Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuronal ceroid lipofuscinosis wikipedia , lookup
Genetically modified crops wikipedia , lookup
X-inactivation wikipedia , lookup
Gene therapy wikipedia , lookup
Population genetics wikipedia , lookup
Gene desert wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Long non-coding RNA wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Essential gene wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Behavioural genetics wikipedia , lookup
Genetic engineering wikipedia , lookup
Dominance (genetics) wikipedia , lookup
Heritability of IQ wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Minimal genome wikipedia , lookup
Genome evolution wikipedia , lookup
Ridge (biology) wikipedia , lookup
History of genetic engineering wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gene expression programming wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Microevolution wikipedia , lookup
Gene expression profiling wikipedia , lookup
Genome (book) wikipedia , lookup
Designer baby wikipedia , lookup
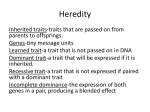
C.A. Alper Z. Awdeh Key words: major histocompatibility complex; incomplete penetrance; autoimmunity; polygenic disease Acknowledgments: This work was supported by grants HL-29583 and AI-14157 from the National Institutes of Health. The authors especially thank Dr. Charles E. Larsen for his thoughtful comments. They also thank Drs. Devendra P. Dubey, Keith Crawford, Gabriel Uko, John Xu and Fred S. Rosen for their valuable suggestions. Incomplete penetrance of MHC susceptibility genes: prospective analysis of polygenic MHC-determined traits Abstract: We propose an approach to understanding incomplete penetrance of disease susceptibility genes as a method of studying the underlying mechanisms of polygenic diseases. Incomplete penetrance is the failure of genetically susceptible individuals to exhibit a trait. We define as baseline penetrance that which occurs in genetically identical (monozygotic) twins of an index subject with a major histocompatibility complex (MHC)-associated disease or trait. We consider two mechanisms for incomplete baseline penetrance: an extrinsic (environmental) trigger and an intrinsic stochastic, gene-associated process. The latter can be detected for dominant expression because susceptibility genes in homozygotes (with their two intrinsic triggers) will be up to twice as frequently penetrant as those in heterozygotes. The extent of MHC and non-MHC gene contribution determines differences between baseline penetrance and apparent penetrance in MHC-identical sib pairs, sib pairs in general and MHC-identical unrelated individuals. Inheritance patterns in families do not reveal modes of inheritance of incompletely penetrant polygenic MHC-determined traits. A method is proposed to study such traits prospectively in persons presumed to be homozygous, heterozygous or non-carrying for susceptibility genes by determining trait expression in homozygotes, heterozygotes or non-carriers of trait-associated conserved extended MHC haplotypes. The method provides direct estimates of apparent penetrance rates, modes of genetic determination, and, if the trait is dominant, the origin of penetrance. When applied to dominant MHC susceptibility gene-determined immunoglobulin deficiencies in two populations, the ratios of affected haplotype homozygotes to heterozygotes near 2.0 were consistent with an intrinsic mechanism for baseline penetrance acting on the MHC susceptibility genes. Authors’ affiliations: C.A. Alper1,2, Z. Awdeh1 1 The Center for Blood Research, Boston, Massachusetts, USA, 2 Department of Pediatrics, Harvard Medical School, Boston, Massachusetts, USA Correspondence to: Dr. Chester A. Alper The Center for Blood Research 800 Huntington Avenue Boston MA 02115–6303 USA Tel: π1 617 278 3333 Fax: π1 617 278 3493 e-mail: alper/cbr.med.harvard.edu The burgeoning of molecular biological techniques over the past several decades has produced incredible advances in our understanding of human genetics. Despite this, progress in unraveling Received 18 November 1999, revised, accepted for publication 15 May 2000 Copyright c Munksgaard 2000 Tissue Antigens . ISSN 0001-2815 Tissue Antigens 2000: 56: 199–206 Printed in Denmark . All rights reserved many complex (polygenic) diseases, particularly those with major histocompatibility complex (MHC) involvement, has been slow. There have been enormous efforts to identify and to understand the role of MHC and non-MHC susceptibility genes in autoimmune 199 Alper & Awdeh : Incomplete penetrance of MHC genes diseases such as type 1 diabetes. Nevertheless, for most, we have etrance, as measured by disease concordance in monozygotic twins, yet to even identify unequivocally the responsible genes, let alone is 30 to 50% (3). This rate would presumably apply to all fully understand