Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neocentromere wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Medical genetics wikipedia , lookup
Genetic engineering wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Y chromosome wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Copy-number variation wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Oncogenomics wikipedia , lookup
Frameshift mutation wikipedia , lookup
Genome evolution wikipedia , lookup
Gene expression profiling wikipedia , lookup
Helitron (biology) wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Gene desert wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
X-inactivation wikipedia , lookup
Gene nomenclature wikipedia , lookup
Gene therapy wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Genome (book) wikipedia , lookup
Gene expression programming wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Point mutation wikipedia , lookup
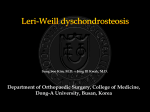
J C E M O N L I N E B r i e f R e p o r t — E n d o c r i n e R e s e a r c h The Jumping SHOX Gene—Crossover in the Pseudoautosomal Region Resulting in Unusual Inheritance of Leri-Weill Dyschondrosteosis Sarina G. Kant, Hetty J. van der Kamp, Marjolein Kriek, Egbert Bakker, Boudewijn Bakker, Mariette J. V. Hoffer, Patrick van Bunderen, Monique Losekoot, Saskia M. Maas, Jan M. Wit, Gudrun Rappold, and Martijn H. Breuning Center for Human and Clinical Genetics (CHCG)-Department of Clinical Genetics (S.G.K., M.K., M.H.B.), Department of Paediatrics (H.J.v.d.K., B.B., J.M.W.), and CHCG-Laboratory for Diagnostic Genome Analysis (E.B., M.J.v.H., P.v.B., M.L.), Leiden University Medical Center, 2300 RC Leiden, The Netherlands; Departments of Clinical Genetics (S.M.M.) and Paediatrics (S.M.M.), Academic Medical Centre, 1105 AZ Amsterdam, The Netherlands; and Department of Human Molecular Genetics (G.R.), University of Heidelberg, 69120 Heidelberg, Germany Context: During meiosis I, the recombination frequency in the pseudoautosomal region on Xp and Yp (PAR1) in males is very high. As a result, mutated genes located within the PAR1 region can be transferred from the Y-chromosome to the X-chromosome and vice versa. Patients: Here we describe three families with SHOX abnormalities resulting in Leri-Weill dyschondrosteosis or Langer mesomelic dysplasia. Results: In about half of the segregations investigated, a transfer of the SHOX abnormality to the alternate sex chromosome was demonstrated. Conclusions: Patients with an abnormality of the SHOX gene should receive genetic counseling as to the likelihood that they may transmit the mutation or deletion to a son as well as to a daughter. (J Clin Endocrinol Metab 96: E356 –E359, 2011) he classic clinical triad in Leri-Weill dyschondrosteosis (LWD) is short stature, mesomelia, and Madelung deformity. In mesomelia, the middle portion of a limb is shortened in relation to the proximal portion, whereas Madelung deformity includes abnormal alignment of the radius, ulna, and carpal bones at the wrist (1, 2). Penetrance of the phenotype appears to be incomplete within families. Besides, both bilateral Madelung deformity and short stature tend to be more common and severe in females than males (3). LWD is caused in a large proportion of patients by mutations or deletions in the short stature homeobox (SHOX) gene or by deletions downstream of the SHOX gene (4). The SHOX gene is located in the pseudoautosomal 1 region (PAR1) of the X- and Y-chromosomes. The SHOX gene escapes X-chromosome inactivation. Two functional T ISSN Print 0021-972X ISSN Online 1945-7197 Printed in U.S.A. Copyright © 2011 by The Endocrine Society doi: 10.1210/jc.2010-1505 Received July 1, 2010. Accepted October 7, 2010. First