Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Complement system wikipedia , lookup
DNA vaccination wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
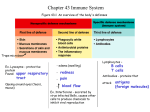
path 184 to 226 Innate Immunity Innate immunity: epithelial barriers, phagocytic cells (neutrophils and macrophages), DCs, NKs, plasma proteins Cellular reactions: inflammation (phagocytic leukocytes recruited and activated to kill microbes) and anti-viral defense (mediated by DCs and NKs) Pathogen-associated molecular patterns: components of microbes essential for infectivity (thus can’t mutate); leukocytes and epithelial cells recognize these to initiate immune response Danger-associated molecular patterns: molecules released by injured and necrotic cells; WBCs recognize these Different TLRs specific for components of different bacteria and viruses o Signal by common pathway that leads to activation of transcription factors (NF-κB), which turns on production of cytokines and proteins that stimulate microbicidal activities of various cells Receptors for mannose residues and receptors for opsonins: bind microbes for phagocytosis Dendritic cells – produce type I interferons (anti-viral cytokines that inhibit viral infection and replication) Complement system activated by microbes using alternative and lectin pathways Mannose-binding lectin and C-reactive protein coat microbes for phagocytosis Adaptive Immunity Complement system activated by antibodies using classical pathway Adaptive immunity = Lymphocytes and their products Cells of the Immune System Lymphocytes differentiate into effector cells (perform function) and memory cells T cells: 60-70% of lymphocytes in blood; recognizes specific cell-bound antigen by means of TCR o TCR consists of α and β chains (disulfide-linked); recognizes peptide antigens displayed by MHC on surface of APCs (MHC restriction) o During T cell development in thymus, TCR genes rearrange to form different combos Enzyme that mediates rearrangement is product of RAG-1 and RAG-2; mutations in these genes result in failure to generate mature lymphocytes o Polyclonal T cell clusters non-neoplastic; monoclonal T-cell proliferations neoplastic o Each TCR noncovalently linked to 5 polypeptide chains that form CD3 complex and ζ chain dimer (identical in all T cells); involved in transduction of signals into T cell after TCR binds antigen o TCR complex = TCR + CD3 + ζ chain dimer o γδ TCR recognizes peptides, lipids, and small molecules w/o required MHC; aggregate at epithelial surfaces o NK-T cells – very limited diversity of TCRs; recognize glycolipids displayed by MHC-like molecule CD1 o CD4 and CD8 expressed on mutually exclusive subsets of αβ T cells; serve as coreceptor that initiates signals necessary for activation of T cells CD4+ function as cytokine-secreting helper cells that help macrophages and B cells; respond to class II MHC molecules CD8+ are CTLs; respond to class I MHC molecules B lymphocytes: develop from precursors in bone marrow; present in blood, lymph nodes, spleen, and MALT o Recognize antigen via B-cell antigen receptor complex o Membrane-bound antibodies (IgM and IgD) on surface of naïve B cells; antigen-binding component of receptor complex; receptors have specificity derived from RAG-mediated rearrangement of Ig genes o Antigen receptor complex also contains Igα and Igβ; essential for signal transduction through antigen receptor o Type 2 complement receptor (CR2 or CD21) is receptor for EBV, which readily infects B cells o Have Fc receptors, complement receptors, and CD40 Dendritic cells (interdigitating dendritic cells): most important APC for initiating primary T-cell responses o Located under epithelial and interstitial of all tissues o Langerhans cell – immature DC in epidermis o Express TLRs and mannose receptors to bind antigens o DCs recruited to T-cell zones of lymphoid organs, where they present antigens to T cells o Express high levels of molecules needed for presenting antigens to and activating CD4+ T cells Follicular dendritic cells – bear Fc receptors for IgG and receptors for C3b; can trap antigen bound to antibodies or complement proteins o Present antigens to B cells and select B cells w/highest affinity for antigen Macrophages that have phagocytosed microbes and protein antigens process antigens and present peptide fragments to T cells o T cells activate macrophages and enhance ability to kill ingested microbes o Participate in effector phase of humoral immunity (phagocytose opsonized microbes w/IgG or C3b) NK cells: 10-15% of peripheral blood lymphocytes; contain abundant azurophilic granules (large granular lymphocytes) o Kill infected and tumor cells w/o prior exposure or activation o CD16 (Fc receptor for IgG; confers ability to lyse IgG-coated target cells [antibody-dependent cellmediated cytotoxicity; ADCC]) and CD56 commonly used to identify NK cells o Functional activity of NK cells regulated by balance between signals from activating and inhibitory receptors o NKG2D receptors recognize surface molecules induced by stress (infection, DNA damage) o Inhibitor receptors recognize self-class I MHC molecules expressed on all healthy cells (either Ig-like receptors or CD94 family of lectins); prevent NK cell from killing normal cells Infection or neoplastic transformation induces expression of ligands for activating receptors and reduces expression of class I MHC molecules o Secrete IFN-γ, which activates macrophages to destroy ingested microbes o Activity regulated by interleukins (IL-2 & IL-15 stimulate proliferation of NKs; IL-12 activates killing function and secretion of IFN-γ) Tissues of the Immune System Generative lymphoid organs – thymus and bone marrow Peripheral lymphoid organs – lymph nodes, spleen, and mucosal and cutaneous lymphoid tissues; organized to concentrate antigens, APCs, and lymphocytes to optimize interactions and adaptive immune responses o Spleen – reacts to blood-borne antigens; blood flows through sinusoids, and antigens trapped by DCs and macrophages in spleen T lymphocytes concentrated periarteriolar lymphoid sheaths surrounding small arterioles B cells in follicles o Cutaneous lymphoid system under epithelial of skin; mucosal lymphoid