Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychoneuroimmunology wikipedia , lookup
Nervous system network models wikipedia , lookup
Haemodynamic response wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Multielectrode array wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Axon guidance wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Metastability in the brain wikipedia , lookup
Synaptogenesis wikipedia , lookup
Optogenetics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neural engineering wikipedia , lookup
Subventricular zone wikipedia , lookup
Neuroanatomy wikipedia , lookup
Development of the nervous system wikipedia , lookup
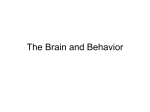
Journal of Clinical Neuroscience (2002) 9(6), 613±617 & 2002 Published by Elsevier Science Ltd. DOI: 10.1054/jocn.2002.1080, available online at http://www.idealibrary.com on Review Current concepts in central nervous system regeneration Ross D. Gurgo1 MBBS, Kuldip S. Bedi2 PHD DSC, Victor Nurcombe2 PHD 1 Department of Neurosurgery, Princess Alexandra Hospital, Brisbane, 2Department of Anatomy and Developmental Biology, The University of Queensland, Australia Summary A dictum long-held has stated that the adult mammalian brain and spinal cord are not capable of regeneration after injury. Recent discoveries have, however, challenged this dogma. In particular, a more complete understanding of developmental neurobiology has provided an insight into possible ways in which neuronal regeneration in the central nervous system may be encouraged. Knowledge of the role of neurotrophic factors has provided one set of strategies which may be useful in enhancing CNS regeneration. These factors can now even be delivered to injury sites by transplantation of genetically modified cells. Another strategy showing great promise is the discovery and isolation of neural stem cells from adult CNS tissue. It may become possible to grow such cells in the laboratory and use these to replace injured or dead neurons. The biological and cellular basis of neural injury is of special importance to neurosurgery, particularly as therapeutic options to treat a variety of CNS diseases becomes greater. & 2002 Published by Elsevier Science Ltd. Keywords: neural, regeneration, neurobiology, neurotrophins, stem cells, transplantation INTRODUCTION Unlike most other systems, the central nervous system has a limited capacity for regeneration, making any injury particularly devastating. Ramon y Cajal reported in 1928 that injured CNS axons could re-grow into pre-degenerated peripheral nerve tissue.1 This was later confirmed by Aguayo's group in the 1980s.2 These researchers went on to show that the CNS neurons were intrinsically able to regenerate their injured axons if exposed to suitable environmental conditions. Over the past decade much work has focused on understanding the cellular and molecular bases of this axonal regeneration. These studies may have application for the treatment of traumatic injuries of the spinal cord and brain. In parallel to these studies a greater understanding of the factors which cause neuronal cell death in the CNS may open up the possibility of enhancing neuronal survival after injury or during degenerative diseases of the nervous system (such as Parkinson's disease or motor neuron disease). Regeneration within the CNS is a multistep process. In order to achieve neuronal regeneration after injury, several factors have to be controlled. First, the injured neurons have to survive or be replaced by newly transplanted neurons. The axons of these neurons must be induced to re-grow and find a pathway to the appropriate targets. The axon terminals are required to form functional synaptic contacts with the correct regions of the targets. Only once all of these conditions have been met is it possible to restore correct functioning of the injured region. Prevention of neuronal cell death after injury is the subject of much current research. Axon growth occurs at the growth cone, which itself is responsive to the external environment. There are known to be factors in the post-lesion CNS environment that can either inhibit or augment growth cone activity. These factors operate via cell surface receptors which when activated cause a cascade of events via intracellular messengers that eventually involve changes in the cytoskeleton. These changes are capable of controlling and directing axonal growth. It is important to appreciate that clinical neurological improvement after injury is not necessarily evidence