Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
X-inactivation wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Human genetic variation wikipedia , lookup
Genome evolution wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Tay–Sachs disease wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Medical genetics wikipedia , lookup
Point mutation wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Copy-number variation wikipedia , lookup
Gene desert wikipedia , lookup
History of genetic engineering wikipedia , lookup
Gene expression profiling wikipedia , lookup
Gene nomenclature wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Gene expression programming wikipedia , lookup
Genetic engineering wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Gene therapy wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Public health genomics wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Genome (book) wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
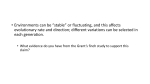
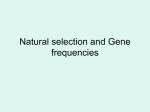
1 Key Medical Terms Associated with Enzymes and Body Chemistry Metabolism is the sum of all the chemical reactions that take place in the cells and the fluids of the body. This includes the absorption of nutrients and minerals, the breakdown and buildup of large molecules, the interconversion of small molecules, and the production of energy from these chemical reactions. Virtually every chemical step of metabolism is catalyzed by an enzyme. Disorders of these enzymes that result from abnormalities in their genes are known as inborn errors of metabolism. Tay-Sachs Disease (TSD) is a autosomal recessive neurodegenerative disease caused by a defective enzyme (hexosaminidase A (Hex-A)) for the breakdown of lipids, particularly the fatty acid derivative called a ganglioside. Hexasaminidase A is a vital hydrolytic enzyme, found in the lysosomes, that breaks down lipids. Babies born with Neuronal lysosomes: Accumulate TSD do not produce the HEX A enzyme lipids due to reduction in breakdown and so harmful quantities of the ganglioside fatty substance of gangliosides accumulates in the liposome’s of their brain cells. The excess accumulation causes nerve cells to bulge, function poorly and die. Usually, the child with this problem appears to be developing normally in the first few months but after about 6 months, it gets worse. Children with this disorder eventually become blind, deaf, mentally retarded and paralyzed, occurring within a year or two and usually die before age 5. Those with less severe forms can affect people into their 20s and 30s. Currently there is no cure or effective way to delay the progression of the disease. TSD is an autosomal recessive genetic disorder, meaning that both parents must be carriers in order to give birth to an affected child. Then, there is a 25% chance with each pregnancy of having a child with TSD. One of the most common initial symptoms is a red spot in the eyes described as a 'cherry-red spot' due to change in the retina at the back of the eye. All babies in the United States and Canada are tested for TSD right after birth. Each year in the U.S. about 1 in 10,000 children are diagnosed with TSD.A review of basic gene transmission can be found at the end of this document. Phenylketonuria (PKU): An autosomal recessive genetic disorder characterized by a mutation in the gene for the liver (hepatic) enzyme phenylalanine hydroxylase (PAH), rendering it nonfunctional. This disorder is the most common genetic disorder of amino acid metabolism affecting about 1 in 10,000 people. This enzyme is necessary to metabolize the amino acid phenylalanine to the amino acid tyrosine. When PAH activity is reduced, phenylalanine accumulates and is converted into phenylketone (hens the name phenylketonuria), which can be detected in the blood and urine. Phenylketone is also known as phenylpyruvate (phenylpyruvic acid). Phenylalanine is an essential amino acid (meaning that it cannot be synthesized in the body and must be taken in through the diet) that is needed for normal growth and development. A blood test is performed to check if a newborn has the PAH enzyme needed to use phenylalanine in his or her body. High blood phenylalanine and phenylketone levels can cause brain damage, seizures, and severe mental 2 retardation. The artificial sweetener aspartame (Equal, NutraSweet), which is added to many diet foods and diet sodas, contains phenylalanine. Federal regulations require that any food that contains aspartame bear this warning: "Phenylketonurics: Contains phenylalanine." This warning helps people with PKU avoid products that are a source of phenylalanine. Symptoms can include mental retardation, hyperactivity, stunted growth, small head size (microcephaly), and fair skin and blue eyes. Reasons for symptoms: Phenylalanine is converted into tyrosine and then to melanin, the pigment responsible for skin and hair color. Therefore, infants with the condition often have lighter skin, hair, and eyes than brothers or sisters without the disease. Tyrosine is the precursor to the neurotransmitters dopamine and norepinephrine (noradrenaline), and to the hormone epinephrine (adrenaline). Dopamine is a major brain neurotransmitter. PKU patients who do not consume enough tyrosine in their diet cannot produce sufficient amounts of