Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DNA supercoil wikipedia , lookup
Public health genomics wikipedia , lookup
Segmental Duplication on the Human Y Chromosome wikipedia , lookup
Pathogenomics wikipedia , lookup
Point mutation wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Metagenomics wikipedia , lookup
Extrachromosomal DNA wikipedia , lookup
Medical genetics wikipedia , lookup
Ridge (biology) wikipedia , lookup
Genomic library wikipedia , lookup
Gene expression profiling wikipedia , lookup
Gene expression programming wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Non-coding DNA wikipedia , lookup
Minimal genome wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Human genome wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Genome evolution wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Genome editing wikipedia , lookup
History of genetic engineering wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Designer baby wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Genomic imprinting wikipedia , lookup
Microevolution wikipedia , lookup
Down syndrome wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Y chromosome wikipedia , lookup
Genome (book) wikipedia , lookup
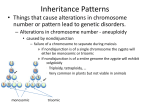
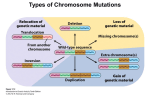
The Biology of Down Syndrome GEORGE F. SMITH Department of Pediatrics Section of Genetics Illinois Masonic Medical Center Chicago, IlIinois 60657 STEPHEN T. WARREN Center for Genetics University of lliinois College of Medicine Chicago, Ilknois 60612 INTRODUCTION Down syndrome is unique because of its preeminent role in shedding light on the biology of mental retardation. Since this disorder was first described in 1866 by John Langdon Down, the study of Down syndrome has contributed important biological knowledge and insight into normal and abnormal human development. Furthermore, Down syndrome research has provided useful information to such disparate scientific fields as oncology, immunology, biochemistry, and the behavioral sciences. The discovery by Professor Lejeune, in 1959, of an extra number 21 chromosome in the cells of individuals with Down syndrome, along with the simultaneous discovery of sex chromosome aneuploidy, firmly established cytogenetics as a bona fide medical discipline.' Although much has been learned about Down syndrome in the past 120 years, many fundamental questions remain unanswered.2 These include, but are not limited to, questions regarding the basis for the relationship between maternal age and nondisjunction; the mechanisms resulting in predispositions toward leukemias; immunologic abnormalities inherent in Down syndrome; and the genes responsible for the clinical phenotype. With the advent of molecular biology, new research methods may now be applied to these previously elusive questions. MOLECULAR ANALYSIS OF DOWN SYNDROME The major breakthrough in molecular biology allowing for the experimental manipulation of DNA is the discovery of restriction endonucleases, bacterial enzymes capable of digesting double-stranded DNA. Each endonuclease is able to recognize and cut within a unique sequence of four or more nucleotides. This has permitted the human genome to be fragmented and cIoned 1 2 ANNALS NEW YORK ACADEMY OF SCIENCES into plasmid or phage vectors, which will then replicate themselves as well as the inserted human DNA within bacterial cells. Thus, a human genomic library may be constructed such that the entire human genome is cloned and contained within several hundred thousand bacterial co10nies.~Alternatively, human chromosomes may first be isolated from one another, either by fluorescence-activated flow sorting or by isolating somatic cell hybrids, thereby placing a particular human chromosome against a distinguishable rodent genomic background. Chromosome-specific genomic libraries may then be generated from the DNA prepared from either p r ~ c e d u r e . ~ . ~ Using chromosome-21 -specific libraries, several groups of investigators have identified and isolated human DNA fragments localized to the number 21 chromosome.6 Those cloned sequences assigned to the region 21q22 are particularly useful because this is the location of the genes which, in a trisomic state, result in the phenotype of Down syndrome. Cloned DNA sequences determined to be specific for the number 21 chromosome may now be used to investigate, at a molecular level, the fundamental aspects of Down syndrome. Generally, such cloned sequences fall into three categories: partial or complete sequences of known genes; anonymous single-copy sequences; and repetitive sequences. All three types of cloned DNA from the number 21 chromosome have now been identified. The entire coding and flanking regions of cytoplasmic superoxide dismutase (SOD 1) have been cloned, as have the genes for ribosomal RNA.'