Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Time perception wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
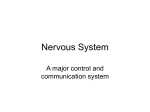
Synaptic gating wikipedia , lookup
Sensory substitution wikipedia , lookup
Neural engineering wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Neuroplasticity wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Development of the nervous system wikipedia , lookup
Neuroregeneration wikipedia , lookup
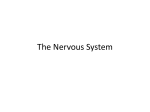
Anatomy of the cerebellum wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
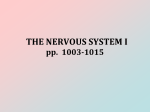
Muscle memory wikipedia , lookup
Microneurography wikipedia , lookup
Embodied language processing wikipedia , lookup
Neuroscience in space wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neuroanatomy wikipedia , lookup
Proprioception wikipedia , lookup
Evoked potential wikipedia , lookup
Central pattern generator wikipedia , lookup
Veterinary Pathophysiology Student’s Lectures, 5th Semester PATHOPHYSIOLOGY OF THE NERVOUS SYSTEM Department of Internal Medicine, Faculty of Veterinary Science Szent István University 1 Circulation of the brain The brain comprises only 2% of the body's weight but receives 20% of the blood supply (cardiac output). Cerebral blood flow (CBF) = 50 ml / 100 g of brain / minute CBF = CPP / CVR (cerebral perfusion pressure=CPP, cerebrovascular resistance=CVR) cerebral blood flow (CBF) cerebral blood volume (CBV) cerebral energy metabolism (CEM) measured as cerebral metabolic rate of oxygen (CMRO2) measured as cerebral metabolic rate of glucose (CMRglu) grey matter > white matter CBF is the same between Part: 60 - 160 mmHg 2 Regulation 1. Metabolic control (or 'metabolic autoregulation') (pH, Pco2 adenosine, glycolytic intermediates, and extracellular potassium) 2. Pressure autoregulation 3. Chemical control (by arterial pCO2 and pO2) 4. Neural control (These neurons contain norepinephrine (NE) and neuropeptide-Y (NPY), which are both vasoconstrictors. A second system consists of parasympathetic neurons in the sphenopalatine and otic ganglia. which contain acetylcholine (ACh) and often coexpress vasoactive intestinal peptide (VIP). The third consists of sensory fibers originating in the trigeminal ganglion. These contain substance P (SP) and calcitonin generelated peptide (CGRP), both of which are vasodilators.) CBF is lost: 10 s – faint!!! 3 Anatomy a. carotis interna (bo.: a. maxill. int.) a. occipitalis – a. basilaris cerebri a. vertebralis a. spinalis ventralis circulus arteriosus cerebri, Circle of Willis rete mirabile epidurale rostrale et caudale 4 PRIMARY STRUCTURAL CHANGES CAUSING CNS-MALFUNCTIONS a. Inflammation of the brain and the spinal cord causes: viruses, bacteria, parasites, fungi and toxic compounds b. Necrosis of the tissues causes: hypoxia, toxins, vitamin deficiency, hypoglycaemia, effects of lipid peroxides, accumulation of some compounds c. Atrophy of the nervous tissue causes: neoplasma, parasites, increased intracranial pressure, discus hernia d. Bleeding causes: capillary damage, embolism, trauma (epidural, subdural, cerebral petechia or haematoma) e. Trauma of the nervous tissue 5 PRIMARY METABOLIC CHANGES CAUSING CNS MALFUNCTIONS 1. a, Altered (decreased or increased) oxygen supply Cause: brain hypoxy (Adams-Stokes syndrome), anaemia, other O2-transport disorders, active or passive hyperaemia Characteristics of blood supply: – lack of anastomoses, presence of own reflex regulation (sinus caroticus: baroreceptors; glomus caroticus: chemoreceptors) – pCO2 local vasodilation – rich in collateral network Consequences: unconsciousness after 7-8 sec of total cortical anoxia, death after 15 minutes The sensitivity to the decreased O2 supply of the central nervous system increases from a