Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Vectors in gene therapy wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gene expression profiling wikipedia , lookup
Genome evolution wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Epigenomics wikipedia , lookup
Gene expression programming wikipedia , lookup
Epigenetics in learning and memory wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Designer baby wikipedia , lookup
Cancer epigenetics wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Genome (book) wikipedia , lookup
Epigenetics of depression wikipedia , lookup
X-inactivation wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Down syndrome wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Oncogenomics wikipedia , lookup
Microevolution wikipedia , lookup
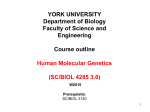
Molecular genetics of Rett syndrome and clinical spectrum of MECP2 mutations Mona D. Shahbaziana and Huda Y. Zoghbia,b,c Rett syndrome, a neurodevelopmental disorder that is a leading cause of mental retardation in females, is caused by mutations in the X-linked gene encoding methyl-CpG-binding protein 2 (MeCP2). MECP2 mutations have subsequently been identified in patients with a variety of clinical syndromes ranging from mild learning disability in females to severe mental retardation, seizures, ataxia, and sometimes neonatal encephalopathy in males. In classic Rett syndrome, genotype-phenotype correlation studies suggest that X chromosome inactivation patterns have a more prominent effect on clinical severity than the type of mutation. When the full range of phenotypes associated with MECP2 mutations is considered, however, the mutation type strongly affects disease severity. MeCP2 is a transcriptional repressor that binds to methylated CpG dinucleotides throughout the genome, and mutations in Rett syndrome patients are thought to result in at least a partial loss of function. Abnormal gene expression may thus underlie the phenotype. Discovering which genes are misregulated in the absence of functional MeCP2 is crucial for understanding the pathogenesis of this disorder and related syndromes. Curr Opin Neurol 14:171±176. # 2001 Lippincott Williams & Wilkins. Departments of aMolecular and Human Genetics and bPediatrics, and cHoward Hughes Medical Institute, Baylor College of Medicine, Houston, Texas, USA Correspondence to Huda Y. Zoghbi, Departments of Molecular and Human Genetics and Pediatrics, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030, USA Tel: +1 713 798 6523; fax: +1 713 798 8728; e-mail: [email protected] Current Opinion in Neurology 2001, 14:171±176 Abbreviations Dnmt1 DNA methyltransferase 1 GFAP glial fibrillary acidic protein HDAC1 and 2 histone deacetylases 1 and 2 ICF immunodeficiency, centromere instability and facial anomalies MBD methyl-CpG-binding domain MeCP2 methyl-CpG-binding protein 2 mRNA messenger RNA RLGS-M restriction landmark genomic scanning using methylation-sensitive endonuclease RTT Rett syndrome TFIIB Transcription Factor IIB TRD transcriptional repression domain XCI X chromosome inactivation # 2001 Lippincott Williams & Wilkins 1350-7540 Introduction Rett syndrome (RTT) was ®rst recognized as a distinct clinical entity by Andreas Rett in 1966. It affects approximately 1 : 15 000 females [1]. This review highlights the discoveries that have provided insight into the cause of Rett syndrome, emphasizing the information gained since the discovery of the causative gene. Neurological deficits in Rett syndrome Fifteen years after Hagberg described it as `a very peculiar condition' [1], Rett syndrome continues to be a subject of interest because of its unusual neurodevelopmental course and constellation of clinical features. Classic Rett syndrome ®rst appears after six to eighteen months of apparently normal development. Neurodevelopment is then interrupted, and affected girls begin to regress intellectually. They lose acquired skills involving language and purposeful hand use, and are generally characterized as mentally retarded with autistic features [2]. One particularly interesting symptom of RTT is the replacement of hand skills