Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Nucleic acid analogue wikipedia , lookup
Genetic engineering wikipedia , lookup
Genomic imprinting wikipedia , lookup
DNA vaccination wikipedia , lookup
Bioinformatics wikipedia , lookup
Gene expression profiling wikipedia , lookup
Molecular cloning wikipedia , lookup
Metagenomics wikipedia , lookup
Cre-Lox recombination wikipedia , lookup
Gene prediction wikipedia , lookup
DNA supercoil wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Real-time polymerase chain reaction wikipedia , lookup
Endogenous retrovirus wikipedia , lookup
Genome editing wikipedia , lookup
Non-coding DNA wikipedia , lookup
Designer baby wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Genomic library wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
History of genetic engineering wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
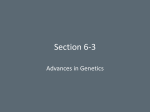
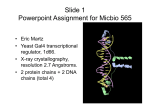
ORIGINAL ARTICLE High-Resolution Array-Based Comparative Genomic Hybridization for Distinguishing Paraffin-Embedded Spitz Nevi and Melanomas Jeff D. Harvell, MD,* Sabine Kohler MD,* Shirley Zhu, MD,* Tina Hernandez-Boussard, PhD,† Jonathan R. Pollack, MD, PhD,* and Matt van de Rijn, MD, PhD* Abstract: Distinguishing between Spitz nevus and melanoma presents a challenging task for clinicians and pathologists. Most of these lesions are submitted entirely in formalin for histologic analysis by conventional hematoxylin and eosin–stained sections, and freshfrozen material for ancillary studies is rarely collected. Molecular techniques, such as comparative genomic hybridization (CGH), can detect chromosomal alterations in tumor DNA that differ between these 2 lesions. This study investigated the ability of high-resolution array-based CGH to serve as a diagnostic test in distinguishing Spitz nevus and melanoma using DNA isolated from formalin-fixed and paraffin-embedded samples. Two of 3 Spitz nevi exhibited no significant chromosomal alterations, while the third showed gain of the short arm of chromosome 11p. The latter finding has previously been described as characteristic of a subset of Spitz nevi. The 2 melanomas showed multiple copy number alterations characteristic of melanoma such as 1q amplification and chromosome 9 deletion. This study has shown the utility of array-based CGH as a potential molecular test in distinguishing Spitz nevus from melanoma. The assay is capable of using archival paraffin-embedded, formalin-fixed material; is technically easier to perform as compared with conventional CGH; is more sensitive than conventional CGH in being able to detect focal alterations; and can detect copy number alterations even with relatively small amounts of lesional tissue as is typical of many skin tumors. Key Words: array-based comparative genomic hybridization, Spitz nevus, melanoma, paraffin-embedded samples, archival samples (Diagn Mol Pathol 2004;13:22–25) T he distinction between Spitz nevus and melanoma can be difficult even for expert dermatopathologists.1 Because these lesions are relatively small as compared with neoplasms of other organ systems, the entire lesion is usually submitted for formalin fixation and paraffin embedding, with no frozen tissue remaining for molecular studies. A molecular technique that could use formalin-fixed, paraffin-embedded tissue to help identify melanoma would be a welcome addition to the diagnostic armamentarium of pathologists. Comparative genomic hybridization (CGH) is a technique that can detect copy number changes in tumor DNA and can identify differences between Spitz nevi and melanomas.2 Conventional CGH entails the comparative hybridization of tumor and normal genomic DNA onto normal metaphase chromosomes and as such has a limited cytogenetic-based mapping resolution of approximately 10-20 Mb. Array-based CGH (aCGH) is a new method that weds traditional CGH and microarray technology. In aCGH, tumor and normal genomic DNAs are differentially fluorescently labeled and co-hybridized onto an array containing mapped DNA sequences, providing measurements of tumor copy number changes at high resolution across the genome. Arrays containing up to 2,500 BAC clones have been used for aCGH.3 Gene arrays, which represent an alternative to individual BAC clones, contain up to 30,000 cDNAs that span the human genome and correspond to individual genes or expressed sequence tags (ESTs). The resolution of gene microarrays thus is significantly higher compared with conventional CGH and even better than that seen with current BAC clone arrays. In this study, we have investigated the utility of high-resolution aCGH with gene microarrays as a potential diagnostic tool in distinguishing Spitz nevus from melanoma, using paraffinembedded material. MATERIALS AND METHODS Case Selection From the *Departments of Pathology