how they cause disease. At least part of the problem is susceptible persons in the population in general. Apparent pen- incomplete penetrance of susceptibility genes. etrance in MHC-identical sibs of patients is on the order of 15%, in Incomplete penetrance in its historic and broadest sense is the sibs in general is 5 to 6%, in parents or children is 3%, and in failure of some individuals who carry a susceptibility gene marker persons homozygous or doubly heterozygous for the diabetes-as- to express the trait (disease, phenotype, function) in question. For sociated genetic markers HLA-DR3 and/or DR4 is about 3 to 5% example, among Caucasian patients with type 1 diabetes, a classic (2). HLA-associated disease, there is an increase in the frequency of These descending rates of apparent penetrance are characteristic HLA-DR3 and DR4 and particularly of HLA-DR3/DR4 hetero- of polygenic disease and reflect the descending frequencies of MHC zygotes. Nevertheless, most Caucasians with these HLA types do and non-MHC susceptibility genes in these groups. A monozygotic not have diabetes. twin of a patient has the same complete set of susceptibility genes Incomplete penetrance is one of the elements of the ‘‘geneticist’s as the patient, no matter how many susceptibility loci there are. An nightmare’’ (1) that characterizes many MHC-determined autoim- MHC-identical sib of a patient has the necessary MHC susceptibility mune diseases and phenomena. It confounds any direct segregation genes but may or may not have the necessary non-MHC susceptibil- or linkage analysis because over 90% of affected persons have no ity genes. All family members have a higher frequency of MHC and affected family members (2). non-MHC susceptibility genes than the general population because We believe that new methods of theoretic genetic analysis to the family was ascertained through a patient who has all of them. complement the rapid accumulation of molecular findings are A patient’s sibs in general have a lower rate than MHC-identical necessary for understanding the mechanisms of polygenic diseases. sibs because MHC susceptibility is not assured. Similarly, in a child In this paper, we shall analyze the elements of penetrance in MHC- or parent of a patient, one allele at each susceptibility locus has a associated disorders, separating the contributions of non-MHC sus- frequency equivalent to the background population frequency. In ceptibility genes from the baseline penetrance observed in monozy- summary, baseline penetrance is the frequency with which a mono- gotic twin pairs. We will then explore possible mechanisms of base- zygotic twin of an affected individual has the trait. Apparent pen- line penetrance, including an external environmental trigger and an etrance varies according to the group of individuals specified and intrinsic random process affecting the susceptibility gene rather reflects both baseline penetrance and the frequencies of all suscepti- than the whole subject. From these considerations, we will develop bility genes in that group. a prospective approach to determine the mode of inheritance and apparent penetrance in unrelated subjects homozygous, heterozygous and non-carrying for conserved extended MHC haplotypes known or suspected to carry susceptibility genes. Finally, data for Penetrance and concordance immunoglobulin deficiencies studied in this way will be analyzed Although it is usual to equate penetrance with concordance rates to show that, for dominant traits, the ratio of affected homozygotes for an MHC-determined trait in monozygotic twin pairs, this is true to heterozygotes supports an intrinsic, MHC gene-based mechanism only if one identifies the pairs through one affected member (4). In for baseline penetrance. essence, one uses the affected twin to determine that the other twin is genetically completely susceptible. One then determines the prevalence of trait expression in the second twins as a group. This Baseline and apparent penetrance is the same as the rate of concordance for trait expression in the It is important to distinguish two aspects of penetrance. The first approach to MHC-susceptible persons. For example, if one wishes is penetrance that is ‘‘baseline’’ as manifested by trait (disease) con- to know the concordance rate in sibs MHC-identical (by descent) to cordance rate in monozygotic (genetically identical) twins. The other the patient, one uses the patient to define MHC susceptibility. Ap- is ‘‘apparent’’ penetrance that is observed in some defined group of parent penetrance in this sib group is the same as concordance for subjects such as persons in the general population with genetic pairs of patients and their MHC-identical sibs. In similar fashion, markers for the trait or defined first-degree relatives of a person one can use the fixity of DNA on MHC susceptibility gene-bearing with the trait. This distinction is easily illustrated by MHC-marker conserved extended haplotypes among random unrelated people to family studies of type 1 diabetes (2). In that disorder, baseline pen- study trait expression, as we shall see below. 