Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Copy-number variation wikipedia , lookup
Frameshift mutation wikipedia , lookup
Gene expression profiling wikipedia , lookup
Genetic testing wikipedia , lookup
Human genetic variation wikipedia , lookup
Population genetics wikipedia , lookup
X-inactivation wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Genome evolution wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Gene desert wikipedia , lookup
Point mutation wikipedia , lookup
Nutriepigenomics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Gene nomenclature wikipedia , lookup
Gene expression programming wikipedia , lookup
Helitron (biology) wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Medical genetics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Genetic engineering wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Public health genomics wikipedia , lookup
Gene therapy wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Genome (book) wikipedia , lookup
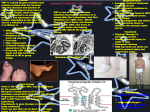
Charcot Marie Tooth Disease Essay, Research Paper Charcot-Marie-Tooth Disorder Charcot-Marie-Tooth Disorder (CMT) is the most common type of hereditary motor and sensory neuropathy (HMSN), occurring in one of every 2500 births. The mean age of onset of clinical symptoms is 12.2 7.3 years. Severity of the disorder varies among the individual and among the subtypes of CMT. Subtypes are distinguishable by testing the nerve conduction velocity (NCV), muscle biopsies, and protein levels in cerebrospinal fluid. Three different subtypes have been identified, fittingly called CMT I, CMT II, and CMT III (or Dejerine-Sottas disease). (Epstein 1993) CMT I shows a fully penetrant phenotype. The onset of clinical symptoms is usually seen by the age of two. Common features of this disorder include pes cavus, a deformity of the foot characterized by an abnormally high arch and hyperextension of the toes, which gives the foot a claw-like appearance, and hammer toes. As CMT progresses, weakness and atrophy of leg muscles occur. Areflexia occurs in the Achilles and patellar areas (absence of reflex), and later muscle degradation affects the intrinsic muscles in the hands. CMT II has a similar clinical phenotype to CMT I, but with a wider range of the age of onset and later appearance of symptoms. There is also less involvement of hand muscles. Dejerine-Sottas Syndrome (DSS or CMT III) is the rarest form of CMT. This syndrome shares clinical, electrophysiological, and pathological findings of CMT I. However, the onset of DSS is generally during infancy and the symptoms are typically more severe. The causes of CMT have been linked to autosomal dominant, autosomal recessive, x-linked, and environmental means. The largest number studies have been done on CMT-IA (an autosomal dominant form), the most common form of CMT. It is often associated with a 1.5 megabase tandem duplication of the short arm of chromosome 17 (17p12) found in approximately seventy percent of unrelated CMT I patients. It is thought that this duplication is a result of unequal crossing-over between two chromosome 17 s during meiosis. (King 1998) Studies of CMT-IA have indicated that it is a demyelinating neuropathy. The tandem duplication of chromosome 17 includes the PMP22 gene. This gene is responsible for encoding a protein expressed in the compact myelin of a peripheral nerve. The exact physical size of the duplication is unknown, but the DNA markers found within the duplication spans a distance of fourteen centimorgans on the female meiotic map and four centimorgans on the male meiotic map. (Lupski et al. 1992) It has been suggested that increased gene dosage of PMP22 is the mechanism by which DNA duplication gives rise to the CMT-IA phenotype. A study was done to test the following hypothesis: if the region duplicated in CMT-IA patients was contained entirely within the large duplication in the partial 17p trisomy patients, and the patients met electrophysiological diagnoses of CMT-IA, the gene dosage model would be supported. Cytogenetic and molecular analyses indicate that a gene dosage effect is indeed responsible for the electrophysiological phenotype associated with CMT-IA. The model of interruption of a candidate CMT-IA gene at the duplication junction can be refuted because the DNA markers are both proximal and distal to the duplication. Linkage analysis of CMT families is not consistent with two chromosome 17p loci so this rules out the possibility of two genes causing the phenotypes. (Lupski et al. 1992) This study indicates that a gene dosage effect may be responsible for other Mendelian disease phenotypes. This may allow scientists to develop therapeutic interventions targeting the gene products. PMP22 is not the only gene that has been linked to CMT. Mutations in the mpz (myelin protein zero) gene have been linked to over forty mutations that have resulted in either CMT-IB or DSS. The gene Cx32 explains the mixed CMTI/CMTII and CMTX variations of CMT. Cx32 mutations are the second most prevalent mutation found in CMT-I. Over 150 mutations have been described, including deletions, missense, nonsense, and frameshift mutations. Unlike PMP22 and mpz, the range of clinical severity is much less in males. (Warner et al. 1999) This