Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Microbial metabolism wikipedia , lookup
Biochemical cascade wikipedia , lookup
Metabolomics wikipedia , lookup
Butyric acid wikipedia , lookup
Electron transport chain wikipedia , lookup
Adenosine triphosphate wikipedia , lookup
Pharmacometabolomics wikipedia , lookup
Mitochondrial replacement therapy wikipedia , lookup
Lactate dehydrogenase wikipedia , lookup
NADH:ubiquinone oxidoreductase (H+-translocating) wikipedia , lookup
Mitochondrion wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Biosynthesis wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Metabolic network modelling wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
Nicotinamide adenine dinucleotide wikipedia , lookup
Oxidative phosphorylation wikipedia , lookup
Glyceroneogenesis wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
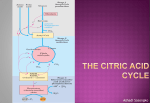
Metabolomics Citric Acid Cycle Intermediates in Cardioprotection Gabor Czibik, MD, PhD;* Violetta Steeples, BSc;* Arash Yavari, BSc, MRCP, DPhil;* Houman Ashrafian, MA, MRCP, DPhil* Abstract—Over the last decade, there has been a concerted clinical effort to deliver on the laboratory promise that a variety of maneuvers can profoundly increase cardiac tolerance to ischemia and/or reduce additional damage consequent upon reperfusion. Here we will review the proximity of the metabolic approach to clinical practice. Specifically, we will focus on how the citric acid cycle is involved in cardioprotection. Inspired by cross-fertilization between fundamental cancer biology and cardiovascular medicine, a set of metabolic observations have identified novel metabolic pathways, easily manipulable in man, which can harness metabolism to robustly combat ischemia-reperfusion injury. (Circ Cardiovasc Genet. 2014;7:711-719.) Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 D of principle, significant reductions in final infarct size (of ≤50%) could be achieved in experimental models.2 Decades of research have successfully dissected out the molecular components of IPC, including the time course of protection, triggers evoking the protective signaling and prosurvival kinase cascades (described in recent reviews9,11,12). In contrast, translation to man has generally been disappointing with no IPC strategy routinely used in clinical practice. Reasons for this failure have recently been reviewed elsewhere.13–15 Because patients with CAD are often elderly with numerous other comorbidities and confounding medical therapies,14 the protective potential of IPC may be compromised, motivating the exploration of new strategies to reduce ischemic cardiac injury and the associated healthcare and societal costs. One such approach has been the application of metabolic strategies to modify the time course of myocardial injury. In the 1960s, preceding the pharmacological or mechanical reperfusion era, Sodi-Pallares proposed using a solution containing glucose, insulin, and potassium to prevent reperfusion arrhythmias.16 The rationale was to support myocardial energy generation through augmentation of ischemic glycolytic activity using pharmacological doses of glucose and insulin.17 This combination reduces circulating free fatty acids that potentially inhibit glycolysis18 (mitigating the Randle cycle via insulin’s inhibitory effect on lipolysis) and has been proposed to prevent arrhythmias through the restoration of intracellular potassium and stabilisation of membrane potential.16 The majority of experimental studies applying glucose, insulin, and potassium treatment have reported reduced infarct size19 with improved postischemic functional20 and energetic recovery,21 with subsequent successful translation to humans.22,23 Encouraged by his success and that of the first Diabetes Mellitus InsulinGlucose Infusion in Acute Myocardial Infarction (DIGAMI) trial,24 the method gained popularity to reduce IR-injury after espite a dramatic drop in the incidence of acute myocardial infarction over recent decades,1 coronary artery disease (CAD) is still the foremost cause of death globally, with >7 million people dying annually.2 In developed countries, reductions in exposure to major risk factors and the application of evidence-based interventions to patients with CAD have shifted the epidemiology of CAD toward older age.3,4 There are concerns that this positive trend may be obviated by the pandemic of obesity and type 2 diabetes mellitus. Advances in cardiac surgery have led to its application to an increasingly older subset of patients, with a correspondingly greater risk of myocardial injury. Sensitive means of detecting myocardial injury have broadened the at-risk population to include those undergoing major noncardiac surgical procedures (eg, vascular or major abdominal surgery), particularly in the elderly.5 Much of the effort to reduce CAD-related myocardial injury has focussed on reducing the burden of coronary atheroma and plaque stability. The delineation of robustly protective alleles reducing the burden of atherosclerosis (eg, PCSK96 and APOC37,8) has signposted potential drug targets to modify the course of CAD. An alternative strategy would be to focus on identifying approaches to protect the myocardium from disease or iatrogenic injury. Ischemic myocardium ultimately necroses unless reperfused.9 Paradoxically, reperfusion itself comes at a cost, a phenomenon termed ischemia-reperfusion (IR) injury.2 IR-injury may manifest in the form of contractile (stunning), vascular (no-reflow phenomenon), electric (reperfusion arrhythmias) impairment, or lethal reperfusion injury.2 To mitigate these complications, enthusiasm for a myocardial protection strategy was inspired in 1986 by the description of ischemic preconditioning (IPC) in which brief, nonlethal episodes of ischemia alternating with episodes of reperfusion powerfully protected the myocardium from subsequent otherwise lethal ischemic challenge.10 As proof From the Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom. Guest Editor for this series was Manuel Mayr, MD, PhD. *Dr Czibik, V. Steeples, A. Yavari, and H. Ashrafian contributed equally to this work. Correspondence to Houman Ashrafian, MA, MRCP, DPhil, Division of Cardiovascular Medicine, Radcliffe Department of Medicine, West Wing, John Radcliffe Hospital, Oxford OX3 9DU, United Kingdom. E-mail [email protected] © 2014 American Heart Association, Inc. Circ Cardiovasc Genet is available at http://circgenetics.ahajournals.org 711 DOI: 10.1161/CIRCGENETICS.114.000220 712 Circ Cardiovasc Genet October 2014 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 acute myocardial infarction.25 The present status of glucose, insulin, and potassium for cardioprotection is controversial because large-scale randomized double-blind studies reported mixed effects.26 Glucose, insulin, and potassium is thus not routinely used but has motivated the search for more clinically applicable metabolic approaches to cardioprotection. For many decades, even before description of the complete citric acid cycle (CAC), ischemia and hypoxia were recognized to stimulate the degradation of myocardial aspartate and glutamate resulting in the production of succinate in