caudal to cranial direction. Fast effect: cerebro-cortical necrosis, unconsciousness, death Slow effect: cerebro-cortical necrosis (encephalomalacia) convulsions Hyperoxia may be as dangereous as hypoxia: ↑oxygen-radicals, ↑ LPO → regressive changes including necrosis 6 Retinopathy, blindness due to pure oxygen inhalation in a preterm baby 7 PRIMARY METABOLIC CHANGES CAUSING CNS-MALFUNCTIONS 2. b, Hyperaemia, cerebral edema Cause: circulatory failure, local or general disorders of the water, electrolyte and protein metabolism, decreased outflow of CSF increased intracranial pressure, capillary permeability Consequence: capillary injury decreased cranial blood supply unconsciousness, general symptoms of cerebral damage, convulsions 8 c, Hyperthermia Cause: thermoregulatory disturbance due to increased external heat or decreased heat loss. Body temperature is > 40-42 °C (heat stroke) Consequences: cerebral hyperaemia, -edema, capillary damage, unconsciousness, convulsions, damage of the respiratory and the circulatory centre 9 PRIMARY METABOLIC CHANGES CAUSING CNS-MALFUNCTIONS 3. d, Metabolic disorders HYPOGLYCAEMIA Causes: baby pig disease, increased blood insulin level, ketosis Consequences: weakness, depression, unconsciousness, convulsions, coma HYPERGLYCAEMIA Causes: hyperosmolarity of the blood due to diabetes mellitus, iatrogenic glucose overload (similar effects develop during saline toxicosis or uraemia) cerebral dehydration cerebrocortical necrosis Consequences: depression, coma HYPOCALCAEMIA Causes: lactation, idiopathic, parathyroid gland dysfunctions (neoplasma) Consequences: tetany, convulsions, tremor ACID-BASE IMBALANCES acidosis depression, coma alkalosis convulsions 10 PRIMARY METABOLIC CHANGES CAUSING CNS-MALFUNCTIONS 4. e, Organ-function disorders Liver failure including PSS Causes: NH3, mercaptane, indol, short chain fatty acids, toxins (due to their decreased catabolism), false neurotransmitters (synaptic effect) Consequences: "Hepato-cerebral syndrome” or hepatic encephalopathy, hepatic coma Renal failure Causes: organic acids, catabolised toxic compounds, changes in Ca-P equilibrium, other electrolyte disturbances, hyperosmosis (uraemia!) Consequences: uraemic unconsciousness, convulsions 11 PRIMARY METABOLIC CHANGES CAUSING CNS-MALFUNCTIONS 4. f, Effects of exogenous chemical compounds Causes: toxins such as organic phosphate-esters, lead, drugs etc. Consequences: general, not characteristic consequences, structural alterations of peripherial nerves 12 CONSEQUENCES OF NERVOUS TISSUE DAMAGE 1. Loss of functions – clinically these are the most important a. Damages of the brain and spinal cord nuclei (cell bodies) - dysfunction of the activatory and/or inhibitory functions ( motor function disorders), - disturbances of consciousness changes in behaviour - disturbances of some sensory pathways decreased sensory functions (hypoaesthesia) b. Damages of stimulatory fibers and tracts • decreased reflex-movements, decreased irritability, loss in activatory and/or inhibitory function • motor function disorders (m. weakness: paresis, paralysis) 2. Increased functions c, Increased irritability of cranial and spinal nuclei 13 excitement, hyperaesthesia, convulsions Lower and upper (motor) neurons The term "upper or lower motor neuron" is actually misleading because these motor neurons are not really motor neurons. Lower motor neurons (a type of second-order neuron) are cranial and spinal nerves. The cell bodies of these neurons are located in the CNS (brain or spinal cord), but their axons can leave the CNS and synapse with the muscles of the body Upper motor neurons are a type of first-order neuron. They never leave the CNS. 14 LOWER MOTOR NEURONS (LMN) 1. Efferent motor neurons: connecting the central nervous system (CNS) and peripherial muscles or glands cell body: in all spinal segments in the intermediate and ventral horns of the gray matter and in the nuclei of the cranial nerves. The muscle or group of muscles innervated by one spinal nerve is called a myotome. Each spinal nerve has a dorsal (sensory) and a ventral (motor) root. 2. Afferent sensory neurons: connecting CNS to skin and visceral organs cell body: in the ganglia of the dorsal roots along the spinal cord and in the ganglia of some cranial nerves with the exception of olfaction, vision, hearing and balance. 