Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pathogenomics wikipedia , lookup
Copy-number variation wikipedia , lookup
Human genetic variation wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Minimal genome wikipedia , lookup
Ridge (biology) wikipedia , lookup
Oncogenomics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Genetic engineering wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Public health genomics wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Point mutation wikipedia , lookup
History of genetic engineering wikipedia , lookup
Gene nomenclature wikipedia , lookup
Helitron (biology) wikipedia , lookup
Gene desert wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Gene therapy wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Genome evolution wikipedia , lookup
Gene expression programming wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Gene expression profiling wikipedia , lookup
Genome (book) wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
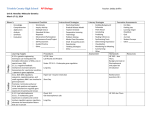
Gw&mscular Research ELSEVIER CardiovascularResearch31(19%) 8704372 Cardiovascular Mystery Series Series Editor: Karl T. Weber Mini-review Glucocorticoid-remediable aldosteronism Robert G. Dluhy, Gordon H. Williams * Department of Medicine, Harvard Medical School and Brigham and Women’s Hospital, Boston, MA, USA Received 9 August 1995;accepted 12March 1996 Keywords: Glucocorticoid remediable aldosteronism 1. Introduction 2. Discussion GRA has been known since 1966 to be a form of mineralocorticoid hypertension characterized by reversal of the mineralocorticoid-excess state by the exogenous administration of a glucocorticoid, such as dexamethasone [ 1,2]. GRA was subsequently shown to be inherited in an autosomal fashion, establishing the genetic basis for this disorder. Clinically, the age of onset of hypertension in GRA patients is in the first two decades of life. This * Correspondingauthor. Elsevier Science B.V. PII SOOOS-6363(96)00069-7 Downloaded from by guest on October 24, 2016 Blood pressure is known to be influenced by heritable and environmental factors. The genetic contribution is complex since multiple genes are known to participate in the regulation of blood pressure. Once blood pressure is elevated, structural change also ensues, although the degree of vascular remodeling probably relates to hormonal and genetic differences. Thus, an attempt to discover ‘hypertensive genes’ or mutations in genes that maintain normotensionmight be ‘misguided’ owing to the multiplicity of factors that regulate blood pressure. However, the genetic basis of a hypertensive disorder has recently been reported, indicating that the discovery of additional mutations in genesthat regulate blood pressurewill be likely in the future. This disorder - glucocorticoid-remediable aldosteronism(GRA) - illustrates that one successfulstrategy to identify ‘ hypertensive genes’ is to subdivide the hypertensive syndromeinto intermediatephenotypes.These phenotypescan then be scrutinized by searching for mutations in candidategenesthat relate to the specific hypertensive phenotypes. contrastssharply with that of subjectswith other causesof primary aldosteronism who are usually diagnosed during the fourth and fifth decadesof life [3]. In contrast to other etiologies of primary aldosteronism, many patients with GRA are not hypokalemic and, thus, a potassium level lacks sensitivity as a screening test for this disorder. GRA had been reported worldwide, but is more common in individuals of Scottish and Irish ancestry; no caseshave yet been reported in Blacks. In GRA aldosterone secretion is positively and solely regulated by adrenocorticotropic hormone CACTI-I) [4,5]. As a consequence,exogenous glucocorticoid administration profoundly suppressesaldosterone secretion in affected subjects. In addition, the exogenous administration of ACTH is associatedwith an exuberant and prolonged increase in aldosterone secretion and blood pressure in such subjects. In contrast, in normal individuals ACTH administration is associated with a rise and subsequent decline in aldosteronelevels to basal over several days. As in other etiologies of primary aldosteronism,plasma renin levels are suppressedin GRA subjects.However, parameters of aldosterone production often overlap the normal range, consistent with one hypothesis that other unmeasured mineralocorticoids contribute to this mineralocorticoid-excess state. However, it should be recalled that aldosteronesecretion in GRA is solely regulatedby ACTH. Thus, there is dysregulation of mineralocorticoid secretion, since aldosterone does not have a feedback-suppressive effect on the pituitary production of ACTH. Two abnormal steroids - 18-hpdroxycortisol (l&OHF) and 18-oxocortisol (18-OXOF) - were found by Ulick and others to be greatly overproduced in the urine in affected GRA subjects [6,7]. Like aldosterone, these 18oxygenated cortisol compounds were found to be positively regulated by ACTH. Moreover, these compounds R.G. Dluhy, G.H. Williams/Cardiovascular Al&s&one synthase 11-0Hase -3 Unequal crossing over 5 Aldosterone synthase Chimaeric gene 11-0Hase Fig. 1. The chimeric gene duplication in GRA, a result of unequal crossing-overbetween the