isolated hearts.27 It has been proposed that this channelling serves to generate ATP in the absence of oxygen. These observations led to the hope that manipulation of the CAC could promote cardioprotection. As a corollary, in the mid-2000s, germline heterozygous loss-of-function mutations in the CAC enzyme fumarate hydratase (FH, catalyzing the hydration of fumarate to malate)28,29 were found to cause hereditary leiomyomatosis and renal cell cancer (HLRCC), an autosomal dominant disorder characterized by smooth-muscle tumors of the skin and uterus, and renal cancer. The resulting accumulation of the CAC intermediate fumarate has several potentially beneficial sequlae, including the stabilization of hypoxia-inducible factor 1α (HIF-1α; a master transcription factor coordinating the response to hypoxia),30 with potentially cytoprotective implications for both cancer biology31 and myocardial protection.32 In this review, we shall start by describing the canonical functions of the CAC with a focus on the myocardium. We will follow by outlining the CAC's recently explored noncanonical metabolic (eg, signaling) roles culminating in our experience with CAC intermediates and their manipulation as promising cardioprotective therapies. A glucose Traditional Functions of the CAC The CAC,33 either in its complete or in its modified forms, is a metabolic hub in all aerobic and some anoxygenic organisms (eg, green sulfur bacteria). The CAC has 2 principal purposes: (1) to harness intermediary metabolism to generate ATP (through oxidative phosphorylation and substrate-level phosphorylation not requiring a terminal electron acceptor, such as oxygen, eg, in hypoxia) and (2) to provide precursors for biosynthetic pathways. As traditionally envisaged (eg, in most biochemistry textbooks), the CAC begins with the condensation of oxaloacetate with acetyl-CoA, consisting of 8 sequential linear irreversible (eg, citrate synthase and the 2-oxoglutarate dehydrogenase complex) and reversible steps, ending with the regeneration of oxaloacetate (Figure 1A). These CAC steps are generally considered to take place predominantly in the mitochondrial matrix. Acetyl-CoA derived from glycolysis (via pyruvate dehydrogenase), from β-oxidation of fatty acids, and from the breakdown of ketone bodies and amino acids, generate the reducing equivalents NADH and FADH2 (reduced nicotinamide adenine dinucleotide and reduced flavin adenine dinucleotide, respectively), which, via the electron transport chain, synthesise ATP by oxidative phosphorylation. In addition there is a comparatively small but significant matrix substrate-level energy generation (guanosine triphosphate, GTP, convertible to ATP) not requiring oxygen. However, the CAC is more than a highly efficient sequence of spatially optimized reactions to degrade acetyl-CoA. Short sections of the CAC are close to thermodynamic equilibrium and are, therefore, bidirectional under different conditions. Krebs emphasized this reversibility by observing (albeit with relatively nonspecific inhibitors, such as malonic acid) that the enzymes interconverting succinate↔fumarate↔malate↔ B Pyruvate NAD+ + CoA-SH Pyruvate dehydrogenase NA DH + H+ + CO2 fatty acids Pyruvate CoA-SH Acetyl-CoA Citrate synthase Oxaloacetate H20 Acetyl-CoA cis-Aconitate Citrate H20 Aconitase Malate dehydrogenase Isocitrate Isocitrate dehydrogenase Malate fatty acids acetyl-CoA Aconitase NA DH + H+ NA D+ malonyl-CoA H20 Citrate CO2 proline arginine histidine Isocitrate aspartate NA DH + H+ Fumarate hydratase H20 cis-Aconitate Oxaloacetate NA D + Oxaloacetate Malate asparagine 2-oxoglutarate glutamate 2-oxoglutarate 2-oxoglutarate dehydrogenase Fumarate Succinate dehydrogenase QH2 Succinyl-CoA Succinyl-CoA synthetase Q Succinate GDP + Pi Fumarate NAD+ + CoA-SH NA DH + H+ + CO2 phenylalanine tyrosine Succinyl-CoA Succinate glutamine heme odd-chain fatty acids methionine valine isoleucine CoA-SH + GTP Figure 1. The citric acid cycle (CAC). A, An overview of CAC reactions. Observe that apart from 3 irreversible steps (citrate synthase, isocitrate dehydrogenase, and 2-oxoglutarate dehydrogenase), the rest of the CAC reactions are reversible, allowing reverse flux under certain conditions (such as in anoxia). B, Anaplerosis and cataplerosis of the CAC. Anaplerosis replenishes CAC intermediates, whereas cataplerosis allows production of various biosynthetic precursors making the CAC as a central metabolic hub, connecting diverse metabolic pathways. CoA-SH indicates reduced coenzyme A; FADH2, reduced flavin adenine dinucleotide; GTP, guanosine triphosphate; NAD+, oxidized nicotinamide adenine dinucleotide; NADH, reduced nicotinamide adenine dinucleotide; and QH2, reduced coenzyme Q. Czibik et al CAC in Cardioprotection 713 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 oxaloacetate are reversible. This reversibility facilitates the generation of precursors for glucose synthesis (from oxaloacetate via the pyruvate recycling pathway), fatty acid and cholesterol synthesis (from citrate), amino acid anabolism, nucleotides (via 2-oxoglutarate [2-OG]), and heme biosynthesis (via succinyl-CoA). In contrast to its perceived role as a perpetual rotor degrading acetyl-CoA, the CAC represents a highly versatile collection of reactions that can be concatenated in its entirety or in part to generate energy (oxidatively or without oxygen) and as a biosynthetic toolbox. Exemplifying the versatility of the CAC as a whole and individual reaction steps per se, dominant mutations in 2 of the 3 isocitrate dehydrogenases (IDH1 and IDH2) have been found to promote glioma, acute myeloid leukemia, chondrosarcoma, and other tumours. In the traditional conception, acetyl-CoA is thought to progress unidirectionally through the CAC. Instead, IDH1 (primarily cytoplasmic and NADP+ dependant) and IDH2 (primarily mitochondrial and NADP+ dependant) along with IDH3 promote the conventional oxidative decarboxylation of isocitrate to 2-OG but may also promote the reverse (reductive carboxylation). Reductively metabolized glutamine has been proposed to be a cellular carbon source for fatty acid synthesis during hypoxia or impaired mitochondrial respiration (eg, FH deficiency).34 Although these observations, adduced from ex vivo cancer cell preparations, remain controversial and potentially confounded by technical aspects of metabolic tracer studies,35 there is little doubt that mutated IDH isoforms also catalyze a neomorphic reaction converting 2-OG to the oncometabolite 2-hydroxyglutarate. This example confirms the complexity of a simple single CAC step and the consequences of its modification. The same flexibility provides potential therapeutic opportunities to mitigate hypoxia/ischemia.36 To maintain its activity and to compensate for metabolite leakage from the mitochondria,37 CAC flux can only be maintained if this cataplerotic activity constituting the removal of intermediates from the CAC is balanced by anaplerotic reactions replenishing CAC intermediates (Figure 1B).37,38 Breakdown of amino acids replenish 2-OG, succinyl-CoA, and oxaloacetate; odd-chain fatty acid oxidation generates succinyl-CoA; carboxylation of pyruvate by pyruvate carboxylase and malic enzyme produces oxaloacetate