Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biochemical cascade wikipedia , lookup
Cryobiology wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Oxidative phosphorylation wikipedia , lookup
Paracrine signalling wikipedia , lookup
Lactate dehydrogenase wikipedia , lookup
Adenosine triphosphate wikipedia , lookup
Phosphorylation wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
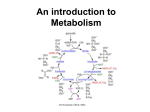
Citric acid cycle wikipedia , lookup
Biochemistry wikipedia , lookup
Block 1 Unit 2 Objectives Bone Tissue Objectives 1. List and describe all cell types, fibers, and components of the ECM of bone. a. Cells i. Osteocytes-mature bone cell. Are in lacunae surrounded by calcified ECM. Have cytoplasmic processes that extend through canaliculi and contact other osteocytes for communication and material transport ii. Osteoblasts-immature non dividing cells that actively lay new extracellular matrix. Simple cuboidal; basophilic iii. Osteoclasts-multinucleate cells (2-70) that release carbonic anhydrase to dissolve the mineral component of the ECM. Also release collagenase and hydrolase to dissolve the fibers of the ECM. Osteoclastic activity takes place on a specialized surface called the ruffled border and is contained by the sealing zone, which flanks the ruffled borders and is rich in integrins to seal the subosteoclastic compartments environment in. iv. Osteoprogenitor cells-unidentifiable cells that give rise to osteoblasts v. Bone Lining cells-cells that line all bone tissue. They are involved in stress sensing and they seal the bony tissue from the outside world (protect microenvironment) b. Fibers i. Type 1 Collagen c. Components i. Organic matrix 1. Low in proteoglycans therefore low in water content 2. Three predominant glycoproteins a. Osteonectin-bind osteocyte to extracellular matrix b. Osteocalcin-binds calcium to the ECM c. Bone Sialoprotein (Osteopontin)ii. Inorganic matrix 1. Hydroxyapetite Crystals 2. List and describe components of the organic and inorganic matrix a. Inorganic i. Hydroxyapetite protein b. Organic i. Type I Collagen ii. Osteonectin iii. Osteocalcin iv. Bone Sialoprotein 3. List and describe the individual components of bone 4. Identify and describe the structural and functional unit of the two types of bone a. Compact Bone i. Osteon b. Trabecular Bone i. Trabecular Packets 5. Describe the morphological organization of spongy and compact bone tissue a. Osteons are in compact bone tissue. They are concentric rings of osteocytes and surrounding ECM. There is a central canal that houses the blood vessel that delivers the nutrients to the osteocytes b. Trabecular packets are in Trabecular bone. They are composed of sheets of lamellar bone that arrange in a triangular pattern. They receive their nutrients through the marrow. 6. Vascular supply is achieved through Volkmann and Haversian Canals. The haversian canals are run through the osteons and are surrounded by concentric rings of osteocytes and extracellular matrix. The nutrients are diffused through the osteocytes by way of the cytoplasmic processes in the canaliculi. This limits the size of the osteons to .2mm in diameter. The vessels in the Volkmann canals supply the vessels in the haversian canals. They traverse osteons and bring in nutrient rich blood and export waste products. 7. Bone is quite vascularized through out the tissue. Cartilaginous tissue is avascular and relies wholly on diffusion. Through the extracellular matrix. Nutrients must difuse through the osteocytes, however this is much easier because of the cytoplasmic processes that are present bony tissue. 8. List and describe how different terminology is used to describe structure and function of bone tissue. 9. Bone has two major functions: Providing structure, and acting as a mineral reservoir. 10. Relate the morphology of bone with its function 11. List and describe the theories of mineralization a. Cellular Nucleation Theory i. Bits of cytoplasm pinch off in vesicles and secrete alkaline phosphatase. Alkaline Phosphatase cleaves pyrophosphate (PPi inhibits calcification, therefore inhibition of PPi would allow for calcification to initiate) b. Macromolecular nucleation Theory i. Multiple Macromolecules are involved 1. Collagen 2. Chondrocalcin a. Bind Calcium to ECM 3. Osteocalcin a. Bind Calcium to ECM 4. Sulfated Proteoglycans a. Releases Calcium needed for calcification 12. Define, describe and differentiate between the process of ossification, calcification and growth. a. Ossification I the overall process of bone formation. b. Calcification is the impregnation c. Bone Growth=Ossification 13. Describe the process of internal remodeling of bone and its structural basis. 