Published Online November 10, 2010 E356 jcem.endojournals.org SHOX genes are needed for normal growth. When both SHOX genes are mutated, this results in Langer mesomelic dysplasia, a more severe form of skeletal dysplasia. Due to crossover during meiosis I in males, transfer of the deleted SHOX gene to the alternate sex chromosome may be observed in some pedigrees. Here we present three families in which this transfer event occurs in almost 50% of the segregations investigated. Patients and Methods Family 1 The index case (III:2) was born at term with a normal birth weight and length. At the age of 8.9 yr, her height (H) was 121.1 cm [⫺2.6 SD score (sds)] with a sitting height (SH)/H ratio of 1.4 Abbreviations: FISH, Fluorescence in situ hybridization; H, height; LWD, Leri-Weill dyschondrosteosis; MLPA, multiplex ligation probe amplification; PAR1, pseudoautosomal 1 region; sds, SD score; SH, sitting height; SHOX, short stature homeobox gene. J Clin Endocrinol Metab, February 2011, 96(2):E356 –E359 J Clin Endocrinol Metab, February 2011, 96(2):E356 –E359 jcem.endojournals.org E357 The fathers came from a family of four. In one other brother (II:4), their sister (II:3), and the (grand-) parents (I:1 and I:2), karyotyping and fluorescence in situ hybridization (FISH) analysis were performed, but clinical measurements were not. Family 3 The index case (II:2) was seen at the age of 40 yr. She was born after an uneventful pregnancy of 40 wk with a birth weight of 4 kg. Her arms and legs were relatively short at birth. Until the age of 35 yr, she was healthy, but since 5 yr ago she had joint pain, especially of her fingers, for which she presented at the hospital. At physical examination, she was 130 cm tall, and she had rhizomelic shortening of the arms and legs. X-rays showed Madelung deformity and shortening of the ulnae. According to the index case, her brother (II:1) has exactly the same H and stature as the proband. He is mentally retarded, and it was not possible to examine him. The mother (I:2) has a H of 160 cm with relatively short arms and legs. Three of the eight sibs of the mother are disproportionately short. The father (I:1) had a normal stature, and his H was 165 cm. He died from leukemia. Cytogenetic and molecular analysis FIG. 1. Clinical photograph and x-rays of the left hand and wrist of patient III:2 of family 1. Note the Madelung deformity. sds (5, 6). Her arm span was ⫺2.2 sds (7). She had a Madelung deformity of both wrists (Fig. 1). Bone age according to Greulich and Pyle (8) was 6.9 yr. Her cousin (III:5) was also known with short stature. At the age of 9.7 yr, her H was 126.8 cm (⫺2.4 sds), and her SH/H ratio was 2.2 sds. Her arm span was ⫺2.0 sds. Her bone age according to Greulich and Pyle (8) was 7.9 yr. She had a mild Madelung deformity. The father of the index case (II:2) had a H of 169.6 cm (⫺2.0 sds) and a SH/H ratio of 1.5 sds. His arm span was ⫺2.0 sds. He had no Madelung deformity. The father of the cousin (II:3) had a H of 179.5 cm (⫺0.6 sds) and a SH/H ratio of 1.5 sds. His arm span was ⫺2.7 sds. He had mild Madelung deformity. A third brother (II:1) did not have short stature or disproportion. The paternal grandfather (I:1) had a H of 165.5 cm (⫺2.6 sds) and a SH/H ratio of 1.8 sds. X-rays of his wrists did not show any abnormality. Treatment with GH and decapeptyl in both cousins was started and resulted in a H gain with an increase of the H sds, whereas their bone age increased only slightly. Family 2 The index case (III:5) in the second family was seen at the age of 11.7 yr. Her H was 134.7 cm (⫺2.7 sds), with a SH/H ratio of 2.5 sds and an arm span of 1.0 sds. An x-ray of the wrist showed no abnormalities. Bone age according to Greulich and Pyle (8) was 11.8 yr. Her