and malate, respectively. (Figure 1B).37 Adequate anaplerosis is especially important because the steady state concentrations of CAC intermediates are typically low in relation to the fluxes through the CAC.37–39 These uneven CAC intermediate pools are explained, in part, by the differential turnover rate of individual metabolic reactions, the differing thermodynamic/kinetic properties of each CAC step and differential mitochondrial inner membrane permeability. The measurement of both concentration and flux is technically challenging, even with dynamic tracer studies (for flux).38 For example, citrate, with the largest pool size (≈200 nmol/g), has a turnover time of minutes, whereas oxaloacetate with the smallest pool size (5–10 nmol/g) has a turnover of the order of 100× per minute.38 Consonant with metabolic control analysis, in the CAC, flux considerations dominate over steady-state thermodynamic principles per se.38 mitochondrial matrix 2-oxoglutarate NAD+ malate NADH Mdh2 oxaloacetate Got2 intermembrane space/cytosol 2-oxoglutarate Slc25a11 NAD+ malate NADH Mdh1 oxaloacetate glycolysis aspartate glutamate Slc1a3 aspartate Got1 glutamate Figure 2. The malate–aspartate shuttle. NADH (reduced nicotinamide adenine dinucleotide) formed during glycolysis needs reoxidizing in the cytosol, and the malate–aspartate shuttle acts as the major cardiac mechanism to transport the protons and electrons to the mitochondrial matrix where they, via the citric acid cycle and electron transport chain, are oxidized to water. Got1 and 2 indicates glutamic-oxaloacetatic transaminase 1 and 2; Mdh1 and 2, malate dehydrogenase 1 and 2; Slc1a3, glutamate/aspartate transporter; and Slc25a11, mitochondrial 2-oxoglutarate/malate carrier protein. To maintain locally high metabolite concentrations, CAC reactions are compartmentalized within the mitochondria. There may be further spatial subcompartmentalization in the vicinity of individual CAC enzymes to maximize local effective substrate concentrations and reaction efficiency. Specialized carrier proteins catalyze the transport of nucleotides, amino acids, inorganic ions, fatty acids, keto acids, and cofactors across the impermeable mitochondrial inner membrane. These transport steps are important to maintain a separate inner mitochondrial pool and micromilieu for ATP production, for amino acid breakdown, for macromolecular and heme biosynthesis, and for heat generation. An example of such a mitochondrial carrier mechanism is the malateaspartate shuttle (MAS). MAS is a key metabolic shuttle, active in the heart, which transfers electrons and protons from glycolysis-derived cytosolic NADH (to which the inner mitochondrial membrane is impervious) into the matrix for use by the electron transport chain using malate as an electron carrier. This involves a series of reactions involving the cytosolic reduction of oxaloacetate to malate, transport of malate into the mitochondrial matrix (in exchange for 2-OG), oxidation of malate to regenerate oxaloacetate with reduction of mitochondrial NAD+ to NADH. Oxaloacetate then undergoes transamination using glutamate as nitrogen donor to generate aspartate (and 2-OG), which exits the matrix via a glutamate–aspartate transporter40 (Figure 2). Although the influence of MAS in the heart in ischemia is complex and requires further clarification, its manipulation is likely to be important in ischemia-reperfusion injury.41 The MAS is the most important although not the only means to transport net protons and electrons from the cytoplasm to the mitochondrial matrix for oxidation. Like the MAS, the glycerol-3-phosphate shuttle helps reoxidise cytosolic NADH to NAD+, making it available for glycolysis. Should this turnover fail, accumulating cytosolic NADH would act as a brake to glycolysis in the face of a diminishing reducible NAD+ pool. Reducing equivalents generated during glycolysis and more substantially by the CAC are converted to ATP through the transfer of electrons to molecular O2 by the electron transport chain. Any lack of oxygen increases the NADH/NAD+ ratio, substrate inhibits glycolysis/CAC, and substantially disrupts 714 Circ Cardiovasc Genet October 2014 energy production. Accordingly, during hypoxia, anaerobic regeneration of NAD+ continues to occur, in part, through reoxidation of NADH by lactate dehydrogenase, which catalyzes electron transfer to pyruvate, rather than O2, to yield lactate. As oxidative phosphorylation and the closely coupled CAC flux are arrested, NADH accumulates. In the absence of molecular oxygen, even glycolytic acceleration may be inhibited by incomplete myocardial NADH reoxidation limiting the regeneration of NAD+ essential for continued glycolysis. As opposed to skeletal muscle, lactate dehydrogenase in the heart is predominantly the H-type, with increased susceptibility to form the abortive ternary complex lactate dehydrogenase-NAD-enol that competes with NADH.42 Thus, without alternative means to deplete NADH, the hypoxic metabolism would slow because of redox imbalance (increased NADH). As a corollary, modalities promoting NAD+ regeneration would potentially improve energetics.43,44 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 Noncanonical Functions of the CAC: Succinate Production in Hypoxia Ischemic cell death likely results from a rapid decline in intracellular ATP concentration, [ATP]IC, that is irreconcilable with viability.45 Maintenance of adequate cellular energy production is thus a fundamental and continual requirement for all tissues, with its disruption leading to significant clinical consequences. Metabolic studies in isolated hearts and muscle preparations and in natural states of extreme physiology (eg, diving mammals) have yielded important insights into cellular mechanisms, specifically emphasizing the CAC components, which maintain [ATP]IC and have broadened our understanding of the CAC. For decades, it has been recognized that hypoxia/ischemia confers substantial changes in CAC metabolites, most prominently succinate. For example, in 1970, while investigating the ability of CAC metabolites to improve cardiac performance in anoxia, Penney and Cascarano46 observed that perfusion of anoxic rat hearts with glucose and a combination of fumarate+malate+glutamate or oxaloacetate+2OG (2-oxoglutarate) enhanced glycogen and ATP levels over glucose perfusion alone, without increased glycolysis. In both CAC metabolite treatment groups, succinate levels were found consistently elevated. The authors concluded that mitochondrial energy production took place even during anoxia; however, the precise nature of this mitochondrial contribution to anoxic energy generation was undefined.46 Similarly, glutamate and aspartate were recognized to lead to increased succinate levels in skeletal muscle before the discovery of the CAC itself.47 The importance of this mechanism was implied by its evolutionary conservation. Hochachka et al48 observed that in diving mammals, blood concentrations of aspartate and 2-OG (2-oxoglutarate) levels decreased, whereas those of lactate, alanine, and succinate increased after diving (a hypoxic manoeuvre). They proposed a model of 2 interlinked, oxygenindependent pathways (Figure 3),48 