14. Know when remodeling first starts and when its stops in the body. Understand how parathyroid hormone and calcitonin help control the internal remodeling process a. Parathyroid Hormone responds to Low Calcium and therefore will upregulate bone resorption. Binding sites are on the osteoblasts, which will then secrete Osteoclast Stimulating Factor. b. Calcitonin responds to High Calcium in the blood and will upregulate bone formation. Receptors are on the osteoclasts. 15. Describe the function of structural and metabolic bone. Be able to relate it to structures we see in bone 16. Know the relative Rates of bone tissue turnover. 17. Describe the morphology of trabeculae and their remodeling Cartilage Objectives 1. All three types of cartilage have some common characteristics. Chondrocytes are the main fixed cell in all three types of cartilage. They are large round cells that are randomly scattered through out the tissue. There is a large area of Extracellular matrix surrounding each cell. This ECM is AVASCULAR unlike bone, which is highly vascularized. All cartilage tissue is surrounded by a perichondrium. The difference between the three forms of cartilage lies in the most prevalent extracellular fiber. Hyaline Cartilage is characterized by predominantly Type II Collagen (Car-two-lage), which does not form fibrils with periodicity like its cousin, Type I collagen. Elastic Cartilage is predominantly formed with Elastic fibers. These must be visualized with a special stain (silver stain) to visualize the elastic fibers. Type II Collagen is also present, but not a much as elastic fibers. Elastic cartilage will appear like hyaline if not specially stained. Fibrocartilage is predominated by Type I collagen bundles. It will appear as if it is dense regular connective tissue, but the nuclei will be large and round. 2. Common Locations for Each Type a. Hyaline Cartilage is found in the costal cartilage, the trachea and bronchi (cartilaginous rings surrounding), larynx, nasal cartilage, the articular cartilage of the synovial joints is a specialized hyaline cartilage, and the fetal skeleton b. Elastic cartilage is found anywhere resilient support is needed, but elasticity and flexibility are also needed as in the pinna of the ear and the epiglottis c. Fibrocartilage is found where toughness and resistance is necessary but give is also needed. Three common locations are the pubic symphysis, the intervertebral discs, and junctions between bone and tendons 3. Cartilage develops when mesenchymal cells condense to form procartilage. The procartilage will secrete a cartilage matrix. 4. Integrate the characteristics of individual components of CT to the structure and function of Cartilage 5. Morphology fits function for the three types of cartilage. Hyaline cartilage is used as a lubricant and as such is high in proteoglycans and glycoproteins. These compounds attract water and therefore support against shock and compression. Elastic cartilage is used to have rigid support but a need for elasticity as in the pinna. For this reason, elastic cartilage has a lot of elastic fiber. Fibrocartilage is used to cushion and absorb impact. It must be rigid so it is full of Type I collagen. 6. List and describe how the three are classified based on prominent fiber a. Hyaline Cartilage is composed mainly of Type II Collagen b. Elastic Cartilages is predominantly Elastic Fibers c. Fibrocartilage is predominantly Type I Collagen Fibers 7. The perichondrium is the layer of tissue around the periphery of the cartilaginous tissue. It is divided into two layers, the fibrous layer and the chondrogenic layer. The fibrous layer is dense irregular connective tissue and contains all the blood vessels that provide the nutrients for cartilage. The chondrogenic layers is composed of cells from the fibrous layer that differentiate into chondroblasts that begin to secret extracellular matrix 8. Ground substance is amorphous; meaning is has no distinct shape. It is quite abundant in cartilage tissue and it is chock full of proteoglycans and glycoproteins. The proteoglycans present are predominantly chondroitin 4/6 sufate and karatan sulfate in the form of aggrecan. This aggrecan molecules form aggregates and are arranged around a hyaluronic acid core. The aggrecan aggregates give the cartilage the gel like consistency. The glycoproteins are chondronectin and chondrocalcin. Chondronectcin is integral in adhering the cell membranes to the extracellular matrix and chondrocalcin is responsible for calcium binding in the ECM 9. Proteoglycans are arranged in aggrecan aggregates that hold a large amount of water (close to 80% in Hyaline Cartilage is water). They allow diffusion of nutrients and resist compression by diffusing the force. 