of axonal regeneration. Often it is possible to explain such improvement as being the result of other mechanisms that may involve the recruitment of other pre-existing pathways to take over the functions of an injured pathway. CONTRIBUTION OF DEVELOPMENTAL NEUROBIOLOGY TO THE UNDERSTANDING OF NEURAL REGENERATION A thorough knowledge of how embryonic neural cells first arise in development from a pool of uncommitted precursors and develop into mature neurons may enhance our ability in understanding neuronal regeneration. It may also show us how transplanted cells may survive, grow and integrate themselves into a host CNS. Our increasing understanding of genomics and stem cell biology has presented us a multitude of genes and gene products that may have crucial roles in neuronal survival and regeneration. It is now known that the extracellular environment, largely created by cellular exudates, is part of a crucial feedback loop. This influences the cell nucleus as to the order of genes that need to be sequentially activated during the developmental cascades. The discipline of developmental neurobiology has identified the inductive interactions that give rise to different neuronal subtypes ± and seeks to explain them in molecular terms. In contrast, neural stem cell biology has concerned itself with the lineage relationships between cells and how they make choices regarding differentiation.3 Received 5 October 2001 Accepted 22 January 2002 NEUROTROPHIC FACTORS Correspondence to: Dr Ross D. Gurgo, Department of Neurosurgery, Princess Alexandra Hospital, Ipswich Road, Woolloongabba Queensland 4102, Australia. E-mail: [email protected] Any review of CNS regeneration is not complete without mention of the neuronal-growth/supportive role of neurotrophic factors. A family of polypeptides, collectively known 613 614 Gurgo et al. as neurotrophins, which include the prototypical NGF, as well as BDNF, NT3, NT4/5 and NT6, are believed to be at least partially responsible for keeping developing neurons viable until their projecting axons and dendrites reach their target tissue.4 Thus, a neurotrophic factor has a neurotrophic function, in addition to its neurotropic role, axon guidance.5 Since the distance axons are required to grow varies between populations of neurons, the timing of specific neurotrophic dependencies also varies accordingly. It has been postulated that neurons are programmed before differentiation to switch chemotrophic dependencies at the right time, irrespective of external signals.6 This can also be demonstrated in vitro (Figs 1, 2). Neurotrophins are not only restricted to the survival of differentiated neurons, they have also been shown to promote differentiation during neural development.7 Neurotrophic activity may be in part dependent on other more mitogenic factors, such as heparin sulphate proteoglycans.8 This mechanism allows tissue and temporally-specific regulation of the neurotrophic factor effect and thus may provide an sopportunity for clinical manipulation. Neurotrophic factors, aside from their actions during CNS development, also have a role in `day-to-day' maintenance of CNS integrity. Fig. 1 Nerve Cells being grown in in vitro cell culture (upper photo) and staining with neuronal-specific staining to indicate neuronal (as opposed to glial) differentiation (lower photo). Journal of Clinical Neuroscience (2002) 9(6), 613±617 Implantation of cells genetically engineered to produce neurotrophic factors may therefore be important in promoting CNS regeneration; however, the optimal way of achieving this has not yet been determined. THE USE OF STEM CELLS IN NEURAL REGENERATION Although much is known about the embryonic development of the brain, the lineages that neural precursors follow during brain growth and their continued role in adult life are only partly understood. Until recently, it was unclear whether neurogenesis proceeded like haematopoiesis ± from a pluripotent batch of stem cells that both self-renew and produce multipotent progenitors that give rise to progressively more committed progeny, or if some other developmental hierarchy was present.9 Recent in vitro studies indicate that multipotent, Fig. 2 Cellular differentiation from a neurosphere (undifferentiated cells). Neurla progenitor cells with differentiate into glial cells (upper photo) unless cultured in a medium containing FGF-1, which will cause them to differentiate into neurons (lower photo). & 2002 Published by Elsevier Science Ltd. Current concepts in CNS regeneration 615 self-renewing