system under epithelia of GI and respiratory tracts Pharyngeal tonsils and Peyer’s patches are mucosal lymphoid tissues o In lymph nodes, B cells concentrated in discrete structures (follicles) in periphery (cortex); if B cell recently responded to antigen, follicle may contain germinal center T cells concentrated in paracortex (adjacent to follicles) Follicles contain follicular DCs, and paracortex contains DCs presenting to T cells Location of cells in follicles or paracortical areas dictated by chemokines produced by lymphocytes there; causes lymphocytes to leave lymph node and migrate to help Lymphocytes constantly recirculate between tissues and home (lymph nodes) o Naïve lymphocytes traverse peripheral lymphoid organs where immune responses initiated o Effector lymphocytes migrate to site of infection and inflammation o Plasma cells remain in lymphoid organs and don’t need to go to actual inflammation site o Naïve T cells migrate to lymph nodes and enter T-cell zones through high endothelial venules (HEVs) In lymph node, naïve cell encounters antigen that it specifically recognizes on APC Activates and alters expression of adhesion molecules and chemokine receptors Differentiated effector T cells leave lymph nodes, enter circulation, and migrate to tissues that harbor microbes Major Histocompatibility Complex (MHC) Molecules Displays peptide fragments of proteins for recognition by antigen-specific T cells Genes for MHC molecules clustered in HLA complex Class I MHC molecules – expressed on all nucleated cells and platelets; encoded by HLA-A, HLA-B, and HLA-C o Each molecule: polymorphic α (heavy) chain linked to non-PM β2-microglobulin not encoded in MHC o o o Extracellular region of α chain divided into 3 domains (α1, α2, α3); 1 & 2 form cleft where peptides bind Polymorphic residues line sides and base of peptide-binding groove; variation why binds diff. peptides Display peptides derived from proteins (viral antigens) located in cytoplasm; proteins degraded in proteasomes, peptides transported to ER, where they bind to newly synthesized class I molecules Peptide-loaded MHC molecules w/β2-microglobulin form stable trimer transported to PM o Nonpolymorphic α3 domain has binding site for CD8 o TCR recognizes MHC-peptide complex; CD8 molecule binds to class I heavy chain Class II MHC molecules – encoded by HLA-D (subregions: HLA-DP, HLA-DQ, HLA-DR) o Each has polymorphic α and β chains, each w/2 domains o Peptide-binding cleft formed by α1 and β1 domains; place where alleles differ o Present antigens that are internalized into vesicles; typically derived from extracellular microbes and soluble proteins Internalized proteins proteolytically digested in endosomes or lysosomes Peptides from lysosomes associate w/class II heterodimers in vesicles; stable peptide-MHC complexes transported to PM Class II β2 domain has binding for CD4 o Mainly expressed in macrophages, B lymphocytes, and DCs MHC locus contains genes that encode some complement components, TNF, and lymphotoxin o Class II locus contains genes that encode proteins involved in antigen processing and presentation (components of proteasome, peptide transporter, and class II-like molecule (DM) that facilitates peptide binding to class II molecules) Combo of HLA alleles in person = HLA haplotype; one set of genes from each parent = expression of 2 different molecules for every locus These are what are seen as foreign in transplanted organs Those that inherit HLA-B27 have much greater risk of ankylosing spondylitis Diseases associated w/HLA locus o Inflammatory diseases: ankylosing spondylitis and several postinfectious athropathies (HLA-B27) o Autoimmune diseases (endocrinopathies) associated w/alleles at DR locus o Inherited errors of metabolism (21-hydroxylase deficiency by HLA-BW47 and hereditary hemochromatosis by HLA-A) Cytokines: Messenger Molecules of the Immune System Interleukins: cytokines that mediate communication between leukocytes Cytokines of innate immunity: produced rapidly in response to microbes and other stimuli; made principally by macrophages, DCs, and NK cells; mediate inflammation and anti-viral defense o Include TNF, IL-1, IL-12, type I IFNs, IFN-γ, and chemokines Cytokines of adaptive immune responses: made principally by CD4+ T lymphocytes in response to antigen and other signals; function to promote lymphocyte proliferation and differentiation and activate effector cells o IL-2, IL-4, IL-5, IL-17, and IFN-γ Colony-stimulating factors: stimulate hematopoiesis; increase WBC numbers during immune and inflammatory responses and replace WBCs consumed during responses TNF antagonists can improve RA Sx Display and Recognition of Antigens Lymphocytes specific for large number of antigens exist before exposure to antigen; when antigen enters, it selects specific cells and activates them (clonal selection hypothesis) During innate response, microbe activates APCs to express molecules (costimulators) and secrete cytokines that stimulate proliferation and differentiation of T lymphocytes o Principal costimulators are B7 proteins (CD80 and CD86) expressed on APCs; recognized by CD28 receptor on naïve T cells o Antigen = signal 1; costimulatory molecules produced during innate immune response = signal 2 Signal 2 can be provided by substances released from necrotic cells (danger-associated mol.) Cell-Mediated Immunity: Activation of T Lymphocytes and Elimination of Intracellular Microbes One of earliest responses of CD4+ T cells is secretion of IL-2 and expression of high-affinity receptors for IL-2 o IL-2 acts on T cells and stimulates proliferation, leading to increase in antigen-specific lymphocytes o Functions of CD4+ T cells mediated by combined actions of CD40L (expressed on CD4+ cell when it recognizes displayed antigens) and cytokines o Some progeny of expanded T cells differentiate into effector cells that secrete different sets of cytokines TH1 secretes IFN-γ (potent macrophage activator) TH2 secretes IL-4 (stimulates B cells to differentiate into IgE-secreting plasma cells) and IL-5 (activates eosinophils) TH17 secretes IL-17; recruits neutrophils and monocytes Humoral Immunity: Activation of B Lymphocytes and Elimination of Extracellular