15 The skin area innervated by one spinal nerve is called a dermatome. the level of lesion b) lumbosacral brachial (b) Schematic representation of the nervous system. UMN pathways are shown descending through the spinal cord to synapse with the LMN cell bodies in the gray matter of the brachial and lumbosacral intumescenses. (Robinson and Huxtable, 1988) 16 - may be Horner's in CT area - LMN signs and LMN: the executioner - Ipsilateral UMN signs below the level of lesion b) lumbosacral brachial 17 MOTOR FUNCTION AND DAMAGE OF LMN-S Function of motor neurons: maintaining muscle tone, proprioception. LMN forms the motor arm (alpha motor neuron) of the stretch reflex TRUNK (myotatic reflex), this can be NERVE superimposed by voluntary movements via a) - LMN signs and upper motor neurons (UMN).- corresponding sensory defects SENSORY NERVE ENDING VENTRAL HORN GREY MATTER VENTRAL NERVE ROOT - LMN signs only - NO corresponding sensory deficit - LMN signs and - may be Horner's in CT area - Ipsilateral UMN signs below the level of lesion NEUROMUSCULAR JUNCTION LMN signs only (Often diffuse and generalized) 18 MOTOR FUNCTION AND DAMAGE OF LMN-S Effects of LMN-damage: so called ”LMN-signs” a, Loss of normal, resting (involuntary) muscle tone (hypotony of muscles, flaccid paresis/paralysis) due to interruption of the myotatic reflex arc. b, Loss of voluntary muscle movement too, as the "final common pathway" is non-functional and the reflex arc for tendon reflexes is disrupted. (The UMN is not effected!) 19 LOWER MOTOR NEURONS (LMN) 1. Efferent motor neurons: connecting the central nervous system (CNS) and peripherial muscles or glands cell body: in all spinal segments in the intermediate and ventral horns of the gray matter and in the nuclei of the cranial nerves. The muscle or group of muscles innervated by one spinal nerve is called a myotome. Each spinal nerve has a dorsal (sensory) and a ventral (motor) root. 2. Afferent sensory neurons: connecting CNS to skin and visceral organs cell body: in the ganglia of the dorsal roots along the spinal cord and in the ganglia of some cranial nerves with the exception of olfaction, vision, hearing and balance. 20 The skin area innervated by one spinal nerve is called a dermatome. MOTOR FUNCTION AND DAMAGE OF LMN-S Signs of LMN-damage (LMN signs): 1. Hypotonia weakness, flaccid paresis/paralysis 2. Hyporeflexia/areflexia reduction in reflex activity 3. Muscle atrophy 4. Electromyographic (EMG) changes after 5-7 days. 5. Contracture and fibrosis of the muscles after weeks If the sensory nerve is not affected, superficial pain perception disappears but deep pain perception is retarded 21 „LMN” signs might be caused by lesions of the neuro-muscular synapsis and/or muscle diseases too SENSORY FUNCTION AND DAMAGE OF LMN-S Function of sensory neurons: sensory innervation of skin, visceral organs, information of posture of the body. a) NERVE TRUNK - LMN signs and - corresponding sensory defects SENSORY NERVE ENDING VENTRAL NERVE ROOT - LMN signs only NEUROMUSCULAR JUNCTION LMN signs only 23 SENSORY FUNCTION AND DAMAGE OF LMN-S Damage of sensory neurons: 1.Anesthesia (complete, most severe consequence) 2.Hypoesthesia or decreased pain sensation (partial lesion) 3.Hyperesthesia or increased sensation or pain (irritative