progenitors of neurons and glia can be isolated from adult brain regions.10 The demonstration that the adult brain contains stem cells raises the attractive possibility that endogenous neurogenesis may be manipulated to therapeutic advantage11 after CNS injury. DNA labelling studies have shown that progenitors residing in the subventricular zones adjacent to the ependyma continuously migrate to the olfactory bulb and differentiate into local interneurons.12 Similarly, in the adult hippocampus, progenitors in the subgranular zone have been shown to give rise to cells that differentiate into dentate gyrus granule cells.13 Moreover, the cells seem to be remarkably plastic: adult hippocampal stem cells can give rise to regionally-specific cell types not only in the hippocampus, but also in the olfactory bulb, cerebellum, and retina.14,15 They can even migrate considerable distances, especially after implantation into the neonatal brain.16 Thus, neural stem cells from both embryo and adult seem to be `re-programmable'; an idea, drawn from haematopoeisis, that there is a generic, `naõÈ ve' brain stem cell. What is proving truly remarkable is the range of cell types that can be produced in a culture dish when the environment ± growth or trophic factors, in combination with particular substrates ± is configured appropriately. In the CNS of the developing embryo the process of neuronal subtype development is dependent on the three-dimensional patterning of the developing neural tube. CNS neuronal specification is now thought to occur within a 3-dimensional coordinate system of inductive signals.17 This produces neuronal subtype specification. The differentiation of dopaminergic neurons occurs much more robustly in threedimensional explant cultures of intact embryonic brain than in single cell culture.18 The contribution of developmental neurobiology to understanding neuronal regeneration and implications for CNS cellular transplantation is clear. There may exist neuronal `stem' cells in the adult CNS that may be cultured and used for CNS repair. If transplantation of cells into the CNS is to continue to progress, lessons from the developing CNS, such as the way in which a developing cell `integrates' into its surrounding environment in a three-dimensional context and the factors which support this occurrence, must be applied. MEDIATORS OF NEURONAL CELL DEATH Compared to other cell types, neurons seem to have evolved quite a complex death mechanism. Unlike most other cells, which are quickly turned over, neurons are postmitotic ± throughout our lives, we maintain roughly the same set of neurons as when we are born. Thus, the CNS seems to have adapted an entirely different defence for neurons aimed at keeping them alive as long as possible. How does knowledge of this complicated set of mechanisms help us as for the treatment of neurodegenerative disorders? It is now known that apoptotic mechanisms contribute to both acute and chronic neurodegenerative diseases.19 The multiple controlling points in the neuronal death pathways provide a large number of possibilities at which to intercede therapeutically. That is, to prevent cell death and stimulate regeneration the intracellular signals that transduce external insults may be altered. Apoptotic cell death is controlled by several transcription factors (p53, fas, c-Jun, bax and bcl-2) that may be manipulated pharmacologically or genetically in order to prevent such cell loss.20 The upregulation of anti-apoptotic genes may also be pro-regenerative. Manipulation of growth-associated proteins such as tubulin, actin and GAP-43 may stimulate a cell to re-enter a regenerative mode. Intracellular calcium and & 2002 Published by Elsevier Science Ltd. second messengers (cAMP, cGMP) also offer means for intervention due to their transducive roles. However, effects observed in in vitro experiments can be difficult to replicate in the in vivo situation. Various drugs which have the intention to manipulate a certain biochemical pathway may be lethal when administered systemically in humans. Furthermore, systemic approaches by their very nature affect all regions of the body and do not allow for cell type individuality and uniqueness of response within the CNS. The response of cells to neurotrophic factors may be altered after injury or encountering an inhibitory substrate.21 Concepts of neuroprotection, well documented in the neurosurgical literature, will complement other concepts, as just described, to prevent neuronal death in a clinical setting. AXON GUIDANCE