with purposeless and stereotypic hand movements. Around the age of three years, microcephaly becomes apparent, as a result of a deceleration in head growth [2]. Gait ataxia and apraxia are usually evident before the ®fth year [3] and other features of Rett syndrome, such as apnea and hyperpnea, seizures, scoliosis, and growth retardation, are common [3]. Rett syndrome genetics The early observation that Rett syndrome occurred exclusively in females led to the hypothesis that it was due to a dominant mutation on the X chromosome that was lethal in hemizygous males [2]. Since affected females rarely reproduce and familial cases are extremely rare (less than one percent), it took years of research to generate data supporting such a genetic mechanism. The rarity of familial cases and the small size of the families made conventional linkage analysis dif®cult, if not impossible. An alternative strategy was to exclude regions of the X chromosome by evaluating polymorphic markers for concordance/discordance in affected individuals of familial RTT [4±7]. These efforts culminated in the exclusion of most of the X chromosome, leaving only Xq28 [8±10]. Although this substantially narrowed the candidate region to about 10 megabases of DNA, the causative gene remained elusive, since Xq28 is 171 172 Developmental disorders extremely gene-dense. Given the list of neuronally expressed genes in the region, probably few would have predicted that mutations would be found in the widelyexpressed gene encoding methyl-CpG-binding protein 2 (MeCP2) [11 .]. Biology of methyl-CpG-binding protein 2 The discovery of the causative gene for Rett syndrome obviously answered an important question, but it also opened up many more. Fortunately, MeCP2 had already been identi®ed as a protein that, through its methyl-CpG-binding domain (MBD), bound to DNA oligonucleotides containing at least one methylated CpG pair [12,13]. Consistent with this ®nding, the in-vivo distribution of MeCP2 paralleled the broad distribution of 5-methyl-cytosine on the chromosomes, encompassing pericentromeric heterochromatin and the euchromatic arms of mouse and rat chromosomes [12]. Nan et al. [14] demonstrated that MeCP2 was suf®cient to repress transcription from a promoter when the upstream sequences were methylated. Upon the demonstration that the transcriptional repression domain (TRD) of MeCP2 associated with the Sin3A corepressor complex, which contains histone deacetylases 1 and 2 (HDAC1 and 2), the mechanism of repression was clari®ed [15]. HDACs cause chromatin to condense by removing acetyl groups from histones, and thereby make the DNA inaccessible to the transcriptional machinery. Recent evidence has demonstrated that the TRD also interacts with Transcription Factor IIB (TFIIB), a component of the basal transcriptional machinery, suggesting an additional and direct effect in transcriptional interference [16]. The messenger RNA (mRNA) encoding MeCP2 is present in a wide variety of tissues in humans and mouse [17], but quantitative immunoblot analysis has shown that levels are approximately six times higher in the brain [12]. In situ studies of the developing and fully differentiated mouse brain demonstrate expression throughout the brain, with elevated levels in the olfactory bulb and hippocampus [17]. Combining the functional data with expression studies, it appears that MeCP2 binds to a multitude of methylated chromosomal sites and modi®es chromatin structure in a way that represses transcription. Additionally, the broad expression pattern of MeCP2 suggests that the protein is essential for chromatin modi®cation/silencing in many tissues. These conclusions, however, are dif®cult to reconcile with the largely neurological phenotype of Rett syndrome. The function of MeCP2, therefore, is likely to be much more complex. Spectrum of MECP2 mutations and connection to protein function As a result of sequence analysis of DNA from Rett syndrome cases, 78 unique MECP2 mutations have been identi®ed in exons 3 and 4 of the gene, which contain a majority of the coding region (Fig. 1) [11 .,18 .,19,20 .