Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Primary transcript wikipedia , lookup
Gene therapy wikipedia , lookup
Genomic library wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
History of genetic engineering wikipedia , lookup
Molecular cloning wikipedia , lookup
Viral phylodynamics wikipedia , lookup
Genome editing wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
SNP genotyping wikipedia , lookup
Microevolution wikipedia , lookup
Microsatellite wikipedia , lookup
Deoxyribozyme wikipedia , lookup
Designer baby wikipedia , lookup
Helitron (biology) wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Bisulfite sequencing wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
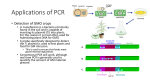
SOMC Overview and Future Directions SOMC Grand Rounds January 8, 2016 Timothy R. Cassity, Ph. D. Microbiologist The opinions expressed in this presentation are those of the presenter. The material presented here does not necessarily reflect the views of Southern Ohio Medical Center. The presenter has no financial interest in (i.e. is not being paid by) any diagnostic testing company or pharmaceutical company or product that may be mentioned in this presentation. Due to the nature of the topic, some slides may seem like an “infomercial.” I apologize in advance! Understand the advantages of molecular methods over traditional diagnostic microbiology tests. Identify situations where molecular methods are not beneficial. Understand problems and limitations that can occur with molecular methods of detecting etiologic agents. The level of molecular testing offered at SOMC would not be possible without the support of Bridget Scott (Lab Administrative Direct) and Dr. Vincent Randaisi (Lab Medical Director) and the SOMC Administration! I would also like to express my appreciation to the physicians who have supported and championed molecular technology, and Dr. David Byers and Dr. Elie Saab in particular. I would like to acknowledge the invaluable guidance of Dr. Darren Adams in the design and implementation of the targets used by our OB/GYN providers. What is “molecular diagnostic testing” in infectious diseases? Detection of etiologic agents of infectious disease by detecting a unique nucleic acid base sequence for specific organisms. The “goal” of molecular testing is no different from classical methods. What is “molecular diagnostic testing” in infectious diseases? Every living organism (and some that aren’t living) are defined by the nucleotide base sequences on their DNA or RNA. For our purposes, each unique DNA or RNA sequence is loosely defined as a “target.” What is PCR? Polymerase Chain Reaction It is the in vitro synthesis of strands of target DNA base sequences directed by homologous primers. There are many other methods of “amplifying” DNA, but I will use the term PCR to include all of those. What is PCR? There are many other methods of “amplifying” DNA, but I will use the term PCR to include all of those. At SOMC we also use: ▪ ▪ ▪ ▪ ▪ Strand Displacement Amplification Loop-Mediated isothermal DNA amplification (LAMP) Gold Nanoparticle-based Methods (Verigene) RotorGene Q 5 channel in house developed PCR Alere™ i isothermal nucleic acid amplification What is DNA Amplification? It is the in vitro synthesis of strands of target DNA base sequences directed by homologous primers producing amplicons. What is DNA Amplification? We do the same thing with a culture, but with a culture we “amplify” by growing individual bacterial cells to a colony that we can easily detect visually. DNA amplification is a lot faster than growth! Note: Product of an artistic tech with too much time on her hands What is multiplexing? Multiplexing is the detection of multiple gene targets at the same time or on the same run. ▪ Respiratory Virus detects 17 targets simultaneously ▪ Blood culture detected 12-15 targets simultaneously ▪ HSV 1 & 2, Trichomonas