Wesche H. IRAK-4: a novel member of the IRAK family with the properties of an IRAK-kinase. Proc Natl Acad Sci USA 2002;99:5567-5572. 32. Cao Z, Henzel WJ, Gao X. IRAK: a kinase associated with the interleukin-1 receptor. Science 1996;271:1128-1131. 33. Cao Z, Xiong J, Takeuchi M, Kurama T, Goeddel DV. TRAF6 is a signal transducer for interleukin-1. Nature 1996;383:443-446. 34. Jiang Z, Ninomiya-Tsuji J, Qian Y, Matsumoto K, Li X. Interleukin1 (IL-1) receptor-associated kinase-dependent IL-1-induced signaling complexes phosphorylate TAK1 and TAB2 at the plasma membrane and activate TAK1 in the cytosol. Mol Cell Biol 2002;22:7158-7167. 35. DiDonato JA, Hayakawa M, Rothwarf DM, Zandi E, Karin M. A cytokine-responsive IκB kinase that activates the transcription factor NF-κB. Nature 1997;388:548-554. 36. Kracht M, Saklatvala J. Transcriptional and post-transcriptional control of gene expression in inflammation. Cytokine 2002;20:91106. 37. Martin MU, Wesche H. Summary and comparison of the signaling 197 Inmunol3/2006 copia 13/12/06 16:38 Página 198 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 198 mechanisms of the Toll/interleukin-1 receptor family. Biochim Biophys Acta 2002;1592:265-280. Heales SJ, Bolanos JP, Stewart VC, Brookes PS, Land JM, Clark JB. Nitric oxide, mitochondria and neurological disease. Biochim Biophys Acta 1999;1410:215-228. O'Banion MK. Cyclooxygenase-2: molecular biology, pharmacology, and neurobiology. Crit Rev Neurobiol 1999;13:45-82. Yamada K, Komori Y, Tanaka T, Senzaki K, Nikai T, Sugihara H, et al. Brain dysfunction associated with an induction of nitric oxide synthase following an intracerebral injection of lipopolysaccharide in rats. Neuroscience 1999;88:281-294. Bsibsi M, Ravid R, Gveric D, van Noort JM. Broad expression of Toll-like receptors in the human central nervous system. J Neuropathol Exp Neurol 2002;61:1013-1021. Campbell A. Inflammation, neurodegenerative diseases, and environmental exposures. Ann N Y Acad Sci 2004;1035:117-132. Rivest S. Molecular insights on the cerebral innate immune system. Brain Behav Immun 2003;17:13-19. Ehrlich LC, Peterson PK, Hu S. Interleukin (IL)-1 beta-mediated apoptosis of human astrocytes. Neuroreport 1999;10:1849-1852. MacGregor RR. Alcohol and immune defense. Jama 1986;256:14741479. Cook RT. Alcohol abuse, alcoholism, and damage to the immune system--a review. Alcohol Clin Exp Res 1998;22:1927-1942. Nelson S, Kolls JK. Alcohol, host defence and society. Nat Rev Immunol 2002;2:205-209. Crews FT, Bechara R, Brown LA, Guidot DM, Mandrekar P, Oak S, et al. Cytokines and alcohol. Alcohol Clin Exp Res 2006;30:720730. Ruiz M, Ewig S, Torres A, Arancibia F, Marco F, Mensa J, et al. Severe community-acquired pneumonia. Risk factors and followup epidemiology. Am J Respir Crit Care Med 1999;160:923-929. Pruett SB, Schwab C, Zheng Q, Fan R. Suppression of innate immunity by acute ethanol administration: a global perspective and a new mechanism beginning with inhibition of signaling through TLR3. J Immunol 2004;173:2715-2724. Dai Q, Zhang J, Pruett SB. Ethanol alters cellular activation and CD14 partitioning in lipid rafts. Biochem