Microbes When activated, B cells proliferate and differentiate into plasma cells that secrete different classes of antibodies Many antigens have multiple identical antigenic determinants (epitopes) able to engage antigen receptor molecules on each B cell and initiate process of B-cell activation Typical globular protein antigens not able to bind to antigen receptors; full response of B cells to protein antigens requires CD4+ T cells B cells ingest protein antigens into vesicles, degrade them, and display peptides bound to MHC molecules for recognition by CD4+ T cells, which express CD40L and secrete cytokines to active B cells Each plasma cell secretes antibodies that have same antigen binding site as cell surface antibodies o Polysaccharides and lipids stimulate secretion mainly of IgM antibody o Protein antigens (by virtue of CD40L and cytokine-mediated CD4+ T cell actions) induce production of antibodies of different isotypes (IgG, IgA, IgE) o Cytokines (IFN-γ, IL-4) induce isotype switching o CD4+ T cells stimulate production of antibodies w/high affinities for antigen (affinity maturation) o Isotype switching and affinity maturation occur mainly in germinal centers (formed by proliferating B cells), esp. in helper T cell-dependent responses to protein antigens Antibodies bind to microbes and prevent them from infecting cells (neutralizing) o IgG antibodies opsonize microbes (neutrophils and macrophages express receptors for Fc tails of IgG o IgG and IgM activate complement system by classical pathway; complement products promote phagocytosis and destruction of microbes o IgA secreted from mucosal epithelia neutralizes microbes in lumen of respiratory and GI tract o IgG actively transported across placenta and protects newborn until immune system mature o IgE and eosinophils cooperate to kill parasites Some antibody-secreting plasma cells migrate to bone marrow and liver for years, producing low Ig levels Decline of Immune Responses and Immunological Memory Majority of effector lymphocytes induced by infectious pathogen die by apoptosis after microbe eliminated Initial activation of lymphocytes generates long-lived memory cells (expanded pool of antigen-specific lymphocytes; more numerous than naïve cells specific for any antigen); respond faster and more effectively when re-exposed to antigen than naïve cells Mechanisms of Hypersensitivity Reactions Hypersensitivity – excessive response due to repeat exposure to antigen; pathologic response Development of hypersensitivity diseases associated w/inheritance of particular susceptibility genes Reflects imbalance between effector mechanisms of immune responses and control mechanisms that serve to normally limit responses Type I (immediate): immune response mediated by TH2 cells, IgE, and mast cells; results in release of mediators (act on vessels/smooth muscle) & pro-inflammatory cytokines (recruit inflammatory cells) o Occurs in minutes after combo of antigen w/antibody bound to mast cells in previously sensitized pt o Immediate (initial) reaction vasodilation, vascular leakage, and sm. muscle spasm or gland secretions o Late-phase reaction infiltration of tissues w/eosinophils, neutrophils, basophils, monocytes, and CD4+ T cells; tissue destruction typically mucosal epithelial cell damage o Most rxns mediated by IgE antibody-dependent activation of mast cells and other WBCs Mast cell: bone-marrow-derived cell widely distributed in tissues (nearest blood vessels, nerves, and subepithelial tissues) PM-bound granules that contain active mediators & acidic proteoglycans Activated by cross-linking of high-affinity IgE Fc receptors Triggered by C5a and C3a (anaphylatoxins), which bind receptors on mast PM Multivalent antigens bind to and cross-link adjacent IgE antibodies and underlying FcεRI, activating signal transduction pathways from cytoplasmic portion of receptors, leading to mast cell degranulation w/discharge of preformed (primary) mediators stored in granules and de novo synthesis and release of secondary mediators Basophils: surface IgE Fc receptors and cytoplasmic granules Mast cells and basophils have FcεRI (specific for Fc portion of IgE) that binds IgE o TH2 cells stimulate IgE production and promote inflammation Antigen presented to naïve CD4+ T cell; in response to antigen and IL-4, T cell differentiates into TH2 cell, which produces cytokines upon subsequent encounter w/antigen IL-4 stimulates class switching to IgE in B cells; promotes development of more TH2 IL-5 involved in development and activation of eosinophils IL-13 enhances IgE productin and acts on epithelial cells to stimulate mucus secretion More chemokines that attract more TH2 cells as well as other WBCs o Preformed mediators Vasoactive amines: histamine; causes intense smooth muscle contraction, increased vascular permeability, and increased mucus secretion by nasal, bronchial, and gastric glands Enzymes: neutral proteases (chymase, tryptase) and acid hydrolases; contained in granule matrix; cause tissue damage and lead to generation of kinins and activated complement components (C3a) by acting on precursor proteins Proteoglycans: include heparin and chondroitin sulfate; package and store amines in granules o Lipid mediators: synthesized by sequential rxns in mast PMs that lead to activation of phospholipase A2 (acts on membrane phospholipids to yield arachidonic acid) Leukotrienes C4 and D4 (most potent vasoactive and spasmogenic agents known); leukotriene B4 highly chemotactic for neutrophils, eosinophils, and monocytes Prostaglandin D2: most abundant mediator produced in mast cells by COX pathway; causes intense bronchospasm and increased mucus secretion Platelet-activating factor (PAF): produced by some mast cells; causes platelet aggregation, release of histamine, bronchospasm, increased vascular permeability, and vasodilation Chemotactic for neutrophils and eosinophils At high concentrations, activates inflammatory cells to degranulate o Cytokines: histamine and leukotrienes responsible for intense immediate rxn (edema, mucus secretin, SM spasm); cytokines recruit additional WBCs o Eosinophils: recruited by chemokines (eotaxin) produced by epithelial cells, TH2 cells, and mast cells Survival in