.* Such a paucity of cloned genes reflects not only the inherent technical difficulties, but also, perhaps, the relatively small size of the number 21 chromosome. Fortunately, anonymous sequences are more readily isolated and have had a wide variety of applications. These sequences are useful by virtue of their ablity to detect restriction fragment length polymorphisms (RFLPs). It has been found that the recognition sequences of restriction endonucleases are quite polymorphic in humans. If a variant individual's DNA has a single nucleotide difference in a recognition sequence, quite often the ability to cleave this sequence by a particular endonuclease will be abolished. Therefore, the next proper recognition Sequence, farther along the DNA strands, will be cleaved, resulting in a larger fragment than is usually generated. If both fragments are partially homologous to an anonymous sequence used as a probe, the difference may be detected following size fractionation of the digested DNA on an agarose gel and subsequent Southern blotting. Genetic linkage between RFLPs and known disease loci have been detected on other chromosomes, and may lead to the diagnosis and/or carrier detection of such diseases as Huntington's chorea, Duchenne muscular dystrophy, and fragile X-linked mental retardati~n.~-"RFLPs on the number 21 chromosome are of particular value for determining the parental origins of the chromosomes, thereby aiding in the analysis of nondisjunction.'2 Repetitive DNA sequences in the human genome have been identified and Some of these sequences are interspersed, in many copies, throughout the entire human genome, while others appear more localized to one or a few chromosomes. Although little is known about the function SMITH & WARREN: BIOLOGY OF DOWN SYNDROME 3 of these interspersed repeats, postulated functions include their influencing gene expression and participating in DNA synthesis. Particularly germane to Down syndrome is the possible role of these repeats in genetic recombination and chromosome pairing during meiosis.l4 Such repetitive sequences, localized primarily to the number 21 chromosome, have been isolated and their study will undoubtedly reveal insight into chromosome behavior and function. Now that these molecular tools are available for the analysis of the number 21 chromosome, problems and questions long associated with Down syndrome may be approached on a different level. It can be anticipated that as these questions become answered, insight into the genesis and pathophysiology of Down syndrome may lead to rational approaches toward therapy and prevention. It must be understood that even with a complete map of the molecular structure of the number 21 chromosome, which would include gene sequencing and ultimately a map of the sequence of base pairs on the entire chromosome, we would still require a tremendous amount of basic biological knowledge to understand how the molecular products of this chromosome produce physical and mental biological effects. For example, if the major genes causing Down syndrome produce “normal gene products”enzymes and proteins-how does having an excess of these gene products in the trisomic condition produce a Down syndrome individual? Recognizing the limitation of the present type of research does not curtail the tremendous amount of good that will come from it. However, having a clear understanding of what this new research can produce in Down syndrome will set the proper research expectations and identify the methods that we will have to use to achieve our goals. MATERNAL AGE AND NONDISJUNCTION One of the most fundamental problems in human biology, and one that is intimately associated with