and †Genetics, Stanford University School of Medicine, Stanford, CA. Reprints: Matt van de Rijn, MD, PhD, Department of Pathology Stanford University Medical Center 300 Pasteur Drive Stanford, CA 94305 (e-mail: [email protected]). Copyright © 2004 by Lippincott Williams & Wilkins 22 Permission to use patient material for these studies was granted according to guidelines set and reviewed by the Stanford University institutional review board for the study of human subjects. Three cases of Spitz nevus and 2 cases of invasive melanoma were culled from the Stanford University pathology files. Case 1 was originally seen at UCSF Diagn Mol Pathol • Volume 13, Number 1, March 2004 Diagn Mol Pathol • Volume 13, Number 1, March 2004 Array-Based CGH for Melanocytic Neoplasms Dermatopathology and previously reported (case 11).4 In each case, the original diagnosis was based on conventional light microscopy. The Spitz nevi and invasive melanomas were classic examples, readily agreed on by 2 dermatopathologists (JDH and SK) (Fig. 1). The clinical characteristics of the individual patients are summarized in Table 1. Array Comparative Genomic Hybridization Gene arrays were obtained from the Stanford Core Facility (http://www.microarray.org/sfgf/jsp/home.jsp) and contained 41,000 cDNA sequences spotted on Corning GAPS II coated microarray slides (Corning Life Sciences, Acton, MA). The chromosomal localization of these genes was uniquely assignable for 35,151 distinct cDNAs, which represented 24,540 different UniGene clusters and 3,225 cDNAs not yet represented in UniGene clusters. Tumor DNA from formalin-fixed, paraffin-embedded tissue and reference DNA (normal gendermatched human leukocytes) were extracted using Qiagen genomic DNA columns. Gender-matched normal reference DNA was isolated from peripheral blood leukocytes and digested with DpnII before further processing. Gel electrophoresis of digested and nondigested DNA isolated from formalinfixed, paraffin-embedded tissue was performed to confirm an appropriate DNA fragment size distribution of approximately 0.5 to 2.0 Kb. Random primer labeling of DNA isolated from tumor samples was performed as described previously 5 (http://www.microarrays.org/protocols.html). Briefly, 2 to 4 micrograms of tumor DNA was fluorescently labeled with Cy5, mixed with reference DNA labeled with Cy3 and an excess of human cot-1, and hybridized overnight to the array. After washing, the array slides were scanned on a GenePix Scanner (Axon Instruments, Foster City, CA) and fluorescence ratios (test/control) calculated using GenePix software. In our experience with this study and other paraffin samples,6 we found that very small samples, less than 5 mm in diameter, could be used if several 10- to 15-µm sections were used to isolate DNA. In our experience, amplification of the genomic DNA was not necessary. For certain types of lesions where the lesional cells are rare compared with surrounding stromal cells laser, capture microdissection may be considered, but for our FIGURE 1. Histopathology of (A) Spitz nevus with 11p amplification and (B) melanoma. A. Nested spindle shaped nevus cells at the dermo-epidermal junction and epithelioid nevus cells within the dermis characterize this Spitz nevus (case 3). (B) Dermal nests of cytologically atypical melanocytes with cytoplasmic melanin and obvious mitotic activity characterize this invasive melanoma (case 4). specimens this did not appear to be necessary and this probably holds true for most melanocytic lesions. Data were uploaded in the Stanford Microarray Database (http://genome-www5.stanford.edu/MicroArray/SMD/)7 for subsequent analysis. Only cDNA spots with a ratio of signal over background of at least 1.5 in the Cy3 channel TABLE 1. Array-Based CGH Changes of Spitz Nevi and Melanoma Case 1* 2 3 4 5 Age/Sex Histologic Diagnosis 9/F 30/M 33/F 77/M 74/M Compound Spitz nevus Intradermal Spitz nevus Compound Spitz nevus Invasive melanoma, superficial spreading type, Breslow 7.0 mm Invasive melanoma, superficial spreading type, Breslow 4.2 mm aCGH Amplifications None None 11p 1q, 15q 6p, 17q aCGH Deletions None None None 9, 10, 11, 15p 1p, 11, 15p *Previously reported.4 © 2004 Lippincott Williams & Wilkins 23 Diagn Mol Pathol • Volume 13, Number 1, March 2004 Harvell et al were included for analysis. Chromosomal localization of the mapped genes was assigned by alignment against the “Goldenpath” genome assembly data. Copy number changes across chromosomes were represented using a smoothing function based on a moving average of 5 adjacent genes8 and were visualized using “CaryoScope” (http://genome-www5. stanford.edu/cgi-bin/dev/rees/nph-aCGH-highres.pl), a software program written by Christian Rees. RESULTS AND DISCUSSION Despite nearly 60 years of study, the accurate diagnosis of Spitz nevus remains a challenge and its exact biologic