± 22 .,23,24 .,25 .,26,27]. MECP2 mutations have been identi®ed in 75-90% of sporadic cases and approximately 50% of familial cases. Interestingly, C to T transitions at eight different CpG dinucleotides in the gene account for almost 70% of these mutations. The described mutations suggest that RTT is due to a loss of protein function. For example, one mutation (Q19X) introduces an extremely early stop codon [25 .], which is likely to be a null allele. Additional nonsense mutations have been found in the MBD (Y141X), between the MBD and TRD (R168X, Q170X, and R198X), and within the TRD (R255X, K256X, R270X, and R294X) [11 .,18 .,19,20 .±22 .,23,24 .,26,27]. Frameshift mutations that give rise to premature stop codons also occur throughout the gene. A partial loss of MeCP2 function cannot be excluded, however, because premature stop codons within the last exon may not lead to nonsensemediated mRNA decay [28]. Therefore, the possibility still exists that premature stop codons within exon 4 may produce a truncated form of the protein that retains partial function. A truncated protein that retains the MBD, for instance, may still be able to bind to methylCpG nucleotides and may, by virtue of solely binding upstream of potential promoter regions, at least partially interfere with transcription. Whether Rett syndrome is caused by both null and hypomorphic alleles remains an interesting question. Missense mutations have been identi®ed in regions of the gene encoding the MBD, TRD, and C-terminus of the protein (Fig. 1). Three of the mutations within the MBD (R106W, R133C, and F155S) have been shown to reduce binding to methylated DNA by more than 100fold [29 .]. It remains to be shown whether missense mutations in the TRD reduce interactions with the Sin3A complex and whether mutations in the Cterminus, which enhances the binding of MeCP2 to nucleosomal DNA [30], decrease interactions with components of the nucleosome. Phenotypic spectrum of MECP2 mutations Since the MECP2 gene is X-linked and subject to X chromosome inactivation (XCI) [31], one would expect XCI patterns to have a potent in¯uence on phenotype. Indeed, it has long been recognized that in addition to classic Rett syndrome, there are milder forms of the syndrome that lack certain signs [1], as well as very severe forms that lack the period of normal development and cause hypotonia and infantile spasms [32]. As more mutation analysis is performed, the classi®cation of these Rett syndrome and MECP2 mutations Shahbazian and Zoghbi 173 Figure 1. Summary of mutations found in the MECP2 gene T158M L124F R106Q R106W P101H P101L P101R P101T D97E D156E F155I F155S P322A P322L R306C R306H P302A P302H P302L P302R P152R A140V* S134C R133C P225R 375delC Q19X 378–2 splice 167–168delCC 407del507 258 –259delCA +ins8 411delG 1036del154 1037del154 1038del154 1053ins10 +1141del55 1096del101 1098del70 +1182del7 1116del84 1130del69 1147del170 K256X 1152del41 1152del44 785del34 1157del41 803delG 1157del44 1158del10 807delC 1159del43 848del388 1163del26 849del388 1163del35 R294X 1165del26 1193insT 914del259 1194insT Q406X* R168X R198X Q170X 602insG 620insT 654del4 677insA Y141X 695delG 696delC 706delG 754del4 R255X Coding Untranslated MBD TRD X487C 1364insC Exons 2 through 4 of MECP2, containing the entire coding region, are illustrated. Missense mutations are shown above the genomic structure, whereas nonsense and frameshift mutations are displayed below. Mutations include those found in Rett syndrome (unmarked) as well as nonsyndromic mental retardation (marked with asterisks). different clinical entities as variants of one syndrome is now being veri®ed at a genetic level [33]. In fact, it is becoming evident that MECP2 mutations produce an even wider range of phenotypes than previously suspected (Table 1). Two of the most interesting ®ndings about the variability of clinical features resulting from MECP2 mutations have come from the analysis of familial cases of RTT, four of which have been described. Four members of one family bore the 803delG mutation: a female with mild neurological and learning de®cits and skewed XCI, her daughter and sister with RTT, and her son with neonatal encephalopathy, who died at seventeen months [18 .]