Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biology and sexual orientation wikipedia , lookup
Genome evolution wikipedia , lookup
Human genetic variation wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gene expression profiling wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Pharmacogenomics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Gene desert wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Public health genomics wikipedia , lookup
Gene nomenclature wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Frameshift mutation wikipedia , lookup
Medical genetics wikipedia , lookup
Genetic engineering wikipedia , lookup
Oncogenomics wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Gene therapy wikipedia , lookup
Gene expression programming wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Point mutation wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Neocentromere wikipedia , lookup
Y chromosome wikipedia , lookup
Microevolution wikipedia , lookup
Designer baby wikipedia , lookup
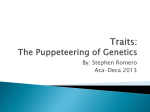
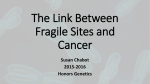
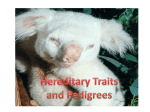
Human Reproduction, Vol. 14, (Suppl. 1), pp. 24-37, 1999 Genetics of male subfertility: consequences for the clinical work-up Wolfgang Kiipker1'5, Eberhard Schwinger2, Olaf Hiort3, Michael Ludwig1, Nikos Nikolettos1, Peter N.Schlegel4 and Klaus Diedrich1 department of Obstetrics and Gynecology, institute of Human Genetics, 3 Department of Pediatrics, Medical University Liibeck, Ratzeburger Allee 160, 23538 Liibeck, Germany and 4James Buchanan Brady Foundation, Department of Urology, New York Hospital - Cornell Medical Center, New York, USA 5 To whom correspondence should be addressed Major principles of genetic failures, chromosomal alterations and the most common syndromes associated with male subfertility should be taken into account before medical therapy and sophisticated techniques of assisted fertilization are applied to help a couple conceive. This review addresses the most common genetic reasons for male subfertility or infertility with special regard to the importance for the clinical work-up in daily routine and the potential risks for the conceptus. Key words: androgen receptor/chromosome disorders/genetics/male subfertility/ Y deletions Introduction Severe male subfertility is assumed to be the reason for infertility in up to 50% of all childless couples. In about 30% of these cases genetic disorders are suspected to be the basis. These disorders present with a large variety of clinical features, but mostly severe oligoasthenoteratozoospermia or azoospermia is the predominant symptom. The human genome probably contains up to 100 000 genes. Alteration in even one base pair of a gene can result in an absent or abnormal protein with potentially serious phenotypic consequences. More than 1000 genes are known to regulate the human fertility status. A mutation in a single gene can cause fertility problems, but on the other hand it has to be taken into account that germ line development, male gonad development and male somatic development are under control of a complex genetic network. Genetic disorders currently known to occur during human spermatogenesis include chromosomal aneuploidy and mutations in spermatogenesis genes. These disorders are inherited or result from new mutations. A screening for genetic failures and chromosomal alterations 24 © European Society for Human Reproduction and Embryology Clinical work-up for male subfertility associated with male subfertility should be carried out before medical therapy and sophisticated techniques of assisted fertilization are applied to help a couple conceive. Numerical and structural chromosome disorders Chromosome disorders are numerical or structural. Polyploidy is defined as a chromosome number that is an exact multiple of 23. Triploidy or tetraploidy are most unlikely to be compatible with life, and are often seen in spontaneous abortions. Structural aberrations result from chromosome breakage. Different types of chromosomal rearrangements have to be distinguished as there are losses of genomic material resulting from deletions, duplications and inversions. Fusion of both ends of a chromosome results in the formation of a ring chromosome. If breakage involves more than one chromosome, translocations occur. In reciprocal translocations genetic material distal to the breakage points is exchanged between homologous and non-homologous chromosomes. If no genetic material has been lost, the individual is phenotypically normal-appearing and healthy — a balanced translocation carrier. As early as 1957, Ferguson-Smith et al. suspected the impact of chromosomal aberrations as the underlying basis for the infertility of their 91 azoo- and oligozoospermic patients, where they were able to detect a Barr body in 10 cases (Ferguson-Smith et al., 1957). Two years later it was demonstrated that those men could be karyotyped as 47,XXY, the Klinefelter syndrome (Jacobs and