Down syndrome, is the association between maternal age and nondisjunction.2 While maternal age has been associated with the nondisjunction of nearly all the autosomes, most often resulting in spontaneous abortion, the manifestations of chromosome 21 nondisjunction has a most profound effect by resulting in Down syndrome. The curve of the risk factor for Down syndrome associated with increasing maternal age is shown in FIGURE 1. At age 20 years, the risk is 1 in 2000 with little increase until age 35, where the risk increases to 1 in 300. By the age of 45 years, the risk of a woman bearing a child with trisomy 21 rises to 1 in 45. Although no precise mathematical model has been developed for this curve, it clearly displays the high correlation between advancing maternal age and nondisjunction. Although many mechanisms have been proposed for this association, they are sometimes exceedingly difficult to test in humans. With the approaches of recombinant DNA technology, this problem may now be examined in greater detail. At the present time, it is not clear whether the ANNALS NEW YORK ACADEMY OF SCIENCES 4 NuMr of births 25 20 30 40 35 45 Maternal agu in vmrs KEY: --- All births (in thousands) - -Down's syndrome Relative incidence FIGURE 1. Incidence of Down syndrome at birth.z -, Down syndrome; -; KEY: - - - - -, all births (in thousands); relative incidence. entire female population, with increasing age, is at risk of producing an infant with Down syndrome, or only a select portion of the female population is at risk. One approach to this problem has been the analysis of the genes coding for ribosomal RNA (rRNA).8 These genes are present in many copies, all located on the short arm and satellites of the acrocentric chromosomes, which includes the number 21. These genes may participate in the segregation of chromosomes for a number of reasons, particularly that this region contains the nucleolar organizing region (NOR), which is intimately involved in spindle formation and, therefore, chromosome separation. Also of significance is the finding that these rRNA genes undergo active recombination and, since chiasmata frequencies may influence nondisjunction, this region of the number 21 chromosome is important. It may be of considerable significance that the double NOR variant has been associated with nondisjunction of the ~ if double NORs number 21 chromosome in preliminary ~ t u d i e s . 'Clearly, are shown by subsequent studies to confer a risk of nondisjunction, the cloned rRNA genes will play a major role in elucidating the responsible mechanism. SMITH & WARREN: BIOLOGY OF DOWN SYNDROME 5 Cytogenetic variants, including the double NOR, have often been used to establish the parental origin of the extra number 21 chromosome as well as to determine at what stage nondisjunction occurred in meiosis. However, these methods are not informative in all families, making data collection difficult. The use of RFLPs has greatly increased the ability to collect such data, since virtually all families will be informative given a bank of chromosome 21 probes and the large number of restriction endonucleases available. Care must be taken, however, to control for recombination between the probed locus and the centromere. Already such RFLP analyses have been carried out in both Down syndrome families and cases of trisomic spontaneous abortions.6.'2 We can anticipate that such studies will determine familial predispositions to nondisjunction (also see the paper by Antonarakis et al. in this volume) as well as establish the role meiotic recombinations may play in this event. On the basis of the huge amount of published clinical data on aging and nondisjunction in Down syndrome during the past 25 years,' it is obvious that there are multiple causes for the production of nondisjunction in this syndrome. The mathematical data would indicate that at least four -and perhaps more- different types of molecular genetic mechanisms should be found to be associated with nondisjunction of the 21st chromosome. Undoubtedly the major molecular genetic mechanism accounting for the greatest number of cases of nondisjunction will be the one associated with nondisjunction and maternal aging. However, all the approaches for elucidating the biological basis for