. In a second family, an asymptomatic mother with completely skewed XCI, her daughter with RTT, and her son with neonatal encephalopathy all shared the T158M mutation [34]. Although DNA was not available from another boy who died neonatally, the R168X mutation was found in his three sisters with RTT and in his normal mother with skewed XCI [18 .]. In a fourth family, the R106W mutation was identi®ed in one sister and a half-sister of a boy with neonatal encephalopathy, for whom DNA was not obtained, but not in their normal mother, presumed to be germline mosaic [11 .]. Although the MECP2 mutation was con®rmed in only two of the four male neonatal encephalopathy cases, it appears that the same mutations that cause classic Rett syndrome in females can also cause neonatal encephalopathy in males, whereas females can be spared part or all of the neurological impairments through skewed XCI. Although it is possible that cells expressing mutant MeCP2 are selected against, this seems unlikely, since the same mutation occurs in carrier females and in their affected daughters. Therefore, the skewed XCI pattern in carrier females is likely to be due to chance. MECP2 mutations are not always lethal in males: Clayton-Smith et al. [35] describe a boy with many features of Rett syndrome, including loss of speech, 174 Developmental disorders Table 1. Spectrum of phenotypes resulting from mutations in MECP2 Phenotype Females: Classic Rett syndrome Mild forms of Rett syndrome Preserved speech variant Mild neurological and learning deficits Mild mental retardation, microcephaly, speech difficulties, gait abnormalities None apparent None apparent Males: Neonatal encephalopathy with respiratory dysfunction Loss of speech, seizures, ataxia, scoliosis, decreased head circumference, limited hand use Severe mental retardation, impaired language development, slow movements, resting tremors Mental retardation, seizures, ataxia, absence of language Mutations Other genetic modifiers Missense, Nonsense, Frameshift Missense, Nonsense, Frameshift Balanced X chromosome inactivation Favorably skewed X chromosome inactivation Missense Balanced X chromosome inactivation Missense, Nonsense, Frameshifta Very late truncation Favorably skewed X chromosome inactivation Balanced X chromosome inactivation Missense, Nonsense, Frameshiftb Frameshift (early truncation) Somatic mosaicism Missense Very late truncation a Mutations found in asymptomatic carrier females. bMutations demonstrated in two cases and presumed in two others based on mutations identified in female siblings. seizures, decreased head circumference, scoliosis, and ataxia. Mutation analysis showed that this male probably survived due to somatic mosaicism for a MECP2 mutation (167-168delCC), such that some of his cells had the mutant allele and some had a wild-type allele, much like females with random X chromosome inactivation. Genotype-phenotype correlations in Rett syndrome and related disorders To determine whether different types of mutations in MECP2 can account for the variability of phenotypes in Rett syndrome, several groups have conducted genotypephenotype correlation studies. Amir et al. studied patients with balanced XCI and classi®ed the genotypes as either missense or truncation mutations; they found no correlation between genotype and overall clinical severity score but did detect increased respiratory abnormalities and decreased cerebrospinal ¯uid levels of homovanillic acid in patients with truncations and increased incidence of scoliosis in patients with missense mutations [20 .]. Neither Bienvenu et al. [21 .] nor Huppke et al. [24 .] found any signi®cant correlation between mutation type and clinical features. Nevertheless, Cheadle et al. found that truncating mutations led to a more severe overall phenotype than missense mutations, and that late truncations correlated with a less severe outcome than early truncations [22 .]