200 Tissue Antigens 2000: 56: 199–206 pairs ascertained through an affected twin. One can extend this Alper & Awdeh : Incomplete penetrance of MHC genes Mode of genetic determination genetic determination. One might also hope that some different To explore methods of study of incompletely penetrant polygenic into the mechanism of baseline penetrance. method of analysis than is currently available might provide insight MHC-determined phenomena, we need first to consider some basic genetic aspects of such situations. For traits determined recessively by an MHC susceptibility gene, only homozygotes for these genes Retrospective approaches or closely linked marker genes will express the trait. If there is one Most MHC allele-association studies have been retrospective in the such MHC allele (or marker), only homozygotes for the allele or sense that patients ascertained for a disease or trait are treated as a marker are susceptible. If there is more than one, homozygotes for population and analyzed for the frequency-distributions of MHC al- each such allele or marker as well as heterozygotes for any pair of leles in comparison with an ethnically matched healthy control popu- susceptibility alleles or markers will be MHC-susceptible. To be lation. From family studies of patients, haplotypes, including con- fully susceptible for the trait in question, all other (non-MHC) sus- served extended haplotypes and their fragments, can be recognized ceptibility gene requirements must also be met in an aggregate sus- with certainty (5–10). Moreover, a set of control MHC haplotypes, ceptibility genotype with at least one susceptibility allele at each those not occurring in any patient in the family, which we call family locus for a dominant trait and two for a recessive trait. Population control haplotypes (11), can be obtained. One can test statistically for penetrance is determined by the ratio of affected individuals (in any differences in frequency in patient and control haplotypes or general or with a specified MHC genotype) to all persons or to those populations and one can calculate an odds ratio for any marker or with this genotype in a population. For a trait determined by a whole haplotype. Except as noted below, such studies provide infor- dominantly expressed MHC susceptibility gene, both homozygotes mation about neither mode of inheritance nor penetrance. and heterozygotes for MHC susceptibility genes are susceptible but, There are two main currently available retrospective approaches again, non-MHC susceptibility genes must also be present in correct to decide the mode of genetic determination of traits caused by dose for the individual to be genetically susceptible. partially penetrant MHC susceptibility genes. One can analyze affected sib pairs (12). If the trait and its genetic markers are rare, The inadequacy of family studies in a recessive disorder all or most sib pairs will be identical for the The high population frequency of susceptibility genes in polygenic order in which one parent carries a susceptibility gene, they need MHC-associated phenomena and diseases is at least as important share one marker only and the sibs will be MHC haploidentical or as incomplete baseline penetrance in obscuring the genetic express- MHC identical in equal proportions. Since many of the traits (dis- ion of MHC-determined traits in family studies. For fully penetrant eases) of interest are relatively common and susceptibility genes are susceptibility genes that alone determine the trait, the patterns of very common, however, such clear-cut results are usually not ob- inheritance within a family are distinctive for rare dominant and tained. For example, in type 1 diabetes, about 55% of affected sib rare recessive genes. The rare dominant gene D causes disease in pairs are MHC identical, about 38% are haploidentical and about all three generations with half of people at risk for inheriting it (i.e., 7% have no MHC haplotypes in common (13). This distribution all those who carry it) expressing the trait. In contrast, a rare reces- does not fit dominant inheritance but is actually consistent with sive susceptibility gene in a monogenic disease is inherited by and recessive inheritance (14). The sharing of only one MHC haplotype expressed in 25% of sibs of a patient. or the sharing of no haplotypes is not due to incomplete penetrance marker or markers on both chromosomes. In a rare dominant dis- These patterns break down when susceptibility genes or their but rather to the common occurrence of unaffected MHC susceptibil- markers are common. Fig. 1A shows how the pattern produced by ity gene