chromosomal trisomies will be important, given the extraordinary frequency of trisomy in humans. MOLECULAR BASIS OF THE PHENOTYPE While in a general way, for the past 26 years, trisomy 21 has been considered responsible for the phenotype of Down syndrome, we must now go to a finer level of resolution and ask what genes are responsible, when in the trisomic state, for the phenotype. It is evident that the clinical entity of Down syndrome is the result of many abnormalities of development. Virtually all the major organ systems within the body are affected in some degree and, it is important to note, in a very consistent fashion among those with trisomy 21. The number of genes involved is unclear at this point. However, when one considers that the human genome contains approximately 100,OOO genes and that the number 21 chromosome represents less than 2% of the genome according to size, the number of genes may be estimated to be approximately one thousand. Since the phenotype of Down syndrome is largely localized to the 21q22 region of the chromosome, this number may be further reduced to less than a hundred genes. Currently, five genes have been confirmed to be located on chromosome 21 (see also the paper in this volume by Cox and Epstein), while five others are provisionally mapped to this chromosome (TABLE1). In addition, several anonymous DNA sequences have also been ANNALS NEW YORK ACADEMY OF SCIENCES 6 TABLE 1. Gene Assignments to Chromosome 21' Marker Status Nucleolar organizing ribosomal RNA (RNR) Cytoplasmic superoxide dismutase (SOD 1) Alpha/beta interferon receptor (IFRC) Phosphoribosylglycinamide synthetase (PRGS) Phosphofructokinase, liver-type (PFKL) Phosphoribosylaminoimidazolesynthetase (PAIS) Cystathionine beta-synthetase (CBS) Surface antigen S14 Surface antigen MF13 Surface antigen MF14 C C C ABBREVIATIONS: C, confirmed assignment; P, provisional assignment. ' Data are from Westerveld and Naylor.16 mapped to chromosome 21.16The best known gene mapped to chromosome 21 is cytoplasmic superoxide dismutase (SOD 1). This gene, which shows a clear dosage effect in Down syndrome, has been cloned, sequenced, and otherwise extensively characterized (see the paper by Groner et al. in this volume). Although its relationship to the phenotype is not understood, the molecular knowledge generated regarding its structure and function should illuminate this point. The number of these genes to be found responsible for the phenotype will likely be quite small when one considers that monosomy for a single gene (i.e., a heterozygote for a metabolic disorder) is phenotypically normal. Therefore, it is not unlikely that for many genes, the presence of an extra copy would likewise be of little consequence. Thus the remaining genes must code for proteins (or RNA) that either have a major role in development by themselves or else are involved in gene regulation, thereby influencing other genes located throughout the genome. Some clues regarding these questions are emerging from animal studies in partially trisomic This system may ultimately prove to be one in which the effect of trisomy on development may be fully elucidated. Also, as additional genes become localized to chromosome 21, a more complete picture may emerge. It may be of relevance to the phenotype that of the few genes now known to be located on chromosome 21,two are involved in purine biosynthesis - phosphoribosylglycinamide synthetase (PRGS) and phosphofructokinase, liver-type (PFKL). As the molecular structure of this chromosome becomes defined and the functions of the genes determined, the approaches for therapeutic considerations will become evident. LEUKEMIA The increased incidence of leukemia in Down syndrome has been a perplexing problem that has defied a suitable scientific explanation. The incidence of leukemia is 15 to 20 times that observed in nontrisomic populations.' Furthermore, transient leukemia and a leukemoid response occur not infrequently SMITH & WARREN: BIOLOGY OF DOWN SYNDROME 7 in newborns with Down syndrome. Either of these hematologic responses is quite unusual in normal newborn infants. Thus, it has long been considered that on the chromosome 21 there resides a gene or genes involved in hemopoiesis or that, in some fashion, predisposes