Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Immunocontraception wikipedia , lookup
DNA vaccination wikipedia , lookup
Complement system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Innate immune system wikipedia , lookup
Autoimmunity wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Molecular mimicry wikipedia , lookup
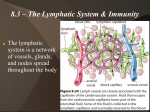
Autoimmune diseases Overview • Immune reactions against self antigens— autoimmunity—are an important cause of certain diseases in humans, estimated to affect at least 1% to 2% individuals • the mere presence of autoantibodies does not indicate an autoimmune disease exists Pathologic autoimmunity Three requirements (1) the presence of an immune reaction specific for some self antigen or self tissue; (2) evidence that such a reaction is not secondary to tissue damage but is of primary pathogenic significance; (3) the absence of another well-defined cause of the disease. Autoimmune diseases Clinical manifestations • Organ disease • • example: diabetes mellitus Generalised disease • example: lupus erythematous Tolerance • Immunologic tolerance is the phenomenon of unresponsiveness to an antigen induced by exposure of lymphocytes to that antigen. • Lymphocytes with receptors capable of recognizing self antigens are generated constantly, and these cells have to be eliminated or inactivated as soon as they recognize self antigens, to prevent them from causing harm Mechanisms of tolerance Central tolerance • immature self-reactive T and B lymphocyte clones that recognize self antigens during their maturation in the central (or generative) lymphoid organs (the thymus for T cells and the bone marrow for B cells) are killed or rendered harmless • Negative selection of self-reactive T cells in thymus: When immature lymphocytes encounter the antigens in the thymus, many of the cells die by apoptosis • • A wide variety of autologous protein antigens, including antigens thought to be restricted to peripheral tissues, are processed and presented by thymic antigenpresenting cells in association with self MHC molecules and can, therefore, be recognized by potentially self-reactive T cells Receptor editing of developing B in bone marrow: B cells that recognize self antigens in the bone marrow reactivate the machinery of antigen receptor gene rearrangement and begin to express new antigen receptors, not specific for self antigens. • If receptor editing does not occur, the self-reactive cells undergo apoptosis, thus purging potentially dangerous lymphocytes from the mature pool. Mechanisms of central tolerance: AIRE Mechanisms of peripheral tolerance • Anergy. • activation of antigen-specific T cells requires two signals: recognition of peptide antigen in association with self MHC molecules on the surface of APCs and a set of costimulatory signals (“second signals”) from APCs such as CD28 on T cells that bind to their ligands (the costimulators B7-1 and B7-2) on APCs. • If the antigen is presented to T cells without adequate levels of costimulators, the cells become anergic. Because costimulatory molecules are not expressed or are weakly expressed on resting dendritic cells in normal tissues, the encounter between autoreactive T cells and their specific self antigens displayed by these dendritic cells may lead to anergy. • Several mechanisms of T-cell anergy have been demonstrated in various experimental systems. One of these, which has clinical implications, is that T cells that recognize self antigens receive an inhibitory signal from receptors that are structurally homologous to CD28 but serve the opposite functions. Two of these inhibitory receptors are CTLA-4, which (like CD28) binds to B7 molecules, and PD-1, which binds to two ligands that are expressed on a wide variety of cells. • • mice in which the gene encoding CTLA-4 or PD-1 is knocked out develop autoimmune diseases. Furthermore, polymorphisms in the CTLA4 gene are associated with some autoimmune endocrine diseases in humans. Anergy also affects mature B cells in peripheral tissues. It is believed that if B cells encounter self antigen in peripheral tissues, especially in the absence of specific helper T cells, the B cells become unable to respond to subsequent antigenic stimulation and may be excluded from lymphoid follicles, resulting in their death. Mechanisms of peripheral tolerance • Suppression by regulatory T cells • A population of T cells called regulatory T cells functions to prevent immune reactions against self antigens. • Regulatory T cells develop