Biophys Res Commun 2005;332:37-42. Goral J, Choudhry MA, Kovacs EJ. Acute ethanol exposure inhibits macrophage IL-6 production: role of p38 and ERK1/2 MAPK. J Leukoc Biol 2004;75:553-559. McClain CJ, Cohen DA. Increased tumor necrosis factor production by monocytes in alcoholic hepatitis. Hepatology 1989;9:349-351. McClain CJ, Barve S, Deaciuc I, Kugelmas M, Hill D. Cytokines in alcoholic liver disease. Semin Liver Dis 1999;19:205-219. Valles SL, Blanco AM, Azorin I, Guasch R, Pascual M, GomezLechon MJ, et al. Chronic ethanol consumption enhances interleukin1-mediated signal transduction in rat liver and in cultured hepatocytes. Alcohol Clin Exp Res 2003;27:1979-1986. Hoek JB, Pastorino JG. Ethanol, oxidative stress, and cytokineinduced liver cell injury. Alcohol 2002;27:63-68. Nagy LE. Recent insights into the role of the innate immune system in the development of alcoholic liver disease. Exp Biol Med (Maywood) 2003;228:882-890. Parlesak A, Schafer C, Schutz T, Bode JC, Bode C. Increased 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. VOL. 25 NUM. 3/ 2006 intestinal permeability to macromolecules and endotoxemia in patients with chronic alcohol abuse in different stages of alcoholinduced liver disease. J Hepatol 2000;32:742-747. Uesugi T, Froh M, Arteel GE, Bradford BU, Thurman RG. Tolllike receptor 4 is involved in the mechanism of early alcoholinduced liver injury in mice. Hepatology 2001;34:101-108. Kril JJ, Halliday GM. Brain shrinkage in alcoholics: a decade on and what have we learned? Prog Neurobiol 1999;58:381-387. de la Monte SM. Disproportionate atrophy of cerebral white matter in chronic alcoholics. Arch Neurol 1988;45:990-992. Harper C, Matsumoto I. Ethanol and brain damage. Curr Opin Pharmacol 2005;5:73-78. Harper C, Dixon G, Sheedy D, Garrick T. Neuropathological alterations in alcoholic brains. Studies arising from the New South Wales Tissue Resource Centre. Prog Neuropsychopharmacol Biol Psychiatry 2003;27:951-961. Alexander-Kaufman K, James G, Sheedy D, Harper C, Matsumoto I. Differential protein expression in the prefrontal white matter of human alcoholics: a proteomics study. Mol Psychiatry 2006;11:5665. Ikegami Y, Goodenough S, Inoue Y, Dodd PR, Wilce PA, Matsumoto I. Increased TUNEL positive cells in human alcoholic brains. Neurosci Lett 2003;349:201-205. Miguel-Hidalgo JJ, Wei J, Andrew M, Overholser JC, Jurjus G, Stockmeier CA, et al. Glia pathology in the prefrontal cortex in alcohol dependence with and without depressive symptoms. Biol Psychiatry 2002;52:1121-1133. Kril JJ, Halliday GM, Svoboda MD, Cartwright H. The cerebral cortex is damaged in chronic alcoholics. Neuroscience 1997;79:983998. Korbo L. Glial cell loss in the hippocampus of alcoholics. Alcohol Clin Exp Res 1999;23:164-168. Lewohl JM, Wixey J, Harper CG, Dodd PR. Expression of MBP, PLP, MAG, CNP, and GFAP in the Human Alcoholic Brain. Alcohol Clin Exp Res 2005;29:1698-1705. Liu J, Lewohl JM, Harris RA, Iyer VR, Dodd PR, Randall PK, Mayfield RD. Patterns of gene expression in the frontal cortex discriminate alcoholic from nonalcoholic individuals. Neuropsychopharmacology 2006;31:1574-82. Ishibashi