whereby NADH produced during glycolysis and through anterograde carbon flow through 2-OG dehydrogenase generating GTP and succinate is coupled to NADH depletion through reducing aspartate-derived Glucose-6P Aspartate Fructose-6P 2-oxoglutarate Fructose-1,6DP NAD+ Triose-P Pi NADH NAD+ NADH NADH NAD+ Oxaloacetate Glutamate Malate Diphosphoglycerate-1,3P Phosphoenolpyruvate NADH Pyruvate Glutamate 2-oxoglutarate NAD+ Lactate Alanine Malate 2-oxoglutarate CO2 Fumarate NAD+ FPred NADH FPox CoA-SH Succinyl-CoA GDP + Pi cytoplasm mitochondrion ADP + Pi ATP Succinate CoA-SH GTP Succinate Figure 3. Modified adaptation of Hochacka’s model of energy production by the citric acid cycle (CAC) in hypoxia.48 In this model, anoxic succinate accumulation was suggested through an oxidative (via pyruvate, 2-oxoglutarate, and succinyl-CoA) and reductive (via aspartate, oxaloacetate, malate, and fumarate) pathway, with CAC-dependent energy generation by substratelevel phosphorylation in addition to glycolytic ATP generation. CoA-SH indicates reduced coenzyme A; FPox, oxidized flavoprotein; FPred, reduced flavoprotein; and GTP, guanosine triphosphate. oxaloacetate to malate. The malate is converted to fumarate and ultimately succinate contrasting with the traditional conception of carbon flow in the CAC (because in the context of lacking oxygen normal CAC flux ceases).48 Other mechanisms contributing to NADH depletion may include mitochondrial diaphorases.49 Increased succinate production has also been observed in hypoxic cardiac myocytes.27 Although there are controversies about the pertinence of this model to IR injury,43,50–53 at least under some circumstances, loading of the CAC using glutamate, fumarate, and aspartate have generally been successful but may not be clinically tractable. This strategy is also not without jeopardy—the energetic benefit of channelling amino acids to succinate may be mitigated by the release of ROS at reperfusion resulting from a burst of FADH2 in the context of too sudden forward flow of succinate through succinate dehydrogenase (complex II). Therapies Modifying CAC Intermediates as Potential Therapies of IR Recognizing the potential value of modifying, specifically augmenting, CAC intermediates, several strategies have been investigated. One readily translatable is the indirect augmentation of CAC intermediates using glutmate/glutamine.54 Czibik et al CAC in Cardioprotection 715 Glutamate/glutamine has exhibited variable promise in animal and human models of myocardial IR, especially as a constituent of cardioplegia in coronary surgery.55–58 Another approach is to augment CAC intermediates using anaplerotic precursors directly. Despite successfully increasing myocardial CAC intermediates, dipropionylcysteine ethyl ester and heptanoate failed to protect the myocardium,59,60 in part, perhaps because of the differing protocols of drug infusion and myocardial ischemia. In contrast, dipyruvyl-acetyl-glycerol decreases myocardial infarct size in the pig.61 This is consistent with the observation that fumarate-enriched cardioplegia results in complete functional recovery of immature myocardium.62 Signaling Roles of the CAC: Insights From Renal Tumours Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 Notwithstanding the controversies surrounding the energetic merits of succinate generation through mitochondrial substrate-level phosphorylation, increased succinate production has been consistently identified in different tissues, in different models in hypoxia/IR. In addition to its metabolic role, elevated succinate seen ubiquitously in ischemia is likely to activate its cognate cell surface receptor—G-protein–coupled receptor 91 (Gpr91).63 Succinate acting through this receptor contributes to retinal neovascularization and acting through prostaglandin E receptor 2–prostaglandin E receptor 4 modifies post–hypoxia-ischemic injury in the brain64, emphasizing A Normoxia Hydroxylation PHD HIFα the pleotropic contributions of CAC metabolites to IR injury.63,64 The discovery of normoxic HIF-1α stabilization by elevated fumarate levels in hereditary HLRCC and elevated succinate in hereditary paraganglioma with pheochromocytomas resulting from deficient FH and SDH (succinate dehydrogenase)28,29,65 respectively, potentially indicates another signaling role for CAC metabolites in the response to IR. The mechanism underlying normoxic HIF-1α stabilization in these tumors is thought to be substrate competition of the accumulating CAC metabolites with 2-OG. The latter is a key cofactor for prolyl hydroxylase domain 1 to 3 proteins66,67 that regulate HIF-1α by hydroxylation under normoxic conditions, promoting its proteosomal destruction (Figure 4A). This mechanism is supported by the finding that addition of excess 2-OG is able to out-compete fumarate, thereby reactivating prolyl hydroxylase domains and hydroxylating HIF-1α.68 The possibility that different metabolic states— signaled by varying levels of CAC intermediates—can regulate the central transcriptional coordinator of the cellular response to hypoxia, resonates with the observation that CAC metabolites are channelled toward succinate during ischemia and has important consequences beyond cancer, in other states of hypoxia/ischemia. Analogous HIF-1α augmentation by succinate may be germane to cardiac ischemia because mice overexpressing HIF-1α in the heart, when subjected to Proteasomal Degradation VHL HO- HIFα 2-oxoglutarate Pseudohypoxia Fumarate and Succinate Hydroxylation HIFα PHD HIFα HIFα HIF-target gene expression 2-oxoglutarate B At Baseline Electrophiles e.g Fumarate Cytoplasmic Sequestration KEAP1 and Proteasomal Degradation NRF2 In the presence of Electrophiles Electrophiles e.g Fumarate KEAP1 MAF NRF2 NRF2 NRF2-target gene expression Figure 4. Signaling functions of citric acid cycle (CAC) intermediates. A, The hypoxia-inducible factor (HIF)-1α-hypoxia pathway. The key in regulation of HIF-1α stability is an O2- and 2-oxoglutaratedependent proline hydroxylation. When in excess, fumarate and succinate can out-compete 2-oxoglutarate and can stabilize HIF-1α protein in normoxia. B, The Nrf2-antioxidant pathway. The critical event in Nrf2 activation is when specific cysteine residues on Keap1 react with electrophiles, such as fumarate, and consequently Keap1 releases Nrf2. KEAP1 indicates Kelch-like ECH-associated protein 1; NRF2, nuclear factor (erythroid-derived 2)-like 2; PHD, prolyl hydroxylase domain; and VHL, von Hippel-Lindau tumor suppressor. 