lesion) 4.Loss of reflexes (hypo-, areflexia) 5.Virtual loss of motor functions (LMN signs) Damage of sensory peripherial nerves influences both superficial and deep pain perceptions 24 Upper motor neurons (UMN) UPPER MOTOR NEURONS (UMN) 1. Mainly motor systems within the CNS. A false terminology too. Cell bodies: in the cerebral cortex, basal nuclei (brainstem). Neurons do not leave CNS. A, General motor function: 1. initiation and continuation of voluntary movements 2. maintenance of appropriate muscle tone against gravity (maintenace of tone in extensor muscles), coordination 3. regulation of posture (UMN modulates muscle tone activity by its control over the myotactic reflex arc /stretch receptor, muscle spindles/ by inhibitory interneurons) UMN is divided into pyramidal and extrapyramidal systems. Ascending sensory pathways are also parts of this system. This is the reason why 26 ”UMN” is a false terminology VENTRAL HORN GREY MATTER - NO corresponding sensory deficit (Often diffuse and generalized) - may be Horner's in CT area UMN: the judge - Ipsilateral UMN signs below - LMN signs and the level of lesion b) lumbosacral brachial 27 UPPER MOTOR NEURONS (UMN) 1. – con’t 1. Extrapyramidal system: Several groups of interconnected and related structures that form a series of neurons in a multisynaptic pathway from the brain to the LMN-s Function: perform basis of voluntary movements 2. Pyramidal (corticospinal) system: Monosynaptic system, axons descend directly via the pyramids of the medulla to the spinal cord. Function: finely skilled movements Inhibitory effects of UMN are limiting/controlling the extensor muscle tone (inhibitory tracts: reticulospinal-, rubrospinal tract) Motor function damage of UMN (UMN signs) 1. Poor performance of postural rections, ataxia 2. Hyperreflexia hyperactive (or normal) spinal reflexes 3. Spasticity increased tone in extensor muscles 28 4. Abnormal reflexes UPPER MOTOR NEURONS (UMN) 2. B, General sensory functions of UMN 1. Responsible for proprioception (sensation of position/posture of the body via fasciculus cuneatus & f. gracilis) 2. Responsible for superficial and deep pain Sensory-function damage of UMN (Especially following compression of the spinal cord) 1. Deficit in reflex-proprioception ( tractus spinocerebellaris) 2. (Conscious) proprioceptive deficit (fasciculus cuneatus, f. gracilis) 3. Loss of superficial pain (at the same time as the lost of voluntary motor activity) 4. Loss of deep pain (last clinically useful sign) 29 Distinguising between UMN and LMN 30 UMN and LMN: a summary - LMN signs only - NO corresponding sensory deficit LMN signs only (Often diffuse and generalized) VENTRAL HORN UMN cell body is the judge, making decisions GREY MATTER may be Horner's in CT branches area influenced byandsensory -and motor i.e. defence - LMN signs - Ipsilateral UMN prosecutor. signs below lawyer and LMN is the executioner the level of lesion b) lumbosacral brachial 32 General information on brain anatomy and functions: the mental status (video) 33 Lobes of the brain (human) 34 35 FUNCTIONS AND MALFUNCTIONS OF THE CORTEX AND THE BASAL NUCLEI (TELENCEPHALON) 1. 1. CORTEX Lobus frontalis/frontal lobe Function: 1. Pyramidal divisions learned/skilled movements 2. Extrapyramidal divisions not skilled, voluntary movements 3. Connection with limbic system (prefrontal area) behaviour (mental status! Remember “thalamocortex”) Damage: 1. Learned and intricated movements may be lost 2. Mild paresis (contralateral hemiparesis) turning of head, wander in large circles towards the affected side - "adverse syndrome" 3. Behavioural, mental disturbances Cortex cingulate septal Dienceph. Thal. Hypothal., hypocampus, amygdala Rostral part of barin stem Frontal lobe – essential part of mental status & behaviour PHINEAS GAGE (1823-1860) „On 13th September, 1848, 25-year-old Gage and his crew were working on the Rutland and Burlington Railroad near Cavendish in Vermont…” 38 FUNCTIONS AND MALFUNCTIONS OF THE CORTEX AND THE BASAL NUCLEI (TELENCEPHALON) 2. 