Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Biochemical switches in the cell cycle wikipedia , lookup
Endomembrane system wikipedia , lookup
Extracellular matrix wikipedia , lookup
Cell growth wikipedia , lookup
Cell encapsulation wikipedia , lookup
Cytokinesis wikipedia , lookup
Tissue engineering wikipedia , lookup
Cell culture wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Cellular differentiation wikipedia , lookup
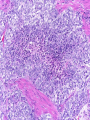
Common Challenges in Endometrial Biopsy Interpretation Aaron Haig Conflict of Interest Disclosures Aaron Haig I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations that could be perceived as a direct or indirect conflict of interest in the content of this presentation. Endometrial biopsies Abnormal uterine bleeding (>95%), Pre or post menopausal Other endometrial cells in pap infertility missed products Adequate? A. Adequate Photo B. Inadequate C. Depends Biopsy Adequacy No universal standards Individual judgment Adequate for one situation, may not necessarily be adequate for another At a minimum, need … some glandular and stromal tissue from the fundus (to ensure entry into the endometrial cavity) Biopsy Adequacy If suspected atrophic …. minimal tissue is expected However, minimal tissue with hyperplasia or high clinical suspicion Then a comment suggesting repeat biopsy is warranted. Biopsy Adequacy No formal criteria Unassessable (or insufficient) has been suggested as a more appropriate term If fits with clinical than repeat biopsy is not needed Outline Endometrial malignancy, subtyping Benign mimics Endometrial vs endocervical carcinoma Vanishing carcinoma Endometrial Malignancies Type I • Endometrioid • variants • Mucinous Type II • Serous • Clear Cell Other • Mixed cell adenocarcinoma • Small cell carcinoma • Squamous cell • Undifferentiated • Others Subtyping endometrial malignancy…… Can be difficult Variant or unusual morphologies Scant tissue High grade Mixed Non endometrial primary What is it? A: Endometrioid B: Serous C:Villoglandular D: Clear cell What is it? A: Endometrioid B: Serous C:Villoglandular D: Clear cell Serous with a pseudoglandular pattern Serous with a prominent glandular pattern Can be mistaken for low grade endometrioid Ca Look for extreme discordance between architectural and cytologic features Irregular luminal borders Cells lack polarity Marked pseudostratification, and nuclear pleomorphism, Brisk mitiotic activity Single cell apoptosis Serous vs Endometrioid Different treatments and prognosis type I vs type II Morphology the most important tool Serous vs Endometrioid Clinical history Background EIC/atrophy hyperplasia Immunohistochemistry if interpreted properly Webpathology.com p53 How many are Serous? A B C D How many are Serous? A. 1 B. 2 C. 3 D. 4 How many are Serous? Endometrioid, nonvillous papillae Serous Endometrioid, villoglandular Endometrioid Adenocarcinoma with Papillary Architecture Villoglandular 1. slender, finger-like papillae - lacks branching and budding 2. columnar cells, minimal nuclear pseudostratification 3. smooth apical luminal border, preserved nuclear polarity 4. mild cytologic atypia - (grade 1, or only focal grade 2) Wikimedia commons Endometrioid Adenocarcinoma with Papillary Architecture Nonvilloglandular 1. small pseudopapillae budding into endometrioid type glands 2. relatively uniform distribution of pseudopapillae 3. cohesive, polygonal cells with abundant eosinophilic cytoplasm 4. mild cytologic atypia - usually grade 1 to focal 2 1. can have overt squamous differentiation Endometrioid vs Serous Immunohistochemical Panel Proposed panel: p16, p53, ER, PR p16 and p53 ER/PR Serous + - Endometrioid - + Endometrioid vs Serous Immunohistochemical Panel Serous Endometrioid p16 p53 ER/PR 70-90% + 80% 5-50% + 40%+ 10-20% (grade 3) 80%+ (falls to 15-50% in grade3) Note: 1. WT1 not reliable for endometrial serous (compared to ovarian serous) 2. p53 can be completely negative in ESC due to a truncated mutation (all or none pattern) Arch Pathol Lab Med, Vol 137, Nov 2013 Take home Not all that is papillary is serous High grade nuclear atypia and luminal irregularity helpful for serous Also, increased mitotic figures and background endometrium ER, PR, p16, p53 good panel but use with caution (especially grade 3 endometrioid). Endometrioid with focal clear cells Secretory endometrioid Endometrioid with clear cell squamous component Serous carcinoma with clear cells Clear cell features NOT favouring clear