716 Circ Cardiovasc Genet October 2014 coronary artery ligation, exhibited a reduction in infarct size and improved postischemic recovery.69 Succinate-augmented HIF-1α levels may contribute to IPC because mice with reduced HIF-1α cannot be preconditioned.70,71 Fumarate Is Cardioprotective via Activation of the Nrf2-Antioxidant Pathway Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 As with succinate, the cardioprotective influence of fumarate has been recognized in both immature62 and adult hearts;72 however, it is likely that the contribution of fumarate to the coupled reductive pathway originally proposed by Hochachka et al48 would not suffice to account for the cardioprotective effect completely.72 Furthermore, the cardioprotective influence observed with exogenous nonesterified fumarate in adult rat hearts was relatively modest,72 raising the possibility of inadequate intracellular penetration of fumarate from the perfusate.32 Analogous to its role in normoxic HIF-1α augmentation, we wondered whether CAC metabolites, such as fumarate, may activate other cytoprotective transcriptional programmes. To augment myocardial fumarate levels reliably, we generated a model of cardiac FH deficiency by crossing mice bearing LoxP sequences flanking exons 2 to 3 of the Fh1 gene with mice carrying Cre recombinase under the ventricular cardiomyocyte-specific Mlc2v promoter. By interrupting the conversion of fumarate to malate, the resulting mice represented a genetic model of augmented cardiac fumarate concentrations. Mice with cardiac Fh1 deficiency were viable and healthy (despite a disrupted CAC) until ≈3 to 4 months.32 The phosphocreatine to ATP ratio (a readout of energetics) was unaltered when compared with control hearts consistent with their viability. Successful Fh1 knockout in the cardiac myocytes was confirmed at both mRNA and protein level. These hearts exhibited increased fumarate levels when compared with control (Fh1 fl/fl, no Cre) hearts. The increases were significant and consistent though modest in magnitude (×1.6 fold of controls in total heart preparations). When subject to ex vivo IR (40 minutes of global ischemia followed by 60 minutes of reperfusion), Fh1 knockout hearts exhibited a marked reduction in mean infarct size from 37% in control hearts to 17% in Fh1 knockout hearts. Assessment of markers of myocardial injury corroborated the robust cardioprotection in Fh1 knockout hearts. A time-course of interstitial metabolite profiling detected reduced ischemic release of succinate, glutamate, and adenosine in Fh1 knockout hearts, a pattern that has been associated with attenuated cardiac injury.73,74 In other models of fumarate augmentation, either using FH-deficient tumors or increased cellular fumarate through the application of cell permeable fumarate analogues, activation of the Keap1-Nrf2-antioxidant pathway has been observed (Figure 4B).31,75 Nrf2 is a transcription factor that coordinates the defense against oxidative stress by activating antioxidant response element genes.76 In unstimulated cells, Nrf2 is sequestered in the cytoplasm by Keap1, promoting Nrf2’s proteosomal destruction.77 On cellular overload with ROS or electrophiles, reactive cysteine residues on Keap1 are modified, resulting in release of Nrf2, its translocation to the nucleus, and heterodimerization with small Maf proteins to transactivate antioxidant response element genes.77 By acting as an electrophile via its unsaturated bond, fumarate (but not succinate which is saturated) binds to the reactive cysteine residues of Keap1, forming an irreversible chemical modification of S-(2-succinyl)-cysteine (2SC), termed succination.78 Proteomic assessment of FH-deficient murine embryonic fibroblasts found a variety of proteins altered by this novel post-translational modification, many of which had metabolic functions and were mitochondrial in location.79 Although the functionality of succination remains generally undefined, the effect of succinated cysteine residues binding an obligatory [Fe4S4]2+ cluster in the CAC enzyme aconitase 2 has been shown to be a dose-dependent inhibition of aconitase activity.79 The iron–sulfur cluster of aconitase 2 is also highly sensitive to oxidation by superoxide, acting as a mitochondrial sensor of oxidative stress.80 Systematic expression profiling of our FH-deficient hearts, consistent with the cancer literature,31,75 supported the observation that fumarate augmentation upregulated several canonical Nrf2 target and coregulated genes, including glutathione S-transferases, methylenetetrahydrofolate dehydrogenase, NAD(P)H:quinone oxidoreductase 1 and, perhaps importantly, heme oxygenase 1 (Hmox1). Examination of succination in Fh1 knockout hearts with an anti-2SC antibody revealed substantially increased succination. This supports the hypothesis that succination of Keap1 may be the likely mechanism for the observed reductions in Keap1 protein and the enhanced stabilization/translocation of Nrf2. Substantial evidence supports the hypothesis that Hmox1 activation is robustly cardioprotective. This inducible cytoprotective enzyme catabolizes the pro-oxidant heme to free iron, carbon monoxide (CO) and biliverdin, with the latter then converted to bilirubin.81 Bilirubin itself is a potent antioxidant, whereas carbon monoxide is a vasodilator with additional anti-inflammatory and antiapoptotic properties.81,82 Both CO and bilirubin protect against cardiac IR injury; the former via activation of p38 MAPK and Akt kinases,2,83 the latter likely via an antioxidant mechanism.84 Although mice heterozygous for Hmox1 were found to be susceptible to IR injury,85 cardiac-restricted overexpression of Hmox1 has been shown to attenuate infarct size both ex vivo and in vivo, with reduced oxidative stress, inflammatory cell infiltration,81 left ventricular dysfunction, and apoptosis.86 Upregulation of Hmox1, coupled with heme resulting from the cataplerosis of succinyl-CoA predicted by our own computational modeling32 and that of others,87 raised the possibility of Hmox1 contributing to the cardioprotection. To address this, we injected control and Fh1 knockout animals with vehicle or zinc deuteroporpyrin 2-4-bis ethylenglycol (ZnBG), a specific heme oxygenase inhibitor88,89 before ex vivo IR. Pretreatment with ZnBG had no effect on infarct size in control hearts, but negated the cardioprotection observed in Fh1 knockout hearts. To assess whether our findings in Fh1 knockout mice were translatable, we used dimethyl fumarate (DMF), an orally available and cell-permeable version of fumarate67 already in clinical use to treat patients with psoriasis and multiple sclerosis.76 Treatment of atrial cardiomyocyte-derived HL-1 cells with DMF induced nuclear translocation of Nrf2. When Czibik et al CAC in Cardioprotection 717 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 administered orally to wild-type mice, dimethylfumarate recapitulated much of the Nrf2 target profiling observed in untreated Fh1 knockout hearts. When subject to IR, hearts from DMF-pretreated wild-type mice displayed a ≈75% reduction in infarct size to 9.3% when compared with 36.9% in vehicle pretreated wild-type hearts, accompanied by an improvement in postischemic coronary flow. To determine whether DMF's infarct-sparing effect translated to an in vivo model, wild-type mice pretreated with oral DMF or vehicle underwent left anterior descending coronary artery ligation with subsequent evaluation of infarct size. A significant reduction in infarct size was observed in the DMF-treated group. This protective effect of DMF was absent in Nrf2 knockout mice, indicating the critical role played by Nrf2 in mediating DMF-conferred cardioprotection.32 These findings do not preclude the possibility that the cardioprotective potential of fumarate is also dependent on other pathways. Motivated by findings in the cancer literature, we examined whether increased fumarate was sufficient