1. CORTEX (con’t) Parietal lobe Function: (touch), pain and conscious proprioception Damage: disorders in these sensory functions Occipital lobe Function: conscious perception of visual stimuli Damage: blindness - does not affect pupillary reflex Temporal lobe Function: perception of hearing, influence on behaviour Damage: central deafness 39 FUNCTIONS AND MALFUNCTIONS OF THE CORTEX AND THE BASAL NUCLEI (TELENCEPHALON) 3. 2. BASAL NUCLEI or BASAL GANGLIA included: caudate nucleus, putamen and globus pallidus. These are parts of the extrapyramidal UMN system. Function: control of muscle tone, voluntary movements and proprioception Damage: contralateral weakness, UMN signs (in humans: Parkinsonism and Huntington’s disease/chorea) Paralysis: Here: Loss of voluntary muscle control resulting in partial or complete loss of movement. (Other forms of paralysis such as muscular, synaptic etc. are also known). Paresis: Here: Muscular weakness of neural origin (less severe than paralysis). 40 DISTURBANCES IN CORTICAL MOTOR FUNCTION 1. 1, SEIZURE (FIT) Paroxismal, transient disturbance of consciousness, usually accompanied by abnormal somatic and visceral motor activity. Sudden onset, cease spontaneously, tend to occur repeatedly often in "clusters". Originate as bursts of activity from neurons in the cerebrum, diencephalon or in the reticular formation (ARAS) of the brainstem, and may be associated with organic lesions (neoplasms, abscesses) or induced by metabolic disturbances (NH3 toxicosis, hypoglycemia) and emotional effects. Phases: prodromal stage, aurea, ictus, postictus (interictus: time between seizures) Widely known form: epileptoform seizure, epilepsy (narcolepsy is also known). For details see Internal Medicine! 41 Epilepsy 42 Narcolepsy Transient status; a sudden fall in sleep (REM /rapid eye movement/phase). A neurological sleep disorder. More common in humans; in dogs rarely occurs. Orexin-mediator releasing disorder (in humans) or orexin-mediator binding disorder (in dog) 43 DISTURBANCES IN CORTICAL MOTOR FUNCTION 2. 2, INCOORDINATION OF MOVEMENT WITHOUT SEIZURES The control of body movement involves the complex interaction of several parts of CNS (cerebrum, midbrain, brainstem, cerebellum, vestibular system, spinal cord). A disturbance in control of voluntary movement means: – skilled/learned movements – ataxia (unsteady or irregular gait, incoordination): CEREBRAL/CORTICAL/PROPRIOCEPTIVE ATAXIA (often together with behavioural changes i.e. apathy, depression) – muscular weakness – involuntary movements, tendency to walk in large circles – no head tilt 45 CORTICAL SENSORY AND BEHAVIOURAL DISTURBANCES 1. Decreased olfactory, visual, hearing, touching sensation and conscious proprioception (centers are located in the cortex) 2. Behavioural disorders (thalamocortex!): • excitament, agressivity, hypersexuality; • loss of learned habits (i.e. in house-trained pets) • depression, dementia • disturbances in consciousness: semi-comatose and comatose state These sensory/behavioural changes are frequently associated with signs of ataxia but rarely with muscular weakness. 