10. Articular cartilage is without perichondrium. This allows for direct matrix to matrix contact which is quite slippery. 11. Articular Cartilage does no have a perichondrium and therefore moves against other articular cartilages quite well. There are large Type II collagen fibers that are arched that run radially to help resist shearing forces. There is a layer of calcified cartilage away from the articular surface to help provide support. 12. Appositional Growth and Interstitial Growth a. Appositional Growth is growth on the surface of tissue. This occurs in the perichondrium in cartilage. b. Interstitial Growth is growth from within. This is caused by cell division of chondroblasts already imbedded in a matrix. 13. Cartilage can usually regenerate it self by appositional growth at the perichondrium, however articular cartilage cannot repair itself because of the lack of nutrient supply. To regrow joint cartilage, holes must be punched through the subchondral bone to allow chondroprogenitor cells to arise from the marrow and migrate into the hole. The chondroprogenitor cells rarely produce hyaline cartilage, but rather more often produce Fibrocartilage. 14. Classification of joints a. Structurally i. Fibrous 1. Sutures 2. Syndesmoses 3. gomphoses ii. Cartilaginous 1. Synchondroses 2. Symphysis iii. Synovial 1. Synovial fluid, cavity, membrane 2. Articular capsule, cartilage b. Functionally i. Synathroses ii. Amphiarthroses iii. Diathroses 15. Describe changes in joint in osteo and rheumatoid arthritis a. Rheumatoid Arthritis i. Inflamatory ii. Autoimmune against synovial membrane primarily iii. Synovial membrane thickens and increase secretion of synovial fluid. iv. Pannus forms across cartilage and erodes cartilage to the bone allowing them to eventually fuse. b. Osteoarthritis i. Non Inflammatory ii. Progressive iii. Fibrillization of articular cartilage iv. Proliferation of peripheral cartilage v. Replacement of cartilage spurs with boney tissue (hence osteo) Muscle I, II, and III Objectives 1. The three types of muscle tissue are Skeletal, Cardiac, and Smooth. Skeletal muscle causes movement/stature of the body. They act on bone tissue to exert a force in a direction. They are striated muscle tissue in that the myofibrils are organized and inline with one another. They are multinucleate and can run long distances if need be. They require an attachment point, usually bone. They are attached to bone by tendons. Cardiac muscle does not attach to bone, but rather itself. Cardiac muscle has a series of cellular connections that allow it to pull on it self. The muscle has striation, but the fibrils are not long and strait. They branch, enabling a cardiac myocyte to pull in multiple directions. They are mononucleate and have 2 types of intercellular connections on different aspects of the cell. The traverse connections are the Intercalated Discs. They are a combination of the fascia adherens and the desmosomes. The desmosomes are present where there is no actin present. These ICDs allows for the conversion of chemical energy (ATP) to mechanical energy (heart pumping). The longitudinal aspect is populated by gap junctions so that all the myocytes can “get the joke” at the same time. Cardiac muscles are controlled by autonomic modulation, but mainly the Sinoatrial node and atrioventricular node. The SA node generates and maintains the beat of the heart. Smooth muscle is arranged in an anastomosing arrangement, meaning they overlap and form an almost quilt like appearance in longitudinal section. They are surrounded by a basal lamina and reticular connective tissue. This allows them to pull and squeeze on each other. They have a single nucleus that is placed somewhat centrally. They are designed for a slow and steady squeezing motion. They can be partially or fully contracted, but this intermediate phase separates them from other muscle tissue, as they cannot do this. 2. Skeletal and Cardiac muscle cells have sarcomeres, as their myofibrils are arranged in a very specific pattern. Smooth muscle cells do not have these organized bundles of myofibrils. Skeletal muscles are multinucleate where as cardiac and smooth are both mononucleate. Skeletal and Cardiac myocytes are not capable of mitosis but smooth muscle is. Skeletal muscles do not have intercellular junctions, but smooth and cardiac both have gap junction. Cardiac also have intercalated discs. Because skeletal and cardiac cannot undergo mitosis, they must find another way to regenerate. Skeletal have a set of undifferentiated cells that can replace them. Cardiac cells are still workin it out. 3. Epimysium contains dense irregular connective tissue. The perimysium is also dense irregular as it is the septa from the epimysium. The endomysium is comprised of loose connective tissue. All three layers contain type 1 collagen, but the endomysium also contains type IV collagen. This connective tissue brings in the neurovascular bundles to oxygenate and innervate the muscle 4. Figure this out 5. The Triad is the combination of two enlarged terminal cisternae flanking a Transverse tubule. This allows for rapid and diffuse depolarization of the membrane. 