Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Environmental enrichment wikipedia , lookup
Human brain wikipedia , lookup
Neurolinguistics wikipedia , lookup
Brain morphometry wikipedia , lookup
Neuroplasticity wikipedia , lookup
Aging brain wikipedia , lookup
Time perception wikipedia , lookup
Neurophilosophy wikipedia , lookup
Metastability in the brain wikipedia , lookup
Data (Star Trek) wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Neuroesthetics wikipedia , lookup
Embodied language processing wikipedia , lookup
Neuroinformatics wikipedia , lookup
Evoked potential wikipedia , lookup
Haemodynamic response wikipedia , lookup
Neurostimulation wikipedia , lookup
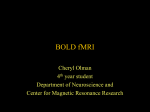
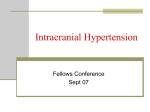
Magnetic Resonance in Medicine 57:538 –547 (2007) Flow-Metabolism Coupling in Human Visual, Motor, and Supplementary Motor Areas Assessed by Magnetic Resonance Imaging Peter A. Chiarelli, Daniel P. Bulte, Daniel Gallichan, Stefan K. Piechnik, Richard Wise, and Peter Jezzard* Combined blood oxygenation level-dependent (BOLD) and arterial spin labeling (ASL) functional MRI (fMRI) was performed for simultaneous investigation of neurovascular coupling in the primary visual cortex (PVC), primary motor cortex (PMC), and supplementary motor area (SMA). The hypercapnia-calibrated method was employed to estimate the fractional change in cerebral metabolic rate of oxygen consumption (CMRO2) using both a group-average and a per-subject calibration. The groupaveraged calibration showed significantly different CMRO2ⴚCBF coupling ratios in the three regions (PVC: 0.34 ⴞ 0.03; PMC: 0.24 ⴞ 0.03; and SMA: 0.40 ⴞ 0.02). Part of this difference emerges from the calculated values of the hypercapnic calibration constant M in each region (MPVC ⴝ 6.6 ⴞ 3.4, MPMC ⴝ 4.3 ⴞ 3.5, and MSMA ⴝ 7.2 ⴞ 4.1), while a relatively minor part comes from the spread and shape of the sensorimotor BOLD–CBF responses. The averages of the per-subject calibrated CMRO2ⴚCBF slopes were 0.40 ⴞ 0.04 (PVC), 0.31 ⴞ 0.03 (PMC), and 0.44 ⴞ 0.03 (SMA). These results are 10 –30% higher than group-calibrated values, and are potentially more useful for quantifying individual differences in focal functional responses. The group-average calibrated motor coupling value is increased to 0.28 ⴞ 0.03 when stimulus-correlated increases in end-tidal CO2 are included. Our results support the existence of regional differences in neurovascular coupling, and argue for the importance of achieving optimal accuracy in hypercapnia calibrations to resolve method-dependent variations in published results. Magn Reson Med 57:538 –547, 2007. © 2007 Wiley-Liss, Inc. Key words: cerebrovascular coupling; functional MRI; oxygen metabolism; BOLD; CBF Over the past decade, blood oxygenation level-dependent (BOLD) MRI methods (1– 4) have been developed to investigate sensorimotor and cognitive function via the hemodynamic correlates of neural activity (5,6). During a period of increased neuronal response in the brain, a disproportional rise in the inflow of fully oxygenated arterial blood dilutes the level of deoxygenated hemoglobin (dHb) in the venous vasculature, resulting in a T2*-weighted signal increase (7,8). Parallel increases in the rate of local cerebral oxygen metabolism (CMRO2) and the cerebral blood volume (CBV) partially counterbalance this cerebral blood Oxford Centre for Functional Magnetic Resonance Imaging of the Brain, Oxford University, John Radcliffe Hospital, Oxford, UK. Grant sponsors: UK Medical Research Council; Rhodes Trust; UK EPSRC. *Correspondence to: Peter Jezzard, Oxford Centre for Functional Magnetic Resonance Imaging of the Brain, Oxford University, John Radcliffe Hospital, Oxford, OX3 9DU, United Kingdom. E-mail: [email protected] Received 5 June 2006; revised 20 November 2006; accepted 20 November 2006. DOI 10.1002/mrm.21171 Published online in Wiley InterScience (www.interscience.wiley.com). © 2007 Wiley-Liss, Inc. flow (CBF)-induced signal increase by augmenting the number of paramagnetic dHb molecules present. There is no reason why such responses should be uniform across brain regions. As many have already noted (9,10), the ability to describe the quantitative relationships among CBF, CBV, and CMRO2 in multiple regions of the brain is crucial for attaining a more complete knowledge of the fundamental neurophysiology reflected in BOLD measurements (11–14). A recently developed model to extract CMRO2 estimates from experimentally available BOLD and CBF measurements (15,16) was derived by combining Fick’s principle of mass balance (17), Grubb’s relationship between fractional CBF and CBV changes (18), and the biophysical description of R2* provided by Ogawa et al. (19) and Boxerman et al. (20). Provided these relationships are accepted, the fractional change in BOLD signal can be expressed as a calibrated function of aerobic metabolism and flow change as follows: 冋 冉 冊冉 冊 册 CMR O2 ⌬BOLD ⫽M 1⫺ BOLD 0 共CMR O2兲 0  CBF CBF 0 ␣⫺ , [1] where M represents the maximum BOLD signal change (effectively in units of%) that can be attained by achieving a theoretical 100% oxygen saturation in the venous vessels (experimentally estimated using hypercapnia to provide an assumed isometabolic CBF increase), ␣ is the Grubb constant (assumed to be 0.38, accounting for an assumed fixed relationship between changes in CBV and CBF) (18), and the exponent  