cell carcinoma Columnar cells Distinctive shape of vacuoles Bland nuclear features No high grade cytologic atypia, tubulocytsic, papillary or solid patterns Immunohistochemistry Negative ER and diffuse p53 favour CCC Significant proportion do not show this Clear cell Endometrioid ER/RP p53 Weak or absent present Diffuse and strong less Ki67 50% CCC; 20% endometrioid p16 too much overlap Endometrial Epithelial Metaplasia Morphology seen elsewhere in Mullerian tract. Mullerian derived structures retain some degree of plasticity Major mechanisms Degenerative/reparative Hormonal Neoplastic Endometrial Epithelial Metaplasia Ciliary (tubal) Eosinophilic Squamous Mucinous Hobnail Clear cell Papillary syncytial Adv Anat Pathol,Vol 16, Jan 2009 Endometrial Epithelial Metaplasia May be present in the full spectrum of endometrial patterns Normal proliferative to adenocarcinoma No clinical significance However, potential for misinterpretation eg. Atypia in tubal metaplasia, carcinoma in clear cell, hobnail and pap metaplasia Picture of diff patterns AP104 pg23 Squamous metaplasia Keratinizing or not keratinizing (morular) Can be seen in reactive, hyperplasia or carcinoma Squamous Metaplasia Degenerative changes or repair No risk of progression Chronic endometritis, infarcted endometrial polyp, IUD Also seen with …. Complex hyperplasia, atypical polypoid adenomyoma (APA), adenocarcinoma Seen in approx 25% of adenoCa Things to remember of Squamous Metaplasia Assessment is based only on glandular component Necrosis or solid growth do not alter interpretation Look for minimal mitotic activity and low proliferation rate Hormonally inert No ER/RP receptors, do not regress with hormones Things to remember of Squamous Metaplasia Diagnosis based on glandular component E.g. simple hyperplasia with squamous morules If extensive squamous differentiation, with no definitive underlying glandular structure Recommend re-biopsy Papillary Syncytial Metaplasia Commonly seen with endometrial breakdown Regenerative process Can raise concern for ESC or EIC. Papillary Syncytial Metaplasia Minimal/reactive cytologic atypia Look for other signs of breakdown - stromal balls - fibrinous material - neutrophilic infiltation - apoptotic bodies Also consistent with features of tumour diathaisis Papillary Syncytial Metaplasia Immunohistochemistry has been shown: ER is down regulated P16 strongly expressed Increased p53 expression Overlapping with serous immunophenotype - Look for low MF and decreased Ki-67 McCluggage Int J Gynecol Pathol Vol.31, May 2012 Papillary Syncytial Metaplasia Look for hyperplasia or EIC Look for high MF with increased Ki-67 Immunohistochemistry can be helpful But do not over interpret Significant overlap with serous carcinoma Carcinoma: Endocervical vs Endocervical Histologic overlap Both can have: endometrioid differentiation mucinous differentiation 5% of endocervical 10% of endometrial Treatment and prognostic implications Webpathology.com Endometrial Mass centered in uterine corpus or LUS Co-existing hyperplasia Squamous morules Scant intervening stroma Foamy histocytes Endocervical Mass in cervix Co-existing AIS (or SIL) Marked associated stromal desmoplasia Endometrioisis Webpathology.com Immunohistochemical Panel Endocervical ER - Vimentin - CEA + p16 diffuse strong Endometrioid ER + Vimentin + CEA - p16 neg, wk, or focal strong Note: significant overlap – IHC not definitive; use a panel Endocervical vs Endometrial Need to correlate: clinical, radiological and IHC findings Still a significant number of cases it is not possible to tell, even after resection Recommendation Biopsy: give differential diagnosis Resection: provide appropriate staging information for both locations with a comment of the diagnostic challenge ‘Vanishing Carcinoma’ Cases with: Biopsy proven endometrial carcinoma No residual carcinoma or biopsy site in subsequent hysterectomy 0 – 19% (~3%) T. Colgan Int J Gynecol Pathol 2007 ‘Vanishing Carcinoma’ Term has been described in prostate Concept may be useful in both clinical and medicolegal practice ‘Vanishing Carcinoma’ Criteria for diagnosis of VCa Malignant dx must be reviewed and confirm 1. r/o floaters etc… 2. Embed and examine entire endometrium 3. Document neoadjuvant tx high dose progestins and preop radiation therapy can eradicate EmCa ‘Vanishing Carcinoma’ Well documented problem not to be assumed lab or Pathologist error. DNA profiling can be use in cases with any suspicious of mix-up or medico-legal cases Questions….