6. The Z Line has three proteins. Z Protein provides the backbone of the z disc. Attached to it is alpha actinin, which binds actin to the z disc and cap Z which binds the (+) end of actin so it can prevent the autopolymerization of actin. 7. The thin filament is mostly actin, however there are other proteins associated with the thin filament. Tropomyosin wraps around the actin chain like a rope cover the myosin-binding site. Troponin is a three-subunit protein that interacts with tropomyosin. TnT binds with Tropomyosin. TnI regulates the inhibition of myosin binding on the actin molecule. TnC is a regulatory site that binds Ca++ and causes the uncovering of the myosin binding site. Also associated with the thin filaments is Nebulin. It acts as backbone for actin. Tropomodulin is also affiliated with actin and binds the (-) end of the actin filament to stabilize its size. 8. The thick filament is mostly myosin, however it does contain other proteins. The myosin is responsible for the actual contraction of the sarcomere. The essential light chain and regulatory light chains affect the bending ability of the myosin flex points. C protein acts as a ring binding the myosin strands together. Titin is an anchor protein that holds the myosin band in the middle of the sarcomere. To keep the sarcomeres separate, myomesin is present to bind and stabilize the thick filaments location in relation to each other. Creatine kinase is also at the m line of the thick filament for rapid reproduction of ATP. 9. Myomesin and Creatine Kinase are at the M Line. Myomesin keeps thick filaments where they are supposed to be so that actin filaments can over lap. Creatine Kinase is for local, rapid ATP regeneration. 10. I got this. 11. Actin Cap proteins are important because actin likes to autopolymerize. The function of sarcomeres is dependent on the length of actin molecules and therefore must remain constant. 12. The electrical event that occurs at the motor end plate of the neuron is the systematic and rapid depolarization of the neuron that leads to the release of neurotransmitters into the primary and secondary synaptic clefts. This will cause the initial depolarization of the membrane by the influx of Na+ by way of ligand-gated channels. The initial depolarization will be further propagated by the voltage-gated Na+ channels. The influx of Na+ will turn DHPR and open up Ryanodine receptors and allow for the release of a whole lot of Ca++ (unless you are the USBME than it is caused by the increase in IP3 formation that causes the opening of an IP3 ligand-gated Ca++ channel) 13. Signal transmission results in increased Ca++ (see above). The increased calcium will interact with TnC and cause the exposure of the myosin-binding site on actin. 14. ADP-Pi bound to myosin is in relaxed state and can bind to actin. The binding causes the release of Pi which then causes the cocking of the myosin head. The new conformation will release ADP and allow for binding of ATP. When ATP binds, the myosin head will release the actin filament. The myosin head remains in the tense position until the ATP is cleaved to form ADP and Pi. 15. See Number 14 16. Muscle relaxation is not a passive process. The Ca++ must be actively pushed back into the sarcoplasmic reticulum. Approximately 50% of the ATP used in a muscle contraction series is consumed post contraction 17. The muscle spindle is the apparatus used to sense the current state of the muscle. They have efferent nervous signals (sent back to brain). There are two types of muscle spindles and two types of efferent nerves. The first type of spindle is the nuclear bag spindle. This cell has many nuclei located in a central location giving the appearance of a “bag of nuclei.” The second type of cell is a nuclear chain spindle. The nuclei of this cell are centrally located, but are in a single file chain. Only one nucleus can be seen in cross section. The two types of efferent nerves are the annulospiral nerves and the flowerspray nerves. The annulospiral nerves wrap around the nuclear bag fibers and sense when the coils become loose indicating a lengthening of the spindle fiber. The flower spray nerves sense stretching apart. They are located on the nuclear bag and nuclear chain spindle. 