mainly in the thymus, as a result of recognition of self antigens • The best-defined regulatory T cells are CD4+ cells that express high levels of CD25, the α chain of the IL-2 receptor, and a transcription factor of the forkhead family, called FOXP3. • Both IL-2 and FOXP3 are required for the development and maintenance of functional CD4+ regulatory T cells. Mutations in FOXP3 result in severe autoimmunity in humans and mice; in humans these mutations are the cause of a systemic autoimmune disease called IPEX (an acronym for immune dysregulation, polyendocrinopathy, enteropathy, X-linked). In mice knockout of the gene encoding IL-2 or the IL-2 receptor α or β chain also results in severe multi-organ autoimmunity, because IL-2 is essential for the maintenance of regulatory T cells. • The mechanisms by which regulatory T cells suppress immune responses are not fully defined, but their inhibitory activity may be mediated in part by the secretion of immunosuppressive cytokines such as IL-10 and TGF-β, which inhibit lymphocyte activation and effector functions. • Regulatory T cells also express CTLA-4, which may bind to B7 molecules on APCs and reduce their ability to activate T cells via CD28. Mechanisms of peripheral tolerance • Deletion by apoptosis. • if T cells recognize self antigens, they may express a pro-apoptotic member of the Bcl family, called Bim, without antiapoptotic members of the family like Bcl-2 and Bcl-x (whose induction requires the full set of signals for lymphocyte activation). • A second mechanism of activation-induced death of CD4+ T cells and B cells involves the Fas-Fas ligand system. if self antigens engage antigen receptors of self-reactive T cells, Fas and FasL are co-expressed, leading to elimination of the cells via Fas-mediated apoptosis. Self-reactive B cells may also be deleted by FasL on T cells engaging Fas on the B cells. • The importance of this mechanism in the peripheral deletion of autoreactive lymphocytes is highlighted by two mice that are natural mutants of Fas or FasL. These mice develop an autoimmune disease somewhat resembling human SLE, associated with generalized lymphoproliferation. In humans a similar disease is caused by mutations in the FAS gene; it is called the autoimmune lymphoproliferative syndrome (ALPS). Immune-privileged sites • Some antigens are hidden (sequestered) from the immune system, because the tissues in which these antigens are located (eye, testis, brain) do not communicate with the blood and lymph. • As a result, self antigens in these tissues fail to elicit immune responses and are essentially ignored by the immune system. • If the antigens of these tissues are released, for example, as a consequence of trauma or infection, the result may be an immune response that leads to prolonged tissue inflammation and injury. This is the postulated mechanism for post-traumatic orchitis and uveitis. Mechanisms of autoimmunity • Autoimmunity arises from a combination of • the inheritance of susceptibility genes • environmental triggers, such as infections and tissue damage Mechanisms of autoimmunity Defective tolerance or regulation. • Despite the advances in understanding mechanisms of immune tolerance and regulation, it is not known why these may become defective in the majority of common autoimmune diseases. Abnormal display of self antigens. • Abnormalities may include increased expression and persistence of self antigens that are normally cleared, or structural changes in these antigens resulting from enzymatic modifications or from cellular stress or injury Inflammation or an initial innate immune response. • Microbes or cell injury may elicit local inflammatory reactions resembling innate immune responses, and these may be critical inducers of the autoimmune disease. Susceptibility genes • Autoimmunity has a genetic component. • • The incidence of many autoimmune diseases is greater in twins of affected individuals than in the general population, and greater in monozygotic than in dizygotic twins, proof that genetics contributes to the development of these disorders. Greatest contribution: HLA genes • Example: HLA-B27 and ankylosing spondylitis and HLA-B27; individuals who inherit this class I HLA allele have a 100-200 fold greater chance (odds ratio, or relative risk) of developing the disease compared with those who do not carry HLA-B27 • • Note that the majority of individuals with this allele will not develop the disease anyway Not clear why: not necessarily due to a better ability of some HLA molecules to display