makes genotype and phenotype correlation very difficult. With a variety of genes thought to be responsible for CMT, clinicians must rely on complex molecular methods to determine which gene is playing a role. The DNA duplication associated with CMT-IA requires FISH (fluorescence in situ hybridization) analysis of interphase nuclei. Molecular analysis using DNA markers is also used to map within the duplicated region. (Roa et al. 1996) Cytogenetic analysis of metaphase chromosomes is not enough to detect this mutation, primarily because the p arm of chromosome 17 is very short. It is for this reason that most cases of CMT are not detected until after the child is born. A case study of four patients with de novo partial duplications of 17p was investigated for neuropathological signs of CMT-IA. Two showed telltale signs of the disorder (a decreased nerve conduction velocity), while the other two had normal NCVs. Cytogenetic and FISH analysis was performed, along with molecular studies to determine whether a duplication of the PMP22 gene was present. One patient (#621) had a reduced NCV and showed an inverted duplication of 17p13.3 p11.2. In addition to patient 621, three others were studied. These individuals also had the 17p partial trisomy, a direct duplication of bands 17p11.2 p12. However, only one of these three showed a decreased NCV. Southern analyses were performed using DNA markers to identify and map the duplicated region. These studies found the PMP22 gene duplicated in those patients with a decreased nerve conduction velocity. However, patients that had the 17p trisomy with a normal NCV did not show duplication for the gene. Using RFLP analysis, it was determined that this gene was maternal in origin. (Roa et al. 1996) FISH analysis showed patients with the duplicated PMP 22 gene displaying four red signals. In contrast, patients that did not have the duplicated gene only showed two red signals. Another probe was used to provide confirmation of 17p patients that did not show the duplication of the PMP22 gene. The results showed that the FLI gene, a gene linked to Smith-Magenis syndrome, was duplicated in these patients. The results of this study confirm that the duplication of the PMP22 gene is associated with CMT-IA in cases of cytogenetic duplication of 17p. Combined cytogenetic and molecular analysis indicates the PMP22 gene maps to band 17p12. Chromosome 17 is not the only chromosome locus that has been shown to play a role in CMT. Loci can differ based on the symptoms, subtypes, and mode of inheritance. Autosomal dominant inheritance is seen in CMT I, CMT II, and CMT X. CMT X is an X-linked form of CMT occurring more often in males than females, but is considered to show a dominant inheritance pattern. CMT I can also show an autosomal recessive pattern. Below is a chart indicating inheritance pattern and chromosome location of each of the subtypes of CMT. (Warner et al. 1999) Inheritance Pattern Chromosome locus CMTI Autosomal dominant Type IA 17p11.2-p12 Type IB 1q21.1-q23q Type IC does not mark to either CMT I Autosomal Recessive 5q23-q33, 8q24, 11q23 CMT II Autosomal dominant Type IIA 1p35-p36 Type IIB 3q13-q22 Type IID 7p14 CMT X Autosomal dominant Xq13.1 CMT tends to run in families and can be passed from mother or father to child. It is hard to diagnosis cases of CMT without a family history, because symptoms are very similar to other chronic inherited or acquired neuropathies. (Murakami et al. 1996) It is also very hard to detect CMT before a child is born. This is because the chromosomal mutation only becomes obvious during FISH analysis. Unless there is a clinical reason given to specifically test for CMT, doctors usually do not look for it. It is possible, however, to identify abnormal genotypes of at risk persons for CMT. Genetic counseling of CMT families is usually limited to parents who either have the disorder themselves or families who have other children with CMT. It is the genetic counselor s responsibility to inform the parents of the risks of transmission and advise them of alternative means. If parents have genetic testing done on their unborn child and they discover that their child is carrying some disorder, they are given several options. These options include an abortion if enough time remains (pregnancy currently in the first trimester), placing the child in institutionalized care once born, or teaching and providing support to the parents about the disorder that their child will have. Since CMT is not usually diagnosed before the child is born, the genetic counselor s role is limited in these patients. They can advise the parents on the risks of having another child with CMT. In the case of CMT, genetic counselors try to discourage parents from even having children at all if the parents are known carriers of the disorder. This is because ninety-some percent of CMT cases have been linked to a genetic cause. Unfortunately, parents do not like to be told that they should not have children. Most religions believe that children are the products of a healthy marriage. When parents know the risks of transmission of CMT and have children anyway, they are basically endangering the child s welfare. This causes ethical issues to arise. Should parents be allowed to have children if