tissues favored by IL-3, IL-5 (most potent), and GM-CSF Liberate proteolytic enzymes, major basic protein, & eosinophil cationic protein (toxic to epithelial cells) Produce C4 and PAF; directly activate mast cells to release mediators; recruited cells amplify and sustain inflammatory response w/o additional exposure to triggering antigen (major cause of Sx in allergic asthma); use steroids to treat o Atopy: predisposition to develop localized immediate hypersensitivity reactions to allergens; genetic Atopic people have higher serum IgE levels and more IL-4-producing TH2 cells o Can be triggered by temp extremes or exercise (non-atopic allergy because no TH2 or IgE) Type II (antibody-mediated): secreted IgG and IgM antibodies to antigens on cell surfaces or ECM participate directly in injury to cells by promoting phagocytosis or lysis; injury to tissues by induced inflammation o Antibodies may interfere w/cellular functions and cause disease w/o tissue injury (myasthenia gravis [inhibitory receptor response] or Graves disease [stimulatory receptor response]) o Cells opsonized by IgG recognized by phagocyte Fc receptors o When IgM or IgG deposited on surface of cell, they can activate complement system (classic path); C3b and C4b deposited on surfaces of cells and recognized by phagocytes that express receptors for proteins Complement activation leads to formation of membrane attack complex (drills holes through lipid bilayer, causing osmotic lysis); effective only w/cells w/thin walls (Neisseria) o ADCC: cells coated w/low concentrations of IgG killed by effector cells that bind to target by Fc receptors Lysis w/o phagocytosis; mediated by monocytes, neutrophils, eosinophils, and NK cells Occurs in transfusion reaction; hemolytic disease of newborn (erythroblastosis fetalis; antigenic difference between mother and fetus); autoimmune hemolytic anemia, agranulocytosis, and thrombocytopenia (antibodies to own blood cells); and certain drug reactions (drug acts as hapten by attaching to surface molecules of RBCs and antibodies produced against drugmembrane protein complex) o When antibodies deposit in fixed tissues, injury due to inflammation; deposited antibodies activate complement, generating by-products, including chemotactic agents (C5a; directs migration of PMNs and monocytes) and anaphylatoxins (C3a and C5a; increase vascular permeability) WBCs activated by engagement of C3b and Fc receptors; results in release or generation of prostaglandins, vasodilator peptides, and chemotactic substances WBC activation leads to production of lysosomal enzymes (proteases) that digest BM, collagen, elastin, and cartilage; produce ROS o Mechanism responsible for glomerulonephritis, vascular rejection of organ grafts Type III (immune complex-mediated): IgG and IgM antibodies bind antigens in circulation; complexes deposit in tissues and induce inflammation; neutrophils and monocytes produce damage by release of lysosomal enzymes and generation of toxic free radicals o Sometimes complexes formed at extravascular sites where antigen may have planted previously (in situ immune complexes) o Acute serum sickness: formation of antigen-antibody complex in circulation, deposition of complex in tissue, initiating inflammatory reaction at sites of immune complex deposition o Complexes of medium size formed in slight antigen excess are most pathogenic o Organs where blood filtered at high pressure to form other fluids (urine, synovial fluid) favored o Vasculitis – inflammatory lesion in blood vessels o Morphology: principal manifestation is acute necrotizing vasculitis w/necrosis of vessel wall and intense neutrophilic infiltration Necrotic tissue and deposits produce smudgy eosinophilic deposit that obscures underlying cellular detail (fibrinoid necrosis) Granular lumpy deposits of Ig and complement in kidney (glomerulonephritis) o If disease from single large exposure to antigen (acute serum sickness), lesions resolve from catabolism of immune complexes o Chronic form results from repeated or prolonged exposure (SLE) o Arthus reaction: localized area of tissue necrosis resulting from acute immune complex vasculitis Can be produced experimentally via scratch test As antigen diffuses into vascular wall, it binds preformed antibody, and large immune complexes formed locally; precipitates in vessel walls and causes fibrinoid necrosis; superimposed thrombosis worsens ischemic injury Type IV (cell-mediated): sensitized T lymphocytes (TH1, TH17, and CTLs) cause cellular and tissue injury o Can be cause of chronic inflammatory disease o Delayed-type hypersensitivity (DTH): CD4+ T cells; sometimes called immune inflammation TH1 and TH17 cells contribute to organ-specific diseases where inflammation prominent TH1 reaction dominated by activated macrophages; TH17 rxn has more neutrophils TH1 cells secrete IFN-γ, which activates macrophages (ability to phagocytose and kill microorganisms augmented; express more class II MHC molecules on surface; secrete TNF, IL-1, and chemokines that promote inflammation; produce more IL-12, amplifying TH1 response) Activated TH17 secrete IL-17, IL-22, chemokines, and several other cytokines that recruit neutrophils and monocytes, promoting inflammation; TH17 secretes IL-21 that amplifies TH17 rxn Tuberculin reaction produced by PPD (tuberculin); DTH characterized by accumulation of mononuclear cells (CD4+ T cells and macrophages) around venules, producing perivascular cuffing; in fully developed lesion, venules show marked endothelial hypertrophy Tubercle bacilli in lungs: perivascular infiltrate dominated by macrophages for 2-3 wks; activated macrophages undergo morphologic transformation into epithelium-like cells (epithelioid cells) surrounded by collar of lymphocytes (granuloma) Contact dermatitis: evoked by contact w/urushiol (antigenic component of poison ivy & poison oak); presents as vesicular dermatitis o Cell-mediated cytotoxicity: CD8+ CTLs kill antigen-bearing target cells; can cause DM type 1 Directed against MHC antigens in graft rejection Perforins and granzymes – preformed mediators in lysosome-like granules of CTLs CTLs that recognize target cells secrete complex of perforin, granzymes, and serglycin (enters