trisomic individuals toward leukemia. Some support for this idea may be drawn from cytogenetic studies in neoplasia. It is widely accepted that nonrandom chromosome changes are important events in carcinogenesis. Chromosome 21 has been implicated in some of these changes. For example, trisomy 21 is a common feature in acute lymphoblastic leukemia. Furthermore, translocations involving chromosome 21 t(8;21)(q22;q22) have been observed in acute nonlymphocytic leukemia.20 A number of cellular genes have recently been identified that, when mutated, amplified, or rearranged, partially transform normal cells.2*The loci of these oncogenes have often been found to be located on chromosomes previously shown to be nonrandomly rearranged in certain cancers. l9 Therefore, it is not unreasonable to search for oncogenes on the number 21 chromosome. Recent data have shown homologous sequences, corresponding to the 5’ region of the c-Haras-1 oncogene, present on chromosome 21. The relationship between this homology and Down syndrome, however, remains to be elucidated.22 IMMUNE COMPETENCE IN DOWN SYNDROME Many researchers working with persons with Down syndrome have beer, convinced that the immune system on these persons is seriously deficient. The evidence for this includes the increased incidence in these persons of infectious disease and the marked increase in death due to pneumonia, which is 70 times that of a control population (without antibiotics). The immune rcsponses, measured in these patients by determining antibody responses to tetanus toxoid, typhoid vaccines and, more recently, bacteriophage OX, have all been abnormal. Autoimmune disease response also appears in Down syndrome. Thyroid autoantibodies are increased and vitiligo occurs with regularity in these persons. Abnormal antibody response to such mundane substances as milk proteins occurs frequently in infants with Down syndrome. Less clear is the ten-fold-increased incidence of the Australian antigen, Au(l), in patients with Down syndrome. This and the abnormal responses to the hepatitis virus, including the persistence of the Au(1) antigen, in patients with Down syndrome with chronic anicteric hepatitis also suggest a problem in immunity. Although an immune defect in Down syndrome has been proposed by Blumberg to explain the increased incidence of chronic virus infection, hepatitis, and leukemia, a major defect in the immune system has not yet been demonstrated. The mapping of the interferon receptor to 21q22 has stimulated new possibilities regarding this pr~blem.’~ Since additional interferon receptor sites may lead certain cells, particularly the immature monocytes, to fail to mature, an extra copy of this gene may be important in the failure to fully de- 8 ANNALS NEW YORK ACADEMY OF SCIENCES velop immune competence. It is hoped that as additional knowledge of the biological aspects of immunity is acquired, particularly information regarding interferon, a molecular basis of this clear clinical problem associated with Down syndrome will develop. CONCLUSIONS Molecular genetics has extended our horizons as to what can be accomplished in Down syndrome research in the forseeable future. As additional genes are regionally assigned to the 21st chromosome, a more complete map of this chromosome may be generated. Using those genes that have been cloned, as well as additional anonymous DNA sequences, it is quite likely that a complete linkage map of chromosome 21 will soon be achieved. This will then lead to the rapid regional assignment of future genes, further strengthening the linkage map and ultimately leading to a complete characterization of the molecular structure of this small autosome. As each additional piece of information on the molecular structure of this chromosome is gleaned, it should be evaluated carefully in terms of what further information it may provide regarding the mechanisms of nondisjunction and the phenotype of Down syndrome. Those loci assigned to the 21q22 region should be especially well studied, since this is the segment most responsible for the syndrome. However, it must be remembered that those genes located in the proximal portion of the chromosome may be important in the variation sometimes observed in Down syndrome, since 96% of the patients are fully trisomic. Through continued research, the molecular basis for chromosome behavior during cell division should emerge. Thus, one or more mechanisms of meiotic nondisjunction may be defined such that the relationship with maternal age will be more clearly understood. It is not overly optimistic to hope that such an understanding may lead to the prospect of prevention of Down syndrome. A firm molecular knowledge of the 21st chromosome and its relationship to the phenotype of trisomy 21 would set the stage for therapeutic approaches. REFERENCES 1. 