Strong, 1959). Another study reviewed the results of 20 studies concerning the karyotypes of severely subfertile or infertile males (De Braekaleer and Dao, 1991). The most frequent aberration was Klinefelter syndrome, in almost 5% of cases, which is a 44-fold higher prevalence compared to a normal fertile population. A total of 1.8% of patients presenting with severe oligoasthenoteratozoospermia and 0.1% with azoospermia were found to have Robertsonian translocations, a fusion of two acrocentric autosomes. In most of those cases a 13; 14 translocation was detected. Reciprocal translocations and pericentric inversions have been seen in a 7-13-fold higher percentage among subfertiles. The prevalence of chromosomal anomalies can be expected to be significantly increased in a range of 2.1% up to 8.6% in a non-selected group of males with subfertility as reported by several authors (Chandley, 1979; Abrahamsson et al., 1982; Zuffardi and Tiepolo, 1982; Yoshida et al, 1995) as compared with the general male population (0.7-1%). Severity of spermatogenic impairment and prevalence of chromosomal anomalies seem to be positively correlated. Studies on male and female in-vitro fertilization (IVF) patients demonstrated an increase of translocations and chromosomal mosaics. Our own studies concerning chromosomal abnormalities among 440 subfertile males designated for an intracytoplasmic sperm injection (ICSI) treatment revealed a prevalence of 4.3% (19/ 440). All patients presented with a sperm concentration below 20xl0 6 /ml. Thus, 25 W.Kiipker et al. treatment options such as ICSI exclusively involve a male population at a particular higher risk for chromosomal abnormalities. The most common numerical chromosome anomaly in infertile men is 47,XXY; 90% of affected males display the classic condition of 47,XXY, and mosaic forms 46,XY,47,XXY also exist. The classic Klinefelter syndrome results from meiotic non-disjunction of the X chromosome. Mosaic forms are caused by mitotic non-disjunction of the X chromosome after fertilization. Patients with Klinefelter syndrome mostly present with a small testes volume and azoospermia. Plasma testosterone concentrations are decreased whereas oestradiol concentrations tend to be elevated. The mosaic variant is not as severe as the classic form. Testes size may be normal, azoospermia is less common. Focal spermatogenesis can be detected (Ferguson-Smith et al., 1957; Gordon et al., 1972). The karyotype XXY is encountered in -1:700-1000 of newborns. Few cases have been reported for men with Klinefelter syndrome having very few motile spermatozoa in the ejaculate (Foss and Lewis, 1971) It is not known why this chromosome constitution causes infertility, but the balance of sex chromosomes seems to play an important role. It was previously reported that testicular sperm extraction yielded motile spermatozoa in four out of nine patients, but pregnancies were not established (Tournaye et al., 1996). It is interesting that spermatozoa from an XXY male have been found to be gonosomal haploid at a very high percentage (Martini et al., 1996). Men with azoospermia and a 46,XX karyotype are found less frequently (1:20 000 newborns). Male development in these patients is due to a chromosomal translocation of the short arm of the Y chromosome on the short arm of the X chromosome. The phenotype of those men depends on the breakpoint of the translocated Y material. Men with azoospermia and the karyotype 45,X are rare. They have an unbalanced karyotype because the distal part of the long arm of the Y chromosome is lost. The other part of the Y chromosome including the SRY locus is translocated to mostly acrocentric autosomes. In order to evaluate risk factors for inheritance of chromosomal abnormalities, analysis of meiotic segregation patterns can be applied. Meiotic segregation patterns With the introduction of fluorescent in-situ hybridization (FISH) and its application in human spermatozoa, a great number of sperm nuclei can be investigated within a short time. The segregation mode for most of the translocations can be studied to determine the ratio of chromosomally balanced, unbalanced and normal spermatozoa. But the frequency of chromosomally unbalanced spermatozoa varies and is dependent on the underlying aberration. Even in different patients with the same anomaly, the rate of unbalanced spermatozoa can vary greatly. Most investigators who looked for meiotic segregation patterns (Balkan and Martin, 1983; Pellestor et al., 1987; Martin et al, 1992; Syme and Martin, 1992) reported a tendency to a much higher rate of normal and balanced gametes than 26 Clinical work-up for male subfertility unbalanced. However, the segregation pattern and the percentage of normal haploid or balanced spermatozoa in the ejaculate of a chromosomal aberrant patient is important for evaluating the risk of inheritance when techniques of assisted fertilization such as ICSI are applied. Azoospermia factor (AZF) and deletions of the Y chromosome Recently, there have been several