vaginalis, Atopobium vaginae, Gardnerella vaginalis, Candida albicans and Candida glabrata are multiplexed. What is RT-PCR? RT-PCR stands for “Reverse Transcriptase Polymerase Chain Reaction It is used with RNA, such as with RNA-containing viruses, like influenza, RSV, HCV Reverse transcriptase is first used to convert RNA to DNA, then the DNA is amplified via conventional PCR What is “Real Time” PCR or molecular detection? In “classical” PCR, amplification took place in a thermocycler and detection in a separate instrument. Real time combines amplification and detection into one process. This is faster and less hands on than classical PCR What is qPCR or qRT-PCR? The “q” refers to “quantitative” When we run a real time PCR, we generate a cycling time. i.e. the number of cycles of amplification it takes before the target is detected. The number of cycles it takes to detect a target is dependent on the number of targets present in the original sample. What is qPCR or qRT-PCR? By measuring the number of cycles on samples of known concentration, a standard curve can be set up. To determine the quantity of targets in the initial sample, the number of cycles is compared to the standard curve. Magic? Nay, Nay! Steps to conventional real-time PCR Extraction Amplification and Detection ▪ Confirmation with DNA melt curve Data analysis ▪ Would not be possible without a computer. One of the instruments we use takes 4,320 data readings a minute – approximately 800,000 data points a run Nucleic Acid Extraction Lyses cells and releases nucleic acids Proteases are incorporated to inactivate nucleases and other enzymes Result is purified RNA and DNA Amplification and Detection Done via thermocycling To confirm ID (i.e. increase specificity) a DNA melt temp curve is run The Perfect Lab test would have 100% sensitivity (No false negatives) and 100% specificity (No false Positives) Much more sensitive (i.e. few false negative tests) than most conventional diagnostic methods used with infectious agents. Example – only method acceptable for the detection of HSV in CSF Analogy – if PCR could be used to detect sugar, you could drop 2 sugar cubes into Lake Michigan and detect it in Lake Michigan water. Target Organism Molecular Method Conventional Method LoD Molecular LoD Conventional Influenza A & B PCR Viral Culture 10-50 PFU/ml 1,000 PFU/ml Influenza A & B Alere-i Viral Culture 1,000 PFU/ml 1,000 PFU/ml HSV-1 or 2 PCR Viral Culture 5 - 15 PFU/ml 500-1,000 PFU/ml 4 cells/ml 1,000 cells/ml Trichomonas PCR Wet Prep CMV PCR Viral culture 100 PFU/ml 1,000 PFU/ml N. gonorrhoeae Strand Disp Culture 50 CFU/ml 100 CFU/ml Cl. difficile LAMP Toxin Detect 30% more sens than toxin testing B. pertussis Nanopart Culture >70% more sens than culture 40% more sens than wet prep If performed properly, specificity is also excellent! Few false positive results, but some are still possible Target Organism Molecular Method Conventional Method % Specificity Molecular % Specificity Conventional Influenza A & B PCR Viral Culture 100% 100% Influenza A & B Alere-i Viral Culture 97% 100% HSV-1 or 2 PCR Viral Culture 99% 100% Trichomonas PCR Wet Prep 100% 90% CMV PCR Viral culture 100% 100% N. gonorrhoeae Strand Disp Culture 98% 100% Cl. difficile LAMP Toxin Detect B. pertussis Nanopart Culture 95% (symptom) 95% 95% 100% Specimens Except for GBS, which has an enrichment step, molecular testing does not require viable organisms. Can use viral swabs, ThinPrep, some dry swabs, refrigerated CSF and sterile fluids Can be used in patients that have antibiotic therapy before clinical sample collection. Specimen transport is not as important as with conventional culture Molecular methods are particularly well adapted for diagnosis of infections caused by fastidious and uncultivable bacterial species. Beneficial for slow-growing organisms Target Organism Molecular Method Conventional Method Min TAT Molecular Min TAT Conventional