self-antigens Non-HLA genes and autoimmune diseases Example: PTPN22. Gene polymorphisms associated with autoimmune diseases reduces the enzymatic activity of the protein (a phosphatase the limits lymphocyte activation, thus leading to enhanced activation of lymphocytes in several diseases) Role of infections Role of infections • infections may upregulate the expression of costimulators on APCs. If these cells are presenting self antigens, the result may be a breakdown of anergy and activation of T cells specific for the self antigens. • some microbes may express antigens that have the same amino acid sequences as self antigens. Immune responses against the microbial antigens may result in the activation of self-reactive lymphocytes. This phenomenon is called molecular mimicry. • • A clear example of such mimicry is rheumatic heart disease, in which antibodies against streptococcal proteins cross-react with myocardial proteins and cause myocarditis. Some viruses, such as Epstein-Barr virus (EBV) and HIV, cause polyclonal B-cell activation, which may result in production of autoantibodies. General features of autoimmune diseases • Autoimmune diseases tend to be chronic, sometimes with relapses and remissions, and the damage is often progressive. • • When the response is inappropriately directed against self tissues, physiological amplification mechanisms exacerbate and prolong the injury. Another reason for the persistence and progression of autoimmune disease is the phenomenon of epitope spreading, in which an immune response against one self antigen causes tissue damage, releasing other antigens, and resulting in the activation of lymphocytes by these newly encountered epitopes The clinical and pathologic manifestations of an autoimmune disease are determined by the nature of the underlying immune response. Some of these diseases are caused by autoantibodies, whose formation may be associated with dysregulated germinal center reactions. Most chronic inflammatory diseases are caused by abnormal and excessive TH1 and TH17 responses; examples of these diseases include psoriasis, multiple sclerosis, and some types of inflammatory bowel disease. CD8+ CTLs contribute to killing of cells, such as islet β cells in type 1 diabetes. In some autoimmune diseases, such as rheumatoid arthritis, both antibodies and T cell–mediated inflammation may be involved. SLE (systemic lupus erythematosus) • SLE is an autoimmune disease involving multiple organs, characterized by a vast array of autoantibodies, particularly antinuclear antibodies (ANAs) • injury is caused mainly by deposition of immune complexes and binding of antibodies to various cells and tissues. • The disease may be acute or insidious in its onset, and is typically a chronic, remitting and relapsing, often febrile, illness. Injury to the skin, joints, kidney, and serosal membranes is prominent. Virtually every other organ in the body, however, may also be affected. • SLE is a fairly common disease, with a prevalence that may be as high as 1 in 2500 in certain populations. • SLE predominantly affects women, with a frequency of 1 in 700 among women of childbearing age and a female-to-male ratio of 9 : 1 during the reproductive age group of 17 through 55 years Autoantibodies in SLE • • Antinuclear antibodies (ANAs). The most widely used method for detecting ANAs is indirect immunofluorescence, which can identify antibodies that bind to a variety of nuclear antigens, including DNA, RNA, and proteins (collectively called generic ANAs). The pattern of nuclear fluorescence suggests the type of antibody present in the patient’s serum. Many basic patterns are recognized: • diffuse nuclear staining usually reflects antibodies to chromatin, histones, and, occasionally, double-stranded DNA. • Rim or peripheral staining patterns are most often indicative of antibodies to double-stranded DNA and sometimes to nuclear envelope proteins. • Speckled pattern refers to the presence of uniform or variable-sized speckles. This is one of the most commonly observed patterns of fluorescence and therefore the least specific. It reflects the presence of antibodies to nonDNA nuclear constituents such as Sm antigen, ribonucleoprotein, and SS-A and SS-B reactive antigens. • Nucleolar pattern refers to the presence of a few discrete spots of fluorescence within the nucleus and represents antibodies to RNA. This pattern is reported most often in patients with systemic sclerosis. • Centromeric pattern. Patients with systemic sclerosis often contain antibodies specific for