studies devoted to defining key regions on the Y chromosome which are suspected to contain important genes responsible for spermatogenesis. These regions are located on the long arm of the Y chromosome (Yqll). A variety of spermatogenic defects have been associated with microdeletions of these regions. The corresponding gene locus is known as azoospermia factor (AZF). In the first report of the presence of such a locus (Tiepolo and Zuffardi, 1976) 1170 subfertile men were karyotyped, of whom six azoospermic males were found to have microscopic deletions on the long arm of the Y chromosome. Thus, the existence of the AZF was claimed. The Y chromosome consists of three different structural and functional parts, the euchromatic part on the short arm (Ypll), the euchromatic part on the long arm (Yqll) and the heterochromatin on the long arm (Yql2). G-banding exhibits 12 different parts of the heterochromatin, which consists almost completely of repetitive DNA sequences. The entire Y chromosome comprises 59 megabases of genetic information in the euchromatic regions on both arms (Vogt et al., 1997). To date, three deletion maps of the Y chromosome have been constructed (Affara et al., 1996). The commonly used map separates the euchromatic region into seven intervals and several subintervals (Vollrath et al., 1992). Ma et al. (1992) identified distinct deletions in two karyotypically normal azoospermic males in interval 6 of Yqll (JOLAR, in subinterval 1 and KLARD, between subintervals 12 and 14), on which basis 1 year later the same authors characterized two genes as being responsible for azoospermia, YRRM1 and YRRM2 (Y chromosome RNA Recognition Motif) which are now known to be RBM (RNAbinding motif) (Ma et al., 1993). Another study described the presence of another gene within the AZF region which they called DAZ (Deleted in Azoospermia) (Reijo et al., 1995). They studied 89 azoospermic men using a polymerase chain reaction (PCR)-based analysis with 84 sequence-tagged sites (STS). Of these men, 12 (13%) were found to have overlapping deletions on Yq. Subsequent analysis of severely oligozoospermic males revealed that DAZ deletions may also be present in men with sufficient spermatogenesis to have spermatozoa in the ejaculate (Reijo et al., 1996). Vogt et al. (1996) published a study on 370 azoospermic and severely oligozoospermic men in which 12 of them were found to have submicroscopic deletions of intervals 5 and 6. They claimed the existence of three genetically active regions, AZFa, AZFb and AZFc. It is postulated that these three regions on the Y-chromosome correspond to different histological patterns of spermatogenic failure. Whereas patients with deletions in AZFa display a complete absence of germ cells, men with deletions in AZFb exhibit a 27 W.Kupker et al. maturation arrest of spermatogenesis before or at meiosis. On the other hand, deletions in AZFc which correspond to the DAZ region seem not to be associated with a specific interruption phase of spermatogenesis and can result either in azoospermia or in oligozoospermia with few mature spermatozoa in the ejaculate. Since the first reports of Y chromosome-specific deletions many studies have been performed (Table I, Figure 1) to look for deletions in azoospermic and oligozoospermic patients referred to assisted fertilization programmes. There is strong evidence that Y deletions are actually involved in the development of spermatogenesis failure, but the apparently diverse findings concerning the prevalence are confusing for the scientific community. It remains to be clarified if these differences are due to patient selection, number of analysed STS or technical problems of PCR application. Reijo et al. (1996) analysed 84 STS in Yqll of patients with non obstructive azoospermia and detected deletions in 13.5%. The same authors (Reijo et al., 1996) found 5.3% in severely oligozoospermic patients using 110 STS. The overall results of Vogt et al. (1997) indicate a significantly fewer (4.6%) after the screening of 700 patients. They applied 27 STS in their PCR assay comprising the relevant Y regions of AZFa, AZFb and AZFc (DAZ). Our own data obtained after screening 245 men for deletions in the DAZ region (six STS in single PCR technique) appear rather disappointing. Out of 92 non-obstructive azoospermic males only one patient displayed a large deletion comprising the complete DAZ region (Ludwig et al., 1998). All blood samples of patients with non-obstructive azoospermia were additionally analysed in a reference laboratory (P.N.Schlegel, New York) using single and multiplex PCR of 35 STS with identical results. On the other hand, using the same 35 STS Schlegel detected a prevalence of 6.3% among his subfertile patients (Girardi et al, 1997). Until now little has been known about the origins and mechanisms of the molecular rearrangements in Yqll resulting in deletions and loss of Y-specific genetic material. Y chromosomal rearrangements and possibly the loss of genetic material are expected to occur during