T, Dakin KA, Stevens B, Lee PR, Kozlov SV, Stewart CL, et al. Astrocytes promote myelination in response to electrical impulses. Neuron 2006;49:823-832. Guerri C, Pascual M, Renau-Piqueras J. Glia and fetal alcohol syndrome. Neurotoxicology 2001;22:593-599. Blanco AM, Pascual M, Valles SL, Guerri C. Ethanol-induced iNOS and COX-2 expression in cultured astrocytes via NF-κ B. Neuroreport 2004;15:681-685. Blanco AM, Valles SL, Pascual M, Guerri C. Involvement of TLR4/type I IL-1 receptor signaling in the induction of inflammatory mediators and cell death induced by ethanol in cultured astrocytes. J Immunol 2005;175:6893-6899. Valles SL, Blanco AM, Pascual M, Guerri C. Chronic ethanol treatment enhances inflammatory mediators and cell death in the brain and in astrocytes. Brain Pathol 2004;14:365-371. Fadda F, Rossetti ZL. Chronic ethanol consumption: from neuroadaptation to neurodegeneration. Prog Neurobiol 1998;56:385431. Inmunol3/2006 copia 13/12/06 16:38 Página 199 INMUNOLOGÍA 77. Crews FT, Braun CJ, Hoplight B, Switzer RC, 3rd, Knapp DJ. Binge ethanol consumption causes differential brain damage in young adolescent rats compared with adult rats. Alcohol Clin Exp Res 2000;24:1712-1723. 78. Collins MA, Zou JY, Neafsey EJ. Brain damage due to episodic alcohol exposure in vivo and in vitro: furosemide neuroprotection implicates edema-based mechanism. FASEB J 1998;12:221-230. 79. Lancaster FE. Alcohol, nitric oxide, and neurotoxicity: is there a connection?--a review. Alcohol Clin Exp Res 1992;16:539-541. 80. Sun AY, Ingelman-Sundberg M, Neve E, Matsumoto H, Nishitani Y, Minowa Y, et al. Ethanol and oxidative stress. Alcohol Clin Exp Res 2001;25(5 Suppl ISBRA):237S-243S. 81. Montoliu C, Sancho-Tello M, Azorin I, Burgal M, Valles S, RenauPiqueras J, et al. Ethanol increases cytochrome P4502E1 and induces oxidative stress in astrocytes. J Neurochem 1995;65:2561-2570. 82. Vallett M, Tabatabaie T, Briscoe RJ, Baird TJ, Beatty WW, Floyd RA, et al. Free radical production during ethanol intoxication, dependence, and withdrawal. Alcohol Clin Exp Res 1997;21:275285. 83. Montoliu C, Valles S, Renau-Piqueras J, Guerri C. Ethanol-induced oxygen radical formation and lipid peroxidation in rat brain: effect of chronic alcohol consumption. J Neurochem 1994;63:1855-1862. 84. Owens T. The enigma of multiple sclerosis: inflammation and neurodegeneration cause heterogeneous dysfunction and damage. Curr Opin Neurol 2003;16:259-265. 85. Syapin PJ, Militante JD, Garrett DK, Ren L. Cytokine-induced iNOS expression in C6 glial cells: transcriptional inhibition by ethanol. J Pharmacol Exp Ther 2001;298:744-752. 86. Wang JH, Sun GY. Ethanol inhibits cytokine-induced iNOS and sPLA2 in immortalized astrocytes: evidence for posttranscriptional site of ethanol action. J Biomed Sci 2001;8:126-133. 87. Naassila M, Roux F, Beauge F, Daoust M. Ethanol potentiates lipopolysaccharide- or interleukin-1 beta-induced nitric oxide generation in RBE4 cells. Eur J Pharmacol 1996;313:273-277. 88. Mori C, Natsuki R. [Effect of ethanol on expression of nitric oxide synthases in the cerebral culture cells from chick embryo]. Nippon Yakurigaku Zasshi 1996;107:197-203. 