centromeres, which give rise to this pattern. • Though the pattern and sensitivity of the ANAs is controversial, the test remains in use. Other autoantibodies: • Directed against blood cells, such as red cells, platelets, and lymphocytes; • Antiphospholipid antibodies are present in 30% to 40% of lupus patients. They are actually directed against epitopes of plasma proteins that are revealed when the proteins are in complex with phospholipids. Some of these antibodies interfere with in vitro clotting tests, such as partial thromboplastin time. Therefore, these antibodies are sometimes referred to as lupus anticoagulant. Despite the observed clotting delays in vitro, however, patients with antiphospholipid antibodies have complications related to excessive clotting (a hypercoagulable state), such as thrombosis. Patterns of ANAs A. B. C. D. Diffuse Rim Speckled Centromeric Pathogenesis of SLE The fundamental defect in SLE is a failure of the mechanisms that maintain self-tolerance. Genetic factors • Family members of patients have an increased risk of developing SLE. As many as 20% of clinically unaffected first-degree relatives of SLE patients reveal autoantibodies and other immunoregulatory abnormalities. • There is a higher rate of concordance (>20%) in monozygotic twins when compared with dizygotic twins (1% to 3%). • Studies of HLA associations support the concept that MHC genes regulate production of particular autoantibodies. Specific alleles of the HLA-DQ locus have been linked to the production of anti–nuclear, and antiphospholipid antibodies, although the relative risk is small. • Some lupus patients have inherited deficiencies of early complement components, such as C2, C4, or C1q. Lack of complement may impair removal of circulating immune complexes by the mononuclear phagocyte system, thus favoring tissue deposition. Knockout mice lacking C4 or certain complement receptors are also prone to develop lupus-like autoimmunity. Various mechanisms have been invoked, including failure to clear immune complexes and loss of B-cell self-tolerance. It has also been proposed that deficiency of C1q results in defective phagocytic clearance of apoptotic cells. Many cells normally undergo apoptosis, and if they are not cleared their nuclear components may elicit immune responses. • Genome-wide association studies have identified several genetic loci that may be associated with the disease. Many of these loci encode proteins involved in lymphocyte signaling and interferon responses, both of which may play a role in lupus pathogenesis, as discussed later. The relative risk for each locus is small, and even taken together these loci account for 20% or less of the genetic predisposition, suggesting an important role for environmental factors, discussed later. Immunologic factors • Failure of self-tolerance in B cells results from defective elimination of self-reactive B cells in the bone marrow or defects in peripheral tolerance mechanisms. • CD4+ helper T cells specific for nucleosomal antigens also escape tolerance and contribute to the production of high-affinity pathogenic autoantibodies. The autoantibodies in SLE show characteristics of T cell-dependent antibodies produced in germinal centers, and increased numbers of follicular helper T cells have been detected in the blood of SLE patients. • TLR (toll-like-receptor) engagement by nuclear DNA and RNA contained in immune complexes may activate B lymphocytes. These TLRs function normally to sense microbial products, including nucleic acids. Thus, B cells specific for nuclear antigens may get second signals from TLRs and may be activated, resulting in increased production of antinuclear autoantibodies. • Type I interferons play a role in lymphocyte activation in SLE. High levels of circulating type I interferons and a molecular signature in blood cells suggesting exposure to these cytokines has been reported in SLE patients and correlates with disease severity. Type I interferons are antiviral cytokines that are normally produced during innate immune responses to viruses. It may be that nucleic acids engage TLRs on dendritic cells and stimulate the production of interferons. In other words, self nucleic acids mimic their microbial counterparts. How interferons contribute to the development of SLE is unclear; these cytokines may activate dendritic cells and B cells and promote TH1 responses, all of which may stimulate the production of pathogenic autoantibodies. • Other cytokines that may play a role in unregulated B-cell activation