homozygous parents. Such parents usually do not have a dominant gene is completely mimicked by the presence of multiple disease because they lack non-MHC genes in proper dosage or, even independent examples of fully penetrant recessive d genes. For in- if they have them, the composite susceptibility genotypes may not completely penetrant susceptibility genes, this problem is exacer- be penetrant. bated, as is seen in Fig. 1B and 1C, where affected persons happen The second retrospective approach is to analyze the homozygote- to be present in two generations, as well as among sibs, for common heterozygote distribution of marker alleles in a population of unre- or rare dominant and common recessive susceptibility genes at ap- lated but ethnically similar persons with the trait (patients) (15). If proximately 50% penetrance. there is a marker that is common among patients and the suscepti- It is clear that methods of analysis other than examination of bility gene determines the trait in a recessive fashion, the distri- inheritance patterns in families must be used to define modes of bution of homozygotes, heterozygotes and non-carriers of that Tissue Antigens 2000: 56: 199–206 201 Alper & Awdeh : Incomplete penetrance of MHC genes Fig. 1. A) A hypothetical family with four independent examples of a common recessive susceptibility gene d. Although expression is recessive (only dd persons have the trait), the pattern of ‘‘inheritance’’ in the family is identical to that of a rare dominant gene. B) A possible pattern of expression of the approximately 50% penetrant dominant susceptibility gene D. Black symbols represent persons with trait expression, gray symbols those with impenetrant susceptibility genotypes. Expression is both in sibs and in two generations. C) A possible pattern of expression of the recessive 50% penetrant susceptibility gene d if genotypes are as shown in (A). Expression is both in sibs and in two generations and the pattern of expression is identical to that shown in (B). marker should fit the Hardy-Weinberg equilibrium. This method by transfection of cells in vitro or rendering inbred strains trans- works perfectly if the marker is the susceptibility allele or if the genic for or devoid of the gene in question. These have proved to marker allele is always on the same haplotype as the susceptibility be fruitful in the exploration of the role of HLA-B27 in ankylosing allele in the population (shows absolute positive linkage disequilib- spondylitis (18) and of HLA class I proteins as targets for natural rium or is part of a completely conserved extended haplotype or its killer (NK) cells (19). fragment). This is largely true of the BF*F1 MHC marker for type 1 diabetes (16). In a second approach, described here, one can analyze for a suspected MHC-determined trait in individuals known to be homo- On the other hand, if the disease is dominantly determined, only zygous, heterozygous or non-carriers of MHC susceptibility genes. the gene on one chromosome is needed and the frequency of alleles In this respect, associated conserved extended haplotypes and their on the other chromosome will reflect the background for that ethnic fragments are extremely useful and analogous to the MHC in syn- group (15, 10). The distributions of HLA-B27 in ankylosing spondy- geneic and recombinant mice. Because of the fixity of DNA within litis (15) and HLA-DR4 in Jewish patients with pemphigus vulgaris the MHC of the extended haplotypes, all or nearly all independent (10) have been shown to fit dominant genetic determination based instances of a trait-associated extended haplotype in a population on such analyses. Because half of first-degree relatives of patients (affected or not) carry the same susceptibility genes. By analyzing with pemphigus vulgaris have low levels of the pemphigus anti- populations of persons homozygous, heterozygous or non-carrying body, formal segregation and linkage analysis were possible and for a known susceptibility extended haplotype for expression of a provided strong corroborative evidence for dominant class II region trait, one can decide if the trait is dominantly or recessively deter- MHC-linked inheritance for this trait (17). Unfortunately, this ability mined. to detect expression of the trait in asymptomatic carriers is unusual For example, it was concluded retrospectively from population among autoimmune diseases. It would be helpful to have other ap- studies of nonresponders to the HBsAg vaccine (20) that there was proaches to the study of polygenic, MHC-controlled phenomena in- an increased frequency of persons (including homozygotes) with the volving partially penetrant genes. extended haplotype [HLA-B8, SC01, DR3]. This suggested recessive determination of the nonresponse. In prospective studies, unrelated The prospective approach homozygotes and heterozygotes for [HLA-B8, SC01, DR3] were im- Animal and in vitro models have been used to test prospectively zygotes were nonresponders whereas the heterozygotes produced whether one or another marker is a susceptibility or protective allele anti-HBs, with no overlap in antibody levels. Family studies con- 202 Tissue Antigens 2000: 56: 199–206 munized with standard courses of HBsAg vaccine (21). The homo- Alper & Awdeh : Incomplete penetrance of MHC genes firmed that the anti-HBs response was dominant and the failure to environmental trigger for autoimmune phenomena and disease, it respond was recessive and strongly MHC linked (22). Thus, the affects genetically susceptible individuals to the same degree. This [HLA-B8, SC01, DR3] haplotype usually lacks an immune response argument is strongly supported by the observation that dizygotic gene for HBsAg. The response is dominant and the nonresponse is twins of patients with type 1 diabetes have precisely the same con- recessive. cordance rate for disease as sibs in general (25). In other words, the In our proposed analysis, homozygotes for the susceptibility entire difference in rates of disease between sibs and monozygotic gene-bearing haplotype have two susceptibility genes, one on each twins must be due to differences in susceptibility gene frequency. chromosome, whereas heterozygotes have only one, if the back- Differences in environmental triggers cannot be responsible for the ground frequency of the susceptibility gene on all other haplotypes difference (although environmental factors may, of course, affect the is low. If baseline penetrance is 100% and the trait is monogenic rate of baseline penetrance). The consequence of this view is that and recessive, all homozygotes, but no heterozygotes or non-carriers baseline penetrance acts in any genetic model as a mathematical will express the trait (i.e. Mendelian inheritance will hold). If base- multiplier that can be applied to all genetically susceptible individ- line penetrance is less than 100% but detectably above zero or if uals in the population, whether related or not. For example, if 10% more than one gene is required for susceptibility, the observed lower of a specified group of subjects is genetically susceptible and base- prevalence of affected homozygotes reflects the population pen- line penetrance is 50%, 5% will be affected. etrance of the susceptible genotype (heterozygotes and non-carriers An alternative to an environmental trigger determining whether will still be substantially unaffected). If the trait is dominantly ex- or not the trait will be manifest in a genetically susceptible person pressed, both homozygotes and heterozygotes but few non-carriers (Fig. 2A for the dominant situation, but also applicable to recessive will be affected. Again, incomplete baseline penetrance and the re- traits) is an ‘‘intrinsic’’ event in a susceptibility gene, a kind of on- quirement for a number of non-MHC genes for trait expression will off switch (Fig. 2B, shown only for the dominant case). This would not change which group of subjects is affected. presumably be set during embryogenesis and would behave as a stochastic process, much as radioactive decay is intrinsic to certain Mechanisms of incomplete baseline penetrance: environmental or intrinsic? isotopes. In this view, if the intrinsic process were influenced by environmental factors, the latter would affect all susceptibles in the same way and to the same extent. Classically, the non-genetic (‘‘environmental’’) portion of incomplete There is an important conceptual difference between an environ- penetrance has been defined by concordance rates for the trait in mental trigger and an intrinsic on-off switch basis for baseline pen- monozygotic twin pairs ascertained because one twin expresses the etrance. The trigger acts on the whole organism, but the intrinsic trait. Commonly invoked to explain this aspect of incomplete pen- switch acts at the gene level. This is shown in Fig. 2 for the domi- etrance is some environmental factor, particularly viral infection. nant case. Implicit in the trigger mechanism is that a genetically This explanation has often been extended to explain the lower ap- susceptible person is converted to expression of the trait by ex- parent penetrance in MHC-identical sibs than in monozygotic twins posure to something such as a pathogen, an immunogen or an aller- by the unstated assumption that there is a larger difference in the gen. In dominant expression of susceptibility genes, the two mech- environments of sibs than of twins. Because many of the diseases anisms predict different apparent penetrances in homozygotes and with incomplete penetrance are characteristically not manifest at heterozygotes. For the external triggering mechanism (Fig. 2A), the birth, the notion of an environmental triggering event is attractive. apparent penetrance per person