describes the oxygenation and fieldstrength dependence of the BOLD effect. (All previous studies with this model used  ⫽ 1.5. However, these studies predominantly were carried out at 1.5T, and at higher fields it is expected to be closer to 1 as the extravascular components of the BOLD signal begin to dominate (20,21)). To describe CMRO2 as a function of measurable MR signal changes, one can reform the equation in terms of the fractional CMRO2 change: 冢 冉 ⌬BOLD CMR O2 BOLD 0 ⫽ 1⫺ 共CMR O2兲 0 M 冊冣 1/ 冉 冊 CBF CBF 0 1⫺␣/ , [2] Table 1 summarizes recent research based on this calibrated model, which uses graded stimulation to measure the relationship between changes in CMRO2 and CBF. The CMRO2:CBF coupling ratios calculated to date span ranges of 0.22– 0.51 for the visual cortex (16,22–24) and 0.30 – 538 Flow-Metabolism Coupling by MRI 539 Table 1 Human Neurovascular Coupling Results in Literature, Using the Hypercapnia Calibrated Model With Graded Stimulation, Compared With This Study Visual cortex Study Hoge et al. (16, 22) Kastrup et al. (25) Uludag et al. (24) Stefanovic et al. (26) Stefanovic et al. (23) Current study (group calibration) Current study (per-subject calibration) Current study (group calibration with ETCO2 correction) Motor cortex SMA M (%) R2* CMRO2: CBF M (%) R2* CMRO2: CBF M (%) R2* CMRO2: CBF 22 — 25 — 7.6 ⫾ 1.3 6.6 ⫾ 3.4 4.4 — 9.6 — 1.5 ⫾ 0.3 2.1 ⫾ 1.1 0.51 ⫾ 0.08 — 0.45 ⫾ 0.03 — 0.22 ⫾ 0.11 0.34 ⫾ 0.03 — 9⫾3 — 7.2 ⫾ 0.01 6.1 ⫾ 1.1 4.3 ⫾ 3.5 — 2.3 ⫾ 0.8 — 1.4 ⫾ 0.002 1.2 ⫾ 0.02 1.3 ⫾ 1.1 — 0.3 ⫾ .06 — 0.44 ⫾ 0.04 0.49 ⫾ 0.13 0.24 ⫾ 0.03 — — — — — 7.2 ⫾ 4.1 — — — — — 2.3 ⫾ 1.3 — — — — — 0.40 ⫾ 0.02 Range 3.9–9.4 Range 1.2–2.9 0.40 ⫾ 0.04 Range 3.5–7.2 Range 1.1–2.3 0.31 ⫾ 0.03 Range 4.7–10.1 Range 1.5–3.2 0.44 ⫾ 0.03 — — — 4.3 ⫾ 3.5 1.3 ⫾ 1.1 0.28 ⫾ 0.03 — — — 0.49 for the motor cortex (23,25,26). The spread in these data obscure any possible significant difference in the neurovascular coupling ratio between these two brain regions. However, Stefanovic et al. (23) recently obtained data from both the visual and motor cortices within a single session, and demonstrated a CMRO2:CBF coupling ratio of 0.49 in the visual cortex and 0.22 in the motor cortex. That study aimed to elucidate the effect of baseline flow on the BOLD and CBF signals; hence both visual and motor stimulations were presented simultaneously, overlapping in time with the presentation of longer-hypercapnia stimuli, which may have confounded the interpretation of the data. In addition to the CMRO2⫺CBF coupling relationship, it is also crucial to identify whether regional differences can be observed in the calibration parameter M, which expresses baseline-CMRO2 BOLD⫺CBF coupling (27,28). In FIG. 1. Schematic of the experimental design, with three levels of visual stimulation and three levels of motor stimulation. In this experiment 36 min were devoted to the alternating presentation of visual and motor stimuli, and 21 min were devoted to the hypercapnic calibration. contrast to other parameters of the model, this value (in principle) can be estimated experimentally. In the present work we extend the current understanding of neurovascular coupling in the human brain by employing a paradigm that presents visual and motor stimulations separately followed by hypercapnia calibration (Fig. 1). We use the experimental scheme to assess not only regional differences but also the impact of particular features of the method on the experimental outcome. MATERIALS AND METHODS Graded Stimulation Ten healthy volunteers (age range ⫽ 24 – 40 years) participated in this study after they provided informed consent. A schematic of the experimental paradigm is provided in Fig. 1. 540 Chiarelli et al. FIG. 2. a: BOLD activation data obtained during the whole-brain pilot experiment, used to plan oblique slices through the PVC, PMC, and SMA. (b) BOLD and (c) CBF activations obtained from a single subject are overlaid on oblique-orientation EPI images. d: CBF activation map obtained from the hypercapnia calibration for the same subject. We executed 45-s blocks of visual and motor stimulations in an alternating fashion, with a pseudo-randomized level of graded stimulation. Stimulation epochs were separated by 45-s blocks of rest, during which the fixation point was displayed against a black background. The room was darkened to ensure minimum ambient light. The graded motor and visual stimulation portion of the experiment lasted for a total of 36 min, followed by 3 min of rest. Subsequently we applied two 5-min epochs of 4% inspired CO2, separated by 4 min of rest. The subjects were instructed to remain alert with their eyes directed toward the fixation point during the whole experiment. Graded visual and motor stimulation tasks were implemented as follows: Visual Stimulation For visual stimulation, a black-and-white oscillating square checkerboard stimulus at 8 Hz (eight full cycles of light and dark within a check per second) was back-projected onto a screen covering the outer bore of the magnet using an In Focus LP1000 projector providing 1024 ⫻ 768 pixels with a ⬃100 Hz refresh rate. The subjects viewed the screen via a mirror. The visual stimulus covered ⬃30° of the visual field, limited by the diameter of the magnet bore. We achieved graded activation by adjusting the “white” squares in the checkerboard to luminance fractions of 4%, 12%, and 41% (representing the values available in Microsoft Powerpoint software to adjust image brightness). The “black” squares remained at maximum darkness. In this manner we were able to simultaneously adjust total luminance and checkerboard contrast, which we found in pilot studies provided the most controllable and widest range of stimulation intensities. 