AND REMOVAL OF GROWTH INHIBITION In addition to axonal regeneration, correct axon guidance and synapse formation is required for functional recovery. A number of axon guidance molecules exist, such as polysialic acid-containing neural adhesion molecules (NCAMs) which have been shown to be associated with regenerating axons in the hippocampus. Other proteins, such as the SLIT group, also act to guide axons during development although their role following neuronal damage is not well understood. Growth inhibitory molecules were first systematically documented by Schwab's group in 1988,22 which discovered an antibody (INO-1) which could block inhibitory effects of glial scars on axonal regeneration. This inhibitory target has now been cloned ± NOGO.23 An understanding of developmental neurobiology and the role of axonal guidance molecules has heightened the understanding of the way in which neurons respond to insult. Some of the inhibitory factors expressed during CNS development may be re-expressed after CNS injury, such as the chemorepellant semaphorin III24 and the proteoglycan NG2.25 Scar tissue, rich in the sugar chondroitin sulfate, may act as a simple barrier to axon regrowth,26 tested by the use of the enzyme chondroitinase against this component.27 Chondroitin sulfate may also induce or enhance immune response after neurotrauma (or indeed transplantation procedures) and so discourage axon growth. Post-traumatic cellular responses, in particular macrophage and microglial activation, may inhibit axon regrowth.28 In fact, when glial scarring has been experimentally reduced, axonal regrowth is significantly enhanced.29 It is clear, however, that axon guidance molecules, both permissive and inhibitory, have the potential to be manipulated to circumvent scar tissue and promote axon growth. CLINICAL APPLICATIONS Cell replacement is an important step in CNS recovery because of the limited regenerative and divisional capacity.30±36 The first step to a successful graft is survival and the second the formation of the required neuronal connections. If stem cells are used, appropriate differentiation into the required cell must occur. Co-implantation of cells which have been genetically engineered to produce neurotrophic factors may enhance stem cell survival.37 Recent research has demonstrated that there stem cells exist in the CNS, mainly the hippocampus and possibly the subventricular zone; such cells could be used as a source of stem cells for reimplantation.3 Fetal cells represent the ideal source of stem cells due to their plasticity Journal of Clinical Neuroscience (2002) 9(6), 613±617 616 Gurgo et al. (pluripotentiality) and relative lack of immune excitation; however, ethical and political issues have impeded their use. `Immortalised' neurons from culture have also been used experimentally, such as the NT2 (human terato-carcinomainitiated neuronal cell line38 and have shown both prolonged survivability after transplantation and, importantly, appropriate integration into local neural circuits. Demyelinating diseases may also be treated by cellular replacement; oligodendrocyte/type 2 astrocyte progenitor cells have been shown to be capable of extensive remyelination when injected into the CNS.39 Cell grafts which have been engineered to produce neurotrophic factors (such as NT3, BDNF, CDNF) also hold promise for axonal regeneration and neuronal recovery. Aguayo has shown that Muller cells engineered to produce BDNF may temporarily rescue injured retinal ganglion cells.40 Fibroblasts engineered to express BDNF have also been shown to promote long-tract regeneration in the spinal cord.41 Various studies have only shown adequate regeneration in the milieu of the growth factors and not beyond.42 The temporary response has been attributed to growth-inhibitory effects induced by the lesion.40 Intrathecal administration of neurotrophic factors has been suggested for a more widespread response.43 A more complete understanding of the widespread effects of neurotrophins on neuronal function, beyond regeneration on neuronal activity (such as membrane excitability) is required before their optimal use in a clinical setting can be achieved. The use of genetically engineered cells which express neurotrophic factors may also promote survival of cells which are predisposed to neurodegenerative disease, for example, nigral tissue.44 The use of such cells to promote survival of grafted tissue has also been suggested.45 Mechanical bridging is a physical necessity to support any form of graft. Bridging