46 DYSFUNCTIONS OF THE BRAINSTEM 1. DIENCEPHALON Diencephalon is the most rostral (cranial) part of the brainstem 1. Hypothalamic dysfunctions autonomic functional disturbances in the regulation of: appetite, thirst, body temperature, endocrine organs 47 DYSFUNCTIONS OF THE BRAINSTEM 1. DIENCEPHALON - con’t 2. Dysfunctions of thalamus – The relay center, “Thalamocortex” –contralateral deficits in sensory functions: vision, proprioception, pain –motor dysfunctions (thalamus relays motor information from the cerebellum and extrapyramidal nuclei to the cortex: contralateral dysmetria –disturbances of consciousness (thalamus is a part of the ascending reticular activating system, ARAS): loss of consciousness, convulsions –behavioural changes (thalamus is connected to the limbic system*): emotional and behavioral abnormalities * The limbic system has hypothalamic connections, hypothalamus has regulative function in the visceral components of the emotional reactions. 48 Ascending reticular activation system - ARAS 49 DYSFUNCTIONS OF THE BRAINSTEM 1. DIENCEPHALON - con’t 2. Dysfunctions of thalamus – The relay center, “Thalamocortex” –contralateral deficits in sensory functions: vision, proprioception, pain –motor dysfunctions (thalamus relays motor information from the cerebellum and extrapyramidal nuclei to the cortex: contralateral dysmetria –disturbances of consciousness (thalamus is a part of the ascending reticular activating system, ARAS): loss of consciousness, convulsions –behavioural changes (thalamus is connected to the limbic system*): emotional and behavioral abnormalities * The limbic system has hypothalamic connections, hypothalamus has regulative function in the visceral components of the emotional reactions. 50 Cortex cingulate septal Dienceph. Thal. Hypothal., hypocampus, amygdala Rostral part of barin stem DYSFUNCTION OF THE BRAINSTEM 2. MIDBRAIN (MESENCEPHALON) DYSFUNCTIONS 1. Disturbances in the function of ARAS (reticular formation, functions to stimulate the cerebral cortexx) damage causes: unconsciousness, semi-comatose/comatose state 2. Disturbances in the function of oculomotor nucleus with the connections of the pontine and the medullary (medulla oblongata) reticular formation 3. Formatio reticularis pontine reticular formation: stimalator of the extensor muscle tone medullary reticular formation : inhibitory influence of extensor muscle tone 52 Severe damage: may develop when intracranial pressure increases and causes unconsciousness (ARAS), opisthotonus (UMN-signs), ventrolateral strabismus with fixed dilated pupils (Oculomotor nucl.) Less severe damage: Depression (ARAS) spastic tetra- or hemiparesis (causes milder UMN signs); pupils are asymmetrical or bilaterally miotic (Oculomotor nucl.) 53 DYSFUNCTIONS OF THE PONS AND THE MEDULLA OBLONGATA • Lesions of motor neurons of this area cause UMN signs (ataxia, spastic paresis, hyperreflexia) of all four limbs (BSE!) - ipsilateral signs if unilateral lesion exists • Simultaneous deficits of cranial motor nerves V to XII (LMN signs – flaccid paresis/paralysis!) • As medullary and pontine areas control vital centres for respiration, blood pressure and heart rate, ARAS - damage of these areas causes life-threatening consequences A sample cut for BSE analysis 54 Cerebellum 55 CEREBELLAR DYSFUNCTIONS The cerebellum regulates and coordinates voluntary movements, monitors information from various parts of CNS concerning body position and movement. Damage of the cerebellum causes: ataxia without weakness (hypermetria, truncal ataxia, tremor, opisthotonus, - exaggeration of movements) – ipsilateral!! vestibular signs (loss of equilibrium, abnormal nystagmus) intention(al) tremor (a tremor that occurs when a voluntary movementv is attempted) Absence of menace response (with vision!!!!!) Symptoms due to the damage of different cerebellar regions: Vermix damage: ataxia, circling Frontal lobe damage: incoordination, stride (straddle) stand Posterior (occipital) lobe damage: tremor 56 Cerebellar diseases - video Malfunctions of cranial nerves Skipped exept vestibulocohlear nerve See Internal Medicine Diagnostics DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 1. CN I. (nervus olfactorius/ olfactory nerve)Anosomia (absence of the sense of smell) CN II. (nervus opticus/optical