to activate the HIF hypoxia pathway but found no evidence to support this.32 There are several possibilities for the apparent discrepancy: (1) Fumarate levels of Fh1 knockout murine embryonic fibroblasts are 100-fold higher than in wild-type murine embryonic fibroblasts,79 suggesting that an estimated 2.2-fold increase in fumarate observed in Fh1 knockout cardiac myocytes (1.6-fold in whole hearts) might be insufficient to outcompete 2-OG; (2) prolyl hydroxylase domain 2, the major HIF-1α hydroxylase,90 has a much higher Kd for fumarate than for 2-OG; accordingly, fumarate levels have to exceed 2-OG greatly for binding to prolyl hydroxylase domain 266; (3) as an alternative mechanism to substrate competition, Sullivan et al91 proposed that elevated levels of fumarate resulted in increased succination and inactivation of the antioxidant glutathione to form GSF, which—by acting as an inhibitory substrate to glutathione reductase—enhances mitochondrial ROS levels, serving to stabilize HIF-1α. In Fh1 knockout cardiomyocytes, the modestly elevated fumarate is unlikely to have altered superoxide levels directly. Notwithstanding these considerations, endogenous antioxidant protection via activation of the Nrf2-dependent arsenal of cytoprotective genes is desirable in the setting of reperfusion injury, where oxidative stress is recognized as a major pathogenic contributor. The preclinical evidence for cardioprotection using the orally available, cellpermeable, and clinically safe DMF provides a tangible agent for clinical testing in the setting of acute coronary syndromes or predictable myocardial injury (eg, cardiac surgery).5,32 Conclusions and Future Directions As outlined above, there is substantial evidence, accumulating over almost a century, that CAC intermediates change dramatically during the course of IR injury. The recognition that these changes, most prominently succinate production, may be beneficial has been substantially enhanced by the recognition that succinate and related metabolites have additional and perhaps more potent effects than ATP generation. These include cell surface receptor activation (eg, Gpr91), HIF-1α activation, and Nrf2 liberation from Keap1. However, relatively simple strategies to exploit the metabolic benefits of CAC intermediate (eg, modification through the provision of feedstock amino acids) have proved clinically challenging with variable efficacy. Alternative metabolic strategies using similar CAC-related products that will augment Hmox1 activity (either through increasing its substrate haem or increasing enzymatic activity) may be germane and are the subject of investigation. Sources of Funding This work was supported by the British Heart Foundation. A.Yavari is supported by the UK Department of Health's National Institute for Health Research. Disclosures H. Ashrafian has received an unrestricted research grant from SBIALA, Japan. The other authors report no conflicts. References 1. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–2398. 2. Yellon DM, Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med. 2007;357:1121–1135. 3. Nichols M, Townsend N, Scarborough P, Rayner M. Trends in age-specific coronary heart disease mortality in the European Union over three decades: 1980-2009. Eur Heart J. 2013;34:3017–3027. 4. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245. 5. van Waes JA, Nathoe HM, de Graaff JC, Kemperman H, de Borst GJ, Peelen LM, et al; Cardiac Health After Surgery (CHASE) Investigators. Myocardial injury after noncardiac surgery and its association with shortterm mortality. Circulation. 2013;127:2264–2271. 6. Abifadel M, Varret M, Rabès JP, Allard D, Ouguerram K, Devillers M, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34:154–156. 7.Bhattacharya S, Wilson TM, Wojciechowski AP, Volpe CP, Scott J. Hypervariable polymorphism in the APOC3 gene. Nucleic Acids Res. 1991;19:4799. 8. Masucci-Magoulas L, Goldberg IJ, Bisgaier CL, Serajuddin H, Francone OL, Breslow JL, et al. A mouse model with features of familial combined hyperlipidemia. Science. 1997;275:391–394. 9. Vinten-Johansen J, Zhao ZQ, Jiang R, Zatta AJ, Dobson GP. Preconditioning and postconditioning: innate cardioprotection from ischemia-reperfusion injury. J Appl Physiol (1985). 2007;103:1441–1448. 10.Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–1136. 11. Tissier R, Berdeaux A, Ghaleh B, Couvreur N, Krieg T, Cohen MV, et al. Making the heart resistant to infarction: how can we further decrease infarct size? Front Biosci. 2008;13:284–301. 12. Bolli R. Preconditioning: a paradigm shift in the biology of myocardial ischemia. Am J Physiol Heart Circ Physiol. 2007;292:H19–H27. 13. Boengler K, Schulz R, Heusch G. Loss of cardioprotection with ageing. Cardiovasc Res. 2009;83:247–261. 14. Ludman AJ, Yellon DM, Hausenloy DJ. Cardiac preconditioning for ischaemia: lost in translation. Dis Model Mech. 2010;3:35–38. 15. Whittington HJ, Harding I, Stephenson CI, Bell R, Hausenloy DJ, Mocanu MM, et al. Cardioprotection in the aging, diabetic heart: the loss of protective Akt signalling. Cardiovasc Res. 2013;99:694–704. 16.Sodi-Pallares D, Testelli MR, Fishleder BL, Bisteni A, Medrano GA, Friedland C, et al. Effects of an intravenous infusion of a potassiumglucose-insulin solution on the electrocardiographic signs of myocardial infarction. A preliminary clinical report. Am J Cardiol. 1962;9:166–181. 17. Morgan HE, Henderson MJ, Regen DM, Park CR. Regulation of glucose uptake in muscle. I. The effects of insulin and anoxia on glucose transport and phosphorylation in the isolated, perfused heart of normal rats. J Biol Chem. 1961;236:253–261. 718 Circ Cardiovasc Genet October 2014 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 18. Randle PJ, Garland PB, Hales CN, Newsholme EA. The glucose fattyacid cycle. Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet. 1963;1:785–789. 19. Jonassen AK, Sack MN, Mjøs OD, Yellon DM. Myocardial protection by insulin at reperfusion requires early administration and is mediated via Akt and p70s6 kinase cell-survival signaling. Circ Res. 2001;89:1191–1198. 20. Zhu P, Lu L, Xu Y, Greyson C, Schwartz GG. Glucose-insulin-potassium preserves systolic and diastolic function in ischemia and reperfusion in pigs. Am J Physiol Heart Circ Physiol. 2000;278:H595–H603. 21. Angelos MG, Murray HN, Gorsline RT, Klawitter PF. Glucose, insulin and potassium (GIK) during reperfusion mediates improved myocardial bioenergetics. Resuscitation. 2002;55:329–336. 22.Rogers WJ, Stanley AW Jr, Breinig JB, Prather JW, McDaniel HG, Moraski RE, et al. Reduction of hospital mortality rate of acute myocardial infarction with glucose-insulin-potassium infusion. Am Heart J. 1976;92:441–454. 23.Howell NJ, Ashrafian H, Drury NE, Ranasinghe AM, Contractor H, Isackson H, et al. Glucose-insulin-potassium reduces the incidence of low cardiac output episodes after aortic valve replacement for aortic stenosis in patients with left ventricular hypertrophy: results from the Hypertrophy, Insulin, Glucose, and Electrolytes (HINGE) trial. Circulation. 2011;123:170–177. 