2. 3. 4. 5. LEJEUNE,J . , M. GAUTIER & R. TURPIN.1959. Etude des chromosomes somatiques de neuf enfants mongoliens. C. R. Acad. Sci. Paris 248: 1721. SMITHG . F. & J . M. BERG.1976. Down’s Anomaly, 2nd ed. Churchill, Ltd. London. MANIATIS, T., E. F. FRITSCH & J . SAMJ~ROOK. 1982. Molecular Cloning: A Laboratory Manual. Cold Spring Harbor Laboratory. Cold Spring Harbor, NY. KRUMLAUF, R., M. JEANPIERRE & B. D. YOUNG.1982. Construction and characterizationof genomic libraries from specific chromosomes. Proc. Natl. Acad. Sci. USA 79: 2971-2975. J . F., C. KEYS, A. VARSANYI-BREINER, F. T. KAO, C. JONES, T. T. GUSELLA, SMITH i% WARREN: BIOLOGY OF DOWN SYNDROME 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 9 PUCK& D. HORISMAN.1980. Isolation and localization of DNA segments from specific human chromosomes. Proc. Natl. Acad. Sci. USA 7 7 2829-2833. KITTUR,S., S. E. ANTONARAKIS, Y. GRONER, J. A. PHILLIPS, D. MEYERS & H. H. KAZAZIAN.1984. Linkage map on human chromosome 21. Am. J. Hum. Genet. 36 (Suppl.): 142s. GRONER,Y. 1984. Personal communication. ARMHEIM, N., M. KUPTAL, R. SCHMICKEL, G.WILSON, 0. RYDER& E. ZIMMER. 1980. Molecular evidence for genetic exchanges among ribosomal genes on nonhomologous chromosomes in man and apes. Proc. Natl. Acad. Sci. USA 77: 7323-7327. GUSELLA, J. F., N. S. WEXLER,P. M. CONNEALLY, S. L. NAYLOR, M. A. ANDERSON, R. E. TANZI,P. WATKINS,K. OTTINA,M. R. WALLACE, A. Y. SAKAGUCHI, A. B. YOUNG,I. SHOULSON, E. BONILLA & J. B. MARTIN.1983. A polymorphic DNA marker genetically linked to Huntington’s disease. Nature 306: 234-238. DAVIES,K. E., P. I. PEARSON, P. S. HARPER,J. M. MURRAY, T. O’BRIEN,M. SARFARZI& R. WILLIAMSON. 1983. Linkage analysis of two cloned DNA sequences flanking the Duchenne muscular dystrophy locus on the short arm of the human X chromosome. Nucleic Acids Res. 11: 2303-2311. WARREN,S. T., T. W. GLOVER, K. L. DAVIDSON & P. JAGADESWARAN. 1985. Linkage and recombination between fragile X-linked mental retardation and the factor IX gene. Hum. Genet. 69: 44-46. HASSOLD, T. J., D. CHILL& J. YAMANE. 1984. Parental origin of autosomal trisomies. Ann. Hum. Genet. 48: 129-144. GRAHAM,G.J., T. J. HALL& M. R. CUMMINGS. 1984. Isolation of repetitive DNA sequences from human chromosome 21. Am. J. Hum. Genet. 3 6 25-35. HENDERSON, S. A. & R. G. EDWARDS. 1968. Chiasma frequency and maternal age in mammals. Nature 218: 22-28. JACKSON-COOK, C. K., D. B. FLANNERY, L. A. COREY,W. E. NANCE& J. A. BROWN.1984. The double NOR variant: A risk factor in trisomy 21. Am. J. Hum. Genet. 36(Suppl.): 975. WESTERVELD, A. & S. NAYLOR.1984. Report of the committee on the genetic constitution of chromosomes 18, 19, 20, 21 and 22. Cytogenet. Cell Genet. 37: 155-175. Cox, D. R., H. KAWASHIMA,S. VORA& C. J. EPSTEIN.1983. Regional mapping SOD-I, PRGS, and PFK-L on human chromosome 21: Implications for the role of these genes in the pathogenesis of Down syndrome. Am. J. Hum. Genet. 35: 188A. EPSTEIN,C. J., L. B. EPSTEIN,J. WEIL& D. R. Cox. 1983. Trisomy 21: mechanisms and models. Ann. N. Y. Acad. Sci. 396: 107-118. YUNIS,J. J. 1983. The chromosomal basis of human neoplasia. Science 221: 227-236. 20. 21. 22. 23. 24. BERGER, R., A. BERNEHIM & A. DE LA CHAPELLI.1982. Chromosome rearrangement in acquired malignant diseases. Hum. Gene Mapping 6:205-207. K. & R. SCHAFER.1984. Human oncogenes. Hum. Genet. 66: 132-142. WILLECKE, SCOGGINS, C.. 1984. Personal communication. & W. T. LONDON.1970. Australia antigen as BLUMBERG, B. S., A. J. SUTNICK a hepatitis virus. Am. J. Med. 48: 1-8. EPSTEIN,L. B., H. S. SPENCER, S. H. S. LEE& C. J. EPSTEIN.1980. Enhanced sensitivity of trisomy 21 monocytes to the maturation-inhibiting effect of interferon. Cell. Immunol. 50: 191-194.