in homozygotes and heterozygotes However, recent studies of persons at high risk for type 1 diabetes for marker susceptibility genes should be the same, since the en- provide strong support for the onset of abnormalities many years vironmental effect should trigger trait expression whether the sub- before overt disease develops (23, 24). Therefore, it is conceivable ject has one or two susceptibility alleles. The ratio of affected homo- that some of these are, in fact, present at birth or earlier in individ- zygotes to affected heterozygotes will remain 1 no matter what the uals destined later to have frank disease. baseline penetrance or the requirement for non-MHC susceptibility Another reason for considering an environmental trigger for genes. MHC-associated diseases with incomplete penetrance is the fact that If penetrance is externally triggered and genetic expression is most are autoimmune. The trigger may be exposure to a foreign recessive, any person with two copies of the susceptibility gene will antigen with high similarity to self antigens and thus capable of express the trait (if the other susceptibility genes are present in the breaking immunologic tolerance to self antigens, such as to the b correct number) if properly triggered by the external agent or event. cells of the pancreas in type 1 diabetes. In our view, if there is an In intrinsic penetrance of a recessive susceptibility gene, only homoTissue Antigens 2000: 56: 199–206 203 Alper & Awdeh : Incomplete penetrance of MHC genes plex. Homozygotes with both genes turned on, as well as those with only one gene turned on, may express the trait. For an apparent intrinsic penetrance p, the frequency of affected homozygotes will be p2π2p(1–p) (or affected homozygotes with two expressed genes (p2)πaffected homozygotes with only one expressed gene (2p(1–p)). For example, at an apparent penetrance of 0.2, determined from trait expression in haplotype heterozygotes, haplotype homozygotes with both susceptibility genes expressed will constitute 0.2¿0.2, or 0.04, of all homozygotes studied. Haplotype homozygotes with only one expressed gene, on the other hand, will constitute 2p(1–p) or, in our example, 0.2 (expressed)¿0.8 (non-expressed)¿2 (since either chromosome can be expressed) or 0.32 of all homozygotes studied. Thus, for a penetrance of 0.2, 0.36 (0.04π0.32) of haplotype homozygotes will be affected and the ratio of affected homozygotes to affected heterozygotes will be 0.36/0.20 or 1.80. Another and mathematically equivalent way of looking at the same problem is to note that penetrance in the homozygote with two susceptibility genes is ideally 2¿p. This needs to be ‘‘corrected’’ by subtracting those individuals (p2) in whom both genes are activated (2p–p2). 2p–p2 is simply a rearranged form of p2π2p(1–p). Fig. 2. Diagrammatic representation of extrinsic and intrinsic expression of a partially penetrant dominant gene D in homozygous (DD) and heterozygous (ND) individuals, shown as circles. Extrinsic expression (A) is shown as an arrow mediated by a trigger and penetrance is a rate per person. Intrinsic expression (B) is shown by an activated (blackened) gene and an arrow. In this model, the rate of expression is per gene or haplotype, with a person manifesting the trait if one or both susceptibility genes are ‘‘activated.’’ Note that for the extrinsic model, the ratio of affected homozygotes to affected heterozygotes is 1 (3:3 in this example). In contrast, in the intrinsic model there are more affected homozygotes than affected heterozygotes (5:3 in the example given). Fig. 3 shows the ratio of affected homozygotes to heterozygotes in relation to intrinsic penetrance. If baseline penetrance is 100%, the ratio is 1, Mendelian inheritance holds and all homozygotes and heterozygotes with susceptibility genes are affected. In the dominant intrinsic model, the process is stochastic and, at low penetrances, the homozygote with two susceptibility alleles has nearly twice the opportunity for expression and therefore should be nearly zygous individuals with activation of the gene on both chromosomes will manifest the trait. Thus, both mechanisms produce the same end result and there is no obvious way to distinguish which mechanism is operative. On the other hand, if the susceptibility gene is dominant and penetrance is intrinsic (Fig. 2B), the rate of trait expression in homozygotes and heterozygotes will differ, since the homozygote with two susceptibility genes has a greater chance (up to two-fold) of the intrinsic switch being turned on. For dominant genetic determination, trait expression (apparent penetrance or p) in susceptibility haplotype heterozygotes is equivalent to prevalence of the trait in this group of subjects. This follows from the fact that heterozygotes have only one susceptibility gene that is either on or off. The per person prevalence