dopamine. Low dopamine levels in the brain disrupt normal communication between nerve cells, which results in impaired cognitive (mental) function. Other symptoms may include: Delayed mental and social skills; Head size significantly below normal (microcephaly); Hyperactivity; Jerking movements of the arms or legs; Mental retardation and seizures. The damage caused by PKU can begin weeks after the baby has started drinking breast milk or formula. Babies with PKU need foods low in phenylalanine to prevent severe brain damage. Phenylalanine is found in most foods that have protein, such as milk, cheese, and meats. Albinism: An autosomal recessive genetic disorder that results in a lack of pigment in the skin, hair and eyes. It is caused by a defective gene that provides instructions to make the enzyme called tyrosinase that produces melanin. This enzyme is located in melanocytes, which are specialized cells that produce a pigment called melanin. Tyrosinase is responsible for the first step in melanin production. Through a series of chemical reactions the amino acid tyrosine is converted to melanin in the skin, hair follicles, the colored part of the eye (the iris), and the retina. There is no cure for albinism. One person in 17,000 in the U.S.A. has some type of albinism. Albinism is an autosomal recessive disorder, meaning that both parents must be carriers in order to give birth to an affected child. Then, there is a 25% chance with each pregnancy of having a child with albinism. 3 Galactosemia: A genetic disorder (autosomal recessive) caused by a deficiency in the enzyme that metabolizes galactose. Milk contains various sugars including the disaccharide lactose (glucose attached to galactose) and the monosaccharide galactose. An infant with galactosemia is unable to use (metabolize) the simple sugar galactose, which reaches high levels in the body, causing damage to the liver, central nervous system and various other body systems. An infant with galactosemia may develop jaundice, vomiting, lethargy, irritability and convulsions. The classic form of galactosemia is due to a deficiency of the enzyme galactose-1phosphate uridyl transferase, and, if untreated, it presents in the infant with fatal liver failure. Screening for Galactosemia by blood sample in the first few days of life has been very successful in identifying the disorder, and simple alteration of the diet (replacing milk with formulas that do not contain galactose or lactose) has permitted a generation of individuals to survive with quite normal lives and, in general, normal intellect. Familial Hypercholesterolemia (FH): A genetic disorder resulting is a reduced ability to remove cholesterol from the bloodstream. FH is characterized by high cholesterol levels, specifically very high levels of low-density lipoproteins (LDL, "bad cholesterol"), in the blood and early cardiovascular disease. Lipids, which include cholesterol, are insoluble in water; therefore, they are transported as complexes of lipoproteins. These proteins also serve as ligands (binding groups) to specific receptors that help move the lipoprotein into the cell. If the cells do not make the receptors or have a reduced number of receptors on their surface then the lipid containing lipoproteins are not transported into the cell very well and remain in the blood stream. Familial hypercholesterolemia (FH) is an autosomal dominant pattern of inheritance meaning that one copy of an altered gene in each cell is sufficient to cause the disorder. However this type of expression is considered to be an incomplete dominant or a semidominant trait, which means there are two forms of the disease - the disease exhibits a gene dosage effect. Homozygous individuals (2 bad gene copies) are more severely affected than are heterozygotes (1 bad gene copy). Heterozygotes for FH occur with a frequency of 1 in 500 which makes this disease one of the most common inherited disorders in 4 metabolism. Heterozygous for the FH gene, means they've inherited one defective gene and one healthy gene. Specifically, patients have mutations in the low-density lipoprotein receptor (LDLR) gene that encodes the low density lipoprotein (LDL) receptor protein, which normally removes LDL from the circulation, or apolipoprotein B (ApoB), which is the part of LDL that binds with the receptor. Heterozygotes will have reduced numbers of Low Density Lipoprotein receptors (LDLR) on their cell surfaces and higher-than-normal levels of blood cholesterol. Although they are at increased risk for atherosclerosis and heart disease, symptoms may not develop at all, or not until later in life. Having two abnormal copies (being homozygous) may cause severe atherosclerosis cardiovascular disease in childhood. A child of two heterozygous parents may be homozygous for the disease form of the FH gene. With two defective genes, a homozygous child has a very severe form of the disease and produces few or no LDL receptors. About 1 in 1 million people have this form of the disease. They may have heart attacks as early as age 2 and seldom live to be 20 years old. As circulating levels of lipids rise (hyperlipidemia), cholesterol nodules accumulate around tendons and beneath the skin creating yellow deposits called xanthomas. Specifically, xanthomas are lesions characterized by accumulations of lipid-laden macrophages. Xanthomas