may be cellular or by the use of artificial substances. The former will be enhanced by an appreciation of developmental neurobiology; the way in which schwann cells or the immature nervous system provides a permissive substance for cell growth. Much promise has been shown recently with cells taken from the olfactory epithelium (olfactory ensheathing cells; the only neuronal cells in the CNS in which spontaneous axonal regeneration after sectioning occurs) which may have the potential to guide regenerating neurons. This has been demonstrated in both spinal cord (long tract) and dorsal root ganglion experimental models.46±48 Evidence also exists that olfactory ensheathing cells may assist regenerating axons in traversing injury-induced glial scar.49 Artificial substrates have the potential for repair of lesions where bridging is required. The substrate required will ideally be immune tolerant and have a porous scaffold. Vinyl chloride porous tubes have been used experimentally in spinal cord injury.50 Alginate gels soaked in neurotrophins have also been suggested,51 and incorporation of guidance molecules discussed in the previous section could also be used. Although the CNS has long been considered an immunologically privileged area, both cellular and humoral immune responses may have a role to play in neuronal response to injury. Although some investigators have suggested that the immune response may assist regeneration, others have shown that inhibition of TNF and TGF-b2 significantly decrease scarring and tissue loss. Some interferons may modulate several extracellular matrix molecules and thus potentially enhance axonal regeneration. Experimental evidence exists that suggests that microglial cells, part of the central immune response may act in a pro-regenerative role, possibly by way of cytokine secretion. Possibly because the CNS is relatively Journal of Clinical Neuroscience (2002) 9(6), 613±617 immunologically `privileged', rejection to cell transplants is probably minimal.52 Neurotrophic factor and stem cell technology has applications in neurodegenerative and genetic diseases, neurotrauma and cerebral ischaemia.53 Neurodegenerative diseases that are amenable to treatment are most notably Parkinson's Disease and Huntington's disease, by transplantation of cells genetically engineered to secrete l-dopa in the former condition and stem cells into the head of the caudate nucleus in the latter. Such treatment is still in its infancy. A number of genetic diseases, such as mucopolysaccharidosis type VII may also be treated by gene therapy techniques,54 the goal being to provide a required protein or block one which is deleterious to normal function. Various polyneuropathies (such as diabetic) may be treated with neurotrophic factor delivery.55 ALS may also be treated with intrathecal neurotrophic factor delivery.56 The optimum method of neurotrophin delivery to give a prolonged effect has not yet been established. The treatment of stroke and head injury (especially secondary neurotrauma, similar to stroke) is potentially treatable by transplantation of cells genetically engineered to secrete neurotrophic factors or by transplantation of stem cells. However, the widespread nature of a cerebro-occlusive or cerebrotraumatic insult may lessen the potential effect of a grafting procedure. Due to its focal nature, spinal cord injury has long been a focus of neural regenerative and repair and would involve a number of the treatment aspects mentioned previously, such as cellular replacement, axon support and guidance and removal of inhibitory factors.57 CONCLUSION Exciting advances are currently occurring in the field of neural regeneration. An increased understanding of the nature of neuronal injury, the factors which cause neuronal death and inhibit neuronal regrowth, the way in which axons direct (and redirect) themselves to a target and the role and actions of neurotrophic factors have begun to hint at ways neuronal injury can be treated more effectively clinically. The importance of developmental neurobiology has become increasingly clear as the quest to appreciate the way in which the CNS attempts to repair itself after injury is undertaken. Cellular transplantation into the CNS is already a reality, and an appreciation of aspects of CNS regeneration will assist in augmenting this process. The introduction, survival and integration of new nerve cells into the damaged CNS remains the ultimate goal. ACKNOWLEDGEMENTS The authors wish to thank Hiram Chipperfield, PhD student at the Department of Anatomy and Developmental Biology, The University of Queensland, for providing the photographs used in this paper. This work was supported by a grant from the Princess Alexandra Hospital Research and Development Foundation. REFERENCES 1. Kesselring J. Neurorehabilitation: a bridge between basic science and clinical practice. Eur J Neurol 2001; 8: 221±225. 