Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of TRPV1 antagonists wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
CCR5 receptor antagonist wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug design wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
NMDA receptor wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Toxicodynamics wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug interaction wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Nicotinic agonist wikipedia , lookup
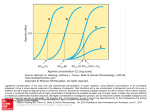
Principles of Pharmacology: Pharmacodynamics Dennis Paul, Ph.D. [email protected] Learning Objectives: Understand the theoretical basis of drugreceptor interactions. Understand the determinants and types of responses to drug-receptor interactions. Know the four major families of receptors. Define potency and efficacy. Understand how to compare drug potency and efficacy. Understand the consequences of receptor regulation Understand measures of drug safety. Biochemistry: L+S LS Biochemistry: L+S LS (Langmuir equation) Pharmacology: L+R LR Biochemistry: L+S LS Pharmacology: L+R LR Response Pharmacodynamics Drugs: Chemical agents that interact with components of a biological system to alter the organism’s function. Examples of such components, sites of drug action, are enzymes, ion channels, neurotransmitter transport systems, nucleic acids and receptors. Many drugs act by mimicking or inhibiting the interactions of endogenous mediators with their receptors Receptors: Regulatory proteins that interact with drugs or hormones and initiate a cellular response – Ion channels – G-protein coupled receptors – Receptor-enzymes – Cytosolic-nuclear receptors Act as transducer proteins – Receptor-effector signal transduction – Post-receptor signal transduction provides for amplification of the signal Ligand-gated Ion Channels Ca++ Ca++ Na+ Mg++ Ca++ Mg++ K+ Na+ Ligand-gated Ion Channels Mg++ Ca++ Na+ K+ Na+ Na+ Ca++ Na+ Na+ Ca++ Na+ Na+ Mg++ G-protein coupled receptors NH3+ COOH- g a b GTP G-protein coupled receptors NH3+ COOH- g a b GDP Receptor-enzyme Catalytic site Receptor-enzyme Catalytic site Cytosolic-Nuclear receptors Cytosolic-Nuclear receptors Classical Receptor Occupancy Theory Ka L+R LR Kd Stimulus Response L: Ligand (Drug) R: Receptor LR: Ligand-Receptor Complex Ka: Association rate constant Stimulus: initial effect of drug on receptor Properties of drugs Affinity: The chemical forces that cause the drug to associate with the receptor. Efficacy: The extent of functional change imparted to a receptor upon binding of a drug. Properties of a biological system Potency: Dose of drug necessary to produce a specified effect. – Dependent upon receptor density, efficiency of the stimulus-response mechanism, affinity and efficacy. Magnitude of effect: Asymptotic maximal response – Solely dependent upon intrinsic efficacy. – Also called efficacy. Determinants of Response Intrinsic Efficacy (ε): Power of a drug to induce a response. Number of receptors in the target tissue. Spare receptors Some tissues have more receptors than are necessary to produce a maximal response. – Dependent on tissue, measure of response and intrinsic efficacy of the drug. Active vs Inactive states Receptors in an active state initiate cell signaling. For any cell, there is an equilibrium between receptors in active and inactive states. The inactive state usually predominates. Each state has its own affinity. Classification of a drug based on drug-receptor interactions: Agonist: Drug that binds to receptors and initiates a cellular response; has affinity and efficacy. Agonists promote the active state. Antagonist: drug that binds to receptors but cannot initiate a cellular response, but prevent agonists from producing a response; affinity, but no efficacy. Antagonists maintain the active-inactive equilibrium. cont. Partial agonists: Drug that, no matter how high the dose, cannot produce a full response. Inverse agonist: Drug that binds to a receptor to produce an effect opposite that of an agonist. Stabilizes receptors in the inactive state. Graded dose-response curves Individual responses to varying doses Concepts to remember: – Threshold: Dose that produces a justnoticeable effect. – ED50: Dose that produces a 50% of maximum response. (EC50: blood concentration that produces a 50% of max response) – Ceiling: Lowest dose that produces a maximal effect. Dose-response curve 100 