Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
DNA supercoil wikipedia , lookup
Metagenomics wikipedia , lookup
Heritability of IQ wikipedia , lookup
Gene expression profiling wikipedia , lookup
Genealogical DNA test wikipedia , lookup
Pathogenomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Molecular Inversion Probe wikipedia , lookup
United Kingdom National DNA Database wikipedia , lookup
Extrachromosomal DNA wikipedia , lookup
Copy-number variation wikipedia , lookup
Molecular cloning wikipedia , lookup
Cre-Lox recombination wikipedia , lookup
Deoxyribozyme wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Genome evolution wikipedia , lookup
Oncogenomics wikipedia , lookup
Epigenomics wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Non-coding DNA wikipedia , lookup
Genome-wide association study wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Comparative genomic hybridization wikipedia , lookup
Public health genomics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Helitron (biology) wikipedia , lookup
Designer baby wikipedia , lookup
Point mutation wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Genomic library wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Microevolution wikipedia , lookup
Segmental Duplication on the Human Y Chromosome wikipedia , lookup
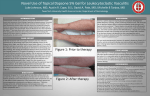
IMBALANCES WITHIN REGIONS CONTAINING LARGE-SCALE COPY-NUMBER VARIATIONS IN INDIVIDUALS WITH DEVELOPMENTAL ABNORMALITIES: WHEN DOES NORMAL BECOME ABNORMAL? Nelson, M., Pickering, D., Golden, D., Haskins Olney, A., Schaefer, G.B., Dave, B.J., Sanger, W.G. Munroe-Meyer Institute, University of Nebraska Medical Center, Omaha, NE Case 1: Clinical Report and Molecular Cytogenetic Findings Large-scale Copy-number Variations (LCV’s): What do we know so far? ¾ 3 ½ month old female previously seen in the newborn period for multiple congenital anomalies. ¾ Patient findings are strongly suggestive of CHARGE Association including congenital heart defects, coloboma and growth retardation. ¾ What are they? LCV’s are large segments of DNA, several to hundreds of kilobases in size, that vary severalfold in copy number between phenotypically normal individuals. ¾ How are they detected? LCV’s manifest themselves as duplication/loss in DNA microarray studies and/or as deletions in FISH studies. They may also be seen to a lesser extent as duplications in interphase FISH studies. Case 2: Clinical Report and Molecular Cytogenetic Findings ¾ Six year old male with developmental delays and moderate to severe bilateral neurosensory hearing loss. ¾ Family history negative for hearing loss or neurodevelopmental delays. ¾ High-resolution G-band studies revealed a 46,XY karyotype. ¾ Family history of a full brother who was stillborn with unknown etiology. ¾ How many are there? Estimates of greater than 200 LCV’s are present in the human population. This is based on limited population studies and may be an underestimation. ¾ High-resolution G-band studies revealed a 46,XX karyotype ¾ How common are they? On average, two individuals vary by 11 or more LCV’s, however less than 50% of the LCV’s currently described were identified in more than 1individual. ¾ Microarray analysis with the Spectral Genomics™ Constitutional Human BAC Array was normal. ¾ Where are they located? Greater than ½ of the polymorphic clones may overlap known coding regions and ¼ may encompass one or more complete genes. Several LCV’s have been identified near loci associated with cancer or genetic syndromes and are frequently in regions susceptible to rearrangement. ¾ Microarray analysis utilizing the Spectral Genomics™ 2600 BAC 1Mb Array confirmed a deletion of BAC clone CTB-31J3 at 4q35.2 (Figure 4) along with deletions at 1p36.33* and 22q13.33* and a duplication at 1p21. ¾ Subtelomeric FISH studies were normal. ¾ FISH studies utilizing a homebrew locus specific DNA probe revealed a deletion of the CHD7 gene at 8q12.2. Deletions of this gene have been associated with CHARGE. ¾ Microarray analysis utilizing the Spectral Genomics™ Constitutional Human BAC Array was normal. ¾ Microarray analysis with the Spectral Genomics™ 2600 BAC 1Mb Array confirmed a deletion at 8q12.2 but also revealed a duplication at 1q44 and 1p36.32-33* (Figure 1). A