father (II:2) had a H of 176 cm (⫺1.1 sds), but had experienced disproportionately short legs. He had a SH/H ratio well above 2.5 sds. His arm span was ⫺1.0 sds. A cousin of the index case (III:2) was also known with short stature, and at the age of 12.8 yr she had a H of 144 cm (⫺2.3 sds), a SH/H ratio of 1.4 sds, and an arm span of ⫺1.0 sds. No abnormalities of the wrist were noted. Bone age was normal. Her father (II:1) had disproportionate short stature with a H of 165.7 cm (⫺2.6 sds) and a SH/H ratio of 2.7 sds. Karyotyping was performed in families 1 and 2 using standard procedures. FISH analysis of the PAR1 region was also performed using standard procedures. In family 1, the FISH probe 29B11 was used, which is located 3⬘ of the SHOX gene. In family 2, the FISH probes 34F5 (SHOX specific) and RP11– 839D20 (subtelomere specific) were used. For family 1 and family 3, sequencing and multiplex ligation probe amplification (MLPA) of the SHOX gene and MLPA of the enhancer region were used to detect mutations or copy number variants using standard procedures. Results Family 1 Karyotyping showed a normal result in the index patient (III:2) and her cousin (III:5). Sequence analysis and MLPA of the SHOX gene revealed no abnormalities in both affected girls. However, FISH analysis showed a deletion in PAR1 downstream of the SHOX gene in the girls, in their fathers (II:2 and II:3), and in the paternal grandfather (I:1). Results of this analysis were described earlier (9). The deletion in this family was confirmed using MLPA techniques. The deletion in both fathers (II:2 and II:3) and the grandfather (I:1) was situated on the Y-chromosome (Fig. 2). The deletion was not observed in the two sisters of the index case (III:3 and III:4), the two brothers of her cousin (III:6 and III:7), and her uncle (II:1). Family 2 Karyotyping in the index patient (III:5) showed a normal female karyotype. FISH analysis demonstrated a terminal deletion of the tip of Xp, including the SHOX gene region, with its breakpoint in Xp22.3 [ish del(X)(p22.3) (34F5-, 839D20-)]. This deletion was located on the X- E358 Kant et al. The Jumping SHOX Gene FIG. 2. Pedigrees of families 1, 2 and 3. Crossing over of the PAR1 abnormality has occurred in family 1 in patients II:1, III:2, III:5, III:6, and III:7; in family 2 in patients II:3, II:4, III:1, III:2, and III:5; and in family 3 in either II:1 or II:2. Light gray symbols, Persons with SHOX haploinsufficiency; dark gray symbols, persons with compound heterozygous mutation of SHOX. Y, SHOX-mutation/deletion on Y chromosome; X, SHOX-mutation/deletion on X chromosome; (?), SHOX-deletion on either X or Y chromosome, derived from the results of both children; n, no deletion. The index persons are indicated by an arrow. chromosome (Fig. 2) in the index case, her aunt (II:3), one of the sons of this aunt (III:9), and the daughter of the father’s brother (III:2). It was demonstrated on the Y-chromosome in the father of the index case (II:2), one of his brothers (II:1), and the grandfather (I:1). The deletion was not observed in the three sisters of the index case (III:3, 4, 6), three of her cousins (III:1, 7, 8), and one of the brothers of her father (II:4). Family 3 In the index case (II:2), MLPA analysis showed a deletion of the promoter region until exon 8 of the SHOX gene, and mutation analysis showed a mutation in exon 4 of the SHOX gene (c.517C⬎T p.Arg173Cys), in accordance with the clinical diagnosis of Langer mesomelic dysplasia. Her brother (II:1) was shown to have the same deletion and mutation. The mother (I:2) appeared to have the deletion of the SHOX gene. DNA of the father (I:1) could not be analyzed. Discussion LWD caused by mutations or deletions of the SHOX gene is known to be clinically