Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biology and sexual orientation wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
X-inactivation wikipedia , lookup
Long non-coding RNA wikipedia , lookup
Pathogenomics wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
History of genetic engineering wikipedia , lookup
Ridge (biology) wikipedia , lookup
Oncogenomics wikipedia , lookup
Minimal genome wikipedia , lookup
Genome evolution wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Public health genomics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Gene expression programming wikipedia , lookup
Microevolution wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Gene expression profiling wikipedia , lookup
Designer baby wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Genome (book) wikipedia , lookup
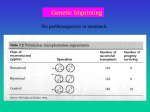
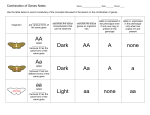
Genomic Conflicts, Health and Disease (1) What are genomic conflicts and how are they involved in health and disease? (2) Main forms of genomic conflict (a) Parent-offspring conflict (b) Genomic-imprinting conflict (c) Sexual conflict The logic & dynamics of genomic evolutionary conflict, in relation to health and disease Frank & Crespi 2011, PNAS (a) Parent-offspring conflict is due to higher relatedness to self/own offspring than to sib/nieces, nephews r = 1/2 r = 1/4 Autosomes: Parent-offspring conflict Parents value offspring equally. Each offspring values itself 2 times more than it values its sibling. Parents will prefer an equitable distribution of parental investment. Offspring will prefer an inequitable distribution of parental investment, with more to self Conflict begins in the womb. X chromosome alleles? Y chromosome alleles? Mom maximizes her inclusive fitness at a lower level of maternal investment than the level that maximizes inclusive fitness for any one offspring Mom Kid Selection for alleles in mom ‘for’ MAIN STAGES OF CONFLICT: adaptations that constrain (1) Survival of conceptus investment (2) Growth in the womb (3) Survival at birth Selection of alleles in offspring (4) Investment in childhood ‘for’ adaptations to take more (5) Inheritance as adult from mom, to the point that negative effects on other sibs Strategies (variation) available? are not too great Mother-offspring conflict example Mother has 100 units to invest in kids Three kids to invest in: Options A 33 33 33 B 50 50 0 C 100 0 0 KIDS 1 2 3 Mothers fitness A 3(.5) = 1.5* B 2(.7) = 1.4 C 1(.9) = 0.9 Units->Survival 33->.5 50->.7 100->.9 Offspring 1’ s fitness 0.5 + 2(.5)(.5)=1.0 0.7 + 1(.5)(.7)=1.05* 0.9 + 0(.5)(0.9)=0.9 Conflict can exist over (1) whether or not to ‘miscarry’ (2) invasiveness of the placenta (3) the nutrient quality of maternal blood -> blood glucose (4) the volume of blood reaching the placenta -> blood pressure Maternal provisioning of a fetus is associated with an ‘opportunity cost’ The opportunity cost translates into lower expected fitness through other offspring If extra resources are transferred to a given embryo (you) -> the embryo’s (your ) expected fitness increases -> the mother’s expected fitness via other offspring decreases TRADEOFF between current & future reproduction Conceptus @ 9 days old Manifestations of maternal-fetal conflict Spontaneous abortion - Should mom maintain the pregnancy? Depends on the quality of the fetus and state of the mother. These hinge on cost/benefit issues in relation to possible future pregnancies. AND WHO is in CONTROL of what? POSSIBILITIES (1) Mother and baby Both ‘want’ pregnancy maintained (2) Baby ‘wants’ pregnancy maintained, mother does not CONFLICT (3) Neither ‘wants’ pregnancy maintained - WHY? WHEN? What is a conceptus to do? Shout that they are here and ‘take over’ the system that maintains pregnancy as rapidly as possible Pregnancy is maintained via the production of LH and LH’s stimulation of progesterone anterior pituitary (P) production. luteinizing hormone Temporary endocrine corpus luteum structure, from ovarian follicle progesterone uterus hCG bypasses this pathway and stimulates the corpus luteum to produce progesterone and by the 8th week of pregnancy, anterior pituitary produces enough P to sustain pregnancy luteinizing hormone on its own. human chorionic gonadotropin placenta corpus luteum progesterone uterus hCG bypasses this pathway and stimulates the corpus luteum to produce progesterone anterior pituitary and by the 8th week of pregnancy, luteinizing hormone produces enough progesterone to sustain pregnancy on its own. chorionic gonadotropin placenta progesterone corpus luteum progesterone uterus Conflicts over food for the growing fetus: (1) Invasion of the placenta into the uterine wall. Allows fetus to prevent cutoff of blood flow (modify spiral arteries), access matermal blood