deletion at 5p14.3 and duplications at 14q12 and 22q13.33* were also present ¾ FISH studies utilizing homebrew loci specific DNA probes derived from the same clones found to be duplicated at 1q44 (RP11-407H12 and RP11-438F14) in the microarray study were positive for a duplication in approximately 1/3 of the interphase cells scored (Figure 2a and 2b). ¾ Microarray and FISH studies of the parental chromosomes revealed that the same 4qter deletion was present in the phenotypically unaffected father implying that this aberration has no pathogenic affect (Figure 3b) and revealed inheritance pattern of other suspected LCV regions. Database of Genomic Variants Supported by: ¾ Microaray and FISH studies of the parental chromosomes revealed the inheritance pattern of the suspected LCVs. ¾ Further investigation revealed that the clones duplicated at 1q44 (RP11-407H12 and RP11-438F14) and 14q12 (RP11125A5) have previously been reported as polymorphic clones located within a LCV region. The clone showing gain at 5p14.3 (RP11-88L18) to the best of our knowledge, however, is not within a reported LCV. Chromosome 1 profile from 1 Mb microarray Legend: A blue dot indicates a reported gain; A red dot indicates a reported loss; An orange dot indicates a reported inversion breakpoint; A green dot to the left of a region indicates that it overlaps with segmental duplication and/or is within 100k of a gap ¾ Mapping of the region with information gained by FISH and microarray has revealed a possible deletion size ranging from <400 bp to 40 kb. This region contains an autosomal dominant deafness gene, DFN24. The possibility of further molecular studies to determine if mutations/deletions of DFN24 are present in the proband are being considered (Figure 5). * The duplications or deletions at 1p36.33 (RP11-703E10) and 22q13.33 (CTD3018K1) observed in multiple individuals could not be resolved due to conflicting results. Chromosome 4 profile from 1 MB microarray LCV’s: What does it mean when they are observed in affected individuals? 703E10 Although LCV’s are considered normal genomic variants, the possible phenotypic consequences of all LCV’s has yet to be determined . ¾ Some LCV’s resulting in deletion may uncover recessive mutations resulting in phenotypic changes. ¾ Some LCV’s may have yet to manifest themselves in age-related susceptibilities. ¾ Some LCV’s may lead to further genetic alterations within adjacent regions. Figure 2a 407H12 438F14 Figure 1 ¾ Subtelomeric FISH studies with Vysis ToTel DNA FISH probe panel revealed a deletion of 4qter (Figure 3a). Figure 2b List of significant clones from 1 Mb microarray Clone Location DNA Copy Reported LCV RP11-407H12 1q44 Gain Yes RP11-438F14 1q44 Gain Yes RP11-88L18 5p14.3 Loss No RP11-91I20 8q12.1 Loss N/A RP11-125A5 14q12 Gain Yes Inherited Mother Mother Mother No Mother Conclusions about associations between LCV’s and phenotypic abnormalities should be approached cautiously. ¾ An aberration in a LCV region should be considered as a possibility for the patients’ malformation only if it has been observed in other patients with similar phenotypes or is associated with regions containing genes which may have contributed to the abnormal phenotype. ¾ Aberrations observed by either DNA microarray or subtelomeric FISH studies that have not been associated with a specific phenotype in other case studies or cannot be tied to a possible causative gene within that region may represent a previously unreported LCV region. ¾ Parental studies are necessary to help classify all possible LCV regions. To achieve optimal utilization of molecular cytogenetic techniques and to enhance our basic understanding of LCV’s it is of great importance to report cryptic aberrations thought to be genomic polymorphisms and this must be accumulated in a national database to allow clinical laboratories to accurately determine whether duplications or deletions, by these methods are clinically relevant. Figure 3a CTB-31J3 Figure 4 Figure 3b List of significant clones from 1 Mb and Constitutional microarray Clone Location DNA Copy Reported LCV Inherited RP11-259N12 1p21 Gain Yes Father RP11-354H17 4q35.2 Normal N/A N/A CTB-31J3 4q35.2 Loss Yes Father RP11-45F23 4q35.2 Normal N/A N/A 354H17 Figure 5 CTB-31J3 45F23 DFN24 (deafness gene)