nerve) This nerve is the sensory path for vision and the pupillary light reflexes no menace response (eye blink and averted head as a result of a threatening gesture) no direct and indirect pupillary light reflex (as a result of light there is a pupillary constriction (miosis) - due to 60 parasympathetic fibers of CN III.) DYSFUNCTIONS OF THE CRANIAL NERVES 2. CN III. (nervus oculomotorius) Decreased function of: 1. parasympathetic motor fibers for pupillary constriction pupil is constantly dilated (mydriasis) 2. general somatic efferent fibers for motor control of the extraocular muscles - dorsal, medial, ventral recti and ventral oblique; motor pathway of m. levator palpebrae fixed ventrolateral strabismus, dropping of the upper eyelid (ptosis) CN IV. (nervus trochlearis/trochlear nerbe) Decreased function of: motor pathway to the dorsal oblique muscle of eye, which normally rotates the dorsal pole of the eye towards the midline - outward rotation of the dorsal pole of the eye 61 DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 3. CN V. (nervus trigeminus/trigeminal nerve) 1. motor division dysfunctions: mandibular, masseter, temporal, rostral digastric, pterygoid, and mylohyoid muscles dropped jaw, drooling saliva, inability to prehend and chew 2. sensory division dysfunctions: a, ophtalmic branch dysfunction absence of the palpebral reflex (blink response by touching the eyelid, medial canthus) no corneal reflex (by gently touching the cornea the eyeball retracts, third eyelid flicks across) b, maxillary branch dysfunction - no palpebral reflex by touching the lateral canthus c, mandibular branch dysfunctions no sensation in lower jaw and cheeks 62 DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 4. CN VI. (nervus abducens/abducens nerve) Dysfunction of the lateral rectus and retractor bulbi muscles medial deviation of the eyeball (strabismus convergens) suppression of the corneal reflex exophtalmus 63 DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 4. CN VII. (nervus facialis/facial nerve) 1. Dysfunction of the motor pathway of the facial muscles (facial expression), (hemi)paresis of facial muscles (mimetic muscles) dropped eyelid, ear, (in case of hemiparesis the nose and upper lip will be drown towards the normal side) menace and palpebral reflex deficiencies involuntary retraction of the eyeball which serves to bring the third eyelid across the eye 2. Sensory dysfunctions of the tongue (taste) 64 DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 5. CN VIII. (nervus vestibulocochlearis) 1. Cochlear division dysfunctions: uni- or bilateral deafness 2. Vestibular division dysfunctions: a) Disorders in maintening the position of the eyes, trunk, limbs imbalance, disorientation (vestibular sensory pathway: receptor cells /inner ear/ - CN. VIII vestibular nuclei of the medulla oblongata or cerebellum) Connections with the vestibular nuclei: 1. spinal cord (vestibulospinal tract) 2. brainstem (medial longitudinal fasciculus) 3. cerebellum a) Disorders of the vomiting center 65 Consequences of unilateral vestibular disease - VESTIBULAR ATAXIA without weakness, due to loss of equilibrium - circling, rolling toward the side of the lesion (ipsilateral) - head tilt, postural abnormalities (ipsilateral) - hypertonia of muscles, hyperreflexia on the side opposite of the lesion (i.e. contralateral, due to removal of the inhibitory contralateral UMN vestibulospinal influence) - vestibular nystagmus (involuntary rhythmic oscillation of the eyeball whenever head moves normally) - abnormal nystagmus: spontaneous and positional nystagmus that occurs while the head is not moving - vestibular strabismus (ventral deviation of the eyeball on the affected side) 66 Vestibular ataxia DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 6. CN IX. (nervus