2. Aguayo AJ, Bray GM, Rasminsky M. Synaptic connections made by axons regenerating in the central nervous system of adult mammals. J Exp Biol 1990; 153: 199±224. 3. Anderson DJ. Stem cells and pattern formation in the nervous system: the possible versus the actual. Neuron 2001; 30: 19±35. & 2002 Published by Elsevier Science Ltd. Current concepts in CNS regeneration 617 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Davies AM. Neurotrophins: more to NGF than just survival. Curr Biol 2000; 10: 374±376. Davies AM. Neurotrophins: neurotrophic modulation of neurite growth. Curr Biol 2000; 10: 198±200. Oppenheim RW. The concept of uptake and retrograde transport of neurotrophic molecules during development: history and present status. Neurochem Res 1996; 21: 769±777. de la Rosa EJ, Arribas A, Frade JM. Role of neurotrophins in the control of neural development: neurotrophin-3 promotes both neuron differentiation and survival of cultured chick retinal cells. Neuroscience 1994; 58: 347±352. Nurcombe V, Ford MD, Wildschut JA. Developmental regulation of neural response to FGF-1 and FGF-2 by heparan sulfate proteoglycan. Science 1993; 260: 103±106. Gage FH. Mammalian neural stem cells. Science 2000; 287: 1433±1438. Rietze RL, Valcanis H, Brooker GF. Purification of a pluripotent neural stem cell from the adult mouse brain. Nature 2001; 412: 736±739. Magavi SS, Leavitt BR, Macklis JD. Induction of neurogenesis in the neocortex of adult mice. Nature 2000; 405: 951±955. Lois C, Alvarez-Buylla A. Long-distance neuronal migration in the adult mammalian brain. Science 1994; 264: 1145±1148. Eriksson PS, Perfilieva E, Bjork-Eriksson T. Neurogenesis in the adult human hippocampus. Nat Med 1998; 4: 1313±1317. Gage FH, Coates PW, Palmer TD. Survival and differentiation of adult neuronal progenitor cells transplanted to the adult brain. Proc Natl Acad Sci USA 1995; 92: 11879±11883. Takahashi M, Palmer TD, Takahashi J. Widespread integration and survival of adult-derived neural progenitor cells in the developing optic retina. Mol Cell Neurosci 1998; 12: 340±348. Brustle O, Choudhary K, Karram K. Chimeric brains generated by intraventricular transplantation of fetal human brain cells into embryonic rats. Nat Biotechnol 1998; 16: 1040±1044. Jessell TM, Sanes JR. Development. The decade of the developing brain. Curr Opin Neurobiol 2000; 10: 599±611. Hynes M, Rosenthal A. Specification of dopaminergic and serotonergic neurons in the vertebrate CNS. Curr Opin Neurobiol 1999; 9: 26±36. Yuan J, Yankner BA. Apoptosis in the nervous system. Nature 2000; 407: 802±809. Naskar R, Dreyer EB. New horizons in neuroprotection. Surv Ophthalmol 2001; 45(Suppl 3): S250±S255; discussion S273±S276. Dikranian K, Ishimaru MJ, Tankova T. Apoptosis in the in vivo mammalian forebrain. Neurobiol Dis 2001; 8: 359±379. Caroni P, Savio T, Schwab ME. Central nervous system regeneration: oligodendrocytes and myelin as non-permissive substrates for neurite growth. Prog Brain Res 1988; 78: 363±370. Bandtlow CE, Schwab ME. NI-35/250/nogo-a: a neurite growth inhibitor restricting structural plasticity and regeneration of nerve fibers in the adult vertebrate CNS. Glia 2000; 29: 175±181. Pasterkamp RJ, Ruitenberg MJ, Verhaagen J. Semaphorins and their receptors in olfactory axon guidance. Cell Mol Biol 1999; 45: 763±779. Margolis, RU, Margolis RK. Chondroitin sulfate proteoglycans as mediators of axon growth and pathfinding. Cell Tissue Res 1997; 290: 343±348. Zuo J, Neubauer D, Dyess K. Degradation of chondroitin sulfate proteoglycan enhances the neurite-promoting potential of spinal cord tissue. Exp Neurol 1998; 154: 654±662. Moon LD, Asher RA, Rhodes KE. Regeneration of CNS axons back to their target following treatment of adult rat brain with chondroitinase ABC. Nat Neurosci 2001; 4: 465±466. Fitch MT, Silver J. Activated macrophages and the blood-brain barrier: inflammation after CNS injury leads to increases in putative inhibitory molecules. Exp Neurol 1997; 148: 587±603. Davies SJ, Fitch MT, Memberg SP. Regeneration of adult axons in white matter tracts of the central nervous system. Nature 1997; 390: 680±683. Horner PJ, Gage FH. Regenerating the damaged central nervous system. Nature 2000; 407: 963±970. Houle JD, Ye JH. Survival of chronically-injured neurons can be prolonged by treatment with neurotrophic factors. Neuroscience 1999; 94: 929±936. Kempermann G, Gage FH. New nerve cells for the adult brain. Sci Am 1999; May: 48±53. & 2002 Published by Elsevier Science Ltd. