Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Gene therapy wikipedia , lookup
Genomic imprinting wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
X-inactivation wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Gene expression profiling wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Genome evolution wikipedia , lookup
Population genetics wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Genetic engineering wikipedia , lookup
Gene expression programming wikipedia , lookup
Public health genomics wikipedia , lookup
Oncogenomics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
History of genetic engineering wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Genome (book) wikipedia , lookup
Frameshift mutation wikipedia , lookup
Designer baby wikipedia , lookup
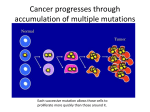
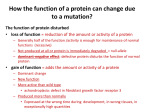
BME INFORMATION DAY,SCOTLAND NDCS AND SMDCS Presentations by: •Dr Mary Shanks (ENT Consultant, Crosshouse) •Dr Juan Mora (Consultant Audio Vestibular Surgeon) ADVANCES IN COCHLEAR IMPLANTATION Mary Shanks Surgical Director Scottish Cochlear Implant Programme NDCS 16th March 2013 Scottish Cochlear Implant Programme 25 years old! 700 adults and 300 children implanted 210 bilateral cochlear implant users 100 cochlear implant operations per year (40 children) What is a Cochlear Implant? An electronic device for severe-to-profoundly deaf people who are unable to benefit from powerful hearing aids The primary aim of cochlear implantation is to promote spoken language Normal Hearing Organ of Corti (Hearing) ‘Critical’ Period for spoken language development Neuroplasticity 0-4 years old After 4 years old auditory areas in brain re- allocated to vision and other functions How a Cochlear Implant Works Electrode Array in Cochlea Surgery Early implantation Electrode Design Bilateral Implantation Advances in Surgery Early Cochlear Implantation possible due to Newborn Hearing Screening Early hearing aid fitting Assessment at 10 months Aim to implant 10-18 months Electrode Design Slimmer more flexible electrodes = less damage to cochlea In future - electrodes which deliver steroids and neurotrophic factors directly to the cochlea Minimising Cochlear Trauma Medel Flex electrodes with choice of lengths 20 – 31 mm Bilateral Implantation Advances in Surgery Bilateral Cochlear Implantation Since 2009 80% parents choose bilateral implantation for their child Better hearing in noise Better sound localisation Back-up device (device failure rate 1-2%) Then…Body worn processors Now… Waterproof Implants Advanced Bionics Neptune Programming Remote Programming via Internet What is a successful outcome? Children using spoken language(s) as their main mode of communication Starting a mainstream school aged 5 with children who have normal hearing Happy children who are able to participate fully in family life and socialise with their friends Children with special needs/disabilities may have different but equally important outcomes for them Successful outcomes depend upon…… Child + Parental support = 90% Surgery + technology + programming = 10% How to help your child develop speech Ensure they wear their Cochlear Implant(s) all day, every day Talk to your child and help them to learn about everyday sounds Follow advice from our rehabilitation specialists and your local team (speech therapists & teachers of deaf) ROLE OF GENETIC COUNSELLING FOR HEARING IMPAIRED CHILDREN FROM MINORITY ETHNIC COMMUNITIES Juan Mora Audiological Physician BME Information Day 16th March 2013 What is genetic counselling? Genetic counselling provides information that helps to understand the possibility of developing a genetic (inherited) health condition. Providing information to allow people to make informed decisions Genetic information The organs and tissues of the body are made of cells. The cells contain genetic information which determines how we are, either alone or by interacting with the environment. The information is stored in a long molecule called Deoxyribonucleic acid (DNA) in an alphabet of four letters A, C, G and T. DNA is found in chromosomes. Each cell in the body contains 23 pairs of chromosomes. What are genes? Genes are sections of the DNA. Each cell contains around 21,000 genes. Each gene contains the instructions to make a particular protein, in a particular cell, at a particular time. Proteins are complex chemicals that make up blood, muscles and all the tissues and organs of the body. How are genes inherited? One of each of the 23 pairs of chromosomes is inherited from each parent. Therefore there are 2 copies of each gene on each cell, with the exception of the sex chromosomes (X and Y). Mutations Mutations are changes in the sequence of DNA in the cells. DNA is constantly being damaged by processes like radiation, sunlight and chemicals. The damage is usually repaired but sometimes the repair is not perfect and this leads to a mutation. Some mutations are neutral and have no effect, others may improve a protein and be beneficial and some result in a protein that does not work, which may cause disease. Mutations Mutations can be inherited from a parent or they can occur when a sperm or egg is made, resulting in a new mutation. Mutations can occur in a dominant gene (only one mutation is enough to cause a medical condition) or in a recessive gene (the mutation has to be present in the two copies of the gene to cause the condition). Patterns of inheritance Recessive inheritance In recessive inheritance, a child inherits a mutation from each parent in both copies of a particular gene and develops a health condition. If the child inherits only one copy of the gene with the mutation, he/she will be a carrier of the condition but will not develop it. When 2 parents are carriers of the same mutation, their children have a 25% possibility of inheriting the mutations from both parents. Patterns of inheritance Dominant inheritance • In dominant inheritance, only one mutation needs to be passed on from either the mother or the father for the child to develop the condition. So, if one of the parents has the condition, there is a one in two chance it will be passed on to the child. Patterns of inheritance X-linked inheritance • Mutations in the X chromosome tend to cause medical conditions only in males. This is because females have two X chromosomes, one of which is almost certainly normal. However males only have one X chromosome, and if there is one mutation there is no other healthy copy of the gene like in females. Consanguinity Unions contracted between persons biologically related up to as second cousins are categorized as consanguineous. The more common form of consanguineous union is between first cousins, in which the spouses share 1/8 of their genes inherited from a common ancestor. That is, their children are predicted to have inherited identical gene copies from each parent at 6.25% over the general population (1) Consanguinity The detrimental health effects associated with consanguinity are caused by the expression of rare, recessive genes inherited from a common ancestor(s). Every person is estimated to have around 100 mutations (4). Children of consanguineous marriages are more likely to inherit the same mutation in both copies of the same gene than in the general population. Consanguinity: morbidity and mortality Empirical studies on the children of first cousins indicate morbidity levels to be some 1% to 4% higher than in the offspring of unrelated couples (2) Children of first cousin parents have higher ratios for neonatal, postnatal, and infant mortality (3) Conclusions Genetic counselling is about providing information on the genetics of medical conditions to help people to make informed decisions. Children of consanguineous parents have a higher possibility of inheriting identical copies of a proportion of genes from their parents. This sometimes may lead to developing health conditions. Conclusions However doctor’s views can be biased because of the nature of their work: Only a minority of parents with close kin marriage have children with health conditions attributable to the consanguinity. The majority of consanguineous couples have healthy children, but doctors do not see them (1). References 1. http://www.consang.net/index.php/Summary 2. Bittles, A.H., and Makov, U. (1988) Inbreeding in human populations: assessment of the costs. InMating Patterns, eds. C.G.N. Mascie-Taylor and A.J. Boyce, pp. 153-167. Cambridge: Cambridge University Press. 3. Grant, J.C., and Bittles, A.H. (1997) The comparative role of consanguinity in infant and child mortality in Pakistan.Annals of Human Genetics61, 143-149. 4. MacArthur D.G. et al. Science 335, 823-828 (2012).