Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Apical dendrite wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Subventricular zone wikipedia , lookup
Axon guidance wikipedia , lookup
Development of the nervous system wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Channelrhodopsin wikipedia , lookup
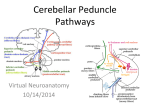
Cell Bio 10- Cerebellum Cerebellum has no direct connections to lower motor neurons Cerebellar lesions result in a characteristic type of irregular uncoordinated movement, ataxia Lesions can be localized easily: 1. Ataxia is ipsilateral to the side of a cerebellar lesion 2. Midline lesions of the cerebellar vermis or flocculonodular lobes mainly cause unsteady gait (truncal ataxia) and eye movement abnormalities 3. Lesions lateral to the cerebellar vermis mainly cause ataxia of the limbs (appendicular ataxia) Deep Cerebellar Nuclei Dentate nuclei: receive projections from the lateral cerebellar hemispheres (active just before voluntary movements) Emboliform & globose nuclei: receive inputs from the intermediate part (active during and in relation to the movement) Fastigial nuclei: receive inputs from the vermis Cell Bio 10- Cerebellum Cerebellar Input and Output pathways INPUT-1: Mossy fibers, ascend through the cerebellar white matter and form excitatory synapses on granule cells Granule cells’ axons form parallel fibers, each of these fibers form excitatory synapses with numerous Purkinje Cells. All output from the cerebellar cortex is carried by the axons of Purkinje cells Purkinje cells form inhibitory synapses onto deep cerebellar nuclei and vestibular nuclei INPUT-2: Climbing fibers arise from neurons in the contralateral inferior olivary nucleus. They wrap around the cell body and proximal dendritic tree of Purkinje cells, forming powerful excitatory synapses A single climbing fiber will branch to supply about 10 Purkinje cells; however each Purkinje cell is excited by just one climbing fiber Cell Layers of Cerebellar Cortex Mossy fibers excite granule cells, which excite the inhibitory Purkinje cells. Climbing fibers excite Purkinje cells directly Purkinje cells have fanlike dendritic trees, parallel fibers pass through these, then basket cell axons pass perpendicular to the parallel fibers All axons projecting upward are excitatory All axons projecting downward are inhibitory The outputs of the deep cerebellar nuclei are excitatory Cell Bio 10- Cerebellum Outputs from the lateral cerebellar hemisphere (below) via the dentate nucleus (involved in motor planning) Output from the intermediate cerebellar hemisphere (above) (involved in the control of ongoing movements of distal extrem. Output from the cerebellar vermis and flocculunodular lobe (below) (vermis: proximal trunk movement; flocculonodular: vestibule-ocular control) Cell Bio 10- Cerebellum Somatotopic Organization of Multimodal Inputs to the Cerebellum Noradrenergic inputs from the locus coeruleus and serotonergic inputs from the raphe nuclei project diffusely throughout the cerebellar cortex o These inputs play a neuromodulatory role Finger-Nose-Finger Test In ataxia, the movements have an irregular, wavering course that seems to consist of continuous overshooting, overcorrecting, and then overshooting again around the intended trajectory Appendicular ataxia: Coordinated actions of agonist and antagonist muscles acting on multiple joints, including the shoulder, elbow, and wrist, are required to smoothly perform this movement in a normal fashion Truncal Ataxia: Lesions confined to the cerebellar vermis affect primarily the medial motor systems. Patients with such lesions therefore often have a wide-based, unsteady “drunklike” gait Appendicular ataxia: Lesions of the intermediate and lateral portions of the cerebellar hemisphere affect the lateral motor systems. Therefore, these patients have ataxia on movement of the extremities