18. The cardiac myocyte is a striated muscle cell however it is not linear. It branches so that it may pull in multiple directions at one time. It is not innervated by the voluntary nervous system, but rather modulated by the autonomic nervous system. It does not have an Epi or perimysium, but rather a tissue type more like the endomysium sandwiched between cells. They are connected to each other which give the characteristic rotational contraction. They are directly connected by cell-cell junctions (Intercalated discs and gap junctions.) 19. The intercalated disc is along the transverse region of cardiac muscle. They consist of desmosomes and fascia adherens. The desmosomes are located where there are no actin filaments from a sarcomere to bind too. The transverse region glues the cardiac myocytes together. The lateral region is populated by gap junctions. These gap junctions allow for intercellular communication. Muscle IV Objectives 1. Characteristics of Muscle Fibers a. Pennated i. Run at least on angle to direction of force vector ii. Slow contracting iii. Space saving iv. Force loss due to physics overcome by increase in fiber count b. Non-Pennated i. Run parallel to the direction of the force vector ii. Fast contracting iii. Few fibers 2. Fiber Types a. Type I i. Slow ii. Oxidative (probably use more fat so more Kreb’s and ETC) iii. High in Mito iv. Aerobic v. Low Vmax b. Type II i. Type IIa 1. Oxidative and glycolytic 2. Intermediate fibers (not red or white, but in btwn) 3. High Mitochondrian 4. High Glycogen 5. Aerobic and Anaerobic ii. Type IIb 1. Only found in Rats 2. fastEST Glycolytic 3. White Fibers 4. Anaerobic 5. Low Mito 6. High Vmax iii. Type IIx 1. White Fibers 2. Fast Glycolytic 3. Between b and a in everything. 3. See Muscle II with Chiaia 4. Think about it 5. General Rule is as Muscle gets longer, force is increased. Biceps brachii and the Quadriceps don’t follow general rule because force arm plays a bigger role. 6. More delicate muscle tasks require more delicate control. As you increase in fine motor necessity, the number of fibrils per motor unit decreases. 7. Muscle spindle is for lengthening and golgi tendon is for tension recognition. 8. Changes in Skeletal Muscle a. Training i. Endurance 1. Increase % of IIa 2. Decrease % of IIb/x 3. Mitochondrian increase in number 4. Oxidative enzymes increase ii. Weight Training 1. Opposite of Endurance Training b. Non-Weight Bearing i. Anti-gravity muscles are most affected. ii. Cross-Sectional area of quads decrease the most. c. Bed Rest i. Same as non-weight bearing d. Aging i. Decrease in all muscle type ii. Increase in percent type II until 35, then decrease in percent type II iii. Aging muscles respond to strength training Glycolysis Objectives 1. Glycolysis takes place in the cytoplasm. First stage is edergonic and uses 2 ATP. The second stage is exergonic and it generates 4 ATP. Net production in 2 ATP 2. Aerobic generates Pyruvate from glucose. Anaerobic glycolysis must regenerate NAD+ so it converts pyruvate to lactic acid. 3. ATP must be used before glucose can be catabolized because (1) glucose must be activated (2) Glucose must be maintained in cell by converting it to glucose 6 phosphate and (3) it allows for regulation of pathway (at Hexokinase and PFK1). Steps that require ATP are step 1 (hexokinase; glucoseglucose 6 phosphate) and step 3 (PFK1; Fructose 6 phosphateFructose 1,6 bisphosphate). Steps that create ATP are step 7 (phosphoglycerate kinase; 1,3 bisphosphoglycerate3 phosphoglycerage) and step (Pyruvate Kinase; Phosphoenol pyruvatepyruvate). ATP generating steps are multiplied by two because glucose produces two sets of 3 carbon chains. 4. GlucoseGlucose-6-PhosphateFructose 6 PhosphateFructose 1,6 bisphosphateDihydroxyacetone Phosphate and Glyceraldehyde 3 Phophate (DHAP is converted to G3P)1,3 Bisphosphoglycerate 3 Phosphoglycerate2 PhosphoglyceratePhosphoenol PyruvatePyruvateLactate (only in anaerobic metabolism) 5. 1. Hexokinase(extrahepatic tissue)/Glucokinase(liver) (GG6P) 2. Phosphoglucoisomerase 3. Phophofructokinase 4. Aldolase 5. Triose Phophate Isomerase (DHAPG3P) 6. Glyceraldehyde 3 Phosphate Dehydrogenase 7. Phosphoglycerate Kinase 8. Phosphoglycerate mutase 9. Enolase (2PGPEP) 10. Pyruvate Kinase 11. Lactate Dehydrogenase. Reaction 6 catalyzes the uptake of Pi 6. Hexokinase has a much higher affinity for glucose than glucokinase. Liver does not use Gycolysis, glucokinase is used for Glycogen Synthesis 7. 