3) ring, (tap 4) little, (tap 5) ring, and (tap 6) middle. This pattern was repeated in synchrony with a flashing fixation point. Subjects were trained to cue tap 1 with the appearance of the fixation point, and to cue tap 4 with the disappearance of the fixation point. To obtain a graded stimulus, the tapping cue was modulated to yield individual finger tapping rates of 1, 3, and 5 Hz. Slice Localization In a separate 165-s pilot session prior to the main experiment, each subject was presented with the oscillating black and white checkerboard in a block design and instructed to perform bilateral finger-tapping coincident with the visual stimulus. Whole-brain BOLD fMRI data were acquired during this time, and were analyzed using the in-line data analysis package provided with the scanner software to obtain functional activation maps and prescribe oblique slices that passed through the primary visual cortex (PVC), primary motor cortex (PMC), and supplementary motor area (SMA) (Fig. 2a). Hypercapnia Filtered air and 5% CO2 in air were mixed to deliver 4% inspired CO2 through a tight-fitting face mask. Respiratory composition within the mask was continuously sampled with the use of equipment from Applied Electrochemistry Inc. (Pittsburgh, PA, USA; CD-3A CO2 sensor, S-3A/I O2 sensor, and Flowcontrol R-2 vacuum pump). Data regarding the CO2 and O2 concentrations in the mask air were logged at intervals of 10 ms with the use of Powerlab software (ADInstruments, Colorado Springs, CO, USA). Motor Stimulation Motor stimulation was accomplished by voluntary cyclic opposition between the thumb and each finger, according to the following pattern: (tap 1) index, (tap 2) middle, (tap MRI Parameters Images were acquired on a Siemens Trio 3T MRI scanner using an eight-channel head radiofrequency (RF) receive Flow-Metabolism Coupling by MRI 541 FIG. 3. (a) Motor and (b) visual responses to 45-s visual stimulation epochs, followed by 2-min and 15-s rest periods. Note the difference in undershoot amplitude between the two stimulus types. coil. An interlaced BOLD/pulsed arterial spin-labeling (ASL) sequence was developed to collect T2*-weighted conventional EPI images and QUIPSS II with thin slice periodic saturation (Q2TIPS) (29,30) cerebral perfusion images in the following scheme: [ASL tag image/BOLD image/ASL control image/BOLD image]n. The parameters for the BOLD measurements included TR/TE ⫽ 4.5 s/32 ms, and for the ASL experiments they were TR/TE/ TI ⫽ 4.5 s/23 ms/1.4 s, TI1/TI2 ⫽ 700 ms/1400 ms, with a TI1 stop time of 1200 ms. The width of the tagging band was 10 cm with a gap of 1.5 cm between the tag and image volumes. In both BOLD and ASL, five slices were acquired per TR, with 4 ⫻ 4 ⫻ 6 mm3 voxel dimensions and a 64 ⫻ 64 imaging matrix. Data Analysis All analyses were performed using the FMRIB Software Library (FSL) package (31). Each fMRI acquisition yielded a sequence of interleaved EPI BOLD and ASL images, which were split and analyzed separately. The processing steps for the BOLD data included 1) 2D-FT and EPI ghost removal, 2) motion correction (32), 3) volume-by-volume extraction of brain matter from surrounding tissue and skull (33), 4) splitting images from the sensorimotor stimulation portion of the experiment and images from the hypercapnia portion into two separate data sets, 5) spatial smoothing with a 5-mm FWHM Gaussian kernel on both data sets, 4) high-pass temporal filtering with a cut-off of 180 s applied to the sensorimotor data and a cutoff of 540 s applied to the hypercapnia data, 7) autocorrelation correction using a general linear model (GLM)based nonparametric estimation method (FMRIB’s Improved Linear Model) (34), and 8) voxelwise GLM-based correlation of the signal time course with an appropriate reference model constructed by convolution of a block design boxcar function with a gamma-variate hemodynamic response model. Analysis of the Q2TIPS perfusion data included steps 1–3 as described above. We performed temporal sinc- interpolation on the set of tag images and the set of control images, shifting the signal intensity of tag images to appear as if they were acquired 0.5 TRs later, and control images to appear as if they were acquired 0.5 TRs earlier, followed by pairwise subtraction of image intensity values. Steps 4 –7 as listed above were not applied to perfusion data. GLM estimation of activation (step 8) was performed in the same manner as for the BOLD data. After the control and tag images were subtracted, the temporal resolution of the perfusion data was half that of the BOLD data set. To analyze the visual response, for which post-stimulus effects have been reported (35,36), we excluded “rest” epochs that immediately followed visual stimulation from the estimate of baseline BOLD and CBF. Only rest blocks corresponding to the intervals following the motor task were included in the estimate of visual baseline. Based on a separate block-design pilot study with alternating epochs of visual and motor stimulation (45 s “on”/135 s “off”), we observed a substantially larger post-stimulus BOLD undershoot following