Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neuroanatomy wikipedia , lookup
Subventricular zone wikipedia , lookup
Neuroregeneration wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Development of the nervous system wikipedia , lookup
Proprioception wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Perception of infrasound wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Circumventricular organs wikipedia , lookup
Synaptogenesis wikipedia , lookup
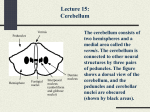
Neuroanatomy بسم هللا الرحمن الرحيم الكثير من الطالب يعاني مع كيفية مذاكرة مادة النيرواناتومي ,قررت بأذن هللا ,تفريغ ما يقوله البروف لطفي ,كون أحد طالب الدفعات السابقة أكد لي أن كل ما يسأل عنه البروف لطفي في االختبارات هو من صميم كالمه . نتمنا اننا نقدر نفيدكم بهذا العمل ,أعذرونا أذا أخطأت في أي معلومة . العمل راح يكون على شكل باوربوينت حتى يسهل ألي أحد تصحيح خطأ لو وجد ,أو أضافة معلومة من عنده ,العمل عبارة عن شرح ساليدات الدكتور لطفي كونها مو كافية . حقوق الطبع غير محفوظة ,ويحق لكل طالب أن يعتبر الساليدات حقته يعمل بها ما يريد أخوانكم :عدنان توفيق اليوسف و علي غالب الهاشم 1- CEREBELLLUM 1st and 2nd lectures Introduction The cerebellum plays a very important role in the control of posture and voluntary movement . It unconsciously influence the smooth contraction of voluntary muscle and carefully coordinates their action ,together with the relaxation of their antagonists. The cerebellum is situated in the posterior cranial fossa and is covered superiorly by the tentorium cerebelli. It is the largest part of the hindbrain and lies posterior to the 4th ventricle , the pons , and the medulla oblongata . It consist of two cerebellar hemispheres joined by narrow median Vermis . The cerebellum is connected to the posterior aspect of the brain stem by 3 symmetrical bundles of nerve fibers called : superior , middle , and inferior cerebellar peduncles . The cerebellum is divided into 3 main lobes : anterior lobe , the middle lobe , and the flocculonodular lobe . From prof. Lutfi slides From prof. Lutfi slides From prof. Lutfi slides Con… The cerebellum plays a very important role in the control of posture and voluntary movement . It unconsciously influence the smooth contraction of voluntary muscle and carefully coordinates their action ,together with the relaxation of their antagonists. Each cerebellar hemisphere controls muscular movement on the same side of the body and that the cerebellum has no direct pathway to the lower motor neurons but exerts its control via the cerebral cortex and brain stem. Function of Cerebellum The function of cerebellum is to maintain muscle tone . Note that “when we mention muscle tone we must mention the posture” Also have an important role in equilibrium and balance . Maintain Posture Sequential Movement Muscle tone Cerebellum Balance Equilibrium What does the cerebellum consist of ? The cerebellum consist of 2 cerebellar hemisphere connected to each others by VERMIS. The cerebellum connect to the brainstem by 3 bundles of nerve fibers :1-superior c. peduncle : connect it to Midbrain 2-middle c. peduncle : connect it to Pons 3-inferior c. peduncle : connect it to Medulla oblongata . The cerebellum was divided into :- lobs and fissure . Cerebellum has 3 lobs : 1-anterior lobe 2-posterior lobe “middle,largest” 3-flocculonodular lobe And the fissures are : 1-primary “separates anterior from posterior” 2-uvulonodular “separates posterior from flocculonodular” From prof. Lutfi slides From prof. Lutfi slides Con… *Flocculonodular lobe : receive incoming vistibular fiber . *There is connection between the flocculonodular lobe and vestibular nuclei *in cerebellum , the gray matter is on the surface , and the white matter is inside , “opposite to brain and spinal cord” , of course the inner white matter is not pure due to presence of INTRACEREBELLUM NEUCLEI . Cerebellar cortex *there are 3 layers of the outer cortex :1-molecular layer 2-purkinje layer 3-granular layer *The parkinje cell is type 1 golgi cell *the dendrite of the purkinje layer is going out to the molecular layer . I. Cerebellar cortex Cerebellar Gray matter Molecular Purkinje Granular