homologous 11/Shydroxylase and aldosterone synthase genes. The chimera fuses the S-regulatory sequencesof the 11r3-hydroxylase gene and the 3’-coding sequencesof the aldosterone synthasegene. From Lifton et al. [14] by permission. QRA Patlent Pituitary v ACTH j cortLsol Mineralocorticoids j JAngiotensin z II f Na I Adrenal Fig. 2. The chimeric gene results in ectopic expression of aldosterone synthaseactivity in the cortisol-producing zona fasciculata (F) under the regulation of adrenocorticotropinCACTI-f).This results in overproduction of aldosterone and other mineralocorticoids (including 18-oxygenated cortisol compounds),which leads to suppressionof the renht-angiotensin system and atrophy of the zona glomerulosa (G). fusing sequencesof the 11P-hydroxylase and aldosterone synthase genes [14] (Fig. 1). This gene duplication was shown to contain the 5’ regulatory sequences,confirming ACTH responsivenessof llP-hydroxylase, fused to more distal coding sequencesof aldosteronesynthase.Given the homologies of the 11Phydroxylase and aldosterone synthasegenes,the mechanismthat would likely createsuch a gene duplication would be a recombination event, an unequal crossing-over between these two genes. This gene duplication appears to explain all of the known physiology and biochemistry previously reported in GRA. First, the promoter region of this chime& gene contains regulatory sequences of 11/3-hydroxylase and would be expected to be regulated by ACTH. In addition, this chimeric gene would allow ectopic expression of aldosteronesynthaseand enzymatic activity in the ACTHregulated zona fasciculata which normally only secretes cortisol (Fig. 2). Thus, the presenceof this gene duplication in the zona fasciculata would also explain the production of the C-18 oxygenated cortisol compounds. Finally, the sole regulation of aldosterone secretion by ACTH and the suppressionof aldosteronesecretionby glucocorticoids is explained by this gene mutation, since the aldosterone synthase,geneis abnormally regulated by ACTH promoter sequences. In an additional study in 11 unrelated GRA pedigrees, all affected subjectshad chimeric gene duplications arising from unequal crossing-over [ 151.Chimeric geneswere also found in a second study of 4 additional patients from unrelated pedigrees [16]. In both studies, the sites of crossing-over were variable, indicating that in different pedigreesthese gene duplications arose independently and Downloaded from by guest on October 24, 2016 were shown to provide a specific means of diagnosis. Although they are also modestly overproduced in patients with aldosterone-producing adenomas (but not bilateral idiopathic hyperplasia), the ratio of these compounds to aldosterone rarely exceeds one. In GRA, these 18oxygenated cortisol compounds are greatly overproduced both in an absolute sense and in relationship to aldosterone, with a ratio that invariably exceeds two. These abnormal steroids are hybrid compounds since they share structural featuresof both the aldosteroneand cortisol-producing zones of the adrenal cortex. Specifically, they are hydroxylated at carbons 17 and 18, featuresof zona fasciculata and zona glomerulosa steroids, respectively. Although it was felt originally that these compounds may contribute to the mineralocorticoid-excessstate in evidence in GRA, they have been found in rodents to have only weak mineralocorticoid activity [8]. However, it is possible that these hybrid compounds possesssignificant mineralocorticoid activity in humans. The molecular basis of GRA was discovered by applying a candidategene approachin a pedigree where affected and unaffected subjects were identified using as the specific biochemical phenotypethesehybrid compounds.Thus, 18-OHF and TH 18-OXOF were measuredin the urine of individuals in three living generations in a large GRA pedigree where a proband had been diagnosed [9]. Of 18 at-risk individuals, GRA was diagnosed in 11 additional patients. A candidate gene approach was then taken with the hypothesis that a mutation in the aldosterone gene could explain GRA. A gene expressing aldosterone synthase activity was known to be closely related to a second gene involved in adrenal steroidogenesis,steroid 11P-hydroxylase [lo-131. Both genes are 95% identical in DNA sequenceand have identical intron-exon structures. Both genes are located in close proximity on chromosome 8. Genetic markers were developed to the aldosterone synthase gene and segregationof these markers was compared with segregationof GRA in the pedigree described. What was found in affected subjects, but not their affected relatives, was an extra gene - a hybrid or chime& gene 871 Research 31 (1996) 870472 872 R.G. Dluhy, G.H. Williams/Cardiovascular 3. Conclusion The genetic basis for one hypertensive syndrome has been discovered using a strategy that could be extended to essential hypertension. That is, hype’rtensive intermediate phenotypes can be developed using physiologic markers, such as non-modulation or insulin resistance. Heritability of such intermediate phenotypes could then be demon- strated by pedigree screening (as in GRA) or in sib pair studies. Then a directed search of the genome could be performed for mutations, using candidate genes appropriate