efficiently. Disruption of the conflict system: pre-eclampsia (2) Fast food for baby - amount of food depends on glucose levels in maternal blood - you want more than mom wants to give you. Insulin keeps blood sugar from getting dangerously high. hPL (placental lactogen) blocks (bonds) maternal insulin. Disruption of the conflict system: gestational diabetes (3) More blood please! Amount of food also depends on maternal blood pressure - you want mom’s blood pressure to be higher Disruption of the conflict system: pre-eclampsia “The border zone … is not a sharp line, for it is in truth the fighting line where the conflict between the maternal cells and the invading trophoderm takes place, and it is strewn with such of the dead on both sides as have not already been carried off the field or otherwise disposed of.” Johnstone (May 1914) Journal of Obstetrics and Gynaecology of the British Empire 25: 231 MAIN STAGES OF PARENT-OFFSPRING CONFLICT: (1) Survival of conceptus (2) Growth in the womb (3) Survival at birth - infanticide and baby fatness, cuteness (4) Investment in childhood lactational amenorrhea, weaning, tantrums, language, learning (5) Inheritance as adult How parent-offspring conflicts contribute to disease (1) Disruption of ‘tugs-of-war’ over resources (mild gestational diabetes or preclampsia leads to a bigger, fatter baby but severe cases endanger the life of both mother and fetus) (2) Wastes of resources (release of compounds by placenta that are ‘ignored’ by mother - hormonal ‘shouting’) (3) Maladaptations in party that ‘loses’ in a conflict (mother ‘stuck’ with pregnancy, fetus takes fatty acids direct from mom’s brain, fetus controls parturition time) (4) Within-family ongoing verbal, physical conflicts and psychological health and well-being Genomic Conflicts, Health and Disease (1) What are genomic conflicts and how are they involved in disease? (2) Main forms of genomic conflict (a) Parent-offspring conflict (b) Genomic-imprinting conflict from dad What is genomic imprinting and why has it evolved? Expression of a gene depending on whether inherited from father or mother Main arenas of imprinting effects on human health: -Placenta -Brain -Carcinogenesis -Stem cells -In vitro fertilization from mom Imprinted gene expression compared to biallelic gene expression How imprinting works, across the life cycle Why imprinting has evolved, in placental mammals: Asymmetries in parental investment are high • the mother alone gestates and lactates • all her children have 50% of her genes • the father contributes only a single sperm • mixed paternity is common across births or broods Evolution of genomic imprinting in placental mammals under multiple paternity and high maternal investment: Paternal gene Relatedness of paternal gene in offspring, to siblings, goes from 0.5 to 0 as we go from monogamy to polygamy Maternal gene Relatedness of maternal gene in offspring, to siblings, is always 0.5 Paternally-expressed genes are expected to be more ‘selfish’, with regard to mother-offspring interactions Evolution of genomic imprinting in placental mammals under multiple paternity and high maternal investment: Paternal gene Relatedness of paternal gene in offspring, to siblings, goes from 0.5 to 0 as we go from monogamy to polygamy EXTREME CASE: Mum’s Brood Maternal gene Relatedness of maternal gene in offspring, to siblings, is always 0.5 IMPRINTED GENES (1) Silenced (‘imprinted’) when inherited from either the father or the mother (-> parent of origin effects) (2) Paternally-expressed (maternally-silenced) genes are expected to be associated with increased demands on the mother, by offspring (3) Maternally-expressed genes are expected to be associated with reduced demands on the mother ‘TUGS-OF-WAR’ can result (eg IGF-II/IGF-IIR in pregnancy) EXAMPLE: TUG-OF-WAR over fetal growth in pregnancy In fetus: IGF-II paternally expressed, IGF-IIR maternally expressed Paternally-expressed gene generates IGF-II, Maternally-expressed gene IGF-IIR serves as non-functional ‘sink’ that degrades IGF-II WITHIN A Fetal Mouse: Imprinted genes are ‘master regulators’ of placentation: they control growth and differentiation CONFLICT THEORY OF IMPRINTING -> abundant support from empirical studies of imprinted genes and growth, in mice and humans (1) IGF2-IGF2R (Haig & Graham 1991 Cell) (2) CDKN1C (Andrews et al. 2007 BMC Dev Biol) (3) GRB10 (Charalambous et al. 2003 PNAS) BeckwithWiedemann Syndrome 2 doses IGF2 Mighty mouse Normal sized human 1 dose IGF2 SilverRussell syndrome 0 doses IGF2 Effects of alterations to imprinted genes on the placenta in mice KNOCKOUTS * Dysregulation of imprinted genes in the placenta is an important cause of intra-uterine growth restriction (IUGR) in humans Imprinting Placentation Imprinting can cause genetic disorders, if both chromosomes