3 Regulatory Enzymes—1. Hexokinase 2. Phosphofructokinase 1 3. Pyruvate Kinase 8. (a) DHAP is converted to G3P in glycolysis to produce energy. (b) DHAP is reduced by NADH giving rise to Glycerol 3 Phophate, which the base for lipid synthesis. (c) DHAP is reduced by NADH to glycerol 3 phosphate which is then converted back to DHAP by a mitochondrial enzyme that oxidizes FAD to transfer protons from the cytoplasm to the ETC. 9. Cleavage of phosphate bonds in glycolysis releases enough energy to create ATP. 10. Reaction 6—Glyceraldehyde 3 Posphate to 1,3 bisphosphoglycerate by Glyceraldehyde 3 Phosphate Dehydrogenase 11. Reaction 11—Lactate dehydrogenase in anaerobic. In aerobic, NAD+ is regenerated by the shuttle systems 12. Primary rate controlling step is PFK-1. It is very dependant on the need for ATP. ATP and Citrate are an allosteric inhibitor. High [H] will turn PFK1 off as well. AMP and Fructose 2,6 bisphosphate will upregulate PFK1. 13. Redox couples! NAD/NADH=-0.32V 3 Phosphoglycerage/Glyceraldehyde 3 Phosphate=-0.55V Eo=-0.32 –(-0.55)=+0.22V deltaG=nFdelta E Therefore HUGE Value for deltaG=-10.45Kcal Highly exergonic 14. Irreversible reactions—hexokinase, phosphofructokinase, and pyruvate kinase 15. (a) 2 ATP in anaerobic (b) 30-32 ATP in aerobic 16. (a) 2 NADH in aerobic (b) 0 NADH in anaerobic 17. The shuttles take the hydrogen’s associated with NADH and bring them into the mitochondrial matrix for use within the ETC. (a) Glycerophosphate Shuttle uses a mitochondrial glycerol phosphate dehydrogenase, which uses FAD as a coenzyme. Hydrogens go right to CoQ. (b) Malate/Aspartate; Oxaloacetate is convereted to malate then transported across mitochondrial membrane using an alphaKG/Malate Antiporter. Malate then produces OxAc by malate dehydrogenase in IMS. OxAC is converted to alpha KG by Apspartate Aminotransferase and is then antiported out using same antiporter. Aspartate is antiported out using an Glutamate/Aspartate Antiporter where the alpha KG is then converted to OxAc using Asp. Aminotransferase. 18. Pyruvateacetaldehyde and CO2Ethanol Reaction from AcetaldehydeEthanol regenerates NAD 19. Ethanol is metabolized by oxidizing EtOH using NAD to create acetaldehyde then it is oxidized again by NAD to create Acetic Acid (AcetylCoAF.A.) 20. Hypoglycemia and Lactic Acidosis. Any process that needs NAD will be put on hold. Lactic Acid won’t be converted to Pyruvate and will lead to Lactic Acidosis. No glycolysis therefore hypoglycemia. Gluconeogenesis Objectives 1. Lactate is converted to Pyruvate, followed by a series of reverse glycolytic steps to get to Glucose. Gluconeogenesis is mainly in the kidneys and liver and takes place in the mitochondria and the cytosol. Lactate and glycerol are used as precursers as well as a slew of amino acids. Lactate comes from the muscles and RBCs and glycerol comes from triglycerides. Oxaloacetate is very important for synthesis of glucose as it is the direct precurser to PEP and helps bypass pyruvate kinase. Glycolytic molecules can be used to make new glucose as well (F6P and G3P). 2. Three irreversible steps in glycolysis a. GlucoseGlucose-6-Phosphate (Hexokinase/Glucokinase) b. Fructose-6-PhosphateFructose-1,6-Bisphosphate (PFK) c. Phosphoenol PyruvatePyruvate (Pyruvate Kinase) 3. Overcome bye a. Glucose-6-Phosphatase b. Fructose-1,6-Phosphotase c. Three steps i. PyruvateOxaloacetic Acid (Pyruvate Carboxylase) this reaction uses biotin to carboxylate and ATP ii. OxaloacetateMalateOxaloacetate(Malate Dehydrogenase) Used for transport from Mitochondrial matrix to cytoplasm iii. OxaloacetatePEP (Phosphoenol Pyruvate Carboxykinase) Uses GTP and liberates CO2 4. Pyruvate Carboxylase adds CO2 to pyruvate to yield Oxaloacetate and is (+) regulated by Acetyl CoA. 5. Acetyl Co A cannot be used to make new glucose and thus cannot use even numbered fatty acids because they produce acetyl CoA. 6. Acetyle Co A is a positive modulator of pyruvate carboxylase 7. Biotin is the coenzyme for carboxylation. It is the carrier of active CO2 in carboxylations. It has an imidozole ring fused to a Thiophene ring with a fatty acid. The carboxylate group will bind with lysine residue in enzyme. (it looks like two houses that are united at the floor. The top house has nitrogen and the bottom house has a sulfur roof. The fatty acid is attached to the bottom house. Biotin participates in carboxylations, such as: a. pyruvate carboxylase, b. Propionyl CoA + CO2Succinyl CoA c. malonyl CoAAcetyl Co A 8. Oxaloacetate is transported to the cytoplasm from the mitochondrial matrix by way of the malate shuttle. OxAc is first converted to malate by malate Dehydrogenase. Malate then crosses the membrane and is converted back to OxAc by the same enzyme. 9. The essence of this question is based in the number of carbons. Glycerol is convered to glycerol-3-phosphate and then to dihydroxyacetone phosphate. 