include the TNF family member BAFF, which promotes survival of B cells. In some patients and animal models, increased production of BAFF has been reported, prompting attempts to block the cytokine or its receptor as therapy for SLE. Environmental factors • Exposure to ultraviolet (UV) light exacerbates the disease in many individuals. UV irradiation may induce apoptosis in cells and may alter the DNA in such a way that it becomes immunogenic, perhaps because of enhanced recognition by TLRs. In addition, UV light may modulate the immune response, for example, by stimulating keratinocytes to produce IL-1, a cytokine known to promote inflammation. • The gender bias of SLE is partly attributable to actions of sex hormones and partly related to genes on the X chromosome, independent of hormone effects. • Drugs such as hydralazine, procainamide, and Dpenicillamine can induce an SLE-like response in humans. A Model for the Pathogenesis of SLE. • Immunologic abnormalities in SLE—both documented and postulated—are varied and complex. • Potential model: • UV irradiation and other environmental insults lead to the apoptosis of cells. • Inadequate clearance of the nuclei of these cells results in a large burden of nuclear antigens. • Underlying abnormalities in B and T lymphocytes are responsible for defective tolerance, because of which self-reactive lymphocytes survive and remain functional. These lymphocytes are stimulated by nuclear self antigens, and antibodies are produced against the antigens. • Complexes of the antigens and antibodies bind to Fc receptors on B cells and dendritic cells, and may be internalized. • The nucleic acid components engage TLRs and stimulate B cells to produce more autoantibodies. TLR stimuli also activate dendritic cells to produce interferons and other cytokines, which further enhance the immune response and cause more apoptosis. • The net result is a cycle of antigen release and immune activation resulting in the production of highaffinity autoantibodies. Model for the pathogenesis of systemic lupus erythematosus. In this hypothetical model, susceptibility genes interfere with the maintenance of self-tolerance and external triggers lead to persistence of nuclear antigens. The result is an antibody response against self nuclear antigens, which is amplified by the action of nucleic acids on dendritic cells (DCs) and B cells, and the production of type 1 interferons. TLRs, Toll-like receptors. Mechanisms of tissue injury • Most of the systemic lesions are caused by immune complexes (type III hypersensitivity). DNA-anti-DNA complexes can be detected in the glomeruli and small blood vessels. Low levels of serum complement (secondary to consumption of complement proteins) and granular deposits of complement and immunoglobulins in the glomeruli further support the immune complex nature of the disease. T cell infiltrates are also frequently seen in the kidneys, but the role of these cells in tissue damage is not established. • Autoantibodies specific for red cells, white cells, and platelets opsonize these cells and promote their phagocytosis and lysis. There is no evidence that ANAs, which are involved in immune complex formation, can penetrate intact cells. If cell nuclei are exposed, however, the ANAs can bind to them. In tissues, nuclei of damaged cells react with ANAs, lose their chromatin pattern, and become homogeneous, to produce so-called LE bodies or hematoxylin bodies. Related to this phenomenon is the LE cell, which is readily seen when blood is agitated in vitro. The LE cell is any phagocytic leukocyte (blood neutrophil or macrophage) that has engulfed the denatured nucleus of an injured cell. The demonstration of LE cells in vitro was used in the past as a test for SLE. With new techniques for detection of ANAs, however, this test is now largely of historical interest. Sometimes, LE cells are found in pericardial or pleural effusions in patients. • Antiphospholipid antibody syndrome. Patients with antiphospholipid antibodies may develop venous and arterial thromboses, which may be associated with recurrent spontaneous miscarriages and focal cerebral or ocular ischemia. This constellation of clinical features, in association with lupus, is referred to as the secondary antiphospholipid antibody syndrome. The mechanisms of thrombosis are not defined, and antibodies against clotting factors, platelets and endothelial cells have all been proposed as being responsible for thrombosis. • The neuropsychiatric manifestations of SLE have been attributed to antibodies