meiosis associated with sister chromatid exchange, spermatid development or in the spermatozoa of the germ line of the patients' fathers or de novo during early embryogenesis (Edwards and Bishop, 1997). A different mechanism leading to Y deletions could relate to the specific patterns of DNA condensation and packing that occur during spermiogenesis. It seems unlikely that very small deletions of, for example, one STS cause severe spermatogenic impairment (Pryor et al., 1997): this has to be ruled out if these deletions are definitely polymorphisms or rather represent inefficient amplification due to technical problems of PCR procedure. Most studies could demonstrate that subfertile men typically present with deletions of at least 0.5-1 X106 base pairs of DNA in length. If there is any relation between the extent of deletion and its region with regard to the testis, histology has to be studied in more detail within the near future. Since Y chromosome inheritance is of paternal origin, men with somatic Y deletions are likely to have male offspring with similar genetic defects after assisted fertilization. Moreover, there is evidence that mosaicism in the paternal 28 Clinical work-up for male subfertility Figure 1. Microdeletions of the Y chromosome as reported in the literature. germ cell line is possible in subfertile males when Y-specific deletions are not detectable in the somatic cell line. These patients could transmit deletions to their male offspring (Kent-First et al., 1996). However, to enable a detailed analysis of the origin of AZF deletions, single cell analysis of spermatids and 29 W.Kupker et al. Table I. Results of Yqll microdeletions in azoo- and oligozoospermic men (according to Vogt, 1998) First author n Azoo Nagafuchi (1993) Kobayashi (1994) Reijo (1995) Kent-First (1996) Najmabadi (1996) Nakahori (1996) Qureshi (1996) Reijo (1996) Stuppia (1996) Vogt(1996) Brown (1997) Foresta (1997) Girardi (1997) Kremer (1997) McElreavey (1997) Simoni (1997) Stuppia (1997) Van der Ven (1997) Vogt(1997) 50 63 89 32 60 153 100 35 33 370 345 38 160 164 100 168 50 204 700 50 59 89 13 50 135 53 0 19 Oligo + AZF 0 4 0 19 10 18 4 35 14 370 228 16 118 53 64 74 0 44 117 22 42 111 36 94 50 158 700 STS AZF 26 16 84 64 23 23 22 110 14 76 82 15 35 8 35 4 27 27 27 6 8 12 4 13 20 8 0 6 13 39 11 10 7 9 5 0 2 32 Oligo 0 2 0 3 1 3 2 2 1 6 9 3 . 3 3 1 2 6 1 12 %a 12.0 16.0 13.5 9.4 18.0 13.0 8.0 5.3 18.0 5.0 11.3 18.4 6.3 4.3 14.0 3.0 12.0 1.0 4.6 Percentage of patients with AZF deletions. n = number of patients; Azoo = patients with azoospermia; Oligo + AZF — patients with oligozoospermia; STS = sequence tagged sites; AZF — patients with deletions in AZFa, b and c; Oligo = patients with oligozoospermia and AZF deletions. spermatozoa might be essential. If we assume that about one in 1000 men is azoospermic and that up to 15% of them will have Y deletions, then the frequency of this genetic defect would be about one in 10 000 births if techniques of assisted fertilization are applied in those infertile couples. Each Y gene, such as RBM and DAZ which are expressed in the testis, is located in Yqll in a position overlapping one of the AZF regions. RBM and DAZ encode an mRNA binding protein whose definite function is not yet known. SPGY (SPermatogenesis Gene locus on the Y; described by Vogt et al., 1996) belongs to the same gene family as DAZ (now DAZ1) and was recently renamed as DAZ2. Moreover, DAZ has one additional gene copy on the short arm of chromosome 3 and is called DAZH (for DAZ Homologue) or DAZL1 (for DAZlike 1). Most recently, 12 new Y genes having multiple copies on the Y chromosome or homologues on the X chromosome have been described (Lahn and Page, 1997). It is up to further research to reveal the secrets of function of these new genes and how they are involved in spermatogenesis. Many genes assumed to be involved in spermatogenesis are not located on the Y chromosome. It is not known if the Y chromosome contains a specific set of spermatogenesis genes serving as primary controls or only as fine tuners in the process of spermatogenesis (Burgoyne, 1991). The genetic control of human spermatogenesis is not only based on the function of single genes but also on regulatory and interactive gene networks. 30 Clinical work-up for male subfertility Obstructive azoospermia and mutations in the CFTR gene Cystic fibrosis (CF) is the most common autosomal recessive disorder with an incidence of 1:2.500 live births and a carrier frequency of 1:20. The cystic fibrosis gene was identified in 1989 and encodes the cyclic adenosine monophosphate-regulated chloride channel found in secretory epithelian cells (Kerem et al., 1989). The gene is called cystic fibrosis transmembrane conductance regulator gene (CFTR). More than 800 gene mutations have been detected in the meantime. Clinical features of classic CF are chronic pulmonary obstruction and infections, insufficiency of the exocrine pancreas, neonatal meconium ileus, elevated sweat electrolytes and male infertility. The loss or