highly variable. Family 1 shows that this is also true for LWD caused by a deletion downstream the SHOX gene in PAR1. The index patient and her cousin J Clin Endocrinol Metab, February 2011, 96(2):E356 –E359 have clear disproportionate short stature, whereas their fathers have normal H, with only slight disproportion. PAR1 is located at the terminal end of Xp and Yp. All genes within PAR1 escape X inactivation in women. However, the only gene in this region associated with human disease is the SHOX gene (10). Inheritance of LWD is pseudoautosomal. The SHOX gene in the normal situation is present in two functional copies. In fact, one might consider PAR1 as a very small extra pair of autosomes (11), except that segregation in autosomes is independent of sex. Here we describe three families in which an abnormality in PAR1 segregates from one sex chromosome to the other in the next generation. PAR1 is highly homologous and is therefore necessary for X-Y chromosome-pairing during male meiosis (11). As with autosomes, it undergoes one obligatory crossover event during this process, which always occurs within the PAR1 region. In males, the recombination frequency in PAR1 is extraordinarily high, about 20 times higher than the genome average (12, 13). It decreases rapidly at the proximal boundary of the 2.6 Mb pseudoautosomal segment in conjunction with a decrease in homology (10, 11). One explanation for the high recombination rate is found in the fact that telomeric regions usually are more recombinogenic than the rest of a chromosome (14, 15), but in the sex chromosomes a special situation exists because recombination in male meiosis is limited to the pseudoautosomal regions. This leads to a recombination frequency across the pseudoautosomal regions being about 10 times higher in male than in female meiosis (12, 14). The phenomenon of transfer of a mutated or deleted SHOX gene from one sex chromosome to the other occasionally led to minimal comment in some reports (16, 17) but has never been described in a high percentage within the same family as in the families that we report here. A recombination event resulting in transfer of a PAR1 abnormality between X- and Y-chromosomes occurred in 11 of the 24 segregations investigated. This high percentage could be due to the fact that males with LWD are overrepresented in the families. The possibility of a crossing over seems not to be dependent on the kind of abnormality in PAR1. Flanagan et al. (16) described one family with at least a deletion of the whole SHOX gene and one family with a splice-site mutation in the SHOX gene, whereas Sabherwal et al. (17) reported on a family with a missense mutation. The families we describe have a deletion downstream the SHOX gene, a deletion of the terminal part of PAR1 including SHOX, a deletion of the whole SHOX gene, and a mutation in the SHOX gene. The fact that SHOX can “jump” from one sex chromosome to the other has consequences for genetic coun- J Clin Endocrinol Metab, February 2011, 96(2):E356 –E359 seling. When giving genetic advice to male patients with LWD, transfer of the mutation or deletion in PAR1 to the other sex chromosome should be discussed. The possibility of such a transfer is also present in female patients, but chances are smaller than in males, and it does not influence their risk of having an affected son or daughter. Acknowledgments Address all correspondence and requests for reprints to: Sarina G. Kant, Center for Human and Clinical Genetics-Department of Clinical Genetics, Leiden University Medical Center, P.O. Box 9600, 2300 RC Leiden, The Netherlands. E-mail: [email protected]. Disclosure Summary: The authors have nothing to disclose. References 1. Ross JL, Scott Jr C, Marttila P, Kowal