flashing checkerboard stimulation compared to the finger tapping task (Fig. 3). After this correction was employed, inspection of the GLM fit to the visual data from the main experiment revealed a significantly improved estimation of the baseline, whereas a negligible difference was observed when a similar analysis was performed for the motor task. Region of Interest (ROI) Definition We calculated BOLD, CBF, and CMRO2 estimates within an ROI defined for each individual subject by the overlap of statistically thresholded BOLD (z-stat ⬎ 4, cluster p-threshold ⬎ 0.05) and CBF (z-stat ⬎ 2.3, cluster p-threshold ⬎ 0.05) images. We obtained each ROI using data from the most intense of the three graded stimulus levels, and used the ROI to interrogate activation estimates at all three BOLD and CBF activation levels. 542 Chiarelli et al. RESULTS AND DISCUSSION Regional CMRO2⫺CBF Coupling BOLD and CBF images acquired at the appropriate oblique orientation are displayed for a representative subject in Fig. 2b and c, respectively, with data overlaid for the separate motor (red) and visual (blue) tasks. The thresholded CBF image (CBF zstat ⬎ 2.3, cluster p-threshold ⬎ 0.05) from the two-epoch 4% hypercapnia challenge is supplied in Fig. 2d, with activated voxels consistent with gray matter. In general the CBF maps tended to be noisier than the BOLD maps, but had a higher spatial specificity to the activated regions (see Fig. 2b and c). This is primarily due to the significantly lower signal-to-noise ratio (SNR) of the ASL data and the weighting of the BOLD signal toward the larger venous vasculature. The significance thresholds for the analyses of each data type were adjusted to account for these inherent differences. The activation maps of the two data sets compared very well with each other as a result, and by using masks constructed from the overlap of the two methods, we were able to remove the spurious voxels from the ASL data along with the activated voxels from the BOLD data set that were distal from the active brain matter regions. Obviously, there are issues that are poorly understood regarding the comparison of BOLD- and ASL-based activation maps (37). Ultimately our goal was to use a threshold criterion that yielded maps similar in size to those used by others (the size of the maps is principally constrained by the CBF threshold), particularly those based on retinotopic maps, which tend to be more spatially restrictive. Figure 4 displays GLM estimates of fractional change in BOLD and CBF for all three stimulus levels from the ROI for each individual in the PVC (Fig. 4a), PMC (Fig. 4b), and SMA (Fig. 4c). Measurements from the three different stimulation levels for a given subject are joined by lines, and data points are consistently labeled so that somatosensory activation data from each individual can be compared against the corresponding hypercapnia activation (red). The changes seen in CBF are somewhat larger than expected, most likely due to inappropriate suppression of the signal from large vessels. BOLD and CBF values for the hypercapnia data were obtained from a combined GLM fit to two consecutive 5-min blocks of 4% inspired CO2, which were separated by 4 min of breathing air. We used 4% hypercapnia instead of 5% to avoid the potential stress response and neuronal effects associated with higher levels of inspired CO2 (38 – 40). 4% CO2 represented a compromise between minimizing the stress response and maximizing the contrast for changes in BOLD and CBF. Average end-tidal CO2 levels were found to rise by ⬃7.4 mmHg during CO2 administration from a baseline value of 42.6 ⫾ 4.6 mmHg. The calibration procedure indicated by Eq. [1] was performed such that the iso-CMRO2 BOLD⫺CBF contour could be fitted to the group average BOLD and CBF values derived from hypercapnia (thick line). We obtained an estimated BOLD calibration amplitude of MPVC ⫽ 6.6 ⫾ 3.4 (similar to the value calculated by Stefanovic et al. (23)), MPMC ⫽ 4.3 ⫾ 3.5 (similar to but significantly lower than reported literature values), and MSMA ⫽ 7.2 ⫾ 4.1. The FIG. 4. Functional activation (black) and hypercapnia data (red) from the (a) PVC, (b) PMC, and (c) SMA. The resting-metabolism iso-CMRO2 contour is shown fit to the hypercapnia data. Data points are consistently labeled across the plots such that individual subject data can be compared. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.] Flow-Metabolism Coupling by MRI 543 trend observed by Stefanovic et al. of a greater M value in the PVC compared to the PMC is supported by our work. Figure 5 displays plots of the estimated fractional CMRO2 change vs. fractional CBF change obtained in the PVC (a), PMC (b), and SMA (c) regions using the single group average value of M calculated in each respective brain region. A linear fit is shown on each CMRO2⫺CBF plot. These fits were constrained to pass through the point (0,0), since all BOLD and CBF values were assumed to be calculated with respect to well-defined coincident baseline epochs. The calculated group-average CMRO2:CBF ratios were 0.34 ⫾ 0.03 (PVC), 0.24 ⫾ 0.03 (PMC), and 0.40 ⫾ 0.02 (SMA). CMRO2 data are displayed for all 10 subjects in Fig. 5, although one subject (⫹) did not complete the CO2 challenge, and therefore contributed no data to the average M value. The PMC data show a substantially weaker linear correlation (R2 ⫽ 0.40) than the other regions (R2 ⱖ 