potential, a controversy. Nonetheless, recent studies comparing both gene microarray expression data from freshly procured mRNA and a CGH data using archival formalin-fixed breast specimens have shown significant correlation between actual gene expression and highly amplified DNA segments.5,6 Many of these difficult lesions find their way to a specialist consultant. While there have been advances in immunohistochemistry and refined histologic criteria for distinguishing Spitz nevus from melanoma, there remains a subset of Spitz nevi that cannot be reliably distinguished from melanoma even by expert dermatopathologists.1 Recently, studies of Spitz nevus and melanoma by conventional CGH have uncovered molecular differences between the 2.2,9 Spitz nevi generally show no genetic changes by conventional CGH, but a subset can show an 11p gain.2,4 In contrast, melanomas show a number of cytogenetic abnormalities, including deletions of chromosomes 9, 10, 6q and 8p, and amplifications of chromosomes 7, 8q, 6p, 1q, 20, 17, and 2.9 Moreover, melanomas do not exhibit the 11p amplification seen in some Spitz nevi.2 Prior studies have already shown the ability of aCGH to accurately distinguish between benign and malignant renal and prostate tumors.3,10 These studies used up to 2460 cDNA BAC clones that spanned the human genome, and in the second study, DNA isolated from formalin-fixed, paraffin-embedded material was used.3 In the present study we used gene microarrays that contained 41,000 individual cDNAs spotted on a single microarray slide, representing 24,540 different mapped UniGene clusters and 3,225 mapped cDNAs not yet represented in UniGene clusters. We analyzed 3 Spitz nevi and 2 melanomas by aCGH. The histologic features of 2 representative cases are shown in Figure 1. Two of 3 Spitz nevi showed no significant chromosomal amplifications or deletions, whereas the third showed a distinct gain of chromosome 11p (Table 1, Fig. 2). Case 1 had been previously studied by conventional CGH4 (case 11) and likewise showed no detectable chromosomal alterations. Both melanomas displayed several of the chromosomal amplifications/deletions characteristic of melanoma9 (Table 1, Fig. 2). The full data set of these experiments is available from SMD (http://genome-www5.stanford. edu/MicroArray/SMD/).7 In addition, histologic images from all cases studied and PDF files from the aCGH experiments 24 FIGURE 2. Array-based DNA copy number profiles of (A) Spitz nevus and (B) melanoma. Individual cDNAs are arranged according to their known location along human chromosomes to produce a representation of tumor DNA copy number changes mapped onto the normal human genome. Each vertical line (red or green) indicates the position of a single cDNA clone, and the length of the line corresponds to the 1og10 fluorescence ratio of tumor versus reference DNA for that locus, reported as a moving average of 5 adjacent clones. Red lines indicate areas of amplification and green lines indicate areas of deletion. (A) Case 3 shows a distinct gain of 11p, as is characteristic of a subset of Spitz nevi. The low level red and green signals on chromosomes 1, 9, and 10 are within the variation seen in normal versus normal hybridizations and therefore are not interpreted as evidence of copy number changes. (B) Case 4 shows alterations characteristic of melanoma, including deletions of chromosome 9, 10, and 11 and amplification of 1q. Raw data from all experiments can be downloaded from SMD, and figures of all aCGH experiments and histology in this paper can be seen at the accompanying web site (http://microarray-pubs.stanford. edu/Spitz). performed can be found at the accompanying web site (http://microarray-pubs.stanford.edu/Spitz). Until very recently, gene array studies of human cancers have been partially limited in their scope due to dependence upon mRNA transcripts, which require the acquisition of fresh tissue. The need for a sizable piece of fresh tumor tissue precluded from study many cutaneous tumors, which are often small, and as a result, cannot be apportioned for research. This is especially the case with melanocytic lesions where the entire specimen is submitted for histologic analysis to determine important prognostic features such as depth of invasion, vascular invasion, regression, etc. The present study used punch biopsies as small as 5 mm in diameter yielding DNA amounts greater than 4.0 µg, thus illustrating that meaningful results can be obtained even with tiny amounts of lesional tissue. Since molecular-based gene expression studies are still considered new technology and since many of the published © 2004 Lippincott Williams & Wilkins Diagn Mol Pathol • Volume 13, Number 1, March 2004 genomic studies have relied on fresh tissue, these typically have only 1 or 2 years clinical follow-up information, which is inadequate to