for each phenotype. Such a search for these gene mutations would only appear to be ‘misguided’ if the efforts were random, and not directed, as illustrated by the strategy used in the case of GRA. References [l] SutherlandDJ, Ruse JL, Laidlaw JC. Hypertension, increasedaldosterone secretion and low plasma renin activity relieved by dexamethasone.Can Med Assoc J 1%6;95:1109-l 119. [2] New MI, PetersonRE. A new form of congenital adrenal hyperplasia. J Clin Endocrinol Metab 1%7;27:300-305. [3] Bravo E, Tarazi R, Dustan H et al. The changing clinical spectrum of primary aldosteronism.Am J Med 1983;74:641-651. [4] Gill JR, Barter FC. Overproduction of sodium-retaining steroids by the zona glomemlosa is adrenocorticotropindependentand mediate hypertension in dexamethasone-suppressiblealdosteronism. J Clin Endocrinol Metab 1981;53:331-337. [51 Obertield SE, Levine LS, Stoner E et al. Adrenal glomendosa function in patients with dexamethasone-suppressiblehyperaldosteronism. J Clin Endocrinol Metab 1981;53:158-164. [6] Ulick S, Chu MD, Land MI. Biosynthesis of I&oxocortisol by aldosterone-producingadrenal tissue. 1983; J Biol Chem 258:54985502. [7] Gomez-SanchezCE, Montgomery M, Ganguly A et al. Elevated urinary excretion of 18-oxocortisol in glucocorticoid-suppressible aldosteronism.J Clin Endocrinol Metab 1984;59:1022-1024. [8] Gomez-SanchezCE, Gomez-SanchezEP, Smith JS et al. Receptor binding and biological activity of ll-oxocortisol. Endocrinology 1985;116:6-10. [9] Rich GM, Ulick S, Cook S et al. Glucocorticoid-remediable aldosteronism in a large kindred: clinical spectrum and diagnosis using a characteristic biochemical phenotype. Ann Intern Med 1992;116:813-820. [ 101 Chua SC, SzaboP, Vitek A et al. Cloning of cDNA encoding steroid 11-hydroxylase (P-450,,,). Pmc Nat1 Acad Sci USA 1987; 84:7193-7197. [ 11I Kawamoto T, Mitsuuchi Y, Ckhnishi T et al. Cloning and expression of a cDNA for human cytochrome P-450,, as related to primary aldosteronism.Bicchem Biophys Res Commun 1990,173:309-316. 1121Momet E, Dupont B, Vitek A et al. Characterization of two genes encoding human steroid 1I-hydroxylase (P-450,,). J Biol Chem 1989;264:20%1-20967. [13] Ogishima T, Shibata H, Shimada H et al. Aldosterone synthase cytochromeP-450 expressedin the adrenalsof patients with primary aldosteronism.J Biol Cbem 1991;266:10731-10734. 1141Lifton RP, Dluhy RG, Powers M et al. A chimeric llhydroxylase/aldosterone synthase gene causes glucocorticoid-remediable aldosteronism and human hypertension. Nature 1992;355:262-265. [15] Lifton RP, Dluhy RG, Powers M et al. Hereditary hypertension caused by chimeric gene duplications and ectopic expression of aldosteronesynthase.Nature Genet 1992266-74. [161 PascoeL, Cumow KM, Slutsker L et al. Glucocorticoid-suppressible hyperaldosteronism results from hybrid genes created by unequal crossoversbetween CYPllBl and CYPllB2. Proc Natl Acad Sci USA 1992;89:8327-8331. Downloaded from by guest on October 24, 2016 did not descend from a single ancestral mutation. However, in all studies, the sites of crossing-over were upstream of exon 5 of aldosterone synthase, suggesting that encoded amino acids in exon 5 are essential for aldosterone synthase enzymatic functions. This hypothesis is strengthened by the construction of chimeric genes and expression of aldosterone synthase enzymatic activity in vitro [16]. In this study, aldosterone synthase enzymatic activity was retained, provided that the site of fusion between 11-hydroxylase and aldosterone synthase genes was upstream of exon 5 of aldosteronesynthase. As a result of these studies, direct genetic screeningfor GRA is now possible. Moreover, the presenceof the gene duplication appears to be 100% sensitive and specific for diagnosing GRA and is concordant with the measurement of the abnormal steroids, TH 18-OXOF, and 18-OHF. It is recommendedthat patients with aldosteronism without radiographic evidence of tumors, as well as individuals with suppressedlevels of PRA (especially children and young adults) should be screenedfor GRA. Moreover, since this is an autosomal dominant disorder, extended screening of at-risk individuals in affected families will yield many additional cases. Treatment of this disorder is gratifying since therapy is directed. Traditionally, the suppression with glucocorticoids has been the preferred treatment. However, many subjects appear to have been overtreated with excessive glucocorticoid dosing, resulting in Cushing’s syndrome. It is urged that if this modality of treatment is used, the lowest dose of a shorter-acting glucosteroid be used and patients monitored carefully for signs of glucocorticoid excess. Alternative treatments include the aldosterone antagonist, spironolactone, and amiloride, an agent which inhibits sodium reabsorption by the renal epithelial sodium channel. Long-term treatment in males with spironolactone is usually deemedunsatisfactory becauseof the antiandrogenie effects of this drug which causegynecomastia,impotency, or both. Potassium-wasting diuretics can be used cautiously, but they may precipitate profound hypokalemia. They are probably best used in combination with potassium-sparing diuretics, with potassium levels being carefully monitored. Research 31 (19%) 870-872