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. Kermer P, Klocker N, Bahr M. Neuronal death after brain injury. Models, mechanisms and therapeutic strategies in vivo. Cell Tissue Res 1999; 298: 383±395. Klocker N, Bahr M. Brain repair ± new avenues to an eternal dream. Trends Neurosci 2001; 24: 3±4 Mansergh FC, Wride MA, Rancourt DE. Neurons from stem cells: implications for understanding nervous system development and repair. Biochem Cell Biol 2000; 78: 613±628. Mehler MF, Kessler JA. Progenitor cell biology. Implications for neural regeneration. Arch Neurol 1999; 56: 780±784. Tuszynski MH, Roberts J, Senut MC. Gene therapy in the adult primate brain: intraparenchymal grafts of cells genetically modified to produce nerve growth factor prevent cholinergic neuronal degeneration. Gene Ther 1996; 3: 305±314. Andrews PW. Retinoic acid induces neuronal differentiation of a cloned human embryonal carcinoma cell line in vitro. Dev Biol 1984; 103: 285±293. Groves AK, Barnett SC, Franklin RJ. Repair of demyelinated lesions by transplantation of purified O-2A progenitor cells. Nature 1993; 362: 453±455. Di Polo A, Aigner LJ, Dunn RJ. Prolonged delivery of brain-derived neurotrophic factor by adenovirus-infected Muller cells temporarily rescues injured retinal ganglion cells. Proc Natl Acad Sci USA 1998; 95: 3978±3983. Liu Y, Kim D, Humes BT. Transplants of fibroblasts genetically modified to express BDNF promote regeneration of adult rat rubrospinal axons and recovery of forelimb function. J Neurosci 1999; 19: 4370±4387. Houle JD, Ye JH. Survival of chronically-injured neurons can be prolonged by treatment with neurotrophic factors. Neuroscience 1999; 94: 929±936. Novikova L, Novikov L, Kellerth JO. Effects of neurotransplants and BDNF on the survival and regeneration of injured adult spinal motoneurons. Eur J Neurosci 1997; 9: 2774±2777. Nakao N, Yokote H, Nakai H. Promotion of survival and regeneration of nigral dopamine neurons in a rat model of Parkinson's disease after implantation of embryonal carcinoma-derived neurons genetically engineered to produce glial cell line-derived neurotrophic factor. J Neurosurg 2000; 92: 659±670. Bjorklund A, Lindvall O. Cell replacement therapies for central nervous system disorders. Neuroscience 2000; 3: 537±544. Ramon-Cueto A, Avila J. Olfactory ensheathing glia: properties and function. Brain Res Bull 1998; 46: 175±187. Bartolomei JC, Greer CA. Olfactory ensheathing cells: bridging the gap in spinal cord injury. Neurosurgery 2000; 47: 1057±1069. Taylor JS et al. Transplants of olfactory bulb ensheathing cells promote functional repair of multiple dorsal rhizotomy. Prog Brain Res 2001; 132: 641±654. Li Y, Field PM, Raisman G. Repair of adult spinal rat corticospinal tract by transplants olfactory ensheathing cells. Science 1997; 277: 2000±2002. Bamber NI et al. Fetal spinal cord tissue in mini-guidance channels promotes longitudinal axonal growth after grafting into hemisected adult rat spinal cords. Neural Plast 1999; 6: 103±121. Tobias CA et al. Grafting of encapsulated BDNF-producing fibroblasts into the injured spinal cord without immune suppression in adult rats. J Neurotrauma 2001; 18: 287±301. Ansari AA et al. Lack of a detectable systemic humoral/cellular allogeneic response in human and nonhuman primate recipients of embryonic mesencephalic allografts for the therapy of Parkinson's disease. Transplant Proc; 1995. 27: 1401±1405. Thompson TP, Lunsford LD, Kondziolka D. Restorative neurosurgery: opportunities for restoration of function in acquired, degenerative, and idiopathic neurological diseases. Neurosurgery 1999; 45: 741±752. Snyder EY, Taylor RM, Wolfe JH. Neural progenitor cell engraftment corrects lysosomal storage throughout the MPS VII mouse brain. Nature 1995; 374: 367±370. Apfel SC et al. Efficacy and safety of recombinant human nerve growth factor in patients with diabetic polyneuropathy: A randomized controlled trial. NGF Clinical Investigator Group. JAMA 2000; 284: 2215±2221. Schluep M. Intrathecal delivery of BDNF. Amyotroph Lateral Scler Other Motor Neuron Disord 2000; 1: 141. Lu J, Waite P. Advances in spinal cord regeneration. Spine 1999; 24: 926±930. Journal of Clinical Neuroscience (2002) 9(6), 613±617