Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Complement system wikipedia , lookup
Duffy antigen system wikipedia , lookup
Immunocontraception wikipedia , lookup
DNA vaccination wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Adaptive immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
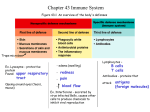
Summary of previous lesson Alveolar (Lung) Macrophage Attacking E. coli (SEM x10,000) © Dr Dennis Kunkel (used with permission) Macrophage Attacking E.coli (SEM x8,800) © Dr Dennis Kunkel I. Chain of Infection Horton & Parker: Informed Infection Control Practice HOST DEFENSE MECHANISMS Lecture nr. 6 Antigens. Antibodies. Immune response. Cell cooperation and mediators in immune response. 15.03.2011 HOST DEFENSE MECHANISMS Definitions of the Immunity Immunity: “Free from burden”. Ability of an organism to recognize and defend itself against specific pathogens or antigens. Immunity refers to the ability of the human body to resist disease agents and their toxins through possession of antibodies. Immunity is a long lasting protection against a specific antigen. Specific Host Defenses: The Immune Response T-cell (part of the specific immune response) The structure of immunoglobulins The Immune Response Immune Response: Third line of defense. Involves production of antibodies and generation of specialized lymphocytes against specific antigens. What is the immune system? The body’s defense against disease causing organisms, malfunctioning cells, and foreign particles How does the immune system respond to different infections? Microbes are recognized by two mechanisms: evolved broad recognition mechanisms (innate immunity), and by highly specific lymphocyte antibodies and T cell receptors (adaptive immunity) Different types of microbes are eliminated by different effectors mechanisms, which are designed to best combat each type of microbe Classification of immunity Characteristics of Innate and Adaptive Immunity Innate Immunity Acquired Immunity Antigen independent Antigen dependent Immediate Take time Genetically determined No Immunologic memory Not genetically determined. Development of memory Classification of the immunity Acquired Immunity: Obtained in the course of daily life. A. Naturally Acquired Active Immunity: Antigens or pathogens enter body naturally. Body generates an immune response to antigens. Immunity may be lifelong (chickenpox or mumps) or temporary (influenza or intestinal infections). B. Naturally Acquired Passive Immunity: Antibodies pass from mother to fetus via placenta or breast feeding (colostrum). No immune response to antigens. Immunity is usually short-lived (weeks to months). Protection until child’s immune system develops. Classification of the immunity II. Artificially Acquired Immunity: Obtained by receiving a vaccine or immune serum. 1. Artificially Acquired Active Immunity: Antigens are introduced in vaccines (immunization). Body generates an immune response to antigens. Immunity can be lifelong (oral polio vaccine) or temporary (tetanus toxoid). 2. Artificially Acquired Passive Immunity: Preformed antibodies (antiserum) are introduced into body by injection. Snake antivenom injection from horses or rabbits. Immunity is short lived (half life three weeks). Host immune system does not respond to antigens. Significance of the Immune System Beneficial: Protection from Invaders Elimination of Altered Self Detrimental: Discomfort (inflammation) Damage to self (autoimmunity) Components of Human Immune System Cells of the immune system Lymphocytes Mediators of adaptive immune responses; only cells with specific receptors for antigens Antigen-presenting cells (APCs) Specialized to capture, concentrate, and display antigens for recognition by lymphocytes Dendritic cells; macrophages, B cells; follicular dendritic cells Different APCs serve different roles in adaptive immune responses Effector cells Function to eliminate microbes; include lymphocytes, granulocytes (neutrophils, eosinophils), macrophages Lymphocytes Originate : in liver, spleen and bone marrow of fetus in bone marrow after birth From stem cells – hemocytoblasts – that produce all blood cells. Lymphocytes To become mature, immunocompetent cells, they must pass through lymphoid tissues in other parts of the body. As they do so, they become committed to becoming either T cells or B cells 1. Cells that migrate through the bone marrow (bursal equivalent) become B cells, and will produce antibodies and participate in humoral immunity. 