target cells by endocytosis) In cytoplasm, perforin facilitates release of granzymes from complex Granzymes cleave and activate caspases (induce apoptosis) Activated CTLs express Fas ligand that binds Fas expressed on target cells and triggers apoptosis Produce cytokines (IFN-γ) involved in inflammatory reactions resembling DTH Autoimmune Diseases 3 requirements to be classified autoimmunity o Presence of immune reaction specific for some self-antigen or self-tissue o Evidence that such reaction not secondary to tissue damage but is of primary pathogenic significance o Absence of another well-defined cause of the disease Immune-mediated inflammatory diseases – uncertainty about target antigens and contribution of true autoimmunity; emphasizes chronic inflammation as part of pathogenesis Immunological tolerance – unresponsiveness to antigen as result of exposure of lymphocytes to that antigen Central tolerance: immature self-reactive B and T clones that recognize self-antigens during maturation in lymphoid organs are killed or rendered harmless o When immature T cells encounter antigens in thymus, cells that express self-antigen receptors die by apoptosis (negative selection, deletion) AIRE stimulates expression of peripheral tissue-restricted self-antigens in thymus; critical for deletion of immature T cells specific for antigens Mutations in AIRE gene cause autoimmune polyendocrinopathy o When developing B cells strongly recognize self-antignes, many reactivate machinery of antigen receptor gene rearrangement to get different receptors (receptor editing) If receptor editing doesn’t occur, self-reactive cells undergo apoptosis Peripheral tolerance: silencing autoreactive B and T cells in peripheral tissues o Anergy – prolonged or irreversible functional inactivation of lymphocytes, induced by encounter w/antigens under certain conditions If antigen presented by cells that dono’t bear costimulators, negative signal delivered, and cell becomes anergic Mechanisms: cells lose ability to trigger biochemical signals from TCR complex because of activation of ubiquitin ligases and proteolytic degradation of receptor-associated signaling proteins; T cells that recognize self-antigens receive inhibitory signal from receptors structurally homologous to CD28 but serve opposite functions Inhibitory receptors include CTLA-4 (binds B7 molecules) and PD-1 (binds 2 ligands expressed on wide variety of cells); loss of either gene develops autoimmune disease Affects mature B cells in peripheral tissues; in absence of specific helper T cells, B cells unable to respond to subsequent antigenic stimulation and may be excluded from lymphoid follicles resulting in their death o Suppression by Tregs – Tregs develop in thymus as result of recognition of self-antigens; may be induced in peripheral lymphoid tissues CD4+ cells that constitutively express CD25, α chain of IL-2 receptor, and Foxp3 IL-2 and Foxp3 required for development and maintenance of functional CD4+ Tregs Mutations in Foxp3 result in IPEX (systemic autoimmune; Immune dysregulation, Polyendocrinopathy, Enteropathy, X-linked) Mutations in IL-2 results in multi-organ autoimmunity Polymorphisms in CD25 cause MS and other autoimmune diseases o Deletion by activation-induced cell death: consequence of T-cell activation If T cells recognize self-antigens, they express pro-apoptotic Bim w/o anti-apoptotic Bcl-2 and Bcl-x (induction requires full set of signals for lymphocyte activation Unopposed Bim triggers apoptosis by mitochondrial pathway Cells express Fas (CD95); FasL (membrane protein structurally homologous to TNF) expressed mainly on activated T lymphocytes Engagement of Fas by FasL induces apoptosis of activated T cells by death receptor path Self-reactive B cells may be deleted by FasL on T cells engaging Fas on B cells Some antigens hidden (sequestered) from immune system (tissues where antigens located don’t communicate w/blood and lymph); self-antigens don’t induce tolerance but fail to elicit immune responses (testis, eye, brain); these sites immune-privileged sites If antigens from these tissues released due to trauma or infection, results in immune response that leads to prolonged tissue inflammation and injury (post-traumatic orchitis and uveitis) Most autoimmune diseases complex multigenic disorders (association w/MHC and HLA mutations) o Polymorphisms in PTPN-22 (encodes tyrosine phosphatase associated w/RA, type 1 DM, etc.); most frequently implicated gene in autoimmunity; mutations unable to control activity of tyrosine kinases involved in lymphocyte responses o Polymorphisms in NOD-2 associated w/Crohn disease (cytoplasmic sensor of microbes) Disease-associate variant ineffective at sensing intestinal microbes, resulting in entry of and chronic inflammatory responses against commensal bacteria o Genes encoding IL-2 receptor (CD25) and IL-7 receptor α chains associated w/MS and others Cytokines control maintenance of Tregs o B cells express Fc receptor that recognizes IgG antibodies bound to antigens and switches off further antibody production; knockout of receptor results in autoimmunity (B cells not controlled) Infections can upregulate expression of costimulators on APCs; if cells present self-antigens, results in breakdown of anergy and activation of T cells specific for self-antigens Some microbes express antigens that have same amino acid sequences as self-antigens (molecular mimicry) o Rheumatic heart disease: antibodies against strep cross-react w/myocardial proteins and cause myocarditis Some viruses cause polyclonal B-cell activation, resulting in production of autoantibodies; tissue injury may release self-antigens and structurally alter self-antigens so they are able to activate T cells not tolerant to new modified antigens o Infections induce production of cytokines that recruit lymphocytes (including self-reactive) to sites of self-antigens Some infections protect against some autoimmune diseases; promote low-level IL-2 production (essential for maintaining Tregs Once autoimmune disease induced, it is progressive, sometimes w/sporadic relapses and remissions o Immune system contains many intrinsic amplification loops that allow small numbers of antigen-specific