are inherited from same parent IMPRINTED GENE EXPRESSION IN THE PLACENTA AND IN THE BRAIN About 100 imprinted genes are known, many more are predicted or apparent (need validation) Primary site of imprinted-gene expression is the (‘social’) placenta, which mediates the transfer of resources between mother and child Small deviations in placental function can benefit the child, or the mother Large deviations are costly to both The second-most important site of imprinted gene expression is the (‘social’) brain Imprinting & the brain ‘most imprinted genes will affect how much an offspring receives from its mother, at the expense of sibs. Thus imprinting is expected at loci that influence placental growth, suckling, neonatal behavior, appetite, nutrient metabolism and postnatal growth rate… it is worth considering the possibility that imprinting influences appetite control and hypothalamic function.’ After the placenta, genes are most-commonly imprinted in the brain Chimeric mouse brain The mother and the ‘maternal brain’ • is the prime nurturer • has equal number of genes in all her children (50%) • her genes ‘build’ the part of the brain that can be nurtured and exercise restraint: the neo-cortex The father and the ‘paternal brain’ • relies on his genes to control growth, development, and behaviour • other children in the family need not share his genes • his genes ‘build’ the limbic brain Paternally-expressed imprinted genes are especially commonly expressed in the hypothalamus, where they affect energy metabolism and other fundamental body functions (food, activity level, sex, sleep) Oppositely-imprinted disorders of the brain: Prader-Willi & Angelman syndromes • Angelman: paternal additions and/or maternal deletions on chromosome 15q1113 • Prader-Willi: maternal additions and/or paternal deletions on chromosome 15q11-13 Angelman Prader-Willi • • • • • prolonged suckling frequent crying hyper-active/sleepless low pleasure threshold severe retardation: no language • autism Every mother’s worst fear, as regards behaviour of a child • • • • • poor suckling weak crying inactive/sleepy high pain threshold affective psychosis in adults Complacent, easy on mom b) Genomic-imprinting conflict What is genomic imprinting and why has it evolved? Expression of a gene depending on whether inherited from father or mother Main arenas of imprinting effects on human health: -Placenta -Brain -Carcinogenesis -Stem cells -In vitro fertilization Imprinting and Cancer: Paternally-expressed imprinted genes enhance growth/proliferation; some are ‘oncogenes’ Maternally-expressed Imprinted genes constrain growth/proliferation; some are ‘tumor suppressors’ PNAS, 2003 Main mechanisms whereby alterations to imprinted genes promote cancer development BWS = BeckwithWiedemann syndrome Alterations to genomic imprinting alter the properties of embryonic stem cells Genomic Conflicts, Health and Disease (1) What are genomic conflicts and how are they involved in disease? (2) Main forms of genomic conflict (a) Parent-offspring conflict (b) Genomic-imprinting conflict (c) Sexual conflicts What is sexual conflict? • Stems ultimately from differential investment by males and females in reproduction (e.g. anisogamy) • Can lead to different optima in males and females for reproductive traits fitness females males trait value Both optima cannot simultaneously be realised = sexual conflict • Reinforced by - multiple breeding episodes with different partners (low shared interest in future reproductive bouts) - low relatedness of mating pairs (usually 0) Sexual conflict • Selection for adaptations that favour each sex reaching its optimum, despite the reduction in fitness this necessarily causes in the other sex • Followed by counter adaptation for ‘resistance’ => sexually antagonistic coevolution T. Chapman 2006, Curr. Biol. Relevence to human health? Think about these concepts when you think about sexual conflict One arena of conflict: male ejaculate chemicals AG T Internal Male Reproductive System T AG Accessory gland proteins (Acps) Accessory glands • SIMPLE PEPTIDES (<100 a/a) • HORMONE-LIKE (200-400 a/a) • LARGE GLYCOPROTEINS (>400 a/a) Effects of Acps Specific Acps: •increase egg production •decrease female receptivity after mating •stimulate feeding •essential for sperm storage •process other Acps •form a mating plug Several Acps: •increase success in sperm competition •have antibacterial activity Acps benefit males • Acps increase egg laying, sperm storage, success in sperm competition, and temporarily prevent females from mating again • in toto they act to increase male paternity, and therefore benefit males but Acps can reduce female fitness 1 0.9 Female survivorship 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 ------ Full Acps ------ No Acps Non-mating control (1) Non-mating control (2) 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 Time (days) (Chapman et al 1995) 33 35 Rapid evolution in reproductive proteins •At least 11% of Acps evolve rapidly e.g. Acp26Aa is fastest evolving gene in melanogaster genome (Ka/Ks ratios >1) •Significant polymorphism AND divergence •Also rapid evolution in female D. melanogaster reproductive tract proteins •Lack of homologues, even between close relatives •Recent evolution of Acp genes and high Acp gene turnover Acps’s in humans: the prostate • Unique to mammals, analogous to accessory glands in Drosophila • Function is production of seminal fluid • Consists of 30-50 sac-like glands connected to excretory ducts • Secretions play key roles in the fertilizing abilities of the spermatozoa in the female reproductive tract Prostate functional design and evolution are essentially unstudied • Is prostate size or form related to mating system, among primates and other animals, or among human races? • What are the functions of the various compounds secreted by the prostate and seminal vesicles? • Roles in human fertility, health? Growth, Differentiation and Human Sexual Dimorphism • Mediated by androgens • The main circulating androgen is testosterone (produced by Leydig cells of the testis) • Testosterone + 5α Reductase (enzyme) Dihydrotestosterone (DHT) This enzyme is specific to the prostate and liver * Androgens increase cell proliferation and inhibit apoptosis Role of DHT in the Prostate • Binds to androgen-receptor proteins • Gets transported into the nucleus • Initiates transcription of androgen dependent genes • Hence DHT controls the expression of many proteins of the seminal fluid Peptides and Proteins in Human Semen Heaps and heaps of compounds of unknown function, plus some known ones • PSA = Prostate Specific Antigen - A biomarker for prostate cancer - Protects the sperm of it’s male and slows the sperm of others • Semenogelin - Two types (I and II) - I- inhibits sperm motility and capacitation - Both involved in the human semen coagulum - Function in sperm competition in primates, evolves faster in primate species with multiple mating known ones • hCG human chorionic gonadotropin ! Evidence for adaptation in primate seminal proteins - though evidence of function is sparse Acps=accessory proteins (made in accessory glands) protein in Drosophila seminal fluids EFFECTS ON THE FEMALE in flies; what about in humanseffects on male and female? • Increase -oogenesis -egg hatchability -sperm storage -ovulation • Decrease -receptivity to remating -postmating viability -sperm loss -remating physically (are a component of the mating plug) Prostate Cancer • Involves a series of sequential mutations • Mutations inhibit apoptosis and drive cell proliferation • Is testosterone-dependent (at least initially); breast cancer is often estrogen-dependent • Progression is mediated by genetic variation in the androgen receptor gene • Killer # 2 after lung cancer, surgery causes impotence and incontinence • Most men get it if they live long enough; starts to develop in 20s - WHY? Hypothesis for the evolution of prostate cancer risk • Strong selection for compounds that enhance male reproductive function, even at a cost to females, and a cost to males, especially in terms of cancer risk * Seminal proteins evolve under sexual conflict - antagonistic coevolution between genome as expressed in males and genome as expressed in females - predicted to show expression patterns associated with cancer -> directly analogous to costs of Acp’s in flies -> one key gene involved in prostate function, and prostate cancer risk, is the androgen receptor Androgen Receptor: protein that ‘activates’ effects of testosterone. Extent of activation is mediated by number of CAG microsatellite repeats • MALES Lower number of repeats - increased activation of receptor and increased male fertility, but increased risk of prostate cancer Expect selection on males for fewer repeats (to a point) • FEMALES Lower number of repeats, higher rates of breast cancer This is Evidence for Sexual Conflict What about other prostate-expressed genes - does their expression, activity affect cancer risk? Main ways that sexual conflicts may be involved in disease: (1) Disruption of dynamic ‘tugs of war’ between parties in conflict over reproductive resources (as in parent - offspring, maternal genes-paternal genes, and males - females) (IGF2-IGF2R in pregnancy) (2) One party may ‘win’ a conflict, with costs imposed on the other party (hCG? androgen receptor?) (3) Strong selection and rapid evolution can result in maladaptive byproducts, whereby strong selection for one trait can result in maladaptation regarding other traits (seminal proteins? androgen receptor?) (4) Ongoing more or less direct physical, psychological conflicts, costly to one or both parties