2. Cells that migrate through the thymus glands become T cells and participate in Cell-mediated immunity. LYMPHOCYTE DEVELOPMENT Congenital immunodeficiency diseases are often caused by blocks at different stages of lymphocyte maturation CD Nomenclature • • Structurally defined leukocyte surface molecule that is expressed on cells of a particular lineage (“differentiation”) and recognized by a group (“cluster”) of monoclonal antibodies is called a member of a cluster of differentiation (CD) CD molecules (CD antigens, CD markers) are: • • • • Identified by numbers Used to classify leukocytes into functionally distinct subpopulations, e.g. helper T cells are CD4+CD8-, CTLs are CD8+CD4Often involved in leukocyte functions Antibodies against various CD molecules are used to: • • • Identify and isolate leukocyte subpopulations Study functions of leukocytes Eliminate particular cell populations Two types of T cells CD4 T cells Help other immune cells Recognize peptide + MHC II CD8 T cells Kill virus-infected cells Recognize peptide + MHC I MHC II is expressed primarily on immune cells MHC I is expressed on all nucleated cells Peptides are from endocytosed antigen Peptides are from cytosolic antigen ANTIGENS Antigens An antigen is a molecule that stimulates an immune response. The word originated from the notion that they can stimulate antibody generation. The modern definition includes all substances that can be recognized by the adaptive immune system. Antigens •Antigens - substances recognized as “non-self”. These can be: Infectious agents - bacteria, viruses, fungi or parasites Noninfectious substances – • Environmental - pollen, foods, bee, venoms • Drugs, vaccines, transfusions and transplanted tissues Chemical nature of antigen Proteins Polysaccharides Nucleic acids Lipids Some glycolipids and phospholipids can be immunogenic for T cells and illicit a cell-mediated immune response Antigens Most are proteins or large polysaccharides from a foreign organism. Microbes: Capsules, cell walls, toxins, viral capsids, flagella, etc. Nonmicrobes: Pollen, egg white , red blood cell surface molecules, serum proteins, and surface molecules from transplanted tissue. Lipids and nucleic acids are only antigenic when combined with proteins or polysaccharides. Antigens Antibody Generator The best antigens are: 1. 2. 3. large recognized as foreign complex Antigens can be classified in order of their origins Exogenous antigens - are antigens that have entered the body from the outside, ex. by inhalation, ingestion, or injection. By endocytosis or phagocytosis, these antigens are taken into the antigen-presenting cells (APCs) and processed into fragments. Endogenous antigens - antigens that have been generated within the cell, as a result of: normal cell metabolism, or viral or intracellular bacterial infection. Types of Antigens Allogenic antigen The specific antigen exists in different individuals. Blood type antigens. Autoantigens usually a normal protein (sometimes DNA or RNA) that is recognized by the immune system of patients suffering from a specific autoimmune disease. Tumor antigens are presented by the MHC I molecules on the surface of tumor cells. can sometimes be presented only by tumor cells and never by the normal cells. they are called tumor-specific antigens (TSAs) and typically result from a tumor specific mutation. Characteristics of Antigen Immunogenicity The capacity to stimulate the production of antibodies or cell-mediated immune responses. Characteristics of Antigen Antigenicity The ability to bind antibody. Complete antigen Incomplete antigen, also known as hapten. Hapten: Small foreign molecule that is not antigenic. Must be coupled to a carrier molecule to be antigenic. Once antibodies are formed they will recognize hapten. Antigens Epitope or, Antigenic determinants: Small part of an antigen that interacts with an antibody. Any given antigen may have several epitopes. Each epitope is recognized by a different antibody and may interact with them by paratopes of Antibody Epitopes: Antigen Regions that Interact with paratopes, Antibodies regions Types of Epitopes 1. Linear epitopes continuous and found in polysaccharides as well as in both native (nondenatured) and denatured proteins, especially fibrillar proteins. specificity depends upon primary sequence. typical size is 5-6 subunits in length. Types of Epitopes 2. Conformational epitopes Discontinuous involve multiple subunits, often located far apart in the primary sequence of the antigen molecule and are thus found only in native (globular) proteins. Antigenic epitopes ANTIBODY Antibodies Proteins that recognize and bind to a particular antigen with very high specificity. Made in response to exposure to the antigen. One virus or microbe may have several antigenic determinant sites, to which different antibodies may bind. Each antibody has at least two identical sites that bind antigen: antigen binding sites. Valence of an antibody: Number of antigen binding sites. Most are bivalent. Belong to a group of serum proteins called immunoglobulins (Igs). Antibody Structure Monomer: A flexible Y-shaped molecule with four protein chains: 2 identical light chains 2 identical heavy chains Variable Regions: Two sections at the end of Y’s arms. Contain the antigen binding sites (Fab). Identical on the same antibody, but vary from one antibody to another. Constant Regions: Stem of monomer and lower