is the same as the per chromosome apparent penetrance. In haplotype homozygotes, the situation is more com- 204 Tissue Antigens 2000: 56: 199–206 Fig. 3. The ratio of affected homozygotes to heterozygotes for a partially penetrant dominant susceptibility gene in relation to penetrance based on the intrinsic mechanism. Note that at very low penetrance, the ratio of affected homozygotes to affected heterozygotes approaches 2, whereas if penetrance is 1, the ratio is 1 (Mendelian inheritance). Alper & Awdeh : Incomplete penetrance of MHC genes twice as often affected as the heterozygote. The requirement for other hand, IgD and IgG3 deficiency occurred in both homozygotes non-MHC genes will have no affect on this ratio since their fre- and heterozygotes at apparent penetrances of 0.37 and 0.20 for IgD quency should be the same in randomly selected MHC homozygotes, and 0.30 and 0.17 for IgG3 deficiency, consistent with dominant heterozygotes and non-carriers. Affected heterozygotes, of course, inheritance. Ratios of affected homozygotes to affected hetero- have only one expressed susceptibility gene and the rate at which zygotes were thus 1.8 and 1.7, respectively, remarkably close to they are affected equals the apparent penetrance rate in this group those predicted by the formula given above for intrinsic penetrance. of subjects. Thus, a test of the mechanism for penetrance is the ratio In a study of Basques and [HLA-B18, F1C30, DR3] (27), the only of the fraction of prospectively ascertained affected homozygotes for deficiency was in IgD, present in unrelated homozygotes and hetero- a dominant trait-associated extended haplotype to that of affected zygotes with apparent penetrances of 0.37 and 0.19, for a ratio of heterozygotes. 1.9. This suggests that, for these traits, the intrinsic model of base- For recessive expression, if p!decimal fraction of all susceptibil- line penetrance applies. As stated previously, since subjects were ity genes that are expressed (as above), and 1–p!the fraction of grouped solely on the basis of homozygosity, heterozygosity or non- non-expressed susceptibility genes, p2π2p(1–p) describes the fre- carrying of [HLA-B8, SC01, DR3] or [HLA-B18, F1C30, DR3], it is quency of subjects with ‘‘activated’’ susceptibility genes. However, reasonable to assume that the frequencies of non-MHC susceptibil- since trait expression can only occur when both chromosomes have ity genes are the same in all three groups. Therefore, baseline pen- activated genes, the term 2p(1–p) drops out because subjects with etrance is probably intrinsic for the MHC susceptibility genes on only one activated gene do not express the trait. Apparent pen- these haplotypes. etrance is the square root of the frequency of the trait in haplotype The prospective genetic analysis of MHC-determined traits out- homozygotes. Thus, without more information, the external trigger lined here is powerful and, if the trait is dominantly expressed, can and intrinsic mechanisms for recessive gene expression are indis- provide evidence for the mechanism of baseline penetrance. It has tinguishable. an additional advantage in that, by studying subjects of specified Our model proposes a simple and precise mechanism for higher genetic makeup, the relationship between phenotype heterogeneity penetrance in dominant susceptibility gene homozygotes than het- and specific susceptibility haplotypes can be explored. Although erozygotes. It should be recognized that the actual mode of genetic the analysis is only helpful in testing the mechanism of baseline expression may be more complicated than that outlined. Although penetrance in the dominant situation, it may be that the intrinsic other mechanisms might also predict higher expression in homozy- mechanism is operative in MHC-recessive diseases, such as type 1 gotes, we prefer the simpler explanation. diabetes. This has important implications for unraveling the identity, nature, and function of MHC genes involved in susceptibility to autoimmune disease, including type 1 diabetes. Moreover, by the Applications prospective selection of individuals with informative fragments of When this analysis was applied to immunoglobulin deficiencies de- arose from ancient crossovers, localization of these genes can be termined by the conserved extended haplotype [HLA-B8, SC01, greatly facilitated. In work in progress, this fragment approach is DR3] (26), IgA deficiency and IgG4 deficiency were found essenti- being used to localize MHC susceptibility genes for the immuno- ally only in homozygotes, suggesting recessive inheritance. On the globulin deficiencies. susceptibility gene-bearing extended haplotypes that presumably References 1. Neel JV. Diabetes mellitus – a geneticist’s nightmare. In: Creutzfeldt W, Köbberling J, Neel JV, eds. The genetics of diabetes mellitus. Berlin: Springer-Verlag, 1977: 1– 11. 