89. Dizon ML, Brown LA, Black SM. Brain nitric oxide synthase levels increase in response to antenatal ethanol exposure. Alcohol 2004;39:101-105. 90. Shih CL, Chi SI, Chiu TH, Sun GY, Lin TN. Ethanol effects on nitric oxide production in cerebral pial cultures. Alcohol Clin Exp Res 2001;25:612-618. 91. Knapp DJ, Crews FT. Induction of cyclooxygenase-2 in brain during acute and chronic ethanol treatment and ethanol withdrawal. Alcohol Clin Exp Res 1999;23:633-643. 92. Simonyi A, Woods D, Sun AY, Sun GY. Grape polyphenols inhibit chronic ethanol-induced COX-2 mRNA expression in rat brain. Alcohol Clin Exp Res 2002;26:352-357. 93. Luo J, Lindstrom CL, Donahue A, Miller MW. Differential effects of ethanol on the expression of cyclo-oxygenase in cultured cortical astrocytes and neurons. J Neurochem 2001;76:1354-1363. 94. Fubini B, Hubbard A. Reactive oxygen species (ROS) and reactive nitrogen species (RNS) generation by silica in inflammation and fibrosis. Free Radic Biol Med 2003;34:1507-1516. 95. Konstantinopoulos PA, Vandoros GP, Sotiropoulou-Bonikou G, Kominea A, Papavassiliou AG. NF-κB/PPARÁ and/or AP- A.M. BLANCO, C. GUERRI 1/PPARÁ 'on/off' switches and induction of CBP in colon adenocarcinomas: correlation with COX-2 expression. Int J Colorectal Dis 2006; Feb 25 (in press, available on line) 96. Hwang D, Jang BC, Yu G, Boudreau M. Expression of mitogeninducible cyclooxygenase induced by lipopolysaccharide: mediation through both mitogen-activated protein kinase and NF-κB signaling pathways in macrophages. Biochem Pharmacol 1997;54:87-96. 97. Chen JC, Ho FM, Pei-Dawn Lee C, Chen CP, Jeng KC, Hsu HB, et al. Inhibition of iNOS gene expression by quercetin is mediated by the inhibition of IκB kinase, nuclear factor-κ B and STAT1, and depends on heme oxygenase-1 induction in mouse BV-2 microglia. Eur J Pharmacol 2005;521:9-20. 98. Davis RL, Syapin PJ. Ethanol increases nuclear factor-κ B activity in human astroglial cells. Neurosci Lett 2004;371:128-132. 99. Wheeler MD, Kono H, Rusyn I, Arteel GE, McCarty D, Samulski RJ, et al. Chronic ethanol increases adeno-associated viral transgene expression in rat liver via oxidant and NFκB-dependent mechanisms. Hepatology 2000;32:1050-1059. 100.Ward RJ, Zhang Y, Crichton RR, Piret B, Piette J, de Witte P. Identification of the nuclear transcription factor NFκB in rat after in vivo ethanol administration. FEBS Lett 1996;389:119-122. 101.Mercurio F, Murray BW, Shevchenko A, Bennett BL, Young DB, Li JW, et al. IκB kinase (IKK)-associated protein 1, a common component of the heterogeneous IKK complex. Mol Cell Biol 1999;19:1526-1538. 102.Mercurio F, Zhu H, Murray BW, Shevchenko A, Bennett BL, Li J, et al. IKK-1 and IKK-2: cytokine-activated IκB kinases essential for NF-κB activation. Science 1997;278:860-866. 103.Griffin BD, Moynagh PN. Persistent interleukin-1‚ signaling causes long term activation of NFκB in a promoter-specific manner in human glial cells. J Biol Chem 2006;281:10316-10326. 104.Ling L, Cao Z, Goeddel DV. NF-κB-inducing kinase activates IKKα by phosphorylation of Ser-176. Proc Natl Acad Sci USA 1998;95:37923797. 