parts of Y arms. Fc region: Stem of monomer only. Important because they can bind to complement or cells. Immunoglobulins IgG - monomer IgA – dimer – 2 units IgM – pentamer – 5 units IgD – monomer IgE – monomer I. IgG Structure: Monomer Percentage serum antibodies: 80% Location: Blood, lymph, intestine Half-life in serum: 23 days Complement Fixation: Yes Placental Transfer: Yes Known Functions: Enhances phagocytosis, neutralizes toxins and viruses, protects fetus and newborn. II. IgM Structure: Pentamer Percentage serum antibodies: 5-10% Location: Blood, lymph, B cell surface (monomer) Half-life in serum: 5 days Complement Fixation: Yes Placental Transfer: No Known Functions: First antibodies produced during an infection. Effective against microbes and agglutinating antigens. III. IgA Structure: Dimer Percentage serum antibodies: 10-15% Location: Secretions (tears, saliva, intestine, milk), blood and lymph. Half-life in serum: 6 days Complement Fixation: No Placental Transfer: No Known Functions: Localized protection of mucosal surfaces Provides immunity to infant digestive tract. IV. IgD Structure: Monomer Percentage serum antibodies: 0.2% Location: B-cell surface, blood, and lymph Half-life in serum: 3 days Complement Fixation: No Placental Transfer: No Known Functions: In serum function is unknown. On B cel surface, initiate immune response. V. IgE Structure: Monomer Percentage serum antibodies: 0.002% Location: Bound to mast cells and basophils throughout body. Blood. Half-life in serum: 2 days Complement Fixation: No Placental Transfer: No Known Functions: Allergic reactions. Possibly lysis of worms. Clonal Selection of B Cells is Caused by Antigenic Stimulation Secretions the Antibodies by B cells B cells develop from stem cells in the bone marrow of adults (liver of fetuses). After maturation B cells migrate to lymphoid organs (lymph node or spleen). Clonal Selection: When a B cell encounters an antigen it recognizes, it is stimulated and divides into many clones called plasma cells, which actively secrete antibodies. Each B cell produces antibodies that will recognize only one antigenic determinant. Apoptosis Programmed cell death (“Falling away”). Human body makes 100 million lymphocytes every day. If an equivalent number doesn’t die, will develop leukemia. B cells that do not encounter stimulating antigen will self-destruct and send signals to phagocytes to dispose of their remains. Many virus infected cells will undergo apoptosis, to help prevent spread of the infection. Antigen presenting cells Antigens must be processed in order to be recognised by T cells T Y Soluble native Ag Cell surface native Ag Soluble peptides of Ag Cell surface peptides of Ag presented by cells that express MHC antigens Cell surface peptides of Ag ANTIGEN PROCESSING No T cell response No T cell response No T cell response No T cell response T cell response The interaction of T cells with macrophages requires antigen catabolism Specific T cells T Microbes NO T CELLS NO T CELLS NO T CELLS BIND BIND BIND M 0mins M M T CELLS BIND M 60mins T cell do not bind stably to antigen presenting cells unless the antigen is catabolised Summary • T and B cells recognise antigen differently • Antigen must be catabolised before T cells can recognise it • Antigen processing generates antigenic peptides • Exogenous antigen processing takes place in lysosomes • Endogenous processing is non-lysosomal • The mechanism of antigen processing depends upon the compartment in which the pathogen replicates • Endogenous and exogenous antigen processing both involve uptake, degradation, complex formation and presentation • Pathogens can evade immunity by disrupting antigen processing Immune response Duality of Immune System I. Humoral (AntibodyMediated) Immunity I. II. Cellular (Cell Mediated) Immunity I. Humoral (AntibodyMediated) Immunity Involves production of antibodies against foreign antigens. Antibodies are produced by a subset of lymphocytes called B cells. B cells that are stimulated will actively secrete antibodies and are called plasma cells. Antibodies are found in extracellular fluids (blood plasma, lymph, mucus, etc.) and the surface of B cells. Defense against bacteria, bacterial toxins, and viruses that circulate freely in body fluids, before they enter cells. Also cause certain reactions against transplanted tissue. How do antibodies actually help eliminate antigens? Consequences of Antigen-Antibody Binding Antigen-Antibody Complex: Formed when an Ab binds to Ag. Affinity: A measure of binding strength. 1. Agglutination: Antibodies cause antigens (microbes) to clump together. IgM is more effective that IgG. Hemagglutination: Agglutination of red blood cells. Used to determine ABO blood types and to detect influenza and measles viruses. Consequences of Antigen-Antibody Binding 2. Opsonization: Antigen (microbe) is covered with antibodies that enhances its ingestion and lysis by phagocytic cells. 