0.82). Three data sets in which the CMRO2⫺CBF trend deviated significantly from the average (based on a pooled variance t-test) are shaded gray to highlight the presence of cases in which graded stimulation did not show concurrent changes between the CMRO2 and CBF. The notion that a larger CMRO2⫺CBF slope in the PVC compared to the PMC may be warranted is supported by a comparison with other results reported by Hoge et al. (16), Kastrup et al. (25), Uludag et al. (24), and Stefanovic et al. (26). Those studies further suggest the possibility that the resting-state BOLD:CBF coupling ratio (M) is larger in the PVC compared to the PMC, a conclusion that is also supported in the present study. A second study by Stefanovic et al. (23) found a trend that is opposite to that obtained in the present study. Although the CMRO2⫺CBF slope obtained by Stefanovic et al. (23) in the PVC lies within the range of the slope obtained here, their value for the PMC is much higher than our data or previous literature data would predict. Systematic Sources of Variability Group-Average Calibration Constant An examination of the CMRO2⫺CBF relationship, as calculated using the group-average M values, hides a systematic source of variability originating from the calibration constant itself. We previously investigated the relative impact of hypercapnia data and functional stimulation data on the calculated measure of CMRO2⫺CBF coupling by the calibrated model. We observed that on a theoretical basis, the hypercapnia calibration constant determines the coupling slope and linearity of coupling for the functional activation task, while the general shape and degree of scatter in the functional BOLD⫺CBF data have a minor impact on these values (41). Figure 6 displays the variation in the experimental estimates of metabolic coupling due to uncertainty in the isometabolic profiles described by M. The thin lines describe the impact of theoretical variation in M beyond the experimentally estimated value on the calculated CMRO2⫺CBF slope in the three brain regions. There is relatively little difference between the coupling slope vs. M behavior for the three data sets, although at any single value of M the PVC data show the lowest coupling slope, the SMA data show an intermediate coupling slope, and the PMC data show the highest slope. The symbols corre- FIG. 5. CMRO2–CBF coupling plots and linear fit (thick line) in the (a) PVC, (b) PMC, and (c) SMA, as calculated using the calibrated model. Labeling of data sets is consistent with Fig. 4, and data sets that deviate significantly from the mean response are labeled in gray. 544 FIG. 6. CMRO2–CBF coupling slope fit to functional activation data from the PVC (), PMC (●), and SMA (■) over a range of possible M values. Points along each curve corresponding to the calculated M value are marked with (⫻). spond to experimental M values calculated in this study, for the PVC (), PMC (●), and SMA (■). The use of experimentally determined M values introduces a substantially further difference between the CMRO2⫺CBF slopes for the three brain regions. Note the large impact of transformed M error on the coupling slope, especially for low values of M. An M-independent measure of neurovascular coupling is likely not feasible in this low M-value regime due to the sensitivity of the model to this parameter. (See Ref. 27 for a detailed analysis of the effect that the estimation of M has on the determination of the coupling constant.) Per-Subject Hypercapnia Calibration In comparison to using a single group-average value of M to calibrate sensorimotor BOLD⫺CBF data from all subjects (as has been done in all studies to date), the use of Chiarelli et al. subject-specific M values to calibrate the corresponding sensorimotor data may more appropriately characterize the inherent variability of CMRO2⫺CBF slope between individuals, and provide a more realistic CMRO2⫺CBF coupling estimate for individuals whose vascular physiology warrants a calibration constant different from the group mean. Figure 7a– c show the range of iso-CMRO2 curves fitted on a subject-by-subject basis to hypercapnia data from the PVC, PMC, and SMA, respectively. x-Axis and y-axis error estimates represent the ⫾95% (confidence interval to mean (CIm) as obtained from the variance of the GLM fit to the underlying BOLD and perfusion hypercapnia data. Figure 7d–f display CMRO2⫺CBF plots that were recalculated using these subject-specific M values for calibration of BOLD⫺CBF data. When a linear fit is applied to the entire set of data, as in Fig. 5, the calculated CMRO2⫺CBF slopes are 0.28 ⫾ 0.08 (PVC); 0.26 ⫾ 0.04 (PMC), and 0.35 ⫾ 0.06 (SMA). These values could be interpreted as suggesting little difference between the regional CMRO2⫺CBF coupling values. However, in each plot (Fig. 7d–f), there appears to be a principle direction about which CMRO2⫺CBF data from the group are clustered. If data sets deemed as outliers (based on a 95% confidence F-test, shaded gray) are excluded from the linear fit, the resulting slopes are 0.40 ⫾ 0.04, (PVC) 0.31 ⫾ 0.03, (PMC), and 0.44 ⫾ 0.03, (SMA). The fits excluding outliers are displayed in Fig. 7, in which coupling in the SMA still reveals the highest slope, and coupling in the PMC still produces the lowest slope. Values in the SMA and PVC are more similar than for the data calculated with a group-averaged M value, as shown in Fig. 5. The recalculated