. It thus appears that in classic Rett syndrome, the correlation between mutation type and phenotype is minimal, with XCI being a major determinant of clinical manifestations. There appears to be a stronger correlation between genotype and phenotype when neurological disorders other than Rett syndrome are considered. Two groups have screened cases of X-linked mental retardation for mutations. Orrico et al. [36 .] found an A140V mutation in four brothers with severe mental retardation and in their mother and sister, who had mild mental retardation, microcephaly, speech dif®culties, and gait abnormalities. Since these males survived into adulthood and the females had balanced XCI patterns [36 .], this mutation may impair the function of MeCP2 less than those causing Rett syndrome. In another study, Meloni et al. [37 .] found that two mentally retarded males had a Q406X mutation, which was also shared by two unaffected carrier females ± who, unexpectedly, showed balanced XCI patterns. The two males had delayed development and macrocephaly, but, like Rett patients, also displayed seizures, ataxia, and absence of language [37 .]. Since the males survived into adulthood and the females were normal despite balanced XCI, this mutation may be less deleterious to MeCP2 function than the A140V mutation and much less than the mutations causing Rett syndrome. Pathogenesis of Rett syndrome In view of the extensive binding pattern of MeCP2 on chromosomes, how does one explain the neuronal speci®city of Rett syndrome? One possibility might be that the higher levels of MeCP2 detected in the brain [12], particularly the hippocampus [17], signify areas where MeCP2 function is uniquely essential. This would imply that binding of MeCP2 to most methylated chromosomal regions is dispensable since, if binding of MeCP2 were indeed essential in every methylated region, the consequence of its loss would be equivalent to loss of methylation. Yet this is not the case: extensive demethylation of the mouse genome by mutation of DNA methyltransferase 1 (Dnmt1) is embryonic-lethal [38], whereas mutation of the murine Mecp2 gene is not [39]. Furthermore, mutations of another DNA methyltransferase, DNMT3B, in humans leads to a syndrome characterized by immunode®ciency, centromere instabil- Rett syndrome and MECP2 mutations Shahbazian and Zoghbi 175 ity and facial anomalies (ICF) [40,41]. In ICF syndrome, genomic methylation is only partially lost, primarily in satellites II and III of constitutive heterochromatin of chromosomes 1, 9, and 16 [41]. Since the phenotype of Rett syndrome does not include features of ICF, it appears that MeCP2 is not essential for mediating the effects of methylation of even this small subset of methylated DNA. In addition, the fact that Dnmt3bde®cient mice, which have hypomethylated minor satellite repeats in centromeric heterochromatin, also die before birth [42] provides convincing evidence for the dispensability of MeCP2 binding in these regions. MeCP2 binding may be essential only for repressing expression of a select group of genes, although the mechanism that might account for this is dif®cult to predict. These genes may be neuronal-speci®c or widely expressed but detrimental only to neuronal development when misexpressed. In support of the idea that MeCP2 might regulate only a subset of genes, the CpG islands associated with the promoters of most genes are nonmethylated, and only a subset of genes are known to be regulated by methylation (e.g., those that are either imprinted or undergo inactivation on the X chromosome). There is a tight correlation in various cell types between methylation and silencing as well as nonmethylation and expression for some genes that are regulated in a tissue-speci®c manner, such as leukosialin (CD43) [43]. Although the cause-and-effect relationship is dif®cult to prove, it is certainly possible that methylation patterns are responsible for the tissuespeci®c expression of some genes. For genes that may be methylated in neurons and silenced by MeCP2, the mutated protein could allow inappropriate expression and thereby disrupt neuronal development. It is worth noting that MeCP2 is a member of a growing family of MBD-containing proteins [44]. Like MeCP2, MBD1 has been shown to act as a transcriptional repressor and to localize to centromeric heterochromatin [45]. Another family member, MBD2, also