that react with neurons or receptors for various neurotransmitters and cross the blood brain barrier. However, this is not established and mechanisms involving other immune factors, such as cytokines, may also underlie the cognitive dysfunction and other CNS abnormalities that are associated with SLE. Type III Hypersensitivity • Antigen-antibody complexes produce tissue damage mainly by eliciting inflammation at the sites of deposition. The pathologic reaction is usually initiated when antigen combines with antibody in the circulation, creating immune complexes that typically deposit in vessel walls. Less frequently, the complexes may be formed at sites where antigen has been “planted” previously (called in situ immune complexes). • The antigens that form immune complexes may be exogenous, such as a foreign protein that is injected or produced by an infectious microbe, or endogenous, if the individual produces antibody against self antigens (autoimmunity). • Immune complex–mediated diseases tend be systemic, but often preferentially involve the kidney (glomerulonephritis), joints (arthritis), and small blood vessels (vasculitis), all of which are common sites of immune complex deposition. Phases of type III HS reactions • Formation of immune complexes. Autoantibodies form antigen-antibody complexes. • Deposition of immune complexes. In the next phase the circulating antigen-antibody complexes are deposited in various tissues. The factors that determine whether immune complex formation will lead to tissue deposition and disease are not fully understood, but the major influences seem to be the characteristics of the complexes and local vascular alterations. In general, complexes that are of medium size, formed in slight antigen excess, are the most pathogenic. Organs where blood is filtered at high pressure to form other fluids, like urine and synovial fluid, are sites where immune complexes become concentrated and tend to deposit; hence, immune complex disease often affects glomeruli and joints. • Inflammation and tissue injury. Once immune complexes are deposited in the tissues, they initiate an acute inflammatory reaction. During this phase (approximately 10 days after antigen administration), clinical features such as fever, urticaria, joint pains (arthralgias), lymph node enlargement, and proteinuria appear. Wherever complexes deposit the tissue damage is similar. The mechanisms of inflammation and injury were discussed above, in the discussion of antibody-mediated injury. The resultant inflammatory lesion is termed vasculitis if it occurs in blood vessels, glomerulonephritis if it occurs in renal glomeruli, arthritis if it occurs in the joints, and so on. Immune complex disease. The sequential phases in the induction of systemic immune complex–mediated diseases (type III hypersensitivity). Blood Vessels. An acute necrotizing vasculitis involving capillaries, small arteries and arterioles may be present in any tissue. The arteritis is characterized by fibrinoid deposits in the vessel walls. In chronic stages, vessels undergo fibrous thickening with luminal narrowing. Kidney. Up to 50% of SLE patients have clinically significant renal involvement. All of the glomerular lesions described later are the result of deposition of immune complexes that are regularly present in the mesangium or along the entire basement membrane and sometimes throughout the glomerulus. Both in situ formation and deposition of preformed circulating immune complexes may contribute to the injury, but the reason for the wide spectrum of histopathologic lesions (and clinical manifestations) in patients with lupus nephritis remains uncertain. The kidney virtually always shows some evidence of renal abnormality if examined by electron microscopy and immunofluorescence. According to the currently accepted classification, six patterns of glomerular disease are seen in SLE. It should be noted that there is some overlap within these classes and over time lesions may evolve from one class to another. Thus, the exact percentage of patients with each of the six classes of lesions is difficult to determine. Suffice it to say that Class I is the least common and class IV is the most common pattern. Minimal mesangial lupus nephritis (class I) is very uncommon, and is characterized by immune complex deposition in the mesangium, identified by immunoflourescence and by electron microscopy, but without structural changes by light microscopy. Mesangial proliferative lupus nephritis (class II) is characterized by mesangial