values for the CMRO2⫺CBF slope in the visual and motor regions correspond roughly to values from Hoge et al. (16) (0.51 ⫾ 0.08) and Uludag et al. (24) (0.45 ⫾ 0.03) in the PVC, and the value from Kastrup et al. (25) (0.3 ⫾ 0.06) in the PMC, despite the large difference in M used to calibrate the BOLD and CBF values. Consistent labeling for the data from each subject allows a comparison between Figs. 5 and 7. Note that the data set labeled (●), whose slope deviates from the average value in FIG. 7. Per-subject hypercapnia calibration (a– c), and corresponding CMRO2–CBF coupling plots (d–f), in the PVC (a and d), PMC (b and e), and SMA (c and f). BOLD (not visible) and CBF error estimates on hypercapnia data represent ⫾CIm, as obtained from the residuals of the GLM fit. Data sets deemed outliers in d–f are labeled in gray and excluded from the linear fit. Flow-Metabolism Coupling by MRI Fig. 5b (motor), no longer is an outlier when the subjectspecific M value is used (Fig. 7e). The calculated M value from this subject is noticeably higher than the mean (Fig. 7b), suggesting a potential difference in vascular architecture. As another example, the data set labeled ⌬ reveals a negligible change in metabolism in the PMC as a function of different levels of graded stimulation when the subjectspecific M value is used. In this case, using the group average M of 4.3 (Fig. 5b) makes the coupling estimates appear closer to the group mean. It is difficult to completely exclude the possibility that the differences in the estimated M-parameters from individual subjects are simply due to inherent experimental errors in the hypercapnia calibration technique. However, a visual inspection of the error margins in Fig. 7a– c suggests that the fitted M values from many subjects overlap statistically, while a number of subjects show fitted M values that do not overlap based on the chosen 95% statistical criterion. Previous research has illustrated the effect of factors such as diet and physiological state on the neural-hemodynamic response to stimulation. It may be possible, therefore, that some of the nonlinear CMRO2⫺CBF coupling relationships between individuals can be accounted for by genuine physiological differences. Our analysis suggests that certain subjects may show such behavior, which would otherwise be masked by the use of single groupaveraged M values. Systemic Effects of Functional Stimuli Functional MRI (fMRI) experiments routinely involve a number of potential confounds related to the effects of stimulus delivery, such as stimulus-correlated motion or modulation of attention (42). One potential confound that is seldom monitored is the fluctuation of blood gasses during the experiment (43). In the current experiment we continuously measured end-tidal CO2 (ETCO2) and O2 (ETO2), which provided us with insight into respiratory effects associated with cerebral stimulation. The average baseline ETCO2 was 42.6 ⫾ 4.6 mmHg. There was a very small tendency toward an increased respiratory rate during the CO2 blocks. Across all subjects, breaths-per-minute averaged approximately 6.5 during baseline, and 7.5 at the end of the hypercapnia blocks. The increase was nearly linear over the duration of the block. Note that the total minute volume was not measured, and this variable is expected to rise with increased inspired CO2 concentration. ETO2 values were observed to rise very slightly from ⬃114 mmHg at baseline to ⬃122 mmHg at the end of the CO2 block, likely induced by the increased minute volume. However, this was a very slow rise since the effect of increased ventilation is partially counteracted by a diminished O2 concentration in the 5% CO2 in air mixture compared to normal air (the inspired level of oxygen actually drops from ⬃157 mmHg to ⬃145 mmHg). We therefore expect the impact of change in O2 concentration to be relatively minor. The issue of changing O2 concentration is an effect that is present in all of the studies compared in this work, and in the future we plan to incorporate dynamic forcing of end-tidal O2 or CO2 levels as a means to avoid this potential effect. Figure 8 displays the subject-average ETCO2 behavior during epochs of the graded motor task. Despite prior 545 FIG. 8. End-tidal CO2 response to presentation of the motor stimulus (gray blocks) for low (L), medium (M), and high (H) tapping rates. Dashed lines serve as a guide to the eye. instruction of subjects to maintain a consistent rate of breathing, we observed a significant involuntary alteration in the respiratory cycle by all subjects during the motor task (note that no difference in breathing or ETCO2 was observed during presentation of the oscillating checkerboard for visual stimulation). None of the subjects reported noticing this difference when questioned after the experiment. In some subjects the alteration in breathing was manifested as shorter, shallower breaths, whereas in others the difference was slower breathing. The result was a rise in ETCO2 levels by 0.45 mmHg during the steady-state portion of the motor task, and a further increase in ETCO2 to 0.76 mmHg above baseline near the end of the task. While these effects appear small, they constitute a sizeable 6% and 10% of the average ETCO2 change elicited by the hypercapnia calibration used in this study. There appeared to be no difference between ETCO2 responses elicited by the low (L), medium (M), and high (H) tapping rates. While the observed change in ETCO2 is not high enough to yield a statistically significant BOLD activation in non-motor areas, it likely does contribute to the measured BOLD and CBF signal changes within the ROI selected due to real PMC activation. Pilot data from lowlevel CO2 challenges suggest that the BOLD response to CO2 is roughly linear from baseline up to the changes elicited by 4% CO2. Using the hypercapnia-derived BOLD signal change in the PMC from this study as a point of reference, we estimate that the breathing-induced change in ETCO2 will yield a stimulus-correlated BOLD signal increase in the PMC between 0.08% and 0.14% (these lower and upper estimates were obtained using ETCO2 data from either of the two plateau regions in Fig. 8, marked by dashed lines). Assuming an additive effect between the apparent activation from this CO2 response and the signal change due to functional activation, we applied a correc- 546 tion to the calculation of CMRO2 by the group-calibrated approach and obtained a value for the CMRO2⫺CBF coupling slope between 0.26 and 0.28. The higher of these two values represents a 16% change from the original calculated value of the coupling slope. These data illustrate the potential importance of monitoring respiration during sensorimotor tasks, which require a large degree of concentration by the subject that may induce involuntary breathholding or respiratory changes. CONCLUSIONS In this study we performed the first simultaneous investigation of neurovascular coupling in three brain regions, and found a larger proportional increase of CMRO2 to CBF in the PVC region compared to the PMC region. An even larger CMRO2⫺CBF coupling constant was observed in the SMA. We observe that a major source of regional variability emerges from the hypercapnia calibration, while real differences between sensorimotor stimulation data in the three brain regions account for only a minor part of this regional difference. Calibration on a per-subject basis revealed a group of tightly clustered CMRO2⫺CBF data in each brain region, but with a number of noticeable outliers, which may reflect true differences in brain physiology and vascular architecture. We uncovered a significant impact of involuntary respiratory changes during the motor task, which has large potential implications for all fMRI studies that involve any kind of exertion or exercise. Chiarelli et al. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. ACKNOWLEDGMENTS We gratefully acknowledge support from the UK Medical Research Council (P.J., S.K.P., D.P.B., and R.W.), Rhodes Trust (P.A.C.), and UK Engineering and Physical Sciences Research Council (EPSRC) (D.G.). REFERENCES 1. Ogawa S, Lee TM, Kay AR, Tank DW. Brain magnetic resonance imaging with contrast dependent on blood oxygenation. Proc Natl Acad Sci USA 1990;87:9868 –9872. 2. Kwong KK, Belliveau JW, Chesler DA, Goldberg IE, Weisskoff RM, Poncelet BP, Kennedy DN, Hoppel BE, Cohen MS, Turner R, Cheng HM, Brady TJ, Rosen BR. Dynamic magnetic resonance imaging of human brain activity during primary sensory stimulation. Proc Natl Acad Sci USA 1992;89:5675–5679. 3. Bandettini PA, Wong EC, Hinks RS, Tikofsky RS, Hyde JS. Time course EPI of human brain function during task activation. Magn Reson Med 1992;25:390 –397. 4. Ogawa S, Tank DW, Menon R, Ellermann JM, Kim SG, Merkle H, Ugurbil K. Intrinsic signal changes accompanying sensory stimulation: functional brain mapping with magnetic resonance imaging. Proc Natl Acad Sci USA 1992;89:5951–5955. 5. Haacke EM, Lai S, Reichenbach JR, Kuppusamy K, Hoogenraad FGC, Takeichi H, Lin W. In vivo measurement of blood oxygen saturation using magnetic resonance imaging: a direct validation of the blood oxygen level-dependent concept in functional brain imaging. Hum Brain Mapp 1997;5:341–346. 6. Yablonskiy DA, Haacke EM. Theory of NMR signal behavior in magnetically inhomogeneous tissues: the static dephasing regime. Magn Reson Med 1994;32:749 –763. 7. Buxton RB, Wong EC, Frank LR. Dynamics of blood flow and oxygenation changes during brain activation: the balloon model. Magn Reson Med 1998;39:855– 864. 8. Lee SP, Duong TQ, Yang G, Iadecola C, Kim SG. Relative changes of cerebral arterial and venous blood volumes during increased cerebral 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. blood flow: implications for bold fMRI. Magn Reson Med 2001;45:791– 800. Li TQ, Haefelin TN, Chan B, Kastrup A, Jonsson T, Glover GH, Moseley ME. Assessment of hemodynamic response during focal neural activity in human using bolus tracking, arterial spin labeling and BOLD techniques. Neuroimage 2000;12:442– 451. Hyder F, Rothman DL, Shulman RG. Total neuroenergetics support localized brain activity: implications for the interpretation of fMRI. Proc Natl Acad Sci USA 2002;99:10771–10776. Rees G, Howseman A, Josephs O, Frith CD, Friston KJ, Frackowiak RSJ, Turner R. Characterizing the relationship between BOLD contrast and regional cerebral blood flow measurements by varying the stimulus presentation rate. Neuroimage 1997;6:270 –278. Nakai T, Matsuo K, Kato C, Takehara Y, Isoda H, Moriya T, Okada T, Sakahara H. Post-stimulus response in hemodynamics observed by functional magnetic resonance imaging— difference between the primary sensorimotor area and the supplementary motor area. Magn Reson Imaging 2000;18:1215–1219. Kim SG. Progress in understanding functional imaging