105.Lee FS, Hagler J, Chen ZJ, Maniatis T. Activation of the IκB α kinase complex by MEKK1, a kinase of the JNK pathway. Cell 1997;88:213-222. 106.Nakano H, Shindo M, Sakon S, Nishinaka S, Mihara M, Yagita H, et al. Differential regulation of IκB kinase α and β by two upstream kinases, NF-κB-inducing kinase and mitogen-activated protein kinase/ERK kinase kinase-1. Proc Natl Acad Sci USA 1998;95:35373542. 107.Dong C, Davis RJ, Flavell RA. MAP kinases in the immune response. Annu Rev Immunol 2002;20:55-72. 108.Karin M. The regulation of AP-1 activity by mitogen-activated protein kinases. J Biol Chem 1995;270:16483-16486. 109.Ryabinin AE, Criado JR, Henriksen SJ, Bloom FE, Wilson MC. Differential sensitivity of c-Fos expression in hippocampus and other brain regions to moderate and low doses of alcohol. Mol Psychiatry 1997;2:32-43. 110.Beckmann AM, Matsumoto I, Wilce PA. AP-1 and Egr DNAbinding activities are increased in rat brain during ethanol withdrawal. J Neurochem 1997;69:306-314. 111.Beckmann AM, Matsumoto I, Wilce PA. Elevated AP-1 DNAbinding activity in rat brain during ethanol withdrawal. Alcohol Alcohol 1994;2 (suppl):223-227. 112.Walker DG, Lue LF. Investigations with cultured human microglia 199 Inmunol3/2006 copia 13/12/06 16:38 Página 200 ALCOHOL AND NEUROINFLAMMATION: INVOLVEMENT OF ASTROGLIAL CELLS AND IL-1RI/TLR4 RECEPTORS on pathogenic mechanisms of Alzheimer's disease and other neurodegenerative diseases. J Neurosci Res 2005;81:412-425. 113.Emerit J, Edeas M, Bricaire F. Neurodegenerative diseases and oxidative stress. Biomed Pharmacother 2004;58:39-46. 114.Takuma K, Baba A, Matsuda T. Astrocyte apoptosis: implications for neuroprotection. Prog Neurobiol 2004;72:111-127. 115.Wyss-Coray T, Mucke L. Inflammation in neurodegenerative disease--a double-edged sword. Neuron 2002;35:419-432. 116.Owens T, Babcock AA, Millward JM, Toft-Hansen H. Cytokine and chemokine inter-regulation in the inflamed or injured CNS. Brain Res Brain Res Rev 2005;48:178-184. 117.Tanga FY, Nutile-McMenemy N, DeLeo JA. The CNS role of Tolllike receptor 4 in innate neuroimmunity and painful neuropathy. Proc Natl Acad Sci USA 2005;102:5856-5861. 118.Marcolini J, Nguyen M, Ericsson C. Klebsiella pneumoniae brain abscess in a Taiwanese adult. J Infect 2002;44:205-210. 119.Aloisi F. Immune function of microglia. Glia 2001;36:165-179. 120.Mack CL, Vanderlugt-Castaneda CL, Neville KL, Miller SD. Microglia are activated to become competent antigen presenting and effector cells in the inflammatory environment of the Theiler's virus model of multiple sclerosis. J Neuroimmunol 2003;144:6879. 121.Bowman CC, Rasley A, Tranguch SL, Marriott I. Cultured astrocytes express toll-like receptors for bacterial products. Glia 2003;43:281291. 122.Esen N, Tanga FY, DeLeo JA, Kielian T. Toll-like receptor 2 (TLR2) mediates astrocyte activation in response to the Gram-positive bacterium Staphylococcus aureus. J Neurochem 2004;88:746-758. 123.Minagar A, Shapshak P, Fujimura R, Ownby R, Heyes M, Eisdorfer C. The role of macrophage/microglia and astrocytes in the pathogenesis of three neurologic disorders: HIV-associated dementia, Alzheimer disease, and multiple sclerosis. J Neurol Sci 2002;202:1323. 