2. Raffel LJ, Scheuner MT, Rimoin DL, Rotter JI. Diabetes mellitus. In: Rimoin DL, Connor JM, Pyeritz RE, eds. Emery and Rimoin’s principles and practice of medical genetics. 3rd edition. New York: Churchill Livingstone, 1997: 1401–40. 3. Barnett AH, Eff C, Leslie RDG, Pike DA. Diabetes in identical twins: a study of 200 pairs. Diabetologia 1981: 20: 87–93. Tissue Antigens 2000: 56: 199–206 205 Alper & Awdeh : Incomplete penetrance of MHC genes 4. Allen G. Meaning of concordance and discordance in estimation of penetrance and gene frequency. Am J Hum Genet 1952: 4: 155–72. 5. Awdeh ZL, Raum D, Yunis EJ, Alper CA. Extended HLA/complement allele haplotypes: Evidence for T/t-like complex in man. Proc Natl Acad Sci U S A 1983: 80: 259–63. 6. Blumenthal M, Marcus-Bagley D, Awdeh Z, Johnson B, Yunis EJ, Alper CA. HLA-DR2, [HLA-B7, SC31, DR2], and [HLA-B8, SC01, DR3] haplotypes distinguish subjects with asthma from those with rhinitis only in ragweed pollen allergy. J Immunol 1992: 148: 411–6. 7. Alper CA, Fleischnick E, Awdeh Z, Katz AJ, Yunis EJ. Extended major histocompatibility complex haplotypes in patients with gluten-sensitive enteropathy. J Clin Invest 1986: 79: 251–6. 8. Degli-Esposti MA, Andreas A, Christiansen FT, Schalke B, Albert E, Dawkins RL. An approach to the localization of the susceptibility gene for generalized myasthenia gravis by mapping recombinant ancestral haplotypes. Immunogenetics 1992: 35: 355–64. 9. Ahmed AR, Katri K, Yunis EJ et al. Major histocompatibility complex susceptibility genes for dermatitis herpetiformis compared with those for gluten-sensitive enteropathy. J Exp Med 1993: 178: 2067– 75. 10. Ahmed AR, Yunis EJ, Khatri K et al. Major histocompatibility complex haplotype studies in Ashkenazi Jewish patients with pemphigus vulgaris. Proc Natl Acad Sci U S A 1990: 87: 7658–62. 206 11. Raum D, Awdeh Z, Yunis EJ, Alper CA, Gabbay KH. Extended major histocompatibility complex haplotypes in type I diabetes mellitus. J Clin Invest 1984: 74: 449–54. 12. Cudworth AG, Woodrow JC. Evidence for HL-A-linked genes in ‘‘juvenile’’ diabetes mellitus. Br Med J 1975: 3: 133–5. 13. Payami H, Thomson G, Motro U, Louis EJ, Hudes E. The affected sib method. IV. Sib trios. Ann Hum Genet 1985: 49: 303–14. 14. Alper CA, Dubey DP, Awdeh Z. A simple estimate of the general population frequency of the MHC susceptibility gene for autoimmune polygenic disease. Exp Clin Immunogenet 2000: 17: in press. 15. Thomson G, Bodmer W. The genetic analysis of HLA and disease association. In: Dausset J, Svejgaard A, eds. HLA and disease. Copenhagen: Munksgaard, 1977: 84–93. 16. Raum D, Awdeh Z, Alper CA. BF types and the mode of inheritance of insulindependent diabetes mellitus. Immunogenetics 1981: 12: 59–74. 17. Ahmed AR, Mohimen A, Yunis EJ et al. Linkage of pemphigus antibody to the major histocompatibility complex in healthy relatives of patients. J Exp Med 1993: 177: 419–24. 18. Hammer RE, Malka SD, Richardson JA, Tang J-P, Taurog JD. Spontaneous inflammatory disease in transgenic rats expressing HLA-B27 and human b2m: An animal model of HLA-B27-associated human disorders. Cell 1990: 63: 1099–112. 19. Storkus WJ, Salter RD, Alexander J et al. Class I-induced resistance to natural killing: Identification of nonpermissive residues in HLA-A2. Proc Natl Acad Sci U S A 1991: 88: 5989–92. Tissue Antigens 2000: 56: 199–206 20. Craven DE, Awdeh ZL, Kunches LM et al. Nonresponsiveness to hepatitis B vaccine in health care workers. Results of revaccination and genetic typings. Ann Intern Med 1986: 105: 356–60. 21. Alper CA, Kruskall MS, Marcus-Bagley D et al. Genetic prediction of nonresponse to hepatitis B vaccine. N Engl J Med 1989: 321: 708–12. 22. Kruskall MS, Alper CA, Awdeh Z, Yunis EJ. Marcus-Bagley D. The immune response to hepatitis B vaccine in man: inheritance patterns in families. J Exp Med 1992: 175: 495–502. 23. Bonifacio E, Bingley PJ, Shattock M et al. Quantification of islet-cell antibodies and prediction of insulin-dependent diabetes. Lancet 1990: 335: 147–9. 24. Rewers M, Norris JM, Eisebarth GS et al. Beta cell autoantibodies in infants and toddlers without IDDM relatives: diabetes autoimmunity study in the young (DAISY). J Autoimmun 1996: 9: 405–10. 25. Kaprio J, Tuomilehto J, Koskenvuo M et al. Concordance for type 1 (insulindependent) and type 2 (non-insulindependent) diabetes mellitus in a population-based cohort of twins in Finland. Diabetologia 1992: 35: 1060–7. 26. Alper CA, Marcus-Bagley D, Awdeh Z et al. Prospective analysis suggests susceptibility genes for deficiencies of IgA and several other immunoglobulins on the [HLA-B8, SC01, DR3] conserved extended haplotype. Tissue Antigens 2000: 20: 216– 20. 27. Calvo B, Castaño L, Marcus-Bagley D, Awdeh Z, Alper CA. The [HLA-B18, F1C30, DR3] conserved extended haplotype carries a susceptibility gene for IgD deficiency. J Clin Immunol 2000: 20: 216– 20.