24. Malmberg K, Rydén L, Efendic S, Herlitz J, Nicol P, Waldenström A, et al. Randomized trial of insulin-glucose infusion followed by subcutaneous insulin treatment in diabetic patients with acute myocardial infarction (DIGAMI study): effects on mortality at 1 year. J Am Coll Cardiol. 1995;26:57–65. 25. Maroko PR, Libby P, Sobel BE, Bloor CM, Sybers HD, Shell WE, et al. Effect of glucose-insulin-potassium infusion on myocardial infarction following experimental coronary artery occlusion. Circulation. 1972;45:1160–1175. 26. Kloner RA, Nesto RW. Glucose-insulin-potassium for acute myocardial infarction: continuing controversy over cardioprotection. Circulation. 2008;117:2523–2533. 27. Taegtmeyer H. Metabolic responses to cardiac hypoxia. Increased production of succinate by rabbit papillary muscles. Circ Res. 1978;43:808–815. 28. Isaacs JS, Jung YJ, Mole DR, Lee S, Torres-Cabala C, Chung YL, et al. HIF overexpression correlates with biallelic loss of fumarate hydratase in renal cancer: novel role of fumarate in regulation of HIF stability. Cancer Cell. 2005;8:143–153. 29. Pollard PJ, Brière JJ, Alam NA, Barwell J, Barclay E, Wortham NC, et al. Accumulation of Krebs cycle intermediates and over-expression of HIF1alpha in tumours which result from germline FH and SDH mutations. Hum Mol Genet. 2005;14:2231–2239. 30. Czibik G. Complex role of the HIF system in cardiovascular biology. J Mol Med (Berl). 2010;88:1101–1111. 31. Adam J, Hatipoglu E, O’Flaherty L, Ternette N, Sahgal N, Lockstone H, et al. Renal cyst formation in Fh1-deficient mice is independent of the Hif/ Phd pathway: roles for fumarate in KEAP1 succination and Nrf2 signaling. Cancer Cell. 2011;20:524–537. 32. Ashrafian H, Czibik G, Bellahcene M, Aksentijević D, Smith AC, Mitchell SJ, et al. Fumarate is cardioprotective via activation of the Nrf2 antioxidant pathway. Cell Metab. 2012;15:361–371. 33. Krebs HA. The citric acid cycle and the Szent-Györgyi cycle in pigeon breast muscle. Biochem J. 1940;34:775–779. 34. Mullen AR, Wheaton WW, Jin ES, Chen PH, Sullivan LB, Cheng T, et al. Reductive carboxylation supports growth in tumour cells with defective mitochondria. Nature. 2012;481:385–388. 35.Fan J, Kamphorst JJ, Rabinowitz JD, Shlomi T. Fatty acid labeling from glutamine in hypoxia can be explained by isotope exchange without net reductive isocitrate dehydrogenase (IDH) flux. J Biol Chem. 2013;288:31363–31369. 36. DeBerardinis RJ, Thompson CB. Cellular metabolism and disease: what do metabolic outliers teach us? Cell. 2012;148:1132–1144. 37. Brunengraber H, Roe CR. Anaplerotic molecules: current and future. J Inherit Metab Dis. 2006;29:327–331. 38. Des Rosiers C, Labarthe F, Lloyd SG, Chatham JC. Cardiac anaplerosis in health and disease: food for thought. Cardiovasc Res. 2011;90: 210–219. 39. LaNoue K, Nicklas WJ, Williamson JR. Control of citric acid cycle activity in rat heart mitochondria. J Biol Chem. 1970;245:102–111. 40. Locasale JW, Cantley LC. Metabolic flux and the regulation of mammalian cell growth. Cell Metab. 2011;14:443–451. 41. Støttrup NB, Løfgren B, Birkler RD, Nielsen JM, Wang L, Caldarone CA, et al. Inhibition of the malate-aspartate shuttle by pre-ischaemic aminooxyacetate loading of the heart induces cardioprotection. Cardiovasc Res. 2010;88:257–266. 42.Fromm H. Determination of dissociation constants of coenzymes and abortive ternary complexes with rabbit muscle lactate dehydrogenase from fluorescence measurements. J Biol Chem. 1963;238:2938–2944. 43.Snaith CD, Wright G, Lofkin M. The effects of aspartate and 2-oxoglutarate upon glycolytic energy metabolites and mechanical recovery following global ischaemia in isolated rat hearts. J Mol Cell Cardiol. 1992;24:305–315. 44. Pisarenko OI, Studneva IM, Shulzhenko VS, Korchazhkina OV, Kapelko VI. Substrate accessibility to cytosolic aspartate aminotransferase improves posthypoxic recovery of isolated rat heart. Biochem Mol Med. 1995;55:138–148. 45. Weerasinghe P, Buja LM. Oncosis: an important non-apoptotic mode of cell death. Exp Mol Pathol. 2012;93:302–308. 46. Penney DG, Cascarano J. Anaerobic rat heart. Effects of glucose and tricarboxylic acid-cycle metabolites on metabolism and physiological performance. Biochem J. 1970;118:221–227. 47. Needham DM. A quantitative study of succinic acid in muscle: glutamic and aspartic acids as precursors. Biochem J. 1930;24:208–227. 48. Hochachka PW, Owen TG, Allen JF, Whittow GC. Multiple end products of anaerobiosis in diving vertebrates. Comp Biochem Physiol B. 1975;50:17–22. 49. Kiss G, Konrad C, Pour-Ghaz I, Mansour JJ, Németh B, Starkov AA, et al. Mitochondrial diaphorases as NAD⁺ donors to segments of the citric acid cycle that support substrate-level phosphorylation yielding ATP during respiratory inhibition. FASEB J. 2014;28:1682–1697. 50. Hohl C, Oestreich R, Rösen P, Wiesner R, Grieshaber M. Evidence for succinate production by reduction of fumarate during hypoxia in isolated adult rat heart cells. Arch Biochem Biophys. 1987;259:527–535. 51. Peuhkurinen KJ, Takala TE, Nuutinen EM, Hassinen IE. Tricarboxylic acid cycle metabolites during ischemia in isolated perfused rat heart. Am J Physiol. 1983;244:H281–H288. 52. Sanborn T, Gavin W, Berkowitz S, Perille T, Lesch M. Augmented conversion of aspartate and glutamate to succinate during anoxia in rabbit heart. Am J Physiol. 1979;237:H535–H541. 53. Wiesner RJ, Deussen A, Borst M, Schrader J, Grieshaber MK. Glutamate degradation in the ischemic dog heart: contribution to anaerobic energy production. J Mol Cell Cardiol. 1989;21:49–59. 54. Pietersen HG, Langenberg CJ, Geskes G, Soeters PB, Wagenmakers AJ. Glutamate metabolism of the heart during coronary artery bypass grafting. Clin Nutr. 1998;17:73–75. 55. Jessen ME, Kovarik TE, Jeffrey FM, Sherry AD, Storey CJ, Chao RY, et al. Effects of amino acids on substrate selection, anaplerosis, and left ventricular function in the ischemic reperfused rat heart. J Clin Invest. 1993;92:831–839. 56. Langenberg CJ, Pietersen HG, Geskes G, Wagenmakers AJ, Lange SD, Schouten HJ, et al. The effect of glutamate infusion on cardiac performance is independent of changes in metabolism in patients undergoing routine coronary artery bypass surgery. Clin Sci (Lond). 2001;101:573–580. 57. Lomivorotov VV, Efremov SM, Shmirev VA, Ponomarev DN, Lomivorotov VN, Karaskov AM. Glutamine is cardioprotective in patients with ischemic heart disease following cardiopulmonary bypass. Heart Surg Forum. 2011;14:E384–E388. 58. Lomivorotov VV, Efremov SM, Shmirev VA, Ponomarev DN, Svyatchenko AV, Deryagin MN, et al. Does glutamine promote benefits for patients with diabetes mellitus scheduled for cardiac surgery? Heart Lung Circ. 2013;22:360–365. 59. Kasumov T, Sharma N, Huang H, Kombu RS, Cendrowski A, Stanley WC, et al. Dipropionylcysteine ethyl ester compensates for loss of citric acid cycle intermediates during post ischemia reperfusion in the pig heart. Cardiovasc Drugs Ther. 2009;23:459–469. 60. Okere IC, McElfresh TA, Brunengraber DZ, Martini W, Sterk JP, Huang H, et al. Differential effects of heptanoate and hexanoate on myocardial citric acid cycle intermediates following ischemia-reperfusion. J Appl Physiol (1985). 2006;100:76–82. 61. Stanley WC, Kivilo KM, Panchal AR, Hallowell PH, Bomont C, Kasumov T, et al. Post-ischemic treatment with dipyruvyl-acetyl-glycerol decreases myocardial infarct size in the pig. Cardiovasc Drugs Ther. 2003;17:209–216. 