can occur in persons of any age, but usually occur in people older than 50 years. They appear anywhere on the body, but are most often seen on the elbows, joints, tendons, knees, hands, feet, or buttocks. Xanthomas may be a sign of a medical condition that involves an increase in blood lipids. Such conditions include diabetes, hyperlipidemia and of course, inherited metabolic disorders such as familial hypercholesterolemia. If you have a disease that causes increased blood lipids, treating the condition may help reduce the development of xanthomas. They can be surgically removed but will return if blood lipid levels remain high. There's so much cholesterol in the blood of FH people that they can develop cholesterol nodules called xanthomas in their skin and tendons. Hyperlipidemia can also result in xanthomas. 5 Genetic Review: Since many of the metabolic disorders are autosomal recessive it is important to have a basic understanding about how this type of inheritance pattern works. The following is a brief review about genes and how they are passed on. We will cover genes and inheritance patterns in more detail during the genetic portion of the class. For now, use this information to help clarify what an autosomal disorder is and then focus primarily on the disorders which you are expected to understand for the upcoming quizzes and exams. The cells of the body contain information, in the form of genes, for the body to make all the necessary structural components and chemicals to ensure normal function. If a gene is changed so that it does not work properly, it is described as defective or faulty. The information contained in the defective gene, and its product, is impaired. The information for our cells to make a specific enzyme is contained within a specific gene(s). To illustrate the inheritance pattern I will use Tay Sach Disease (TSD) as an example which is due to a defective gene for the enzyme called hexosaminidase A (Hex-A). The information for our cells to make the HEX A enzyme is contained in a gene, called the HEX A gene, located on chromosome number 15. We all have two copies of chromosome number 15 in all our body cells which you received from each of your parents, and therefore two copies of the gene that codes for the HEX A enzyme. As there are two copies of each gene, if a person has a change in one copy of their HEX A gene, and the other copy is working, they will still produce sufficient amounts of the HEX A enzyme for normal body function. People who have one working copy of the HEX A gene and one that is defective are called 'carriers' of the change that makes the gene defective or genetic carriers for TSD. Genetic carriers for TSD do not have Tay-Sachs disease and are not affected in any way because they can still produce enough HEX A enzyme. People with TSD have both copies of their HEX A gene as defective: they cannot produce the important HEX A enzyme. Important note about Genetic carriers. Individuals who are genetic carriers for TSD have one working copy of their HEX A gene and one copy that is faulty in every cell. Being a genetic carrier for TSD or any other genetic disorder is not like being a carrier of an infectious virus like hepatitis. Genetic carriers for TSD cannot pass it on to others like a virus. They can, however pass the defective gene on to their children. The effect of the change in the gene is 'recessive' or hidden by the presence of the working copy of the gene. The pattern of inheritance in families of the defective gene causing TSD is therefore described as autosomal recessive inheritance. In Figures 1 and 2 which illustrate the pattern of inheritance, the faulty HEX A gene is represented by 'r'; the working copy by 'R'. There are four possibilities, in every pregnancy, for the combinations of genes passed from the parents. As shown in Figure 1, if a couple are both carriers of the defective HEX A gene, in every pregnancy there is a 1 in 4 chance, or 25%, that they will have a child who inherits both copies of the defective gene from his/her parents. In this case, no working gene product will be produced and their child will be affected by TSD. There is a 1 in 4 chance, or 25%, that their child will inherit both copies of the working gene and will be unaffected by TSD and cannot pass the faulty gene on to their children. There is a 1 in 2 chance (2 in 4 chances), or 50%, that their child will inherit one faulty copy of the gene and one working copy of the gene from each parent and he/she will be an unaffected genetic carrier for TSD, just like the parents. 6 Figure 1: Autosomal recessive inheritance where both parents are carriers of the faulty HEX A gene. The faulty HEX A gene copy is represented by 'r'; the working copy by 'R'. Figure 2: Autosomal recessive inheritance where only one parent is a carrier of the faulty HEX A gene. The faulty HEX A gene copy is represented by 'r'; the working copy by 'R'. If only one parent is a carrier of the faulty HEX A gene (Figure 2), in every pregnancy there is no chance that the couple will have a baby affected with TSD. There is a 1 chance in 2 (2 chances in 4) or 50% that the baby will be an unaffected genetic carrier for TSD, just like his/her parents. We will be going over these types of inheritance patterns in detail during our lab on genetics. However, if you have any questions please let me know.