124.Carpentier PA, Begolka WS, Olson JK, Elhofy A, Karpus WJ, Miller SD. Differential activation of astrocytes by innate and adaptive immune stimuli. Glia 2005;49:360-374. 125.Wilflingseder D, Mullauer B, Schramek H, Banki Z, Pruenster M, Dierich MP, et al. HIV-1-induced migration of monocyte-derived dendritic cells is associated with differential activation of MAPK pathways. J Immunol 2004;173:7497-7505. 126.Wu D, Marko M, Claycombe K, Paulson KE, Meydani SN. Ceramideinduced and age-associated increase in macrophage COX-2 expression is mediated through up-regulation of NF-κ B activity. J Biol Chem 2003;278:10983-10992. 200 VOL. 25 NUM. 3/ 2006 127.Buss H, Dorrie A, Schmitz ML, Hoffmann E, Resch K, Kracht M. Constitutive and interleukin-1-inducible phosphorylation of p65 NF-κB at serine 536 is mediated by multiple protein kinases including IκB kinase (IKK)- α, IKKβ, IKKε, TRAF family memberassociated (TANK)-binding kinase 1 (TBK1), and an unknown kinase and couples p65 to TATA-binding protein-associated factor II31-mediated interleukin-8 transcription. J Biol Chem 2004;279:5563355643. 128.Jiang Z, Johnson HJ, Nie H, Qin J, Bird TA, Li X. Pellino 1 is required for interleukin-1 (IL-1)-mediated signaling through its interaction with the IL-1 receptor-associated kinase 4 (IRAK4)-IRAK-tumor necrosis factor receptor-associated factor 6 (TRAF6) complex. J Biol Chem 2003;278:10952-10956. 129.Peoples RW, Li C, Weight FF. Lipid vs protein theories of alcohol action in the nervous system. Annu Rev Pharmacol Toxicol 1996;36:185201. 130.Pike LJ. Lipid rafts: bringing order to chaos. J Lipid Res 2003;44:655667. 131.Simons K, Toomre D. Lipid rafts and signal transduction. Nat Rev Mol Cell Biol 2000;1:31-39. 132.Triantafilou M, Miyake K, Golenbock DT, Triantafilou K. Mediators of innate immune recognition of bacteria concentrate in lipid rafts and facilitate lipopolysaccharide-induced cell activation. J Cell Sci 2002;115:2603-2611. 133.Triantafilou M, Morath S, Mackie A, Hartung T, Triantafilou K. Lateral diffusion of Toll-like receptors reveals that they are transiently confined within lipid rafts on the plasma membrane. J Cell Sci 2004;117:4007-4014. 134.Triantafilou M, Triantafilou K. The dynamics of LPS recognition: complex orchestration of multiple receptors. J Endotoxin Res 2005; 11:5-11. 135.Olsson S, Sundler R. The role of lipid rafts in LPS-induced signaling in a macrophage cell line. Mol Immunol 2006;43:607-612. 136.Dolganiuc A, Bakis G, Kodys K, Mandrekar P, Szabo G. Acute ethanol treatment modulates Toll-like receptor-4 association with lipid rafts. Alcohol Clin Exp Res 2006;30:76-85. 137.Syapin PJ. Alcohol and nitric oxide production by cells of the brain. Alcohol 1998;16:159-165. 138.Vinson RB, Carroll JL, Pruett SB. Mechanism of suppressed neutrophil mobilization in a mouse model for binge drinking: role of glucocorticoids. Am J Physiol 1998;275:R1049-1057. 139.Boe DM, Nelson S, Zhang P, Bagby GJ. Acute ethanol intoxication suppresses lung chemokine production following infection with Streptococcus pneumoniae. J Infect Dis 2001;184:1134-1142.