Response 80 60 40 20 0 0 200 400 Dose 600 800 1000 Dose-response curve 100 Response 80 60 40 20 0 0.1 1 10 Dose 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 100 80 60 40 20 0 0.1 = Agonist 1 10 100 1000 10000 Dose-response curve Ceiling 100 Response 80 60 ED50 40 Threshold 20 0 0.1 1 10 Dose 100 1000 10000 Full vs Partial agonists 100 Full Agonist % Effect 80 60 40 20 Partial Agonist 0 0.1 1 10 Dose 100 1000 10000 Full vs Partial agonists These terms are tissue dependent on – Receptor density – Cell signaling apparatus – Other receptors that are present – Drug history Partial agonists have both agonist and antagonist properties. Inverse Agonist % Effect 100 80 Full agonist 60 40 Partial agonist 20 0 -20 Inverse agonist -40 Dose Relative Potency 100 B A Effect 80 60 40 20 0 0.1 1 10 100 Dose 1000 10000 Relative Potency 100 A B Effect 80 60 40 20 0 0.1 1 10 100 Dose 1000 10000 Relative Potency =ED50B/ED50A 320/3.2=100 Relative Efficacy 100 Relative Efficacy 80 60 40 20 0 0.1 1 10 100 1000 10000 Antagonists Competitive: Antagonist binds to same site as agonist in a reversible manner. Noncompetitive: Antagonist binds to the same site as agonist irreversibly. Allosteric: Antagonist and agonist bind to different site on same receptor Physiologic: Two drugs have opposite effects through differing mechanisms 120 100 80 60 40 20 0 -10.5 = Agonist -10 -9.5 -9 -8.5 = Antagonist -8 -7.5 -7 -6.5 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 120 100 80 60 40 20 0 -11 = Agonist -10 -9 = Antagonist -8 -7 -6 Competition 1200 Effect 1000 800 600 ID50 or IC50 400 200 0 -11 -10 -9 -8 log [antagonist] -7 -6 = Agonist = Antagonist = Agonist = Antagonist = Agonist = Antagonist = Agonist = Antagonist = Agonist = Antagonist = Agonist = Antagonist = Agonist = Antagonist Competitive antagonists 100 A B C 10 100 1000 Response 80 60 40 20 0 0.1 1 Dose 10000 Noncompetitive antagonists 100 A Response 80 60 B 40 C 20 0 0.1 1 10 Dose 100 1000 10000 Allosteric and Physiologic antagonists Response can be irregular Allosteric Antagonism Allosteric Antagonism Allosteric Antagonism Allosteric Antagonism Allosteric antagonists 1 100 A Response 80 60 40 20 0 0.1 1 10 Dose 100 1000 10000 Allosteric antagonists 2 100 A Response 80 60 B 40 C 20 0 0.1 1 10 Dose 100 1000 10000 Quantal Dose-Response Curves Also known as concentration-percent or dose-percent curves Used when the dose of a drug to produce a specified effect in a single patient is measured (individual effective dose or concentration.) The percent of subjects responding at a dose is plotted. Percent Responders Quantal Dose-Response Curves 100 90 80 70 60 50 40 30 20 10 0 1 3.2 10 32 100 Dose 320 1000 3200 Percent Responders Cumulative Quantal DoseResponse Curves 120 100 80 60 40 20 0 1 3.2 10 32 100 Dose 320 1000 3200 Percent Responders Cumulative Quantal DoseResponse Curves 120 100 80 60 40 20 0 1 10 100 Dose 1000 10000 Receptor regulation Reduced responsivity: Chronic use of an agonist can result in the receptor-effector system becoming less responsive – eg. alpha-adrenoceptor agents used as nasal decongestants Myasthenia gravis: decrease in number of functional acetylcholine nicotinic receptors at the neuromuscular junction. Receptor regulation Increased responsivity: Chronic disuse of a receptor-effector system can result in an increased responsiveness upon reexposure to an agonist. – – – Denervation supersensitivity at skeletal muscle acetylcholine nicotinic receptors Thyroid induced upregulation of cardiac beta-adrenoceptors Prolonged use of many antagonists (pharmacological as well as functional) can result in receptor upregulation Receptor Upregulation Most receptors are internalized and degraded or recycled with age and use. Antagonists slow use-dependent internalization Inverse agonists stabilize the receptor in the inactive state to prevent internalization. The cell continues to produce receptors. Desired vs undesired effects: Indices of drug safety. Safety Index Therapeutic Index “Potency means nothing. I can always give a bigger pill.” J. Hunter Safety index: LD1/ED99 ED99 100 80 Sleep Death 60 40 LD1 20 10 0K 10 K 1K 10 0 10 1 -20 0. 1 0. 00 01 0. 00 1 0. 01 0 Therapeutic index: LD50/ED50 100 80 Sleep Death 60 40 20 10 0K 10 K 1K 10 0 10 1 -20 0. 1 0. 00 01 0. 00 1 0. 01 0 Safety Index vs. Therapeutic Index 100 Percent Effect 80 Desired Effect 60 Lethality Therapeutic Index 40 20 Safety Index ED50 0 1 10 ED99 100 Dose LD1 1000 LD50 10000 100000