3. Neutralization: IgG inactivates viruses by binding to their surface and neutralize toxins by blocking their active sites. Consequences of Antigen-Antibody Binding 4. Antibody-dependent cell-mediated cytotoxicity: Used to destroy large organisms (e.g.: worms). Target organism is coated with antibodies and bombarded with chemicals from nonspecific immune cells. 5. Complement Activation: Both IgG and IgM trigger the complement system which results in cell lysis and inflammation. Consequences of Antibody Binding Immunological responce Primary Response: After initial exposure to antigen, no antibodies are found in serum for several days. A gradual increase in titer, first of IgM and then of IgG is observed. Most B cells become plasma cells, but some B cells become long living memory cells. Gradual decline of antibodies. Immunological responce Secondary Response: Subsequent exposure to the same antigen displays a faster and more intense antibody response. Increased antibody response is due to the existence of memory cells, which rapidly produce plasma cells upon antigen stimulation. Antibody Titer: The amount of antibody in the serum. Antibody Response After Exposure to Antigen Duality of Immune System I. Humoral (AntibodyMediated) Immunity I. II. Cellular (Cell Mediated) Immunity II. Cellular (Cell Mediated) Immunity Involves specialized set of lymphocytes called T cells that recognize foreign antigens on the surface of cells, organisms, or tissues: Helper T cells Cytotoxic T cells T cells regulate proliferation and activity of other cells of the immune system: B cells, macrophages, neutrophils, etc. Defense against: Bacteria and viruses that are inside host cells and are inaccessible to antibodies. Fungi, protozoa, and helminths Cancer cells Transplanted tissue T Cells and Cell Mediated Immunity Antigens that stimulate this response are mainly intracellular. Requires constant presence of antigen to remain effective. Unlike humoral immunity, cell mediated immunity is not transferred to the fetus. Cytokines: Chemical messengers of immune cells. Over 100 have been identified. Stimulate and/or regulate immune responses. Interleukins: Communication between WBCs. Interferons: Protect against viral infections. Chemokines: Attract WBCs to infected areas. T Cells and Cell Mediated Immunity T cells are key cellular component of immunity. T cells have an antigen receptor that recognizes and reacts to a specific antigen (T cell receptor). T cell receptor only recognize antigens combined with major histocompatability (MHC) proteins on the surface of cells. MHC Class I: Found on all cells. MHC Class II: Found on phagocytes. T Cells Only Recognize Antigen Associated with MHC Molecules on Cell Surfaces Cells and Cell Mediated Immunity Types of T cells 1. T Helper (TH) Cells: Central role in immune response. Most are CD4+ Recognize antigen on the surface of antigen presenting cells (e.g.: macrophage). Activate macrophages Induce formation of cytotoxic T cells Stimulate B cells to produce antibodies. Central Role of Helper T Cells Types of T cells (Continued) 2. Cytotoxic T (Tc) Cells: Destroy target cells. Most are CD4 negative (CD4 -). Recognize antigens on the surface of all cells: Kill host cells that are infected with viruses or bacteria. Recognize and kill cancer cells. Recognize and destroy transplanted tissue. Release protein called perforin which forms a pore in target cell, causing lysis of infected cells. Undergo apoptosis when stimulating antigen is gone. Cytotoxic T Cells Lyse Infected Cells Types of T cells (Continued) 3. Delayed Hypersensitivity T (TD) Cells: Mostly T helper and a few cytotoxic T cells that are involved in some allergic reactions (poison) and rejection of transplanted tissue. 4. T Suppressor (Ts) Cells: May shut down immune response. Nonspecific Cellular Components 1. Activated Macrophages: Stimulated phagocytes. Stimulated by ingestion of antigen Larger and more effective phagocytes. Enhanced ability to eliminate intracellular bacteria, virus-infected and cancerous cells. 2. Natural Killer (NK) Cells: Lymphocytes that destroy virus infected and tumor cells. Not specific. Don’t require antigen stimulation. Not phagocytic, but must contact cell in order to lyse it. B and T cells mediate specific immunity B cells Matures in Type of immunity Secretes Antigen receptor Where found bone marrow humoral antibodies surface Ig spleen Targets bacteria, viruses Yes Memory T cells thymus cell-mediated cytokines T cell receptor blood, lymph nodes infected cells, tumor cells? Yes Cellular Interactions in the Immune Response Antigen-Presenting cells (macrophages) place antigen on their cell surface in combination with the MHC II complex Ag is presented to a specific helper T cell that has receptors that bind the Ag – MHC II complex After binding, the APC produces Interleukin -1 (IL-1) which stimulates the TH Cell to produce IL-2 and/or IL-4 Interleukin-2 has an autocrine function, causes TH Cell to clone itself, and make more