allow for meaningful correlation of gene expression changes with outcome. Case 1 was originally diagnosed 11 years ago illustrating that relatively antiquated paraffin blocks can provide meaningful results that can be correlated with long-term follow-up data. This is especially important for borderline melanocytic lesions where prolonged follow-up over many years may be required to ensure benign biologic behavior (ie, absence of metastasis). Gene expression profiling experiments use mRNA harvested from fresh tumor tissue, from which cDNAs are produced and used for hybridization. They have the benefit of detecting which genes are being actively expressed (ie, transcribed), but have the disadvantage of requiring fresh tumor tissue. Genomic DNA is used in aCGH, but since the procured DNA comprises both transcribed and nontranscribed genes, the ability to determine which genes are actually being expressed within a tumor is less apparent. Nonetheless, recent studies comparing both gene microarray expression data from freshly procured mRNA and aCGH data using archival formalin-fixed breast specimens have shown significant correlation between actual gene expression and highly amplified DNA segments.5 As reflected in the present study, aCGH has the further advantage of using DNA from formalin-fixed and paraffin-embedded biopsies. Furthermore, aCGH is technically easier to perform than conventional CGH since the investigator does not have to be expert in cytogenetics to interpret results. Finally, the sensitivity of aCGH for the detection of localized alterations is superior to traditional CGH because of the increased physical mapping resolution afforded by measuring changes across 41,000 individual genes or short genomic segments. This increased sensitivity may uncover other genetic changes characteristic of melanoma, which are not detectable by conventional CGH or aCGH with fewer DNA targets. For instance, in this study, both melanomas displayed deletions of chromosome 11, which to our knowledge, has not been previously emphasized. In summary, we have demonstrated the possibility of using genome wide array-based CGH as a diagnostic aid in dif- © 2004 Lippincott Williams & Wilkins Array-Based CGH for Melanocytic Neoplasms ferentiating Spitz nevus from melanoma. The procedure can be applied to archival formalin-fixed and paraffin-embedded biopsies and can provide meaningful results even from small punch biopsies. The present study is small and used classic examples of Spitz nevus and melanoma and needs to be confirmed by a larger study that includes histologically questionable cases with long-term follow-up. We believe that aCGH will prove to be a valuable adjunct in correctly classifying melanocytic tumors, in much the same way that PCR-based gene rearrangement studies have aided the classification of cutaneous lymphoproliferative disorders.11 REFERENCES 1. Barnhill RL, Argenyi ZB, From L, et al. Atypical Spitz nevi/tumors: lack of consensus for diagnosis, discrimination from melanoma, and prediction of outcome. Hum Pathol. 1999;30:513–520. 2. Bastian BC, Wesselmann U, Pinkel D, et al. Molecular cytogenetic analysis of Spitz nevi shows clear differences to melanoma. J Invest Dermatol. 1999;113:1065–1069. 3. Paris PL, Albertson DG, Alers JC, et al. High resolution analysis of paraffin-embedded and formalin-fixed prostate tumors using comparative genomic hybridization to genomic microarrays. Am J Pathol. 2003;162: 763–770. 4. Harvell JD, Bastian BC, LeBoit PE. Persistent (recurrent) Spitz nevi: a histopathologic, immunohistochemical, and molecular pathologic study of 22 cases. Am J Surg Pathol. 2002;26:654–661. 5. Pollack JR, Sørlie T, Perou CM, et al. Microarray analysis reveals a major direct role of DNA copy number alteration in the transcriptional program of human breast tumors. Proc Natl Acad Sci U S A. 2003;99:12963– 12968. 6. Linn SC, West RB, Pollack JR et al. Gene expression patterns and gene copy number charges in dermatofibrosarcoma protuberans. Am J Path. 2003;163:2383–2395. 7. Gollub J, Ball CA, Binkley G, et al. The Stanford Microarray Database: data access and quality assessment tools. Nucleic Acids Res. 2003;31: 94–96. 8. Pollack JR, Perou CM, Alizadeh AA, et al. Genome-wide analysis of DNA copy-number changes using cDNA microarrays. Nat Genet. 1999; 23:41–46. 9. Bastian BC, LeBoit PE, Hamm H, et al. Chromosomal gains and losses in primary cutaneous melanomas detected by comparative genomic hybridization. Cancer Res. 1998;58:2170–2175. 10. Wilhelm M, Veltman JA, Olshen AB, et al. Array-based comparative genomic hybridization for the differential diagnosis of renal cell cancer. Cancer Res. 2002;62:957–960. 11. Kohler S, Jones CD, Warnke RA, et al. PCR-heteroduplex analysis of T-cell receptor gamma gene rearrangements in paraffin-embedded skin biopsies. Am J Dermatopathol. 2000;22:321–327. 25