Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epigenetics of depression wikipedia , lookup
Copy-number variation wikipedia , lookup
Genomic imprinting wikipedia , lookup
Oncogenomics wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Point mutation wikipedia , lookup
Genome evolution wikipedia , lookup
Genetic engineering wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Public health genomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Gene desert wikipedia , lookup
Epigenetics in learning and memory wikipedia , lookup
Gene nomenclature wikipedia , lookup
Genome (book) wikipedia , lookup
Gene therapy wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
History of genetic engineering wikipedia , lookup
Gene expression programming wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Gene expression profiling wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Microevolution wikipedia , lookup
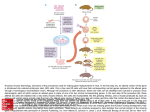
FTO and IRX3 Genes: What Research Shows The official name of this gene is “fat mass and obesity associated.” In 2007, an international team of researchers proclaimed that they had discovered the first genetic variant linked to increased obesity risk. People with two copies of the FTO gene were 3 kilograms heavier than those without the gene. About 16% of people of European descent have two copies of the gene. Female mice with two copies of the FTO gene became 22% heavier than normal female mice after 20 weeks on a standard diet. Male mice with two copies of the FTO gene became 10% heavier than normal mice. Mice with FTO overactivity ate more food than normal mice, which was believed to account for the weight gain. It was found that individuals with variations in obesity genes eat more meals and snacks, consume more calories per day, and have a greater preference for high-fat and sugary foods. However, the researchers emphasize that having these genetic traits does not mean that obesity is inevitable. Making good lifestyle choices still will have a large impact on body weight and composition. Individuals with a variant of the FTO and brain-derived neurotrophic factor (BDNF) genes are at a higher risk for becoming obese. Both genes are expressed in the hypothalamus, where eating and appetite are controlled. Individuals with BDNF variations consumed more servings from dairy, meat, eggs, nuts, and beans, and also ate about 100 more calories a day, compared to those without the variation. Recent research has found that FTO interacts with the IRX3 gene. It appears that the IRX3 gene is the functional obesity gene, while the FTO gene itself appears to have only a peripheral effect on obesity. It was found that disabling the FTO gene in mice does not lead to obesity and that not all humans with FTO variants are obese. IRX3 seems to control body mass and regulate body composition. Mice without the IRX3 gene were significantly leaner than their normal counterparts. They weighed about 30% less, primarily through reduced fat, despite normal levels of caloric intake and physical activity. In fact, mice without the IRX3 gene retained the same weight and fat levels on a high-fat diet that they did on a normal diet. To the contrary, mice with the IRX3 gene gained almost twice as much fat when fed the high-fat diet. The fat cells in the IRX3-deficient mice were smaller, the mice had more brown fat, and they were better able to metabolize glucose. Elderly people with a common variant of FTO were found to have low blood concentrations of leptin (the satiety hormone) and high levels of ghrelin (the hunger hormone). In fact, the elderly individuals with the variant had ghrelin levels about 9% higher and leptin levels about 11% lower than those without the variant. FTO indirectly affects the function on the primary cilium, a hairlike appendage on brain and other cells. The abnormalities of the cilium molecules then increase body weight by affecting the function of leptin receptors. Researchers from the Columbia University Medical Center found that when FTO expression was either increased or decreased, a nearby gene RPGRIP1L also changed expression. RPGRIP1L is known to play a role in regulating the primary cilium, and mutations in the cilium are implicated in rare forms of obesity. When the FTOs’ intron sequence was analyzed, it was found to serve as a binding site for the CUX1 protein, which is a transcription factor that modifies the expression of RPGRIP1L. When mice were bred in a lab to lack one of their two RPGRIP1L genes, they had a higher food intake, gained significantly more body weight, and had a higher percentage of body fat, when compared to controls. In a follow-up experiment, it was found that the RPGRIP1L-deficient mice also had impaired leptin signaling. Some researchers have speculated that obesity is a ciliopathy, such as polycystic kidney disease. University of Alabama at Birmingham researchers speculated that the mutations in the primary cilia might scramble signaling pathways in the hypothalamus and trigger chronic obesity. Mutated primary cilia also seem unable to dock the melanin-concentrating hormone (MCH), which is a key controller of appetite. When the Birmingham researchers looked at genetically modified mice models of Bardet-Biedl syndrome (a ciliopathy that results in obesity, cystic kidneys, blindness, mental deficits, and extra toes and fingers), they found that the mice lost leptin sensitivity when obese, but regained sensitivity when their diet was restricted and they lost weight. These findings indicate that the leptin sensitivity is a secondary consequence, rather than a cause, of the obesity. Previous research from The Ohio State University, found that the MCH receptor, which is involved in appetite regulation, localizes in primary cilia in normal brain cells known to regulate eating behavior. In normal brain cells of the hypothalamus, the MCH receptor is in the primary cilia. However, in the Bardet-Biedl syndrome mice, the MCH receptor was unable to enter the cilium. References and recommended readings American Society for Cell Biology. Is obesity a ciliopathy, triggered by malfunctioning primary cilia? ScienceDaily® Web site. http://www.sciencedaily.com/releases/2011/12/111206131442.htm. Published December 15, 2011. Accessed August 7, 2014. Columbia University Medical Center. Common obesity gene contributes to weight gain. ScienceDaily Web site. http://www.sciencedaily.com/releases/2014/05/140522175252.htm. Published May 22, 2014. Accessed August 7, 2014. Lifespan. ‘Obesity genes’ may influence food choices, eating patterns. ScienceDaily Web site. http://www.sciencedaily.com/releases/2012/05/120523114847.htm. Published May 23, 2012. Accessed August 7, 2014. University of Chicago Medical Center. ‘Master regulator’ of obesity? Distant IRX3 gene appears to interact with obesity-related FTO gene mutations. ScienceDaily Web site. http://www.sciencedaily.com/releases/2014/03/140312150057.htm. Published March 12, 2014. Accessed August 7, 2014. University of Oxford. Overactive FTO gene does cause overeating and obesity. ScienceDaily Web site. http://www.sciencedaily.com/releases/2010/11/101116220332.htm. Published December 6, 2010. Accessed August 7, 2014. Uppsala Universitet. Obesity gene linked to hormonal changes that favor energy surplus. ScienceDaily Web site. http://www.sciencedaily.com/releases/2014/06/140611112746.htm. Published June 11, 2014. Accessed August 7, 2014. Contributed by Elaine Koontz, RDN, LD/N Review Date 8/14 G-2060