IL-2 and /or IL-4 Central Role of Helper T Cells Helper T cells TH1 cells produce IL -2 and IFN-ɣ and influence cell-mediated immunity TH2 cells produce IL -4 (and other IL’s) and influence antibody-mediated (humoral) immunity When B cell comes in contact with the antigen and IL-4, the B cell produces plasma cells and memory cells Tc Cells come in contact with the antigen on the surface of infected cells in combination with the MHC 1 complex. When also have binding with IL-2, cells produce activated Tc Cells and memory cells. Relationship Between CellMediated and Humoral Immunity Antibody Production T-Dependent Antigens: Antibody production requires assistance from T helper cells. A macrophage cells ingest antigen and presents it to TH cell. TH cell stimulates B cells specific for antigen to become plasma cells. Antigens are mainly proteins on viruses, bacteria, foreign red blood cells, and hapten-carrier molecules. T-Independent Antigens: Antibody production does not require assistance from T cells. Antigens are mainly polysaccharides or lipopolysaccharides with repeating subunits (bacterial capsules). Weaker immune response than for T-dependent antigens. Humoral Response to T Dependent Antigens Overview of the Immune Response Principal mechanisms of defense against microbes Antibodies Phagocytes T cells (CTLs) (may work with antibodies, T cells) All microbes All microbes Intracellular microbes, esp. viruses Disorders of Immunity Hypersensitivity Exaggerated Immune Response Hypersensitivity Types Allergy Exogenous, non-human antigen Isoimmunity (alloimmunity) Exogenous, human antigen Autoimmunity Endogenous antigen Hypersensitivity Mechanisms Type I: IgE mediated Type II: Tissue specific Type III: Immune complex mediated Type IV: Cell mediated Type I Immediate hypersensitivity IgE mediated Exogenous antigen Most (but not all) Allergies Type I: Mechanism Repeated antigen exposure causes increased IgE production IgE binds to mast cells Sensitization occurs Type I: Mechanism Antigen binds to IgE on mast cell membrane Mast cell releases histamine, chemotaxic factors Inflammatory response occurs Type I: Signs/Symptoms Clinical signs, symptoms = response to histamine release GI, skin, respiratory system High mast cells numbers Most sensitive Type I: Signs/Symptoms Histamine effects Vasodilatation Increased capillary permeability Non-vascular smooth muscle spasm Type I: Signs/Symptoms Skin: flushing, itching, edema, urticaria Respiratory: bronchospasm, laryngospasm, laryngeal edema Cardiovascular: tachycardia, hypotension GI: nausea, vomiting, cramping, diarrhea Type I: Atopia “Allergy prone” individuals Genetic predisposition More IgE More mast cell receptors for antibodies than normal Type I: Anaphylaxis Severe, generalized Type I reaction Life-threatening Loss of airway Ventilatory failure Hypoperfusion Type II Tissue specific Reaction to tissue-specific antigens Causes target cell destruction, dysfunction Exogenous or endogenous antigen Type II Most commonly affected cells Red blood cells Thyroid cells Type II: Mechanisms Antibody binds to cell membrane, triggers compliment-mediated lysis Examples Reaction to transfused blood Hemolytic disease of newborn Type II: Mechanisms Antibodies promote target cell clearance by macrophages Type II: Mechanisms Antibodies bind to target cells and cytotoxic T-cells Trigger release of toxins to destroy target cells Type II: Mechanisms Antibody binds to cell membrane, causes alterations in target cell function Example: Graves' disease Antibody binds to thyroid cell membrane Mimics Thyroid Stimulating Hormone action Causes production of excessive amounts of thyroid hormone Results in common form of hyperthyroidism Type III Mediated by antigen/ antibody complex deposition in tissues Exogenous or endogenous antigen Type III: Mechanism Ag-Ab complex deposited in tissues Especially sensitive tissues are blood vessels, GI, respiratory system Causes complement activation, increased neutrophil activity Neutrophils have trouble digesting complexes, release lysosomes causing damage Type III Immune complex quantity varies over time Symptomatic periods alternate with periods of remission Type III: Serum Sickness Repeated intravenous antigen injections Immune complexes deposited in tissues Fever, rash, pain, lymphadenopathy Type III: Raynaud’s Phenomenon Temperature governs immune complex deposition in peripheral circulation Exposure to cold causes redness, pain of fingers, toes followed by numbness, cyanosis, gangrene Type III: Arthus Reaction Occurs after repeated LOCAL exposure to exogenous antigen Immune complexes in vessel walls Examples Celiac disease from wheat protein Hemorrhagic alveolitis from moldy hay inhalation Type IV Delayed Mediated by Td (lymphokine-producing) or Tc (cytotoxic) cells No antibody involved Type IV Examples Graft rejection Contact allergic reactions (poison ivy) Hypersensitivity Targets Allergins Pollen (hay fever) Drug reactions Foods THANK YOU!