62. Pearl JM, Hiramoto J, Laks H, Drinkwater DC Jr, Chang PA. Fumarateenriched blood cardioplegia results in complete functional recovery of immature myocardium. Ann Thorac Surg. 1994;57:1636–1641. Czibik et al CAC in Cardioprotection 719 Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 63. Sapieha P, Sirinyan M, Hamel D, Zaniolo K, Joyal JS, Cho JH, et al. The succinate receptor GPR91 in neurons has a major role in retinal angiogenesis. Nat Med. 2008;14:1067–1076. 64. Hamel D, Sanchez M, Duhamel F, Roy O, Honore JC, Noueihed B, Zhou T, Nadeau-Vallee M, Hou X, Lavoie JC, Mitchell G, Mamer OA, Chemtob S et al. G-protein-coupled receptor 91 and succinate are key contributors in neonatal postcerebral hypoxia-ischemia recovery. Arterioscler Thromb Vasc Biol. 2014;34:285–293. 65. Selak MA, Armour SM, MacKenzie ED, Boulahbel H, Watson DG, Mansfield KD, et al. Succinate links TCA cycle dysfunction to oncogenesis by inhibiting HIF-alpha prolyl hydroxylase. Cancer Cell. 2005;7:77–85. 66. Hewitson KS, Liénard BM, McDonough MA, Clifton IJ, Butler D, Soares AS, et al. Structural and mechanistic studies on the inhibition of the hypoxia-inducible transcription factor hydroxylases by tricarboxylic acid cycle intermediates. J Biol Chem. 2007;282:3293–3301. 67. Koivunen P, Hirsilä M, Remes AM, Hassinen IE, Kivirikko KI, Myllyharju J. Inhibition of hypoxia-inducible factor (HIF) hydroxylases by citric acid cycle intermediates: possible links between cell metabolism and stabilization of HIF. J Biol Chem. 2007;282:4524–4532. 68. MacKenzie ED, Selak MA, Tennant DA, Payne LJ, Crosby S, Frederiksen CM, et al. Cell-permeating alpha-ketoglutarate derivatives alleviate pseudohypoxia in succinate dehydrogenase-deficient cells. Mol Cell Biol. 2007;27:3282–3289. 69. Kido M, Du L, Sullivan CC, Li X, Deutsch R, Jamieson SW, et al. Hypoxia-inducible factor 1-alpha reduces infarction and attenuates progression of cardiac dysfunction after myocardial infarction in the mouse. J Am Coll Cardiol. 2005;46:2116–2124. 70.Cai Z, Zhong H, Bosch-Marce M, Fox-Talbot K, Wang L, Wei C, et al. Complete loss of ischaemic preconditioning-induced cardioprotection in mice with partial deficiency of HIF-1 alpha. Cardiovasc Res. 2008;77:463–470. 71. Eckle T, Köhler D, Lehmann R, El Kasmi K, Eltzschig HK. Hypoxiainducible factor-1 is central to cardioprotection: a new paradigm for ischemic preconditioning. Circulation. 2008;118:166–175. 72. Laplante A, Vincent G, Poirier M, Des Rosiers C. Effects and metabolism of fumarate in the perfused rat heart. A 13C mass isotopomer study. Am J Physiol. 1997;272(1 Pt 1):E74–E82. 73. Vincent G, Comte B, Poirier M, Rosiers CD. Citrate release by perfused rat hearts: a window on mitochondrial cataplerosis. Am J Physiol Endocrinol Metab. 2000;278:E846–E856. 74.Wikström BG, Ronquist G, Waldenström A. Dynamics of myocardial metabolism in the preconditioned porcine heart studied using continuous microdialysis. Eur Heart J. 1995;16:563–569. 75. Ooi A, Wong JC, Petillo D, Roossien D, Perrier-Trudova V, Whitten D, et al. An antioxidant response phenotype shared between hereditary and sporadic type 2 papillary renal cell carcinoma. Cancer Cell. 2011;20:511–523. 76. Gold R, Kappos L, Arnold DL, Bar-Or A, Giovannoni G, Selmaj K, et al; DEFINE Study Investigators. Placebo-controlled phase 3 study of oral BG12 for relapsing multiple sclerosis. N Engl J Med. 2012;367:1098–1107. 77. Hayes JD, McMahon M, Chowdhry S, Dinkova-Kostova AT. Cancer chemoprevention mechanisms mediated through the Keap1-Nrf2 pathway. Antioxid Redox Signal. 2010;13:1713–1748. 78. Frizzell N, Lima M, Baynes JW. Succination of proteins in diabetes. Free Radic Res. 2011;45:101–109. 79. Ternette N, Yang M, Laroyia M, Kitagawa M, O’Flaherty L, Wolhulter K, et al. Inhibition of mitochondrial aconitase by succination in fumarate hydratase deficiency. Cell Rep. 2013;3:689–700. 80. Gardner PR. Aconitase: sensitive target and measure of superoxide. Methods Enzymol. 2002;349:9–23. 81. Yet SF, Tian R, Layne MD, Wang ZY, Maemura K, Solovyeva M, et al. Cardiac-specific expression of heme oxygenase-1 protects against ischemia and reperfusion injury in transgenic mice. Circ Res. 2001;89:168–173. 82. Melo LG, Agrawal R, Zhang L, Rezvani M, Mangi AA, Ehsan A, et al. Gene therapy strategy for long-term myocardial protection using adenoassociated virus-mediated delivery of heme oxygenase gene. Circulation. 2002;105:602–607. 83. Fujimoto H, Ohno M, Ayabe S, Kobayashi H, Ishizaka N, Kimura H, et al. Carbon monoxide protects against cardiac ischemia–reperfusion injury in vivo via MAPK and Akt–eNOS pathways. Arterioscler Thromb Vasc Biol. 2004;24:1848–1853. 84. Clark JE, Foresti R, Sarathchandra P, Kaur H, Green CJ, Motterlini R. Heme oxygenase-1-derived bilirubin ameliorates postischemic myocardial dysfunction. Am J Physiol Heart Circ Physiol. 2000;278:H643–H651. 85. Yoshida T, Maulik N, Ho YS, Alam J, Das DK. H(mox-1) constitutes an adaptive response to effect antioxidant cardioprotection: A study with transgenic mice heterozygous for targeted disruption of the Heme oxygenase-1 gene. Circulation. 2001;103:1695–1701. 86. Vulapalli SR, Chen Z, Chua BH, Wang T, Liang CS. Cardioselective overexpression of HO-1 prevents I/R-induced cardiac dysfunction and apoptosis. Am J Physiol Heart Circ Physiol. 2002;283:H688–H694. 87. Frezza C, Zheng L, Folger O, Rajagopalan KN, MacKenzie ED, Jerby L, et al. Haem oxygenase is synthetically lethal with the tumour suppressor fumarate hydratase. Nature. 2011;477:225–228. 88. Vreman HJ, Lee OK, Stevenson DK. In vitro and in vivo characteristics of a heme oxygenase inhibitor: ZnBG. Am J Med. Sci. 1991;302:335–341. 89. Czibik G, Sagave J, Martinov V, Ishaq B, Sohl M, Sefland I, et al. Cardioprotection by hypoxia-inducible factor 1 alpha transfection in skeletal muscle is dependent on haem oxygenase activity in mice. Cardiovasc Res. 2009;82:107–114. 90. Berra E, Benizri E, Ginouvès A, Volmat V, Roux D, Pouysségur J. HIF prolyl-hydroxylase 2 is the key oxygen sensor setting low steady-state levels of HIF-1alpha in normoxia. EMBO J. 2003;22:4082–4090. 91. Sullivan LB, Martinez-Garcia E, Nguyen H, Mullen AR, Dufour E, Sudarshan S, et al. The proto-oncometabolite fumarate binds glutathione to amplify ROS-dependent signaling. Mol Cell. 2013;51:236–248. Key Words: cardioprotection ◼ citric acid cycle ◼ fumaric acid ◼ oxidationreduction ◼ nuclear factor (erythroid-derived 2)-like 2 ◼ reperfusion injury Citric Acid Cycle Intermediates in Cardioprotection Gabor Czibik, Violetta Steeples, Arash Yavari and Houman Ashrafian Downloaded from http://circgenetics.ahajournals.org/ by guest on May 6, 2017 Circ Cardiovasc Genet. 2014;7:711-719 doi: 10.1161/CIRCGENETICS.114.000220 Circulation: Cardiovascular Genetics is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2014 American Heart Association, Inc. All rights reserved. Print ISSN: 1942-325X. Online ISSN: 1942-3268 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circgenetics.ahajournals.org/content/7/5/711 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Genetics can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Genetics is online at: http://circgenetics.ahajournals.org//subscriptions/