Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Time perception wikipedia , lookup
Neuroeconomics wikipedia , lookup
Cortical cooling wikipedia , lookup
Human brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Aging brain wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Embodied language processing wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Microneurography wikipedia , lookup
Synaptic gating wikipedia , lookup
Environmental enrichment wikipedia , lookup
Transcranial direct-current stimulation wikipedia , lookup
Cerebral cortex wikipedia , lookup
Evoked potential wikipedia , lookup
Treatment of Thalamic Pain by Chronic Motor
Cortex Stimulation
TAKASHI TSUBOKAWA, YOICHI KATAYAMA, TAKAMITSU YAMAMOTO,
TERUYASU HIRAYAMA, and SEIGOU KOYAMA
Erom the Department of Neuorological Surgery, Nihon University School of Medicine, Tokyo,
Japan
TSUBOKAWA, T., ET AL.: Treatment of Thalamic Pain by Chronic Motor Cortex Stimulation. All forms
0/ therapy, including chronic stimulation of Ihe thaiamic relay nucleus, can provide satisfactory pain
control in only 20%-30% of cases of thalamic pain syndrome. In order to deveJop a more effective
treatment for thaJamic pain syndrome, we investigated the effects of stimulation of various brain regions
on the burst hyperactivity 0/thaJamic neurons recorded in cats after deafferentiation of the spinotholamic
pathway. Complete, long- term inhibifion of the burst fiyperacfivity was induced by slimuJation of the
motor cortex. Based on this experimental finding, we treated seven cases of thalamic pain syndrome by
chronic motor cortex stimulation employing epidural plate electrodes. Excellent or good pain controJ
was obtained in all cases ivithout any complications or side effects. During the stimulation, an increase
in regional blood flow of the cerebral cortex and (halamus. a marked rise in temperature of the painful
skin regions, and improved movements of the painful limbs were observed. These results suggest that
thalamic pain syndrome can be most effectively treated by chronic motor cortex stimulation. (PACE,
Vol. 14, January 1991}
thalamic pain, cortex stimulation, chronic, blood flow, glucose metabolism
Introduction
All forms of therapy, including chronic stimulation of the thalamic relay nucleus, can provide
satisfactory pain control in only 20%-30% of cases
of thalamic pain syndrome.^ In order to develop
a more effective treatment for thalamic pain syndrome, we, therefore, investigated the effects of
stimulation of various brain regions on the hurst
hyperacfivity of thalamic neurons recorded in cats
and in humans during stereotaxic surgery for the
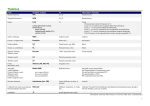
relief of thalamic pain. Complete and long-term
inhibition of the hurst hyperactivity was induced
hy stimulation of fho motor cortex (Fig. 1}.^ Based
on these findings, we treated seven cases of thalamic pain syndrome by epidural motor cortex
chronic stimulation.
This presentation describes the chronic stim-
Address for reprints: Takashi Tsubokawa, M.D., D.M.Sc, Department of Neurological Surgery, Nihon University School of
Medicine, Tokyo 173, Japan. Fax:
PACE. Vol. 14
ulation technique for motor cortex stimulation
and the effect on thalamic pain.
Methods
Clinical Evaluation and History of the Treated
Cases Suffering from Thalamic Pain
All seven cases selected as candidates for
chronic motor corfex stimulation treatment, suffered from severe thalamic pain caused by stroke.
Six cases had small lesions in the thalamic relay
nucleus caused by thalamic lateroventral infarct
(four cases) or small thalamic hemorrhage (two
cases). The other case had a small lesion in the
posterior limb of the internal capsule caused by
hemorrhage of the putamen.
The intervals after the onset of the primary
stroke were 1-4 years. The patients had been
treated with various kinds of medication (anticonvulsants and antidcpressants) and psychotherapy, but their pain could not be Gontrolled at
January 1991
131
TSUBOKAWA, ET AL.
i
50msec
B
Motor Cortex
C
Sensory Cortex
46sec
0
Figure 1. Effects on burs! firing neurons in (he vicinity of the dcjmcij>ed thalamic area following
either motor or sensory cortex stimtilalion. {A) High frequency burst firing recorded at the border
zone of the damaged thaJamic relay nucleus. (B) Long-lusting inhibitory effects on the burst
firing by motor corfex stimu/alion. (CJ Effect on the burst firing by st^nsory cortex stimulation.
alL Five cases displayed slight motor weakness,
but they could walk without help.
Before chronic implantation of the stimulating electrode, all cases were examined for lesions
by both X-CT and MRI, and were also checked by
the morphine and barbiturate tests.'^ The thalamic
pain in four of the cases was barbiturate sensitive
and insensitive to the morphine test. In two cases,
the barbiturate test was partially sensitive and
there was no sensitivity to the morphine test. The
other case was insensitive to the morphine and
barbiturate tests.
Chronic Implantation of the Stimulating
Electrode at the Kpidural Space on the Motor
Cortex
Under local anesthesia, the location of the
central sulcus was mapped on the scalp using
132
Kronlein's anatomical measurements (Fig, 2).