10. Muscle and Brain cannot synthesize glucose from lactate because they lack Glucose-6-Phosphatase. This is good because then all the glucose can only be used for energy rather than be exported (like the liver and kidney). 11. Lactate and alanine are converted in the liver. Lactate is converted to Pyruvate and alanine is converted to pyruvate 12. Adipose Tissue lacks Glycerol Kinase so the glycerol that is liberated in the break down of fatty acids cannot be phosphorylated 13. Amino Acids can be converted to glycolytic intermediates of the TCA and will then eventually become Oxaloacetate. 14. Acetyl CoA positively modulates pyruvate carboxylase. Secondary Control is regulated at the fructose-1,6-bisphosphotase. Glucagon stimulates F16BP by inhibiting F26Bisphophate formation (F26BP stimulates PFK). Look at Pg221 of Unit 2 for more information. 15. 4 ATP, 2 GTP and 2 NADH a. ATP at 2 spots i. PyruvateOxAc ii. 3-phosphoglycerate1,3 Bisphosphoglycerate b. GTP from OxAcPEP c. NADH from 1,3 BisphosphoglycerateGlyceraldehyde-3-Phosphate 16. Ethanol inhibits the conversion of Lactate to Pyruvate by having a strong hold on the NADH population. Inhibits Lactic Acid Dehydrogenase. Causes Lactic Acidosis. Glycogen Metabolism Objectives 1. Alpha and Beta Linkages are differentiated by the linkages at the anomeric carbon. Glucose C1 Fructose C2 2. Glycogen is found in muscle and liver. There is more in the muscle. Starch and glycogen differ because starch is made of two polymers (amylopectin and amylose). Amylopectin is most analogous to glycogen, however glycogen has more branch points. In the liver, glycogen is a storage vessel of glucose. The liver does not used glucose for its own purposes. Muscle stores glycogen for its own use. The general features of glycogen are: a. Branched mass of Glucose Residues b. Alpha 1,4 Linkage straight chains c. Alpha 1,6 Linkage Branch Points 3. Features of Metabolism a. Breakdown-Glucose is stripped from the outer branches by way of phophorylation with phosphorylase. Hence this process is called phosphorolysis. Debranching enzyme cleaves three glucose residues from branch and puts them on the main chain and amylo 1,6 glucosidase cleave the last glucose on the branch. b. Synthesis-Glycogenin plus 10 UDPGlucose autocatalyzes to form a primer for glycogen biosynthesis. Activated Glucose (UDPGlucose) will be added to the primer by Glycogen Synthase. Branching enzyme moves a sugars nn+6 and adds them to n-3 c. Phosphorylasealpha 1,4 d. Transferasealpha 1,4 e. Glucosidasealpha 1,6 4. Glucose-1-Phosphate 5. After debranching enzyme moves the tri-saccharide from the branch to the main chain, amylo 1,6 glucosidase will hydrolyze the bond to liberate free glucose 6. Active glucose is Uridine Diphosphate glucose (UDP-G) 7. UDPG is formed by converting G6P to G1P by phosphoglucomutase. G1 will react with UTP to form UDPG and Pyrophosphate by way of UDPG Pyrophosphorylase. PiPi will be quickly convered to 2 x Pi thus pulling the rxn forward. 8. Phosphorylase cleaves glucose-1-phosphate from glycogen chains by adding phosphate to the mix. Phophorylation turns on phosphorylase. It is turned off by phosphatase which cleaves the phosphate from the enzyme 9. Glycogen synthase creates the alpha 1,4 glycosidic bonds that link main chain. Phosphorylation turns glycogen synthase off. See page 239. 10. The same mechanisms that stimulate glycogen sythesis will turn off glycogenolysis. Insulin turns up glycogen metabolism and glucagon turns up glycogenolysis. Cyclic AMP is upregulated by Glucagon and activate protein Kinase A. PKA phosphorylates phosphorylase kinase which will activate phosphorylase by phosphorylating it. 11. Glucagon and epinephrine release the beta subunit of the receptor which activates adenylate cyclase. Glucagon only acts in the liver. Epinephrine acts in both. 12. Diseases a. Von Gierke’s DiseaseDefective Glucose-6-phosphatase. Glucose cannot be released into the blood. b. Anderson’s DiseaseDefective Branching Enzyme. No branches, just very long chains c. McArdle’s DiseaseDefective Phosphorylase. Cannot break down glycogen in the muscles. Pentose Phosphate Pathway Objectives 1. The primary functions of the PPP are: Produces NADPH from glucose, direct synthesis of ribose from glucose. It occurs in the cytoplasm. Ribose can also be derived from Fructose 6 Phosphate and Glyceraldehyde 3 phosphate by reverse of non-oxidative pathway. PPP is an alternative way to degrade glucose. 2. Reactions a. Glucose-6-PhosphateDeltaLactone plus NADPH i. by way of G6PD ii. NADPH is produced b. DeltaLactone6-Phosphogluconate i. Phosphgluconolactase 3. 4. 5. 6. 7. 