signals. Proc Natl Acad Sci USA 2003;100:3550 –3552. Obata T, Liu TT, Miller KL, Luh WM, Wong EC, Frank LR, Buxton RB. Discrepancies between BOLD and flow dynamics in primary and supplementary motor areas: application of the balloon model to the interpretation of BOLD transients. Neuroimage 2004;21:144 –153. Davis TL, Kwong KK, Weisskoff RM, Rosen BR. Calibrated functional MRI: mapping the dynamics of oxidative metabolism. Proc Natl Acad Sci USA 1998;95:1834 –1839. Hoge RD, Atkinson J, Gill B, Crelier GR, Marrett S, Pike GB. Investigation of BOLD signal dependence on cerebral blood flow and oxygen consumption: the deoxyhemoglobin dilution model. Magn Reson Med 1999;42:849 – 863. Jezzard P, Ramsey NF. Functional MRI. In: Tofts P, editor. Quantitative MRI of the brain: measuring changes caused by disease. West Sussex, UK: John Wiley & Sons; 2003. Grubb Jr RL, Raichle ME, Eichling JO, Ter Pogossian MM. The effects of changes in PaCO2 on cerebral blood volume, blood flow, and vascular mean transit time. Stroke 1974;5:630 – 639. Ogawa S, Menon RS, Tank DW, Kim S-G, Merkle H, Ellermann JM, Ugurbil K. Functional brain mapping by blood oxygenation level-dependent contrast magnetic resonance imaging. A comparison of signal characteristics with a biophysical model. Biophys J 1993;64:803– 812. Boxerman JL, Bandettini PA, Kwong KK, Baker JR, Davis TL, Rosen BR, Weisskoff RM. The intravascular contribution to fMRI signal change: Monte Carlo modeling and diffusion-weighted studies in vivo. Magn Reson Med 1995;34:4 –10. Buxton RB. Introduction to functional magnetic resonance imaging. Cambridge, UK: Cambridge University Press; 2002. p 394 –395. Hoge RD, Atkinson J, Gill B, Crelier GR, Marrett S, Pike GB. Linear coupling between cerebral blood flow and oxygen consumption in activated human cortex. Proc Natl Acad Sci USA 1999;96:9403–9408. Stefanovic B, Warnking JM, Rylander KM, Pike GB. The effect of global cerebral vasodilation on focal activation hemodynamics. Neuroimage 2006;30:726 –734. Uludag K, Dubowitz DJ, Yoder EJ, Restom K, Liu TT, Buxton RB. Coupling of cerebral blood flow and oxygen consumption during physiological activation and deactivation measured with fMRI. Neuroimage 2004;23:148 –155. Kastrup A, Krüger G, Neumann-Haefelin T, Glover GH, Moseley ME. Changes of cerebral blood flow, oxygenation, and oxidative metabolism during graded motor activation. Neuroimage 2002;15:74 – 82. Stefanovic B, Warnking JM, Pike GB. Hemodynamic and metabolic responses to neuronal inhibition. Neuroimage 2004;22:771–778. Chiarelli PA, Bulte DP, Piechnik S, Jezzard P. Sources of systematic bias in hypercapnia-calibrated functional MRI estimation of oxygen metabolism. Neuroimage 2007;34:35– 43. Chiarelli PA, Bulte DP, Piechnik S, Jezzard P. Sources of systematic bias in hypercapnia calibrated functional mri estimation of oxygen metabolism. In: Proceedings of the Annual Meeting of ISMRM, Seattle, WA, USA, 2006 (Abstract 2764). Luh WM, Wong EC, Bandettini PA, Hyde JS. QUIPSS II with thin-slice TI1 periodic saturation: a method for improving accuracy of quantitative perfusion imaging using pulsed arterial spin labeling. Magn Reson Med 1999;41:1246 –1254. Flow-Metabolism Coupling by MRI 30. Wong EC, Buxton RB, Frank LR. Quantitative imaging of perfusion using a single subtraction (QUIPSS and QUIPSS II). Magn Reson Med 1998;39:702–708. 31. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TEJ, Johansen-Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004;23(Suppl 1):S208 –S219. 32. Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 2002;17:825– 841. 33. Smith SM. Fast robust automated brain extraction. Hum Brain Mapp 2002;17:143–155. 34. Woolrich MW, Ripley BD, Brady M, Smith SM. Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimage 2001;14: 1370 –1386. 35. Schroeter ML, Kupka T, Mildner T, Uludag K, von Cramon DY. Investigating the post-stimulus undershoot of the BOLD signal— a simultaneous fMRI and fNIRS study. Neuroimage 2006;30:349 – 358. 36. Buxton RB, Wong EC, Frank LR. The post-stimulus undershoot of the functional MRI signal. In: Moonen CTW, Bandettini PA, editors. Functional MRI. New York: Springer; 1999. p 253–262. 547 37. Tjandra T, Brooks JCW, Figueiredo P, Wise R, Matthews PM, Tracey I. Quantitative assessment of the reproducibility of functional activation measured with BOLD and MR perfusion imaging: implications for clinical trial design. Neuroimage 2005;27:393– 401. 38. Kliefoth AB, Grubb Jr RL, Raichle ME. Depression of cerebral oxygen utilization by hypercapnia in the rhesus monkey. J Neurochem 1979; 32:661– 663. 39. Stein SN, Pollock GH. Central inhibitory effects of carbon dioxide II. Proc Soc Exp Biol Med 1949;70:290 –291. 40. Kogure K, Busto R, Scheinberg P, Reinmuth O. Dynamics of cerebral metabolism during moderate hypercapnia. J Neurochem 1975;24:471– 478. 41. Chiarelli PA, Bulte DP, Piechnik S, Jezzard P. Sources of systematic bias in hypercapnia-calibrated functional mri estimation of oxygen metabolism. In: Proceedings of the 14th Annual Meeting of ISMRM, Seattle, WA, USA, 2006 (Abstract 2764). 42. Lund TE, Norgaard MD, Rostrup E, Rowe JB, Paulson OB. Motion or activity: their role in intra- and inter-subject variation in fMRI. Neuroimage 2005;26:960 –964. 43. Wise RG, Ide K, Poulin MJ, Tracey I. Resting fluctuations in arterial carbon dioxide induce significant low frequency variations in BOLD signal. Neuroimage 2004;21:1652–1664.