reduction of chloride channel function as well as defective acidification of intracellular compartments in CF epithelia likely account for the majority of the classical clinical symptoms in CF. Infertility results from congenital bilateral absence or atrophy of the vas deferens (CBAVD). The body of the epididymis may also be affected but the testicular efferent ducts tend to be spared and some may be dilated. Semen analysis reveals azoospermia in almost all adults with CF. But CBAVD can also be detected as an isolated anomaly of the Wolffian duct structures. It has been shown that anomalies of the Wolffian duct structures seem to be associated with mutations of the CFTR gene without any other clinical manifestations of CF. Recently, it could be demonstrated that men who are affected by CBAVD have a striking increase (60%) of heterozygous mutations in the CFTR gene including compound heterozygotes, which means different mutations in each gene copy (Patrizio and Asch, 1994). A majority of these heterozygotes could be shown to have a DNA variant in a non-coding sequence of the CFTR gene, the 5 T (thymidines) allele in the 3' splicing region of intron 8 (Chillon et al., 1995). Seven T or nine T are normally found in this region, whereas the reduction of T (5 T) results in the reduction of efficiency of splicing exon 9 to code for transcription of CFTR mRNA (Figure 2). In the presence of 5 T of two alleles with only 10-40% of CFTR mRNA is produced in its complete form, resulting in the reduction of CFTR protein or the expression of non-functional proteins, although the amount of CFTR protein may be sufficient to prevent CF symptoms in lung and pancreas. In this way, obstructive azoospermia can be an important marker for mild features of CF in phenotypically healthy males. Moreover, there are reports of occasional fertile men with CF mutations and with minimal evidence of disease (Barreto et al., 1991). Another condition associated with obstructive azoospermia and chronic sinopulmonary infections is Young's syndrome. Although an increased frequency of CFTR gene mutations has been observed in males with Young's syndrome, a clear association between the syndrome and CF could not be established (LeLannou et al., 1995). Androgen receptor gene mutations in male subfertility Spermatogenesis is dependent on functioning androgen metabolism, mainly on testosterone. Testosterone potentiates the prevention of Sertoli cell apoptosis 31 W.Kiipker et al. 5T 7T 9T -GTGTG(T) n AACAG CFTR gene Exon 10 Exon9 Exon8 Intron Intron CFTRmRNA Exon 8 Exon 9 Exon 10 CFTRmRNA Functional CFTR Translation CFTRmRNA (no exon 9) Inactive CFTR Figure 2. Impact of different numbers of T (thymidines) on CFTR gene expression. synergistically with follicle stimulating hormone to maintain sperm maturation (Tesarik et al., 1998). A form of minimal androgen resistance was believed to play a biochemical role in some cases of male infertility (Aiman et al., 1979); however, its importance is controversial (Aiman et al., 1982; Bouchard et al., 1986). Testosterone and dihydrotestosterone act via the androgen receptor (AR) to regulate transcription of target genes in these cells and thus the AR gene can be a candidate gene for male infertility. The AR belongs to the large steroid receptor superfamily and consists of three major functional domains (Figure 3). Transcriptional regulation is mediated by sequences within the N-terminal end, while distinct DNA- and hormone-binding regions are present. In clinical human disease, the AR has drawn attention because mutations of the AR gene cause various virilization disorders in 46,XY individuals with phenotypes ranging from unequivocally female through to patients with ambiguous genitalia and to males with only slight inhibition of masculinization (Hiort et al., 1996). Interestingly, patients with androgen insensitivity all have a severe defect of spermatogenesis. The AR gene is located on the X chromosome and mutations are inherited through healthy female carriers. It comprises 8 exons encoding for a protein of 919 amino acids. Within the large first exon, two polymorphic repeat regions are located, one CAG (polyglutamine) repeat and one GGN (poly-glycine) repeat. However, the exons 2 to 8 are highly conserved within the steroid receptor family. With the cloning of the AR gene, over 300 patients with distinct mutations have been described (Gottlieb et al., 1998). These mutations can be spread throughout the gene, affecting all major domains of the AR protein. However, 32 Clinical work-up for male subfertility X-Chromosome q 11-12 2 2 3 3 4 4 5 5 6 6 7 7 8 3' COOH NH2 AR + 7*-. ++ Z n +++ Zn Steroid binding site Figure 3. Gene expression and structure of the androgen receptor. even with the same mutation, the phenotype may be highly variable (Hiort et al, 1996; Wang et al, 1998a). To date, nine males have been described with a distinct point mutation in the AR gene and a severe defect of spermatogenesis without a virilization deficit (Akin et al, 1991; Tsukada et al., 