represses transcription in vitro and, along with MBD4, colocalizes with regions of methylated satellite DNA [44,46]. With the high level of functional similarity between these proteins, it is possible that these or other comparable proteins could substitute for at least the broad, chromatin-binding role of MeCP2. Notably, no other MBD-containing protein has been shown to have as high af®nity for methyl-CpG dinucleotides as MeCP2, which can bind just a single symmetrical pair [12]. Therefore, MeCP2 may be the only family member that can silence genes regulated by low methylation density, and it may be misexpression of these genes that underlies the Rett syndrome phenotype. Another aspect of the Rett syndrome phenotype that is dif®cult to reconcile with the expression pattern of MeCP2 is the delay in the onset of overt features. One possible explanation is that the genes repressed by MeCP2 do not become methylated until later in development. Several neuronal gene promoters have, in fact, been found to undergo a developmental change in methylation. With restriction landmark genomic scanning using methylation-sensitive endonuclease (RLGS-M), Suzuki et al. [47] showed that Stac, a gene expressed primarily in brain (and at highest levels in the hippocampus, cerebellum, and inferior olive), displays a developmental change in methylation pattern in the mouse brain. In addition, the glial ®brillary acidic protein (GFAP) gene undergoes methylation during neuronal maturation in the rat brain [48]. Furthermore, when inducing differentiation with nerve growth factor, the expression of genes encoding the helix-loop-helix proteins Id1, Id2, and Id3 was reduced, but only in the presence of DNA methyltransferase activity [49]. All these examples demonstrate that neuronal maturation may require changes in expression of genes mediated by DNA methylation. Any of these genes, or other similarly regulated genes, could be targets of MeCP2 repression. Conclusion The discoveries that the MECP2 gene was mutated in Rett syndrome and in non-syndromic forms of mental retardation provide a great advance in clinical neurology. Patients with features resembling Rett syndrome, nonsyndromic mental retardation, and neonatal encephalopathy of unknown etiology can now be evaluated for MECP2 mutations. Genetic counseling can be offered to families with carrier females to reduce the risk of recurrence. It remains to be determined why mutation of the widely expressed MECP2 gene leads to a neuronal phenotype, what genes are regulated by MeCP2, and how mutations in MECP2 give rise to the characteristic features of Rett syndrome. When suitable animal models become available, addressing these perplexing issues will be possible. References and recommended reading Papers of particular interest, published within the annual period of review, have been highlighted as: . of special interest .. of outstanding interest 1 Hagberg B. Rett's syndrome: prevalence and impact on progressive severe mental retardation in girls. Acta Paediatr Scand 1985; 74(3):405±408. 2 Hagberg B, Aicardi J, Dias K, Ramos O. A progressive syndrome of autism, dementia, ataxia, and loss of purposeful hand use in girls: Rett's syndrome: report of 35 cases. Ann Neurol 1983; 14(4):471±479. 3 Trevathan E. Diagnostic criteria for Rett syndrome. The Rett Syndrome Diagnostic Criteria Work Group. Ann Neurol 1988; 23(4):425±428. 4 Archidiacono N, Lerone M, Rocchi M, et al. Rett syndrome: exclusion mapping following the hypothesis of germinal mosaicism for new X-linked mutations. Hum Genet 1991; 86(6):604±606. 5 Ellison KA, Fill CP, Terwilliger J, et al. Examination of X chromosome markers in Rett syndrome: exclusion mapping with a novel variation on multilocus linkage analysis. Am J Hum Genet 1992; 50(2):278±287. 176 Developmental disorders 6 Schanen NC, Dahle EJ, Capozzoli F, et al. A new Rett syndrome family consistent with X-linked inheritance expands the X chromosome exclusion map. Am J Hum Genet 1997; 61(3):634±641. 7 Schanen C, Francke U. A severely affected male born into a Rett syndrome kindred supports X- linked inheritance and allows extension of the exclusion map. Am J Hum Genet 1998; 63(1):267±269. 