layer layer layer Basket cells Stellate cells From prof. Lutfi slides Granule cells Golgi cells From prof. Lutfi slides Con… The molecular layer has 2 types of cells :1-basket cells 2-stellate cells These cells synapse with the dendrite of the purkinje cell . The purkinje cell’s axon go out form cortex , “the only efferent fibers that leave the cerebellar cortex are the axons of purkinje cell” > they go to INTRACELLEBLAR NUCLEI . Note : not all of the purkinje cell axon are going to Intracelleblar but few of them, specially from the Flocculonodular lobe are going directly to the vestibular nuclei . * The granular cell layer has 2 types of small cells :1-granular cells 2-golgi cells Con… Granular cell has very little cytoplasm and very dens nuclei , they are small with very tall dendrites reach the molecular layer. The dendrites of the granular cell synapse with purkinje cells. Golgi cells are larger than granular cells . There are 2 type of afferent fiber that reach the cerebellar cortex :1-climbing fiber 2-mossyl fiber Climbing fiber : They go to the molecular layer and synapse with parkinje cells Note: each parkinje cell synapse with ONE climbing fiber ,but one climbing fiber may synapse with up to 10 parkinje cells . The climbing fibers are coming from olivary nuclei . Con… Mossy fiber : They originate from the anterior and posterior spinocerebellur tract , vistibulocerebellar , reticilocerebellar , cuneocerebellar , etc. And they end by synapses with the granular dendrites . # the mossy and climbing fibers have stimulatory effect on the purkinje cell but the axon of the purkinje cell to the intracerebellar nuclei are inhibatory , and this inhibtion effect is due to neurons found in the cerebellar cortex that synapse with purkinje cell such as golgi cell , basket , stellate and granular. The affect of them on the purkinje cell are inhibitory and the result is that the axon of the purkinje cell is inhibitory . Note: the affarent fiber “ mossy and climbing” before they enter the cerebellar cortex they give collateral fibers to the intracerebellar nuclei. Con... There are no direct fibers from the cerebellum to the spinal cord , they deal with other brain structure to mediates its function such as : red nucleus , reticular formation , thalamus and vestibular nuclei. II. Intracerebellar nuclei Fastigial Globose Emboliform Dentate nucleus nucleus nucleus nucleus From prof. Lutfi slides From prof. Lutfi slides Location of intracerebellar nuclei Vermis & flocculonodular lobe Fastigeal nucleus Paravermal zone of the hemispheres Globose & Emboliform nuclei Lateral zone of the hemispheres Dentate nucleus From prof. Lutfi slides Afferent & efferent fibers of the cerebellum In cerebellum the are nerve fiber which enter the cerebellum , and the other go out from it . The fibers which enter the cerebellum called AFFERENT FIBERS , and these fibers are come from SPINAL CORD , VESTIBULAR NERVE , VESTIBULAR NUCLEI, AND CEREBRAL CORTEX . The fibers which go out from the cerebellum called EFFERENT FIBERS , this fibers go to the RED NUCLEUS , VESTIBULAR NUCLEI , THALAMUS , AMD RETECULAR FORMATION . WE WILL MENTION THESE PATHWAY IN THE NEXT SLIDES Functions of the cerebellum 1-Maintaining balance & equilibrium Lateral vestibular nuclei & RF Vestibulocerebellum (flocculonodular lobe) Vestibular nerve From prof. Lutfi slides CON.. By the vestibular nerve , the cerebellum maintain the balance and equilibrium , the ganglion of the vestibular nerve are located in the internal acoustic meatus , its peripheral fibers come from semicircular canal , sacule and utricle . MOST of the fibers end in the vestibular nuclei , BUT SOME OF THEM GO DIRECT TO THE CEREBELLUM FROM THE INFERIOR CEREBELLAR PEDUNCLE. There are fibers go from cerebellum ‘ efferent fibers from fastigeal nucleus’ to the vestibular nuclei and retecular formation . Functions of the cerebellum 2-Control of muscle tone & coordination of muscular activity (unconscious proprioception) Vestibular nuclei Reticular formation Red nucleus Thalamus Spinocerebellum (Vermis & paravermal zone) Spinal cord From prof. Lutfi slides CON.. قوم سوي لك كوب شاي و تعال كمل مذاكرة In this pathways “ from spinal cord to the cerebellum “ we have the fibers which reach the cerebellar cortex : CLIMBING FIBERS AND MOSSY FIBERS . 