1994; Yong et al., 1994; Hiort et al, 1997; Wang et al, 1998a,b; Shkolny et al, 1999). These males suffered from severe oligoteratozoospermia or even from azoospermia. However, in three males successful pharmacological treatment with clomiphene, tamoxifen, or high dose androgen treatment resulted in major improvement of the sperm count and even in pregnancy (Gooren, 1989; Akin, 1993; Yong et al, 1994). The CAG-trinucleotide repeat within the first exon has drawn specific attention. This polymorphism usually comprises 13-30 repeats. Elongation of this repeat region encoding for more than 40 glutamines is associated with the development of a spinal and bulbar muscular atrophy (Kennedy's disease), a neurodegenerative disorder affecting adult males who also present with a slight virilization deficit. It was recently demonstrated that infertile males have significantly longer CAG repeats within the normal range than normal controls (Tut et al, 1997). This elongation is associated with a reduced transactivational capability of the AR. This concept, however, was challanged by Giwercman et al. (1998), who could not demonstrate this finding in a large cohort of infertile males from Sweden. In conclusion, the AR gene may play an important role as a genetic determinant of male subfertility. Whether infertile or subfertile males with AR gene mutations generally respond favourably to conservative treatment options still remains to be investigated. However, further identification of molecular abnormalities of the 33 W.Kiipker et al. AR gene in those males will give interesting insight into the mechanisms of androgen action needed for normal spermatogenesis. Conclusions Male subfertility is based on genetic abnormalities in about 30% of total cases. According to Engel and Schmidt, the prevalence of genetically linked subfertility would increase from 1.8 to 2.3% within 600 years, if genetically linked subfertility accounted for 100% of subfertility and conception was achieved exclusively by using assisted reproductive techniques (Engel and Schmidt, 1995). Thus, according to them assisted reproduction does not significantly influence the human genetic pool. When carrying out assisted reproduction treatment for male and female infertility practitioners are obliged to assure the transmission of the minimum of genetic alterations. Therefore the assessment of the chromosomal state and their inheritance is recommended. Thus in patients presenting with oligoasthenoteratozoospermia, chromosome analysis must be included in the diagnostic procedure. The role of deletions of the Y chromosome and the androgen receptor remains to be further investigated. Patients with obstructive azoospermia should be investigated for mutations in the CFTR-gene. To analyse the segregation patterns in spermatozoa and thus to assess the risk for inheritance, the FISH technique is extremely useful. Moreover, besides the technical screening, the first and most important step in undergoing infertility treatment is the physician's support and guidance to enable couples to make individual decisions. References Abramsson, L., Beckman, G., Dunchek, M. et al. (1982) Chromosomal aberrations and male infertility. J. Urol, 128, 52-53. Affara, N., Bishop, C , Brown, W. et al. (1996) Report of the Second International Workshop on Y chromosome mapping 1995. Cytogenet. Cell. Genet., 73 (Suppl.), 33-76. Aiman, J. and Griffin, J.E. (1982) The frequency of androgen receptor deficiency in infertile men. J. Clin. Endocrinol. Metab., 54, 725-732. Aiman, J., Griffin, J.E, Gazar, J.M. et al. (1979) Androgen insensitivity as a cause of infertility in otherwise normal men. N. Engl. J. Med., 300, 223-227. Akin, J.W. (1993) The use of clomiphene citrate in the treatment of azoospermia secondary to incomplete androgen resistance. Fertil. Steril., 59, 223-224. Akin, J.W., Behzadian,A., Tho, S.P.T. and McDonough, P.G. (1991) Evidence for a partial deletion in the androgen receptor gene in a phenotypic male with azoospermia. Am. J. Obstet. Gynecoi, 165, 1891-1894. Balkan, W. and Martin, R. (1983) Segregation of chromosomes into the spermatozoa of a man heterozygous for a 14q21q Robertsonian translocation. Am. J. Med. Genet., 16, 169-172. Barreto, C , Piato, M., Duarte, A. et al. (1991) A fertile male with cystic fibrosis: molecular genetic analysis. J. Med. Genet., 28, 420. Bouchard, P., Wright, E, Portois, M.C. et al. (1986) Androgen insensitivity in oligospermic men: A reappraisal. J. Clin. Endocrinol. Metab., 63, 1242-1246. Brown, L.G., Alagappan, R., Sawai-Kawagucci, T. et al. (1997) Deletions of the DAZ gene cluster in men with azoospermia and oligozoospermia. Abstract. Cytogenet. Cell Genet., 79, 1-20. 