8 Sirianni N, Naidu S, Pereira J, et al. Rett syndrome: confirmation of X-linked dominant inheritance, and localization of the gene to Xq28. Am J Hum Genet 1998; 63(5):1552±1558. 9 Webb T, Clarke A, Hanefeld F, et al. Linkage analysis in Rett syndrome families suggests that there may be a critical region at Xq28. J Med Genet 1998; 35(12):997±1003. 10 Xiang F, Zhang Z, Clarke A, et al. Chromosome mapping of Rett syndrome: a likely candidate region on the telomere of Xq. J Med Genet 1998; 35(4):297± 300. 11 Amir RE, Van den Veyver IB, Wan M, et al. Rett syndrome is caused by . mutations in X linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet 1999; 23(2):185±188. This paper was the first to show that mutations in MECP2 cause Rett syndrome. 12 Lewis JD, Meehan RR, Henzel WJ, et al. Purification, sequence, and cellular localization of a novel chromosomal protein that binds to methylated DNA. Cell 1992; 69(6):905±914. 13 Nan X, Meehan RR, Bird A. Dissection of the methyl-CpG binding domain from the chromosomal protein MeCP2. Nucleic Acids Res 1993; 21(21):4886±4892. 14 Nan X, Campoy FJ, Bird A. MeCP2 is a transcriptional repressor with abundant binding sites in genomic chromatin. Cell 1997; 88(4):471±481. 15 Nan X, Ng HH, Johnson CA, et al. Transcriptional repression by the methylCpG-binding protein MeCP2 involves a histone deacetylase complex. Nature 1998; 393(6683):386±389. 16 Kaludov NK, Wolffe AP. MeCP2 driven transcriptional repression in vitro: selectivity for methylated DNA, action at a distance and contacts with the basal transcription machinery. Nucleic Acids Res 2000; 28(9):1921±1928. 17 Coy JF, Sedlacek Z, Bachner D, et al. A complex pattern of evolutionary conservation and alternative polyadenylation within the long 3'-untranslated region of the methyl-CpG-binding protein 2 gene (MeCP2) suggests a regulatory role in gene expression. Hum Mol Genet 1999; 8(7):1253±1262. 18 Wan M, Lee SS, Zhang X, et al. Rett syndrome and beyond: recurrent . spontaneous and familial MECP2 mutations at CpG hotspots. Am J Hum Genet 1999; 65(6):1520±1529. This study highlights the spectrum of phenotypes resulting from MECP2 mutations, from males with neonatal encephalopathy to unaffected female carriers. 19 Amano K, Nomura Y, Segawa M, Yamakawa K. Mutational analysis of the MECP2 gene in Japanese patients with Rett syndrome. J Hum Genet 2000; 45(4):231±236. 20 Amir RE, Van den Veyver IB, Schultz R, et al. Influence of mutation type and X . chromosome inactivation on Rett syndrome phenotypes. Ann Neurol 2000; 47(5):670±679. These authors conducted a comprehensive genotype-phenotype correlation study, taking into account X chromosome inactivation. 21 Bienvenu T, Carrie A, de Roux N, et al. MECP2 mutations account for most . cases of typical forms of Rett syndrome. Hum Mol Genet 2000; 9(9):1377± 1384. This paper identified mutations in 65% of RTT patients and found no significant correlation between mutation and phenotype. 22 Cheadle JP, Gill H, Fleming N, et al. Long-read sequence analysis of the . MECP2 gene in Rett syndrome patients: correlation of disease severity with mutation type and location. Hum Mol Genet 2000; 9(7):1119±1129. Mutation analysis in this study revealed mutations in 80% of sporadic and familial RTT cases and showed some effect of genotype on clinical severity. 23 Hampson K, Woods CG, Latif F, Webb T. Mutations in the MECP2 gene in a cohort of girls with Rett syndrome. J Med Genet 2000; 37(8):610±612. 24 Huppke P, Laccone F, Kramer N, et al. Rett syndrome: analysis of MECP2 and . clinical characterization of 31 patients. Hum Mol Genet 2000; 9(9):1369±1375. These authors found mutations in 77% of RTT patients and showed that genotype did not correlate with phenotype. 25 Kim SJ, Cook Jr EH. Novel de novo nonsense mutation of MECP2 in a patient . with Rett syndrome. Hum Mutat 2000; 15(4):382±383. This paper describes an interesting RTT case with the earliest known nonsense mutation. 26 Obata K, Matsuishi T, Yamashita Y, et al. Mutation analysis of the methylCpG binding protein 2 gene (MECP2) in patients with Rett syndrome. J Med Genet 2000; 37(8):608±610. 