8. ii. Hydrolysis reaction c. 6-PhosphogluconateRibulose-5-Phosphate i. 6-Phosphogluconate Dehydrogenase ii. NADPH is produced iii. Removal of Hs from position 2 iv. CO2 is Produced (C6C5) d. Ribulose-5-PhosphateRibose-5-Phosphate i. Phosphopentose Isomerase NADPH serves as a Hydrogen and Electron Donor in REDUCTIVE BIOSYNTHESIS. Fatty Acid Biosynthesis. Cholesterol Biosynthesis. Neurotransmitter Synthesis, Nucleotide Synthesis. Also Detoxification: Reduction of Oxidized glutathione (GS-SH2GSH), Cytochrome P450 Monoxygenase (NADPH is the coenzyme to activate O2 to Hydroxylate) 6 Important Ribose containing compounds a. NAD b. FAD c. ATP d. AMP e. GTP f. NADP g. RNA PPP is required for synthesis of Fatty acids and there fore is integral in formation of Adipose Tissue. PPP is very important in Red Blood Cells because is used in Glutathione reduction. Two GSH will react with H2O2 to form GS-SH by way of Glutathione peroxidase. NADPH reacts with GS-SH to form 2GSH by way of Glutathione Reductase. H2O2 reacts with Hemoglobin (HbFe++HbFe+++). H2O2 also creates disulfide bonds and Bisulfate (SO3H) and leads to Denaturation. G6PD deficiency will lead to NADPH deficiency. Problem arises when patients with this deficiency are given oxidizing drugs. H2O2 levels will increase causing increase in MetHb and increase in oxidized sulfhydral groups and denaturation. Denaturation will cause precipitation of proteins (then called Heinz Bodies). Glyceraldehyde 3 Phosphate and Fructose 6 Phosphate Three Reactions/two Enzymes a. Transketolase b. Transaldolase c. Reactions get these things i. 1 gets G3P ii. 2 gets F6P iii. 3 Gets both d. Rx1 Xyulose-5-Phosphate + Ribose-5-Phosphate Glyceraldehyde 3 Phosphate and Seduheptulose (C5+C5 C3+C7) e. Rx 2 Seduheptulose+Glyceraldehyde 3 PhosphateErythrose+Fructose-6-Phosphate (C7+C3C4+C6) f. Rx 3 Erythrose + Xyulose-5-PhosphateGlyceraldeyde-3-Phophate + Fructose-6-Phosphate (C4+C5C3+C6) g. Total stoichiometry i. Start with 3xC5=15 carbon ii. End with 2xC6 + 1xC3= 15 carbon 9. TK transfers 2 carbons (CH2OH) and TA transfers 3 Carbons 10. TPP participates in the transketolase reaction. If no TPP no transketolase so its used as a test for thiamine deficiency. 11. Using the Fructose 6 Phosphate and Glyceraldehyde 3 Phosphate and the process of Gluconeogenesis 12. 6 rounds of oxidative and 6 rounds of non-oxidative will cause the complete loss of 6 carbons (signify one molecule of glucose). Interconversion of Hexoses Objectives 1. Galactose is phosphorylated to formed Galactose-1-Phosphate by galactokinase. Then urydilic acid (UMP) is transferred to Gal-1-P from UDPGlucose by way of Galactose-1-Phosphate Urydil transferase. 2. UDP-Galactose is activated galactose. One fate is it can bind with with glucose to form lactose by way of lactose synthase. It can also be converted to UDP Glucose by way of Uridine Diphospogalactose-4-Epimerase. 3. Galactose-1Phoshate Urydil Transferase is blocked in galactosemia. It causes a build up of galactitol (cataracts) and Galactose-1-Phosphate which causes liver toxicity. 4. Fructose metabolism a. Liver—In the liver, fructose is first phosphorylated at the 1 position to make fructose-1-phosphate. It is then cleaved by aldolase b to make DHAP and D-Glyceraldehyde. There is NO regulation of this pathway b. Extrahepatic Tissue—In extrahepatic tissue, fructose is treated like glucose and is first phosphorylated at the 6 position to make fructose6-phosphate. It is then phosphorylated again to make Fructose 1,6 bisphosphate by PFK. PFK is regulated by ATP. 5. Essential fructose uria is a defect in fructokinase. This is a benign condition that results in increased fructose in the urine. In Hereditary Fructose Intolerance, there is a defect in Aldolase B which causes a build up of Fructose-1-Phosphate, which is toxic. HFI patients least’s to depletion of ATP and Phophate pools. This then results in decreased Gluconeogenesis and glycogenolysis and persistent hypoglycemia. 6. UDP-Glucuronic Acid is produced from Glucose-6-Phosphate by the uronic acid pathway. Glucose-6-Phosphate is converted by Glucose-1-Phosphate by way of phosphoglucomutase. Glucose-1-Phosphate is converted to Uridine Diphosphoglucose by way of UDP glucose pyrophosphorylase. Urinine Diphosphoglucose is convered to Uridine Diphosphoglucuronic Acid (UDPGlucuronic acid). These can react with organic insolubles and make them soluble and bring them for excretion. 7. The uronic acid pathway can make UDP-Glucose. It can also create intermediates for the pentose phosphate pathway (hexoses to pentoses). The UAP also is a source of active glucurinate (UDP Glucuronic Acid), which participates in detoxification. UAP is also a metablic pathway for non phosphorylated sugars. Not in humans in primates, but Vitamin C is synthesized by the UAP. 8. Humans cannot synthesize ascorbic acid because we lack the Gulonolactone Oxidase.