they are at a higher risk of transmission of a genetic disorder? It is argued that everyone has an inalienable right to have children. (Dickenson: 1995 p. 75) On the other hand, should this right be limited in those that are known carriers of genetic diseases? Another question that is often raised is, if treatment options are available, such as gene therapy or medication, are all other concerns made void? Since CMT has a strong genetic link, it may be possible to use somatic cell gene therapy when it becomes available. The ultimate achievement of somatic cell gene therapy would be to replace a defective gene with a normal one and thus provide a normal gene product. (Rosenberg and Iannaccone 1995) Should the child be subjected to treatments simply because their parents ignored all the warnings about the risks? Scientists in Japan have created a solution to the problem of X-linked disorders such as Duchenne s muscular dystrophy. They use a preimplantation sexing method for exclusion of male embryos (50% of which have the genetic disease trait) as an option for parents at risk (Ijichi and Ijichi: 1996, p. 198) Should parents even have children if they are using such measures to avoid having a child with a genetic disease? Since CMT can arise through X-linked traits, this treatment is a possibility for parents who are carriers and wish to have children. Neurogenetics has shifted focus from clinical descriptions and classifications to a molecular science that has been successful in identifying specific gene alterations in a significant number of major neurogenetic diseases. It is hoped that these disorders can be treated with metabolic gene therapy to stabilize or reverse progression. It has often been questioned if at-risk persons would be interested in knowing their risks, and a recent estimate has indicated that the approximate size of the United States market for testing healthy people for CMT is 100,000 families. (Rosenberg and Iannaccone 1995) However, there are issues concerning insufficient quality control over genetic testing laboratories. So far there has not been conclusive evidence indicating quality control problems resulting in false positives. I feel that genetic counselors and doctors should offer alternatives to parents who wish to have children. Adoption is an excellent choice. There are a number of healthy children in foster homes who need a family. Instead of risking a transmission of a genetic illness, parents should consider giving a home to a child who needs one. If the child has already been conceived and parents learn that he or she has a disease, they should seek counseling and outside help rather than give up and consider an abortion. Once they know of their risk to pass the disease onto their other children, they should consider the consequences of having more children. Even if gene therapy is an option, it is a very experimental and risky procedure. Risks might outweigh the benefits, especially if the risks include a premature death of the child. Even though causes of CMT have been determined and a gene has been isolated, a cure has yet to be found. Life expectancy of these patients is fairly average. CMT is a progressive disorder; symptoms and behaviors are expected to be more readily display themselves over time. Researchers are currently working on gene therapy as a possible cure. A cure is foreseen in the near future due to advances in genetics. Technology learned from other neurogenetic diseases can be applied to CMT. This makes the task of finding a cure that much easier. I am personally in favor of advanced genetic testing of myself, my family, and any children that I might have. Sources Dickenson, D. (1995). Carriers of Genetic Disorder and the Right to Have Children. Acta Geneticae Medicae et Gemellologiae 44, 75-80. Epstein, Charles J., ed. The Phenotypic Mapping of Down Syndrome and Other Aneuploid Conditions: Proceedings of a National Down Syndrome Society Conference. New York: WileyLiss, p. 7, 10, 187-205, 1993. Ijichi, S., and Ijichi, N. (1996). Preimplantation gender determination and X-linked diseases: ethical controversy. Lancet 348, 198-199. King, P.H., et al. (1998). Charcot-Marie-Tooth phenotype produced by a duplicated PMP22 gene as a part of a 17p trisomy-translocation to the X chromosome. Clinical Genetics 54, 413-416. Lovelace, Robert E., and Howard K. Shapiro, ed. Charcot-Marie-Tooth Disorders: Pathophysiology, Molecular Genetics, and Therapy. New York: Wiley-Liss, 1990. Lupski, J. R., et al. (1992). Gene dosage is a mechanism for Charcot-Marie-Tooth disease type 1A. Nature Genetics 1, 29-33. Murakami, T., et al. (1996). Charcot-Marie-Tooth Disease and Related Inherited Neuropathies. Medicine 75, 233-250. Roa, B. B., et. al. (1996). Duplication of the PMP22 gene in 17p partial trisomy patients with Charcot-Marie-Tooth type-1A neuropathy. Human Genetics 97, 642-649. Rosenberg, Roger N., and Susan T. Iannaccone (1995). The prevention of Neurogenetic Disease. Archives of Neurology 52, 356-362. Valentijn, Linda J., and Frank Bass (1998). Genetic Basis of Peripheral Neuropathies. Progress in Brain Research 117, 249-264. Warner, Laura E. et al. (1999) Hereditary Peripheral Neuropathies: Clinical Forms, Genetics, and Molecular Mechanisms. Annual Review of Medicine 50, 263-275.