1- CLIMBING Only one pathway as we saied before spino-olivary-cerebro-olivary cerebellar tract . They collect in inferior olivary nuclei and then enter the cerebellum via INFERIOR CEREBELLAR PEDUNCLE . The give collateral branch to the intracerebellar nuclei before go to the cerebellar cortex . Con.. 2- MOSSY The other pathway : A- anterior spinocerebellar tract Its axon enter the spinal cord from muscle spindle ,tendon and joint receptor and synapse with NUCLEUS DORSALIS ‘ CLARKEKS NUCLEI’ , MOST OF AXONS CROSS TO THE OPPOSITE SIDE .this fibers enter the cerebellum via SUPERIOR CREBELLAR PEDUNCLE as mossy fibers in cerebellar cortex . It gives collateral branch to the intracerebellar nuclei . It is belived that those fibers cross back within the cerebellum . B- posterior spinocerebellar tract : Same as anterior , but these fibers go direct to the cerebellum ‘ do not cross and cross back ‘ and they enter via inferior cerebellar peduncle. C-cuneocerebellar NOTE: all the fibers that mention before come from C8 BELOW TO L3 spinal segment EXCEPT THIS PATHWAY which come from above C8 segment. Con... These fibers collected in Cuneatus nucleus , and enter the cerebellum via inferior cerebral peduncle . From prof. Lutfi slides Functions of the cerebellum 3-Monitoring of sequential motor activity Thalamus (VL nucleus) Cerebral cortex Pontine nuclei Inferior olivary nucleus & reticular formation Pontocerebellum (Lateral zone) From prof. Lutfi slides From prof. Lutfi slides Afferent Input Climbing fibers Mossy fibers • Olivocerebellar fibers • All other afferents From prof. Lutfi slides From prof. Lutfi slides Cerebellar efferent fibers From prof. Lutfi slides Cerebellar peduncles SCP • mainly efferent: • Cerebellothala mic & cerebellorubral fibers • Some afferents: ventral spinocerebellar tract & tectospinal MCP • Only afferent: Pontocerebell ar fibers ICP • mainly afferent: OSCV • Some efferent to vestibular nuclei & reticular formation From prof. Lutfi slides Summary of cerebellar connections Output Spinal cord Vestibular nerve Cerebral cortex Proprioceptive information from muscles & joints Information about location & movement of head in space Plans of motor activity Cerebellum Thalamus (VL) brainstem Efferent Red nucleus Vestibular nuclei Reticular formation Afferent Input From prof. Lutfi slides Blood supply Three cerebellar • arteries: Superior cerebellar .1 artery Anterior inferior .2 cerebellar artery (AICA) Posterior inferior .3 cerebellar artery (PICA) From prof. Lutfi slides Blood supply (cont.) Venous drainage: • into adjacent venous dural sinuses From prof. Lutfi slides Clinical case A 56-year-old woman was examined by a neurologist and was found to have the following signs: Irregular swaying gait • Diminished tone of the muscles of • her right upper & lower limbs Right sided tremor • Difficulty in performing finger-to- • nose test using her right hand CT brain revealed a right-sided cerebellar tumor So its main function is: Control of muscle tone & coordination of voluntary movement From prof. Lutfi slides Analysis of the clinical case 1- Irregular swaying gait : بحيث ان المريض يسير مع انحراف او ميالن الى الجهة المصابة, يكون هنالك خلل في طريقة المشي “hypotonia” >>(lose of muscle tone and posture ) 2- Diminished tone of the muscle of the right upper and lower limps: In normal the muscle tone must be resilience and firmness but if the muscle lose it’s tone , it’ll be like dough . Now , how do we test for muscle tone : A- suppose that , the patient has right side lesion , passively flex and extend his arm or his leg , and then compare it to the opposite side , then you will notice that the side which has a lesion will show no resistance , no firmness or resilience . 