lymphocytes to accomplish task of eradicating infections; when response inappropriately directed, amplification mechanisms exacerbate injury o Epitope spreading – infections damage tissues, release self-antigens, and expose epitopes of antigens normally concealed from immune system; result is continuing activation of lymphocytes that recognize previously hidden epitopes Clinical and pathological manifestations determined by nature of underlying immune response o TH1 responses – destructive macrophage-rich inflammation and production of antibodies that cause tissue damage by activating complement and binding Fc receptors o TH17 responses underlie inflammatory lesions dominated by neutrophils as well as monocytes Autoimmune diseases show substantial clinical, pathologic, and serologic overlaps, so precise phenotypic classification difficult Systemic Lupus Erythematosus Vast array of autoantibodies, particularly ANAs Acute or insidious in onset; chronic remitting and relapsing, often febrile, illness characterized principally by injury to skin, joints, kidney, and serosal membranes Antibodies recognize diverse nuclear and cytoplasmic components of cell; not organ or species specific o Some directed against cell surface antigens of blood els ANAs directed against nuclear antigens grouped into o Antibodies to DNA o Antibodies to histones o Antibodies to nonhistone proteins bound to RNA o Antibodies to nucleolar antigens ANAs detected by indirect immunofluorescence; sensitive (positive in virtually every SLE patient) not specific (pts w/other autoimmune diseases frequently positive) o Homogeneous (diffuse) nuclear staining – antibodies to chromatin, histones, and occasionally ds DNA o Rim (peripheral) staining – antibodies to ds DNA o Speckled pattern – presence of uniform or variable-sized speckles; least specific (presence of antibodies to non-DNA nuclear constituents) o Nucleolar pattern – few discrete spots of fluorescence in nucleus and represents antibodies to RNA; most often in patients w/systemic sclerosis Generic ANAs – bind variety of nuclear antigens (DNA, RNA, and proteins) Antibodies to ds DNA and Smith (Sm) antigen diagnostic SLE; don’t penetrate PM (only if cell damaged and nucleus exposed) Antiphospholipid antibodies present in 40-50% of lupus patients; directed against epitopes of plasma proteins when in complex w/phospholipids o Include prothrombin, annexin V, β2-glycoprotein I, protein S, and protein C o Antibodies against phospholipid-β2-glycoprotein complex also bind cardiolipin antigen (used in syphilis serology) and therefore, SLE patients may have false-positive syphilis test Can interfere w/clotting tests (PTT), so sometimes called lupus anticoagulant o Have hypercoagulable state (venous and arterial thromboses associated w/miscarriages and focal cerebral or ocular ischemia) o Above = secondary antiphospholipid antibody syndrome o Primary antiphospholipid syndrome – above without associated SLE Fundamental defect in SLE is failure of mechanisms that maintain self-tolerance Specific alleles of HLA-DQ locus linked to production of anti-ds DNA, anti-Sm, and antiphospholipid antibodies Some SLE patients have inherited deficiencies of early complement components; lack of complement impairs removal of circulating immune complexes by mononuclear phagocyte system, favoring tissue deposition o Deficiency of C1q results in defective phagocytic clearance of apoptotic cells Immunological factors o Failure of self-tolerance in B cells o CD4+ T cells specific for nucleosomal antigens contribute to production of autoantibodies o Nuclear DNA and RNA contained in immune complexes may activate B lymphocytes by engaging TLRs o Peripheral blood lymphocytes exposed to type I interferons (antiviral cytokines normally produced during innate immune responses to viruses) Nucleic acids engage TLRs on DCs and stimulate production of interferons (self-nucleic acids mimic microbial counterparts) o BAFF – promotes survival of B cells; increased production in SLE patients Exposure to UV light exacerbates disease in many individuals; irradiation induces apoptosis in cells and alters DNA to become immunogenic o Modulates immune response by stimulating keratinocytes to produce IL-1 (promotes inflammation) Sex hormones – frequency 10x greater in women than men in 17-55 age group; exacerbation during menses and pregnancy Drugs such as hydralazine, procainamide, and D-penicillamine induce SLE-like response Most visceral lesions caused by type III hypersensitivity LE cell – any phagocytic leukocyte that has engulfed denatured nucleus of injured cell (LE bodies); sometimes found in pericardial or pleural effusions in patients Lupus nephritis – up to 50% of pts; immune complex deposition in glomeruli, tubular or peritubular capillary BMs, or larger blood vessels o Thrombi in glomerular capillaries, arterioles, or arteries; often associated w/antiphospholipid Ig’s o Class I (minimal mesangial), class II (mesangial proliferative), class III (focal proliferative), class IV (diffuse proliferative), and class V (membranous) Mesangial lupus glomerulonephritis: no or slight (class I) to moderate (class II) increase in both mesangial matrix and number of mesangial cells o Granular mesangial deposits of immunoglobulin and complement always present Focal proliferative glomerulonephritis (class III); lesions may be segmental (affecting only portion of glomerulus) or global (involving entire glomerulus); glomeruli may exhibit crescent formation, fibrinoid necrosis, proliferation of endothelial and mesangial cells, infiltrating leukocytes, and eosinophilic deposits or intracapillary thrombi (correlate w/hematuria and proteinuria) Diffuse proliferative glomerulonephritis (class IV) most severe form; 35-60% of pts; proliferation of endothelial, mesangial, and sometimes epithelial cells (producing cellular crescents that fill Bowman’s space) o Hematuria and proteinuria; hypertension and mild to severe renal insufficiency common Membranous glomerulonephritis (class V) – diffuse thickening of capillary walls; 10-15% of pts; severe proteinuria or nephrotic syndrome All classes show variable amounts of mesangial deposits (mainly subepithelial in membranous); subendothelial (between endothelium and BM) in proliferative types (class III and IV) o Deposits create homogeneous thickening of capillary wall (wire-loop in light microscopy) Characteristic erythema affects malar area (butterfly) in 50% of patients o Urticaria, bullae, maculopapular lesions, and ulcerations occur o Exposure to sunlight incites or accentuates o Involved areas show vascuolar degeneration of basal layer of epidermis o Edema and perivascular inflammation in dermis o Vasculitis and fibrinoid necrosis may be prominent o Deposition of immunoglobulin and complement along dermoepidermal junction (may be present in uninvolved skin) Joint involvement – nonerosive synovitis w/little deformity Neuropsychiatric symptoms – noninflammatory occlusion of small vessels by intimal proliferation sometimes noted; due to endothelial damage by antiphospholipid antibodies Pericardial involvement in up to 50% of patients o Myocarditis (mononuclear cell infiltration) may cause resting tachycardia and electrocardiographic abnormalities o Valvular abnormalities primarily in mitral and aortic valves; diffuse leaflet thickening associated w/dysfunction (Libman-Sacks endocarditis) Warty deposits on any heart valve on either surface of leaflets o Can have coronary atherosclerosis (HTN, obesity, and hyperlipidemia more common in SLE pts) Immune complexes and antiphospholipid antibodies cause endothelial damage and promote Splenomegaly, capsular thickening, and follicular hyperplasia common features; central penicilliary arteries show concentric intimal and smooth muscle cell hyperplasia (onion-skin lesions) Pleuritis and pleural effusions affect almost 50% of pts; sometimes chronic interstitial fibrosis and secondary pulmonary HTN LE (hematoxylin) bodies in bone marrow or other organs strongly indicative of SLE Lymph nodes may be enlarged w/hyperplastic follicles or necrotizing lymphadenitis Prone to infections because of underlying immune dysfunction and treatment w/immunosuppressive drugs During acute flare-ups, increased formation of immune complexes and accompanying complement activation result in hypocomplementemia Disease exacerbatins usually treated by corticosteroids or immunosuppressive drugs Most common causes of death are renal failure and intercurrent infections Chronic Discoid Lupus Erythematosus Disease where skin manifestations mimic SLE, but systemic manifestations rare Presence of skin plaques showing varying degrees of edema, erythema, scaliness, follicular plugging, and skin atrophy surrounded by elevated erythematous border Face and scalp usually affected Disease usually confined to skin (5-10% develop multisystem manifestations after many years) Antibodies to ds DNA rarely present Immunofluorescence of skin biopsy show deposition of immunoglobulin and C3 at dermoepidermal junction Subacute Cutaneous Lupus Erythematosus Predominant skin involvement; skin rash tends to be widespread, superficial, and non-scarring Most have mild systemic Sx consistent w/SLE Strong association w/antibodies to SS-A antigen and HLA-DR3 genotype Group intermediate between SLE and lupus erythematosus localized only to skin Drug-Induced Lupus Erythematosus Develops in pts receiving hydralazine, procainamide, isoniazid, and D-penicillamine Drugs produce ANAs, but most patients don’t have Sx Multiple organs affected, but renal and CNS don’t Extremely high frequency of antibodies for histone People w/HLA-DR4 allele at greater risk of developing after administration of hydralazine Disease remits after withdrawal of drug Rheumatoid Arthritis Affects primarily joints but may involve extra-articular tissues (skin, blood vessels, lungs, and heart) Sjögren Syndrome Chronic disease characterized by dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia) resulting from immunologically mediated destruction of lacrimal and salivary glands; infiltrate of activated CD4+ T cells and some B cells (including plasma cells) Isolated disorder (sicca syndrome) or more often in association w/another autoimmune (secondary form) RA most common associated disorder 75% of pts have rheumatoid factor (antibody reactive to IgG) whether or not coexisting RA ANAs detected in 50-80% of pts Antibodies directed against 2 ribonucleoprotein antigens: SS-A (Ro) and SS-B (La) detected in 90% of pts o Pts w/high titers of SS-A antibodies more likely to have early disease onset, longer duration, and extraglandular manifestations (cutaneous vasculitis and nephritis) Weak association w/HLA-B8, HLA-DR3, DRW52, HLA-DQA1, and HLA-DQB1 loci o In pts w/anti-SS-A or anti-SS-B antibodies, specific alleles of HLA-DQA1 and HLA-DQB1 frequent o Inheritance of certain class II molecules predisposes Initiating trigger may be viral infection of salivary glands (causes local cell death and release of tissue selfantigens); in genetically susceptible, CD4+ T cells and B cells specific for self-antigens may have escaped tolerance and are able to react Viruses that serve as initiating stimuli include EBV and hepatitis C viruses o Small proportion of individuals infected w/human T-cell lymphotropic virus type 1 develop identical Sx Any exocrine gland may be involved; just prefer lacrimal and salivary o Periductal and perivascular lymphocytic infiltration lymphoid follicles w/germinal centers found ductal lining epithelial cells may show hyperplasia, obstructing ducts atrophy of acini, fibrosis, and hyalinization atrophy and replacement of parenchyma w/fat High risk for development of B cell lymphomas Corneal epithelium becomes inflamed, eroded, and ulcerated; oral mucosa atrophies w/inflammatory fissuring and ulceration; dryness and crusting of nose leads to ulcerations and perforation of nasal septum Most commonly in older women (50-60) Thick secretions accumulate in conjunctival sac Extraglandular (1/3) synovitis, diffuse pulmonary fibrosis, and peripheral neuropathy o More common in people w/high titers of anti-SS-A antibodies o Glomerular lesions extremely rare (defects of tubular function (renal tubular acidosis, uricosuria, and phosphaturia) often seen) Mikulicz syndrome – combo of lacrimal and salivary gland inflammatory involvement from any cause o Biopsy of lip to examine minor salivary glands essential