Trephination was performed on the line, which
indicates the central sulcus and 3- to 4-cm lateral
to the midline for upper extremity pain or 1-cm
lateral to the midline for lower extremity pain.
A quadruple disc stimulating electrode (5 mm
in diameter at the active point, 10 mm between
the poles IMedtronic, Inc., model 3587, Minneapolis, MN, USA]) was inserted into the epidural
space corresponding to the motor cortex. The location of the electrode was identified by recording
somatosensory evoked potentials through the
electrode in response to stimulation of the peripheral nerves which innervated the painful area.
Whenever the electrode was placed in the right
position on the motor cortex, the N^o of the sensory evoked potential could be recorded as P20
(phase reversal to N20) (Fig. 2). The electrode was
January 1991
PACE. Vol. 14
CORTEX STIMULATION FOR THALAMIC PAIN
so%
Nasion
100% Inion
Kronlein
Figure 2. Idf;nti/icafion o/ the location of ihe. slinuiJaling electrode. A( Ihe first .step, the central
suJcus was drawn on the scalp using Kroniein's method Qi\d Ihe electrode inserted into the
epidurnl space. A/ler insertion, somatosensory evoked polenliuls were recorded from (he inserfed electrode, whenever the eJectrode VJQ.?, placed on the motor cor(ex, and the N20 wave
showed phase reversal.
moved to the correct position by using this response.
After checking that the stimulating electrode
had been placed on the motor cortex by recording
the V-iu of the somatosensory evoked potentials,
the electrode was connected to a transmitter
which was implanted in the subcutaneous area
of the anterior chest wall as an internal chronic
stimulation system. The strength of the stimulation was below the threshold for muscle twitching
(< 1.0 mA maximum with 0.1-0.5 msec width,
50—120 Hz square wave, ramp type current).
The clinical effectiveness for thalamic pain
and the side effects or complications in all seven
cases were followed up for more than 1 year after
using the chronic stimulation.
At 4-10 days after implantation of the chronic
stimulating system and the beginning of stimulation, the regional cerebral blood flow was esti-
PACE, Vol. 14
mated by the T^' amphetamine SPECT scanning
method and the skin temperature was measured
by thermography. in order to check the effects of
the chronic motor cortex stimulation.
Results
In all cases, the intractable thalamic pain was
subject to satisfactory control. The pain subsided
within a few minutes after initiation of the stimulation, and the effect on the pain continued for
4-5 hours following 5 minutes stimulation. Usually, 5-10 minutes of stimulation was applied 5
to 6 times per day at the early stage, but this was
changed to about 2 to 3 times in the daytime only
at the chronic stage after implantation.
The regional cerebral blood flow showed a
marked increase to 150%-200% of the level in the
prestimulation period in the stimulated cortex
January 1991
133
TSUBOKAWA, ET AL.
and the ipsilateral thalamic and brain stem area.
The skin temperature in the painful area increased
to almost the same level as that in the contralateral
nonpainful area.
At 1 year after the implantation, five of tbe
cases did not have any complaints about pain
without any supplemental medication, and the
other two cases also had satisfactory pain control
witb some supplemental medication. Tbey did not
suffer any side effects such as seizures or sensory
disturbance or any complications. The niotor disability also underwent improvement in all cases
with previous disturbance of motor function,
mainly of coordination.
cerebral blood flow of the cortex and thalamus was
increased and the skin temperature was also increased during the motor cortex stimulation in effective cases.
Based on these results, chronic motor cortex
stimulation is considered not only to exert an inhibitory effect on tbe burst firing occurring in the
vicinity of thalamic lesions, but also to have certain neuroplastic effects on the damaged thalamus, as suggested by an increase of regional cerebral blood flow and metabolism in the brain and
increased skin temperature in the painful area.
Conclusion
Discussion
Chronic motor cortex stimulation was able to
induce remarkable pain relief in cases suffering
from thalamic pain who failed to derive any beneficial effect from medical and psychological
treatments. Furthermore, according to the 1-year
follow-up results, 71% of the treated cases were
able to maintain excellent effects. The regional
Severe thalamic pain can be controlled by
chronic motor cortex stimulation. The pain relief
mechanism is based not only on an inhibitory effect on the burst firing in the vicinity of the damaged thalamus. but also on the effect of increased
regional cerebral blood flow and glucose metabolism in the cortex and thalamus contralateral to
the painful area.
References
1. Tsubokawa T, Katayama Y, Yaniamoto T, et al.
Deafferentation pain and stimulation of thalamic
sensory relay nucleus. Appl Neurophysiol 1985;
48:166-171.
2. Hirayama T, Tsubokawa T, Katayama Y, et al.
Chronic changes in activity of thalamic relay neurons following spino thalamic tractomy in cat. Ef-
134
January 1991
fects of motor cortex stimulation. Pain 1990;
5fSuppl.1:273.
Tsubokawa T. Chronic stimulation of deep brain
structures for for treatment of chronic pain. In Tasker RR (ed.): Neurosurgery State of Arts Review,
Vol. 2, Stereotaxic Surgery. Hanley and Belfus, Inc.,
Philadelphia, 1985, pp. 235-255 .
PACE, Vol. 14