K, Nass A, Papenhausen P, Abboudi J, Osterman L, Kushner H, Carter P, Ezaki M, Elder F, Wei F, Chen H, Zinn AR 2001 Phenotypes associated with SHOX deficiency. J Clin Endocrinol Metab 86:5674 –5680 2. Rappold G, Blum WF, Shavrikova EP, Crowe BJ, Roeth R, Quigley CA, Ross JL, Niesler B 2007 Genotypes and phenotypes in children with short stature: clinical indicators of SHOX haploinsufficiency. J Med Genet 44:306 –313 3. Binder G, Renz A, Martinez A, Keselman A, Hesse V, Riedl SW, Häusler G, Fricke-Otto S, Frisch H, Heinrich JJ, Ranke MB 2004 SHOX haploinsufficiency and Leri-Weill dyschondrosteosis: prevalence and growth failure in relation to mutation, sex, and degree of wrist deformity. J Clin Endocrinol Metab 89:4403– 4408 4. Benito-Sanz S, Thomas NS, Huber C, Gorbenko del Blanco D, AzaCarmona M, Crolla JA, Maloney V, Rappold G, Argente J, CamposBarros A, Cormier-Daire V, Heath KE 2005 A novel class of pseudoautosomal region 1 deletions downstream of SHOX is associated with Leri-Weill dyschondrosteosis. Am J Hum Genet 77:533–544 5. Fredriks AM, van Buuren S, Burgmeijer RJ, Meulmeester JF, Beuker RJ, Brugman E, Roede MJ, Verloove-Vanhorick SP, Wit JM 2000 Continuing positive secular growth change in The Netherlands 1955–1997. Pediatr Res 47:316 –323 jcem.endojournals.org E359 6. Fredriks AM, van Buuren S, van Heel WJ, Dijkman-Neerincx RH, Verloove-Vanhorick SP, Wit JM 2005 Nationwide age references for sitting height, leg length, and sitting height/height ratio, and their diagnostic value for disproportionate growth disorders. Arch Dis Child 90:807– 812 7. Gerver WJ, de Bruin R 1996 Paediatric morphometrics—a reference manual. 1st ed. Utrecht, The Netherlands: Bunge; 140 –143 8. Greulich WW, Pyle SI 1959 Radiographic atlas of skeletal development of the hand and wrist. 2nd ed. Stanford, CA: Stanford University Press 9. Sabherwal N, Bangs F, Röth R, Weiss B, Jantz K, Tiecke E, Hinkel GK, Spaich C, Hauffa BP, van der Kamp H, Kapeller J, Tickle C, Rappold G 2007 Long-range conserved non-coding SHOX sequences regulate expression in developing chicken limb and are associated with short stature phenotypes in human patients. Hum Mol Genet 16:210 –222 10. Blaschke RJ, Rappold G 2006 The pseudoautosomal regions, SHOX and disease. Curr Opin Genet Dev 16:233–239 11. Burgoyne PS 1986 Mammalian X and Y crossover. Nature 319: 258 –259 12. Schmitt K, Lazzeroni LC, Foote S, Vollrath D, Fisher EM, Goradia TM, Lange K, Page DC, Arnheim N 1994 Multipoint linkage map of the human pseudoautosomal region, based on single-sperm typing: do double crossovers occur during male meiosis? Am J Hum Genet 55:423– 430 13. May CA, Shone AC, Kalaydjieva L, Sajantila A, Jeffreys AJ 2002 Crossover clustering and rapid decay of linkage disequilibrium in the Xp/Yp pseudoautosomal gene SHOX. Nat Genet 31:272–275 14. Rappold GA, Klink A, Weiss B, Fischer C 1994 Double crossover in the human Xp/Yp pseudoautosomal region and its bearing on interference. Hum Mol Genet 3:1337–1340 15. Lien S, Szyda J, Schechinger B, Rappold G, Arnheim N 2000 Evidence for heterogeneity in recombination in the human pseudoautosomal region: high resolution analysis by sperm typing and radiation-hybrid mapping. Am J Hum Genet 66:557–566 16. Flanagan SF, Munns CF, Hayes M, Williams B, Berry M, Vickers D, Rao E, Rappold GA, Batch JA, Hyland VJ, Glass IA 2002 Prevalence of mutations in the short stature homeobox containing gene (SHOX) in Madelung deformity of childhood. J Med Genet 39: 758 –763 17. Sabherwal N, Blaschke RJ, Marchini A, Heine-Suner D, Rosell J, Ferragut J, Blum WF, Rappold G 2004 A novel point mutation A170P in the SHOX gene defines impaired nuclear translocation as a molecular cause for Léri-Weill dyschondrosteosis and Langer dysplasia. J Med Genet 41:e83