for Dx of Sjögren syndrome Lymph nodes hyperplastic If reaction continues unabated, strong tendency for individual clones in population of B cells to gain growth advantage; indicative of development of marginal zone lymphoma Systemic Sclerosis (Scleroderma) Chronic disease characterized by o Chronic inflammation from autoimmunity o Widespread damage to small blood vessels o Progressive interstitial and perivascular fibrosis in throughout body Skin most commonly affected, GI tract, kidneys, heart, muscles, and lungs frequently involved In most, disease progresses to visceral involvement w/death from renal failure, cardiac failure, pulmonary insufficiency, or intestinal malabsorption Diffuse scleroderma (widespread skin involvement at onset w/rapid progression and early visceral involvement) Limited scleroderma (skin involvement confined to fingers, forearms, and face; late visceral invovlement) o Some pts develop combo of calcinosis, Raynaud’s phenomenon (episodic vasoconstriction of arteries in extremities), esophageal dysmotility, sclerodactylly, and telangiectasia (CREST) syndrome Autoimmune response, vascular damage, and collagen deposition contribute to ultimate tissue injury CD4+ T cells accumulate in skin and release cytokines that activate inflammatory cells and fibroblasts o Secreted cytokines (TGF-β and IL-13) stimulate transcription of genes that encode collagen and ECM proteins in fibroblasts o Other cytokines recruit WBCs and propagate chronic inflammation Virtually all patients have ANAs that react w/variety of nuclear antigens o Anti-Scl 70: directed against DNA topoisomerase I; 10-20% of pts; highly specific; more likely to have pulmonary fibrosis and peripheral vascular disease o Anticentromere antibody: 20-30% of pts; tend to have CREST syndrome or limited cutaneous form Microvascular damage early in course; intimal proliferation; capillary dilation w/leaking and destruction o Nailfold capillary loops distorted early in course; disappear later o Signs of increased endothelial activation and injury (vWF) and increased platelet activation (increase in circulating platelet aggregates) Repeated cycles of endothelial injury followed by platelet aggregation lead to release of PDGF and TGF-β that trigger perivascular fibrosis o Vascular smooth muscle cells increase expression of adrenergic receptors o Widespread narrowing of microvasculature leads to ischemic injury and scarring Progressive fibrosis from actions of fibrogenic cytokines produced by infiltrating WBCs, hyperresponsiveness of fibroblasts to cytokines, and scarring following ischemic damage from vascular lesions Marfan syndrome – mutations in fibrillin-1 gene; some features of systemic sclerosis also seen Diffuse sclerotic atrophy of skin; begins in fingers and distal regions of UEs; extends proximaly o Edema and perivascular infiltrates of CD4+ T cells w/swelling and degeneration of collagen fibers (become eosinophilic) o Capillaries and small arteries thicken basal lamina; endothelial cell damage; partial occlusion o Increasing fibrosis of dermis, which becomes tightly bound to SQ structures; increase of compact collagen in dermis w/thinning of epidermis, loss of rete pegs, atrophy of dermal appendages, and hyaline thickening of walls of dermal arterioles and capillaries o In advanced stages, fingers have tapered, claw-like appearance w/restriction of ROM; loss of blood supply leads to cutaneous ulceration and atrophic changes in terminal phalanges (can amputate) Alimentary tract affected in 90% of patients; progressive atrophy and collagenous fibrous replacement of muscularis (most severe in esophagus); lower 2/3 of esophagus develops rubber-hose inflexibility o Dysfunction of lower esophageal sphincter gives rise to GERD o Mucosa thinned and may ulcerate; excessive collagenization of lamina propria and submucosa o Loss of villi and microvilli in small bowel cause malabsorption syndrome Inflammation of synovium w/hypertrophy and hyperplasia of synovial soft tissues early stage; fibrosis later o Joint destruction not common o Inflammatory myositis (similar to polymyositis) may develop in 10% of pts Renal abnormalities in 2/3 of patients w/systemic sclerosis; vascular lesions most prominent o Interlobular arteries show intimal thickening as result of deposition of mucinous or finely collagenous material (stains for glycoprotein and acid mucopolysaccharides) o Concentric proliferation of intimal cells; restricted to smaller vessels and not always associated w/HTN o HTN occurs in 30% of pts; 20% have malignant HTN Vascular alterations more pronounced; associated w/fibrinoid necrosis involving arterioles w/thrombosis and infarction Often die of renal failure o Proteinuria – rarely severe enough to cause nephrotic syndrome Lungs involved in more than 50% of pts; pulmonary HTN and interstitial fibrosis o Pulmonary vasospasm (secondary to pulmonary vascular endothelial dysfunction) important in HTN Pericarditis w/effusion and myocardial fibrosis w/thickening of intramyocardial arterioles; 1/3 of pts o Clinical myocardial involvement less common o Myocardial fibrosis may cause either arrhythmias or cardiac failure Raynaud’s phenomenon in virtually all patients Destruction of esophageal wall leads to atony and dilation, esp. in lower end Inflammatory Myopathies Group of disorders characterized by injury and inflammation of mainly skeletal muscles Dermatomyositis, polymyositis, and inclusion-body myositis comprise this group; may occur alone or in combo (esp. w/systemic sclerosis) Mixed Connective Tissue Disease Clinical features mixture of features of SLE, systemic sclerosis, and polymyositis Characterized by serologically high titers of antibodies to ribonucleoprotein particle-containing U1 ribonucleoprotein Modest renal involvement, but good response to corticosteroids Can evolve into classicl SLE or systemic sclerosis Complications include pulmonary HTN and renal disease resembling systemic sclerosis Polyarteritis Nodosa and Other Vasculitides Necrotizing inflammation of walls of blood vessels of immunological pathogenesis Noninfectious vasculitis – not due to direct infection of blood vessel wall (as occurs in wall of abscess); any type of vessel involved