Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Apical dendrite wikipedia , lookup
Aging brain wikipedia , lookup
Perception of infrasound wikipedia , lookup
Synaptic gating wikipedia , lookup
Optogenetics wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neuroanatomy wikipedia , lookup
Subventricular zone wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Development of the nervous system wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Circumventricular organs wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Microneurography wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Channelrhodopsin wikipedia , lookup
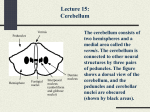
The Cerebellum FARAH NABIL ABBAS MBCHB-MSC-PHD NEUROPHYSIOLOGY Anatomically consists of two hemispheres and vermis it divided by number of fissures into ten lobules and connected to the brain stem by the peduncles. The human cerebellar cortex is actually a large folded sheet, deep beneath the folded mass of cerebellar cortex lies the deep cerebellar nuclei. Cerebellum can not initiate muscle function by itself, instead, it always function in association with other systems of motor control. Basically the cerebellum plays major roles in the timing of motor activities and in rapid, smooth progression from one movement to the next e.x. running, typing, playing the piano, and talking. Cerebellum also helps to control intensity of muscle contraction when the muscle load changes and controls the necessary interplay between agonist & antagonist muscle groups. The cerebellum is recognized as the “silent area of the brain”, because electrical excitation doesn’t cause any sensation and rarely causes any motor movement. Removal of cerebellum, however, does cause movement to be highly abnormal with marked incoordination; however No Paralysis of any muscle could be found. Anatomical Functional Areas of Cerebellum The Anterior Lobe. The Posterior Lobe. The Flocculonodular Lobe along with vestibular system responsible for equilibrium. The center of the cerebellum has a narrow band called the Vermis, it is the area for control of axial body, neck, shoulders and hips muscle movements. Next to vermis, The Intermediate Zone, the site for the distal muscle control especially hands and feet, even more lateral, The Lateral Zone, is situated and is responsible for tiring of coordination of muscle movements with the help of cerebral cortex, its damage leads to in-coordination. Input Pathways to Cerebellum A.Afferent from other parts of brain: 1.From cerebral cortex through the corticosponto cerebellar pathway, the largest source of Mossy fibers which transmit information about muscle movements planned by cortex. 2.From olivary nucleus through olivocerebellar tract. From vestibular apparatus or from brainstem vestibular nuclei through vestibulocerebellar pathway. 3.From reticular formation through the reticulocerebellar pathway. B.Afferents from the periphery: 1.Dorsal spinocerebellar tract, comes mainly from muscle spindle, and apprises the cerebellum about body parts movements, dynamic and static muscle length and tension. 2.Ventral spinocerebellar tract, excited mainly by the motor signals arriving in the anterior horns of spinal cord from brain through corticospinal and rubrospinal tracts and from spinal cord. This pathway informs cerebellum which motor signals have arrived at anterior horns. The Input Arranged into: 1. Climbing Fibers: all originate from inferior olive of medulla, characterized by single prolonged peculiar action potential (complex spike) in each Purkinje cell, these fibers are synapse too. They are the excitatory fibers. 2. Mossy Fibers: characterized by much weaker short duration action potential (simple spike) on Purkinje cell. Many Mossy fibers must be stimulated simultaneously to excite the Purkinje cell. The Mossy fibers are all the other fibers that enter the cerebellum from higher brain, brainstem and spinal cord other fibers that enter the cerebellum from higher brain, brainstem and spinal cord. Output Pathways from Cerebellum 1. From vermis to medullary and pontine regions of brainstem this circuit controls equilibrium along with vestibular nuclei. 2. From Intermediate zone to ventrolateral and ventroanterior nuclei of thalamus, to cerebral cortex, basal ganglia, red nucleus and reticular formation. This complex circuit helps to coordinate reciprocal contractions of agonist and antagonist muscles in limbs especially hands, fingers and thumbs. 3. From lateral zone to dentate nucleus and then to the cerebral cortex. This pathway helps to coordinate sequential motor activities initiated by cerebral cortex. Functional Unit of Cerebellar Cortex Cerebellar Cortex: it has five neurons: Purkinje, Granule, Basket, Stellate, and Golgi cells. The axons of Purkinje cells are inhibitory and are the only output from cerebellar cortex to deep nuclei. The Granule cells (excitatory) receive input from the Mossy fibers and send the bifurcated axons (parallel fibers) to synapse with other cerebellar cortical cells. The Stellate and Basket cells are inhibitory inter-neurons, which synapse with Purkinje cells. Golgi cells are inhibitory inter-neurons which receive input from parallel fibers, Mossy fibers and Purkinje cells and send inhibitory signals to granule cells. Deep Cerebellar Nuclei: They are Dentate, Globose, Emboliform and Fastigle nuclei. Receive excitatory inputs from Mossy and climbing fibers and inhibitory inputs from Purkinje cells. The outputs of deep cerebellar nuclei to brainstem and thalamus and its always excitatory. The Cerebellar Neuronal Circuit Major Features Input-output signals are very rapid and no reverberating. All cerebellar cortical cells are inhibitory except Granule cells are excitatory. All cerebellar cells are constantly active. Climbing fibers inputs exert a strong excitatory effect on single Purkinje cells whereas Mossy fibers inputs exert a weak excitatory effect on many Purkinje cells via the Granule cells in addition to excitation of other cells (Basket and Stellate cells) which are inhibitory to Purkinje cells and Gogli cells which inhibit the transmission from Mossy fibers to Granule cells. The Main Functions of Cerebellum 1.Damping function of the cerebellum i.e. preventing “overshoot” by monitoring, comparing and making corrective adjustments between the signals of higher motor centers and the actual motor response at the level of anterior motor neurons. In cerebellar dysfunction overshooting does occur (Dysmetria or Past Pointing) trying to make corrections to this overshoot, the arm oscillate back and forth several times before it finally fixes on its target (Intention Tremor). 2.Planning, programming and timing the next movement at the same time of present movement with help of motor cortex, sensory cortex and basal ganglia. In cerebellar dysfunction extreme incoordination and failure of progression of the purposeful movements of hands, fingers and feet which is called Dysdiadochokinesia. Speech is also affected (Dysarthria) due to lack of coordination between individual muscles of larynx, mouth and respiratory system, leading to load syllables and others weak, some long, others short. 3.Control of equilibrium: because cerebellum is responsible for controlling the balance between agonist and antagonist muscles during changes if body position. Cerebellar dysfunction leads to Cerebellar ataxia. 4.Control of ballistic movements e.x. movement of fingers in typing or eye movements when reading, the control of these movements are cerebellar functions. 5.Role of cerebellum in predicting the rate of progression of auditory and visual stimuli e.x. a person can predict from the change in visual scenes how rapidly he is approaching an object. Clinical Abnormalities of Cerebellum Dysmetria: an attempt to touch an object with a finger results in overshooting to one side or other. Intention tremor: finger oscillation back and forth - absent at rest and appears whenever patient attempt to perform some voluntary action. Rebound phenomenon: patient inability to "put on brakes", to stop movement promptly (flexion against resistance and sudden release). Clinical Abnormalities of Cerebellum Dysdiadochokinesia: Inability to perform rapidly alternating opposite movements (repeated hand supination and pronation). Hypotonia: muscle tone on side of cerebellar lesion especially when dendate and interposed nuclei were damaged. Nystagmus: Damage of flocculonodular lobe damage rapid eye movements when attempts to fixate eyes on a view to one side of head.