3- right side tremor : Due to lack of coordination in action of antagonist muscle , for example : if I flex my elbow , the Biceps muscle contract and the triceps muscle relax , but if there is no coordination , triceps muscle wont accept to relax , and then both muscle will contract !!! Leading to tremor . There are many causes of tremor : A- parkinsonism B- thyrotoxicosis C- cerebellar lesion * How can we differentiate between them ? A-In parkinsonism : if the patient is calm , there will be tremor but when he/she wants to perform an action , the tremor will go away , also in sleep there is no tremor . B- thyrotoxicosis : ask the patient to put his/her hands straight , and put up to them a paper then you will see the both hands are shaking . C- cerebellar lesion : it’s hidden , Ie . At rest the patient doesn’t show an obvious tremor , but if he/she try to do something it becomes exaggerated . One way to testing it , is to ask the patient to touch his/her nose by the lesioned side of his/her body . If you ask hem to do it by the non-lesioned side “hand” he/she will smoothly touch his/her nose ,but by the lesioned side , when he/she become close to his/her nose will notice that his hand will go faraway from his nose , or touch it with roughness . So, this type of tremor called intention tremor . 4- Difficulty in performing finger to nose test using her right hand due to DYSDIADOCHKINESIA Another symptoms may present “ not related to our clinical case “ *Also in the cerebellar lesion , due to loss of coordination the patient will suffer from NYSTAGMUS, lack of coordination between median and lateral rectus , also , the patient will show difficulty in speaking”DYSARTHRIA” due to lack of coordination of Laryngeal muscle , tongue muscle and palatal muscle . The speech feature of the patient will be prolong , discontinuous and finally explosive all these symptoms are due to ATAXIA . *the patient head is often rotated and flexed , and the shoulder on the side of the lesion is lower than the normal side . *the patient also assumes a wide base when he/she stands and often stiff legged to compensate lose of muscle tone . *also the patient will show DYSDIADOCHKINESIA which is inability to performe alterative movement regularly and rapidly . “in book P:244” Lesions of the cerebellum Congenital agenesis or hypoplasia • Acute alcohol poisoning • Trauma • Infection (meningitis, encephalitis) • Vascular disorders • Tumors (medulloblastoma, meningioma, glioma) • Multiple sclerosis • From prof. Lutfi slides Signs & symptoms of cerebellar lesions Loss of muscle tone Remember! These occur on the ipsilateral side of the body Incoordination of voluntary muscular activity (ataxia) From prof. Lutfi slides Hypotonia Postural changes Abnormal gait Intention tremor Decomposition of movement Dysdiadochokinesia Pendular knee jerk Nystagmus dysarthria The specific deficits that result depend on which functional component of the cerebellum is most affected: lesions of the vestibulocerebellum affect posture • & balance Lesions of the spinocerebellum (vermis syndrome) • truncal ataxia Lesions of the pontocerebellum (cerebellar • hemisphere syndrome) inappropriate control of sequential motor movements From prof. Lutfi slides Summary Cerebellum is controlled by contralateral cerebral • hemisphere Cerebellum controls the ipsilateral half of the • body Cerebellar lesions do not lead to paralysis but • produce motor dyskinesia (ataxia) Cerebellar lesion produces hypotonia but no • atrophy Cerebellar lesion does not produce loss of • sensation From prof. Lutfi slides Summary (cont.) Acute lesion produces sudden symptoms • Chronic lesion can be compensated by other • parts of CNS Cerebellum has no direct neuronal connection to • LMNs Cerebellum does not control the smooth muscles • Cerebellum cannot initiate voluntary movement • Wish you all best From prof. Lutfi slides Nice information not related to the cerebellum 1- if an old person complain from epigastric pain you should first think about HEART PROBLOMES. 2- If a young person complain from heart pain you should think first about EPIGASTRIC PROBLEMS. 3-Any patient have COMA should this occur due to these causes : You can remember them from the VOWEL letters A: Alcoholism or Apoplexy E: Encephalitis or Epilepsy I: Infection or Insulinism O: Opiate ‘ drugs’ U: Uremia ‘ due to kidney failure’