27 Xiang F, Buervenich S, Nicolao P, et al. Mutation screening in Rett syndrome patients. J Med Genet 2000; 37(4):250±255. 28 Carter MS, Li S, Wilkinson MF. A splicing-dependent regulatory mechanism that detects translation signals. Embo J 1996; 15(21):5965±5975. 29 Ballestar E, Yusufzai TM, Wolffe AP. Effects of Rett syndrome mutations of the . methyl CpG binding domain of the transcriptional repressor MeCP2 on selectivity for association with methylated DNA. Biochemistry 2000; 39(24):7100±7106. In vitro binding assays in this paper show that three of the Rett mutations decrease the affinity of MeCP2 for methyl-CpG. 30 Chandler SP, Guschin D, Landsberger N, Wolffe AP. The methyl-CpG binding transcriptional repressor MeCP2 stably associates with nucleosomal DNA. Biochemistry 1999; 38(22):7008±7018. 31 D'Esposito M, Quaderi NA, Ciccodicola A, et al. Isolation, physical mapping, and northern analysis of the X-linked human gene encoding methyl CpGbinding protein, MECP2. Mamm Genome 1996; 7(7):533±535. 32 Hagberg B. Clinical delineation of Rett syndrome variants. Neuropediatrics 1995; 26(2):62. 33 De Bona C, Zappella M, Hayek G, et al. Preserved speech variant is allelic of classic Rett syndrome. Eur J Hum Genet 2000; 8(5):325±330. 34 Villard L, Cardoso AK, Chelly PJ, et al. Two affected boys in a Rett syndrome family: clinical and molecular findings [In Process Citation]. Neurology 2000; 55(8):1188±1193. 35 Clayton-Smith J, Watson P, Ramsden S, Black GC. Somatic mutation in MECP2 as a non-fatal neurodevelopmental disorder in males. Lancet 2000; 356(9232):830±832. 36 Orrico A, Lam C, Galli L, et al. MECP2 mutation in male patients with non. specific X linked mental retardation. FEBS Lett 2000; 481(3):285±288. This paper describes the interesting finding that males with a missense mutation can survive to adulthood, albeit with severe mental retardation. 37 Meloni I, Bruttini M, Longo I, et al. A mutation in the Rett syndrome gene, . MECP2, causes X-linked mental retardation and progressive spasticity in males. Am J Hum Genet 2000; 67(4):982±985. These authors found a very late nonsense mutation in males with mental retardation and in an unaffected female with balanced XCI. 38 Li E, Bestor TH, Jaenisch R. Targeted mutation of the DNA methyltransferase gene results in embryonic lethality. Cell 1992; 69(6):915±926. 39 Dragich J, Houwink-Manville I, Schanen C. Rett syndrome: a surprising result of mutation in MECP2. Hum Mol Genet 2000; 9(16):2365±2375. 40 Hansen RS, Wijmenga C, Luo P, et al. The DNMT3B DNA methyltransferase gene is mutated in the ICF immunodeficiency syndrome. Proc Natl Acad Sci USA 1999; 96(25):14412±14417. 41 Xu GL, Bestor TH, Bourc'his D, et al. Chromosome instability and immunodeficiency syndrome caused by mutations in a DNA methyltransferase gene. Nature 1999; 402(6758):187±191. 42 Okano M, Bell DW, Haber DA, Li E. DNA methyltransferases Dnmt3a and Dnmt3b are essential for de novo methylation and mammalian development. Cell 1999; 99(3):247±257. 43 Kudo S, Fukuda M. Tissue-specific transcriptional regulation of human leukosialin (CD43) gene is achieved by DNA methylation. J Biol Chem 1995; 270(22):13298±13302. 44 Hendrich B, Bird A. Identification and characterization of a family of mammalian methyl-CpG binding proteins. Mol Cell Biol 1998; 18(11):6538±6547. 45 Ng HH, Jeppesen P, Bird A. Active repression of methylated genes by the chromosomal protein MBD1. Mol Cell Biol 2000; 20(4):1394±1406. 46 Ng HH, Zhang Y, Hendrich B, et al. MBD2 is a transcriptional repressor belonging to the MeCP1 histone deacetylase complex. Nat Genet 1999; 23(1):58±61. 47 Suzuki H, Kawai J, Taga C, et al. Stac, a novel neuron-specific protein with cysteine-rich and SH3 domains. Biochem Biophys Res Commun 1996; 229(3):902±909. 48 Barresi V, Condorelli DF, Giuffrida Stella AM. GFAP gene methylation in different neural cell types from rat brain. Int J Dev Neurosci 1999; 17(8):821± 828. 49 Persengiev SP, Kilpatrick DL. The DNA methyltransferase inhibitor 5azacytidine specifically alters the expression of helix-loop-helix proteins Id1, Id2 and Id3 during neuronal differentiation. Neuroreport 1997; 8(9-10):2091± 2095.