Influenza A & B PCR Viral Culture 4 hours 1-2 days Influenza A & B Alere-i Viral Culture 20 min 1-2 days HSV-1 or 2 PCR Viral Culture 4 hours 1 – 2 days Trichomonas PCR Wet Prep 4 hours 20 min CMV PCR Viral culture 4 hours 1 – 4 days N. gonorrhoeae Strand Disp Culture 3 hours 3 days Cl. difficile LAMP Toxin Detect 1 hour 1 hour B. pertussis Nanopart Culture 2 hours 5 days RSV Nanopart Virus Culture 2 hours 2-4 days In many cases, with blood cultures, rapid detection of resistance genes influence initial treatment. Example: E. coli with ESBL or CRE Rapid results may permit discontinuance or de-escalation of antibiotics earlier than conventional culture. Can be an important part of antibiotic stewardship Can decrease length of stay Several studies have shown positive blood cultures identified by molecular detection average a 1.2 day shorter length of stay Too sensitive in some cases – can yield falsepositive results Example: C. difficile molecular detection Tests should be performed only on symptomatic patients PCR results must be correlated with clinical presentation and patient history The biggest potential problem with PCRbased tests is amplicon contamination. Samples cannot be handled in the same area they are amplified Instruments and the environment must be “disinfected” after every use! PCR tests cannot accurately differentiate infection from commensalism or chronic carriage Not good for opportunistic pathogens and for clinical specimens collected at nonsterile sites. Genetic Drift Genomes are not necessarily static If your target sequence changes in an organism you can no longer detect it! ▪ Example – Staphylococcus aureus and mecA gene cassette ▪ Some organisms such as Streptococcus sp. do not show much genetic change. Others, like influenza viruses, show genetic change more often There are methods to detect some genes responsible for resistance, such as mecA, some ESBLs, and some CREs. However, there are many more that we cannot test, or don’t even know about. Therefore, for organisms that can have variable susceptibility to antibiotics, culture and conventional susceptibility testing is still necessary. Molecular-based diagnostics are much more expensive than convention culture or antigen testing! But for now, reimbursement is very good! Laboratory Cost Medicare Reimbursement Influenza A & B – Alere-i $42 $96 HSV 1 & 2 $26 $96 Chlamydia/GC $20 $90 Respiratory panel – complete panel $110 $376 C. difficile $29 $48 GBS $33 $59 Atopobium/Gardnerella $46 $96 Candida albicans/C. glabrata $46 $96 Bordetella pertussis group $42 $141 Test Currently we have molecular tests for 58 infectious disease targets! 15 Gram positive blood culture targets 14 Gram negative blood culture targets 18 Respiratory virus and pertussis targets 10 STD and OB/GYN targets 1 GI target (C. difficile), with 10 more under development Positive Blood Culture on the BacT/Alert Subculture to plates and incubate Prepare and stain Gram stain Read and report Gram stain Call provider & clinical Pharmacist per protocol Has patient been admitted to SOMC – not expired? Yes No No Do not perform molecular ID Workup and Report from plates Call provider & clinical Pharmacist per protocol with Result First POS Blood culture? Yes Perform molecular ID & Workup and Report from plates Organism Gene Target Staphylococcus aureus S. aureus gyrB gene Staphylococcus epidermidis Staph epi hsp60 gene Staphylococcus lugdunensis Staph lugdunensis sodA gene Streptococcus agalactiae Strep agalactiae hsp60 gene Streptococcus anginosus group Strep anginosus gyrB gene Streptococcus pneumoniae Strep pneumoniae gyrB gene Streptococcus pyogenes Strep pyogenes hsp60 gene Enterococcus faecalis Enterococcus faecalis hsp60 gene Enterococcus faecium Enterococcus faecium hsp60 gene Staphylococcus sp. Staphylococcus sp tuf gene Streptococcus spp. Streptococcus tuf gene Listeria sp. Listeria sp. tuf gene mecA mecA gene vanA vanA