34 Clinical work-up for male subfertility Burgoyne, PS. (1991) Y chromosome function in mammalian development. Adv. Dev. Biol, 1, 1-29. Chandley, A.C. (1979) The chromosomal basis of human infertility. Br. Med. Bull., 35, 181-186. Chillon, M., Casals, T., Mergier, B. et al. (1995) Mutations in the cystic fibrosis gene in patients with congenital absence of the vas deferens. N. Engl. J. Med., 332, 1475-1480. De Braekeleer, M. and Dao, T.N. (1991) Cytogenetic studies in male infertility: a review. Hum. Reprod., 6, 245. Edwards, R.G. and Bishop, C.E. (1997) On the origin and frequency of Y chromosome deletions responsible for severe male infertility. Mol. Hum. Reprod., 3, 549-554. Engel, W. and Schmidt, M. (1995) Gibt es genetische Risiken der mikroassistierten Reproduktion? Fertilitat, 11, 214-228. Ferguson-Smith, M.A., Lennox, B., Mack, W.S. et al. (1957) Klinefelter's syndrome: frequency and testicular morphology in relation to nuclear sex. Lancet, ii, 167. Foresta, C , Ferlin, A., Garolla, A. et al. (1997) Y-chromosome deletions in idiopathic severe testiculopathies. J. Cell. Embryol. Morphol, 82, 1075-1080. Foss, G.L. and Lewis, FJ.W. (1971) A study of four cases with Klinefelter's syndrome, showing mobile spermatozoa in their ejaculates. /. Reprod. Fertil., 25, 401^408. Girardi, S.K., Mielnik, A. and Schlegel, P.N. (1997) Submicroscopic deletions in the Y chromosome of infertile men. Hum. Reprod., 12, 1635-1641. Giwercman, Y.L, Xu, C , Arver, S. et al. (1998) No association between the androgen receptor gene CAG repeat and impaired sperm production in Swedish men. Clin. Genet., 54, 435^-36. Gooren, L. (1989) Improvement of spermatogenesis after treatment with the antiestrogen tamoxifen in a man with incomplete androgen insensitivity syndrome. J. Clin. Endocrinol. Metab., 68, 1207-1210. Gordon, D.L., Krmpotic, E., Thomas, W. et al. (1972) Pathologic testicular findings in Klinefelter's syndrome. Arch. Intern. Med., 139, 726. Gottlieb, B., Lehvaslaiho, H., Beitel, L.K. et al. (1998) The androgen receptor gene mutation database. Nucleic Acids Res., 26, 234-238. Hiort, O., Sinnecker, G.H.G., Holterhus, P.M. et al. (1996) The clinical and molecular spectrum of androgen insensitivity. Am. J. Med. Genet., 63, 218-222. Jacobs, PA. and Strong, J.A. (1959) A case of human intersexuality having a possible XXY sexdetermining mechanism. Nature, 183, 302-303. Kent-First, M.G., Kol, S., Muallem, A. et al. (1996) The incidence and possible relevance of Ylinked microdeletions in babies born after intracytoplasmic sperm injection and their infertile fathers. Mol. Hum. Reprod., 2, 943-950. Kerem, B.S., Rommens, J.M., Buchanan, J.A. et al. (1989) Identification of the cystic fibrosis gene: genetic analysis. Science, 245, 1073. Kobayashi, K., Mizuno, K., Hida, A. et al. (1994) PCR analysis of the Y chromosome long arm in azoospermic patients: evidence for a second locus required for spermatogenesis. Hum. Mol. Genet., 3, 1965-1967. Kremer, J.A.M., Tuerlings, J.H.A.M., Meulemans, E.J.H. et al. (1997) Microdeletions of the Y chromosome and intracytoplasmic sperm injection: from gene to clinic. Hum. Reprod., 12, 687-691. Lahn, B.T. and Page, D. C. (1997) Functional coherence of the human Y chromosome. Science, 278, 675-680. LeLannou, D., Jezequel, P., Blayau, M. et al. (1995) Obstructive azoospermia with agenesis of vas deferens or with bronchiectasia (Young's syndrome): a genetic approach. Hum. Reprod., 10, 338. Ludwig, M., Kiipker, W., Hahn, K. et al. (1998) Klinische Bedeutung Y chromosomaler Mikrodeletionen im Rahmen reproduktionsgenetischer Routinediagnostik bei schwerer mannlicher Subfertilitat. Geburtsh. u. Frauenheilk., 58, 73-78. Ma, K., Inglis, J.D., Sharkey, A. et al. (1993) A Y chromosome gene family with RNA-binding protein homology: candidates for the azoospermia factor AZF controlling human spermatogenesis. Cell, 75, 1287. Martin, R.H., Ko, E. and Hildebrand, J. (1992) Analysis of sperm chromosome complements from a man heterozygous for a Robertsonian translocation 45, XY t(15q22q). Am. J. Med. Genet., 43, 855-857. 35 W.Kiipker et al. Martini, E., Geraedts, J.P.M:, Liebaers, I. et al. (1996) Constitution of semen samples from XYY and XXY males as analysed by in-situ hybridisation. Hum. Reprod., 11, 1638. McElreavey, K., Barbaux, S., Bourgeron, T. et al. (1997) Mutation screening of the long arm of the human Y chromosome, including the Y-linked DAZ gene family, and the autosomal gene DAZLA in infertile men. Abstract. Cytogenet. Cell Genet., 79, 1-20. Nagafuchi, S., Namiki, M., Nakahori, Y. et al. (1993) A minute deletion of the Y chromosome in men with azoospermia. J. Urol. USA, 150, 1155-1157. Najmabadi, H., Huang, V., Yen, P. et al. (1996) Substantial prevalence of microdeletions of the Ychromosome in infertile men with idiopathic azoospermia and oligozoospermia detected using a sequence-tagged-site-based mapping strategy. J. Cell. Embryol. Morphol., 81, 1347-1352. Nakahori, Y, Kuroki, Y Komaki, R. et al. (1996) The Y chromosome region essential for spermatogenesis. Horm. Res., 46, 20-23. Patrizio, P. and Asch, R.H. (1994) The relationship between congenital absence of the vas deferens (CBAVD), cystic fibrosis (CF) mutations, and epididymal sperm. Assist. Reprod. Rev., 4, 95-100. Pellestor, R., Sele, B. and Jalbert, H. (1987) Chromosome analysis of spermatozoa from a male heterozygous for a 13; 14 