glossopharyngeus/glossopharingeal nerve) Dysfunctions of the motor pathway of the pharynx, zygomatic and parotid glands, sensory difficulties at the caudal one-third of the tongue and pharyngeal mucosa loss of gag reflex, loss of taste and dryness of tongue pharyngeal asymmetry CN X. (nervus vagus/vagal nerve) Dysfunctions of the motor pathway of the pharynx, larynx, palate, and parasympathetic motor pathways to the viscera of the body Sensory dysfunctions of the caudal pharynx, larynx and viscera of the body Symptoms: dysphagia, megaesophagus, vocalization defects and 68 tachycardia DYSFUNCTIONS OF THE CRANIAL NERVES (CN) 7. CN XI. (nervus accessorius/accessory nerve) Dysfunction of the motor pathway of the trapezius, sternocephalicus and brachiocephalicus muscles - no typical signs CN XII (nervus hypoglossus/hypoglossal nerve) Dysfunction of the intrinsic and extrinsic muscles of tongue. - paralysis, atrophy 69 Spinal cord disorders 70 SPINAL CORD DYSFUNCTIONS 1. Upper cervical zone (comprises cord segment C1 to C4, which is at the anterior level to the brachial plexus) Lesion causes: – UMN signs of all four limbs (spastic tetraparesis/paralysis) – ataxia, hypertonia, hyperreflexia, weakness (tetraparesis), – reduced conscious proprioception, respiratory failure – (ataxia is more severe in the hindlimbs: wobbler-syndrome, CVI=cervical vertebral instability) 71 SPINAL CORD DYSFUNCTIONS 1. Cervicothoracic zone (extends from C5 to T2; includes the origin of the brachial plexus) Lesion causes: – LMN signs in the forelegs/-limbs, UMN signs in the hindlegs – Pain sensation (hypo-/anaesthesia) 72 SPINAL CORD DYSFUNCTIONS 2. Thoracolumbar zone (extends from T3 to L3; includes no major peripherial nerves) Lesion causes: • UMN signs in the hindlegs, suppression of pain perception • (forelimbs are not affected, except Schiff-Sherrington phenomenon) 73 SPINAL CORD DYSFUNCTIONS 2. Thoracolumbar zone (in fact upper thoracic region damagae) (in the L2 – L4 segment there are „border neuron cells”) Lesion causes: Schiff-Sherrington phenomenon UMN signs in the forelegs/-limbs, LMN signs in the hindlimbs 74 SPINAL CORD DYSFUNCTIONS 2. Lumbosacral zone (extends from L4 to S2; origin of the major nerves of hindlimbs, perineum and pelvic viscera) Lesions cause: cauda equina complex (CEC or CES) • LMN signs in the hindlimbs, perineum and adversely affected bladder function • increased pain sensation (hyperaesthesia) of pelvic limbs, tail and perineum 75 SPINAL CORD DYSFUNCTIONS 2. Sacrococcygeal zone (extends from S3 to Co segments; controls the tail movement) Lesions cause: –hypotonia/weakness of the tail –reduced pain perception 76 SPINAL CORD DYSFUNCTIONS 3. SUMMARY 1. Consequences of dysfunctions in afferent (sensory) tracts: a) hypoesthesia, anesthesia b) hyperesthesia c) paresthesia d) extension of the pain perception according to the dermatomes (Head`s zones or areas) Sir Henry Head: English neurologist, 1861-1940 77 SPINAL CORD DYSFUNCTIONS 3. SUMMARY 2. Consequences of dysfunctions in efferent (motor) tracts: a, mainly LMN signs: flaccid paresis (paralysis), areflexia, reduced muscular tone b, UMN signs: hyperreflexia, increased muscular tone (spastic paralysis) ATAXIA IS ALSO COMMON (SPINAL ATAXIA) 78 Spinal ataxia - video SPINAL CORD DYSFUNCTIONS 3. con’t DISTURBANCES IN URINATION (MICTURITION) AND DEFECATION a) UMN signs: loss of cortical and supracortical effects incontinence, abnormal positioning/posture during urination b) LMN signs: decreased muscular tone of the urinary bladder, anal muscles, and tail Detrusor – n. pelvicus parasymp Sphincter – n. pudendalis Sympathetic innervation (L1-L4) -receptors: increase sphincter muscle tone -receptors: promote relaxation of the bladder wall 80 SPINAL CORD DYSFUNCTIONS 3. con’t Cauda equina – CES (cauda equina syndrome) 81