gene vanB vanB gene Bacterial Genera and Species Acinetobacter spp. Citrobacter spp. Enterobacter spp. Proteus spp. Escherichia coli1 Klebsiella pneumoniae Klebsiella oxytoca Pseudomonas aeruginosa Resistance Markers CTX-M (blaCTX-M) KPC (blaKPC) NDM (blaNDM) VIM (blaVIM) IMP (blaIMP) OXA (blaOXA) Organism/Target Method Viable Specimen Needed? Chlamydia trachomatis Strand Displacement Amplification No Neisseria gonorrhoeae Strand Displacement Amplification No Group B Streptococcus Loop-Mediated Amplification following Enrichment in LIM broth YES Herpes Simplex 1 & 2 Conventional real-time PCR No Trichomonas vaginalis Conventional real-time PCR No Atopobium vaginae Conventional real-time PCR No Candida albicans Conventional real-time PCR No Gardnerella vaginalis Conventional real-time PCR No Candida glabrata Conventional real-time PCR No Typically Ordered by Groups, but can be ordered individually if desired. Groups include: Complete panel (12 targets) Influenza A & B (2 to 4 targets) RSV only (2 targets) Bordetella pertussis (3 targets) Can be customized per provider request Influenza A & B – Rapid Method – Alere-i Two targets – influenza A & influenza B Done on a dry swab or viral swab in UTM Requires approximately 20 min to perform Unlike rapid antigen tests, it does not require PCR or culture backup CLIA-waived, suitable for point of care Influenza A & B – Verigene Done on a variety of specimens – swab in UTM or other transport medium, BAL, Bronch Wash Four targets Gives H-type ID (ex. Influenza A H1) Can be done in about 2.5 hours >10X more sensitive than the Alere-i Influenza A & B – Conventional RT-PCR Done on a variety of specimens – swab in UTM or other transport medium, BAL, Bronch Wash Two targets – influenza A & influenza B Most sensitive method – LoD < 50 PFU Can be done in about 4.5 hours More labor-intensive – we do not do this much anymore. Used only as backup or to resolve questionable results. RSV (only) – Done on the Verigene Done on a variety of specimens – swab in UTM or other transport medium, BAL, Bronch Wash Two targets (RSV A & RSV B) Can be done in about 2.5 hours More sensitive than rapid antigen tests Can be done on adult patients as well as children Common Respiratory Viruses Comprehensive Panel that includes: ▪ Influenza A & B, with influenza A H subtypes ▪ RSV A & RSV B ▪ Parainfluenza 1, 2, 3 & 4 ▪ Human metapneumovirus ▪ Adenovirus ▪ Rhinovirus (it’s free so we throw it in for good measure) Bordetella pertussis panel Include B. pertussis, B. holmesii, and B. parapertussis/B. bronchiseptica Should be used only with symptomatic patients Used to diagnose whooping cough type illnesses HSV and CMV These can also be ordered on respiratory tract specimens. More relevant in immunosuppressed patients than immunocompetent ones HSV-1 found in around 30-40% of specimens, but most are not clinically significant These were routinely done with viral cultures Currently, only C. difficile is offered Very sensitive - can detect asymptomatic carriage – must be performed only on symptomatic patients 30% more sensitive than toxin testing – only 1 specimen needed to rule out C. difficile Molecular replacement for stool culture under development – Spring 2016 Stool culture TAT – 48 – 72 hours Molecular enteric pathogen TAT – 3 hours Expanded spectrum of etiologic agents Disadvantages Stool culture for susceptibility testing will be needed if Shigella sp. (and some Salmonella sp.) are found. Targets will include: Bacteria Toxins Viruses Campylobacter Group Shiga Toxin 1 (stx1) Norovirus Salmonella spp. Shiga Toxin 2 (stx2) Rotavirus Shigella spp. Vibrio Group Yersinia enterocolitica Infectious Agents GI pathogens – estimated Spring, 2016 Ureaplasma urealyticum HPV Mycoplasma genitalium (maybe) Non-infectious targets BRAF Mutation Analysis EGFR (Epidermal Growth Factor Receptor) JAK 2 (Janus Kinase 2) KRAS mutation (Kirsten rat sarcoma viral oncogene homolog)