cell proliferation, often accompanied by accumulation of mesangial matrix, and granular mesangial deposits of immunoglobulin and complement without involvement of glomerular capillaries. Focal lupus nephritis (class III) is defined by involvement of fewer than 50% of all glomeruli. The lesions may be segmental (affecting only a portion of the glomerulus) or global (involving the entire glomerulus). Affected glomeruli may exhibit swelling and proliferation of endothelial and mesangial cells associated with leukocyte accumulation, capillary necrosis, and hyaline thrombi. There is also often extracapillary proliferation associated with focal necrosis and crescent formation (Fig. 6-26A). The clinical presentation ranges from mild hematuria and proteinuria to acute renal insufficiency. Red cell casts in the urine are common when the disease is active. Some patients progress to diffuse glomerulonephritis. The active (or proliferative) inflammatory lesions can heal completely or lead to chronic global or segmental glomerular scarring. Diffuse lupus nephritis (class IV) is the most common and severe form of lupus nephritis. The lesions are similar to those in class III, but differ in extent; typically, in class IV nephritis half or more of the glomeruli are affected. As in class III, the lesions may be segmental or global and on the basis of this, it can be subclassified as Class IV segmental ( IV-S) or Class IV global (IV-G). Involved glomeruli show proliferation of endothelial, mesangial and epithelial cells (Fig. 6-26B), with the latter producing cellular crescents that fill Bowman’s space (Chapter 20). Subendothelial immune complex deposits may create a circumferential thickening of the capillary wall, forming “wire loop” structures on light microscopy (Fig. 6-26C). Immune complexes can be readily detected by electron microscopy (Fig. 6-26D) and immunofluorescence (Fig. 6-26E). Lesions may progress to scarring of glomeruli. Patients with diffuse glomerulonephritis are usually symptomatic, showing hematuria as well as proteinuria. Hypertension and mild to severe renal insufficiency are also common. Membranous lupus nephritis (class V) is characterized by diffuse thickening of the capillary walls due to deposition of subepithelial immune complexes, similar to idiopathic membranous nephropathy, described in Chapter 20. The immune complexes are usually accompanied by increased production of basement membrane-like material. This lesion is usually accompanied by severe proteinuria or nephrotic syndrome, and may occur concurrently with focal or diffuse lupus nephritis. Advanced sclerosing lupus nephritis (class VI) is characterized by sclerosis of more than 90% of the glomeruli, and represents end-stage renal disease. Changes in the interstitium and tubules are frequently present in lupus nephritis patients. Rarely, tubulointerstitial lesions may be the dominant abnormality. Discrete immune complexes similar to those in glomeruli are present in the tubular or peritubular capillary basement membranes in many lupus nephritis patients, but the clinical significance of these extraglomerular deposits is not established. Often, there are well-organized B-cell follicles in the interstitium, with plasma cells that may be sources of autoantibodies. Lupus nephritis. A, Focal proliferative glomerulonephritis, with two focal necrotizing lesions at the 11 O’clock and 2 O’clock positions (H&E stain). Extracapillary proliferation is not prominent in this case. B, Diffuse proliferative glomerulonephritis. Note the marked increase in cellularity throughout the glomerulus (H&E stain). C, Lupus nephritis showing a glomerulus with several “wire loop” lesions representing extensive subendothelial deposits of immune complexes (periodic acid-Schiff stain). D, Electron micrograph of a renal glomerular capillary loop from a patient with SLE nephritis. Subendothelial dense deposits (arrowheads) correspond to “wire loops” seen by light microscopy. B (with arrow) refers to the basement membrane. E, Deposition of IgG antibody in a granular pattern, detected by immunofluorescence. B, Basement membrane; End, endothelium; Ep, epithelial cell with foot processes; Mes, mesangium; RBC, red blood cell in capillary lumen; US, urinary space. Systemic lupus erythematosus involving the skin. A, An H&E-stained section shows liquefactive degeneration of the basal layer of the epidermis and edema at the dermoepidermal junction. B, An immunofluorescence micrograph stained for IgG reveals deposits of Ig along the dermoepidermal junction.