Robertsonian translocation. Hum. Genet., 76, 116-120. Pryor, J.L., Kent-First, M.G., Muallem, A. et al. (1997) Microdeletions in the Y chromosome of infertile men. N. Engl. J. Med., 336, 534-539. Qureshi, S.J., Ross, A.R., Ma, K. et al. (1996) Polymerase chain reaction screening for Y chromosome microdeletions: a first step towards the diagnosis of genetically-determined spermatogenic failure in men. Mol. Hum. Reprod., 2, 775-779. Reijo, R., Lee, T.L., Salo, P. et al. (1995) Diverse spermatogenic defects in humans caused by Y chromosome deletions encompassing a novel RNA-binding protein gene. Nature Genet., 10, 383. Reijo, R., Alagappan, R.K., Patrizio, P. et al. (1996) Severe oligozoospermia resulting from deletions of azoospermia factor gene on Y chromosome. Lancet, 347, 1290-1293. Shkolny, D.L., Beitel, L.K., Ginsberg, J. et al. (1999) Discordant measures of androgen-binding kinetics in two mutant androgen receptors causing mild or partial androgen insensitivity, respectively. J. Clin. Endocrinol. Metab., 84, 805-810. Simoni, M., Gromoll, J., Dworniczak, J. et al. (1997) Screening for deletions of the Y chromosome involving the DAZ (Deleted in Azoospermia) gene in azoospermia and severe oligozoospermia. Fertil. Steril., 67, 542-547. Stuppia, L., Mastroprimiano, G. and Calabrese, G. (1996) Microdeletions in interval 6 of the Y chromosome detected by STS-PCR in 6 of 33 patients with idiopathic oligo- or azoospermia. Abstract. Cytogenet. Cell Genet., 72, 155-158. Stuppia, L., Calabrese, G., Gatta, V. et al. (1997) Microdeletions of the Y chromosome in oligozoospermic patients are clustered in the subinterval E of interval 6 and do not involve the DAZ gene: evidence for an oligozoospermia specific locus. Cytogenet. Cell Genet., 79, 1-20. Syme, R.M. and Martin, R.H. (1992) Meiotic segregation of a 21;22 Robertsonian translocation. Hum. Reprod., 7, 825-882. Tesarik, J., Guido, M., Mendoza, C. and Greco, E. (1998) Human spermatogenesis in vitro: respective effects of follicle-stimulating hormone and testosterone on meiosis, spermiogenesis, and sertoli cell apoptosis. J. Clin. Endocrinol. Metab., 83, 4467-4473. Tiepolo, L. and Zuffardi, O. (1976) Localization of factors controlling spermatogenesis in the nonfluorescent portion of the human Y chromosome long arm. Hum. Genet., 34, 119-124. Tournaye, H., Staessen, C , Liebaers, I. et al. (1996) Testicular sperm recovery in nine 47, XXY Klinefelter patients. Hum. Reprod., 11, 1644. Tsukada, T., Inoue, M., Tachibana, S. et al. (1994) An androgen receptor mutation causing androgen resistance in undervirilized male syndrome. J. Clin. Endocrinol. Metab., 79, 1202-1207. Tut, T.G., Ghadessy, F.J., Trifiro, M.A. et al. (1997) Long polyglutamine tracts in the androgen receptor are associated with reduced trans-activation, impaired sperm production, and male infertility. J. Clin. Endocrinol. Metab., 82, 3777-3782. Van der Ven, K., Montag, M., Peschka, B. et al. (1997) Combined cytogenetic and Y chromosome microdeletion screening in males undergoing intracytoplasmic sperm injection. Mol. Hum. Reprod., 3, 699-704. 36 Clinical work-up for male subfertility Vogt, P.H. (1997) Human Y chromosome deletions in Yqll and male fertility. In Ivell, R. and Holstein, A.-F. (eds), The Fate of the Male Germ Cell, Advances in Experimental Medicine and Biology. Plenum Press, New York, pp. 17-30. Vogt, P.H. (1998) Human chromosome deletions in Yqll, AZF candidate genes and male infertility: history and update. Mol. Hum. Reprod., 4, 739-744. Vogt, P.H, Edelmann, A., Kirsch, S. et al. (1996) Human Y chromosome azoospermia factor (AZF) mapped to different subregions in Yqll. Hum. Mol. Genet., 5, 933-943. Vogt, PH., Affara, N. Davey, P. et al. (1997) Report of the third international Workshop on Y chromosome mapping 1997. Cytogenet. Cell Genet., 79, 10-20. Vollrath, D., Foote, S., Hilton, A. et al. (1992) The human Y chromosome: a 43-interval map based on naturally occurring deletions. Science, 258, 52-59. Wang, Q,, Ghadessy, FJ., Trounson, A, et al. (1998a) Azoospermia associated with a mutation in the ligand-binding domain of an androgen receptor displaying normal ligand binding, but defective trans-activation. J. Clin. Endocrinol. Metab., 83, 4303-4309. Wang, Q., Ghadessy, F.J., Yong, E.L. (1998b) Analysis of the transactivation domain of the androgen receptor in patients with male infertility. Clin. Genet., 54, 185-192. Yong, E.L., Ng, S.C., Roy, A.C. et al. (1994) Pregnancy after hromonal correction of severe spermatogenetic defect due to mutation in androgen receptor gene. Lancet, 344, 826-827. Yoshida, A., Tamayama, T., Nagao, K. et al. (1995) A'cytogenetic survey of 1007 infertile males. Contracept. Fertil. Sex., 23, 103a. Zuffardi, O. and Tiepolo, L. (1982) Frequencies and types of chromosome abnormalities associated with human male infertility. In Crosignani, P.G. and Rubsin, B.L. (eds), Genetic Control of Gamete Production and Function. Serono clinical Colloquia on Reproduction. HI. Academic Press/Grune and Stratton, London, pp. 261-273. 37