Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Microneurography wikipedia , lookup
Neural coding wikipedia , lookup
Metastability in the brain wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Time perception wikipedia , lookup
Animal echolocation wikipedia , lookup
Sound localization wikipedia , lookup
Single-unit recording wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Sensory cue wikipedia , lookup
Perception of infrasound wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Psychophysics wikipedia , lookup
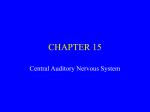
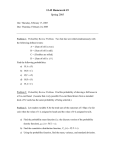
26 Brainstem Auditory Evoked Potentials Jacob R. Berger and Andrew S. Blum Summary Brainstem auditory evoked potentials (BAEPs) are electrical field potentials generated by stimulation of the auditory pathways. With repetitive auditory stimulation, reproducible electrical potentials can be elicited and recorded from scalp electrodes. These waves are generated by specific brain regions and occur at predictable intervals. Clinically, this neurophysiological property is useful to evaluate the integrity of auditory pathways (plus, by extension, neighboring CNS structures) and to localize defective transmission. This chapter summarizes the methodology and clinical application of BAEPs in the investigation of disorders affecting auditory pathways and the surrounding brainstem. Key Words: Acoustic nerve; cerebellopontine angle; hearing; intraoperative monitoring; latency; midbrain; pons. 1. INTRODUCTION Brainstem auditory evoked potentials (BAEPs) are electrical field potentials generated by stimulation of the auditory pathways. With repetitive auditory stimulation, reproducible electrical potentials can be elicited and recorded from scalp electrodes. Differences in electrical potential between active and reference electrodes are displayed graphically as a function of time after the auditory stimulus. These waves are generated by specific brain regions and occur at predictable intervals. Clinically, this neurophysiological property is useful to evaluate the integrity of auditory pathways (plus, by extension, neighboring CNS structures) and to localize defective transmission. 2. ANATOMY OF AUDITORY PATHWAYS AND CORRELATION WITH BAEP GENERATORS To accurately interpret BAEP waveforms, a working knowledge of auditory pathway anatomy and physiology is important. The auditory pathway starts in the cochlea. Vibrations from sound waves cause hydrostatic pressure changes that are sensed by hair cells in the organ of Corti. Hair cells communicate with bipolar neurons that have cell bodies in the cochlea. These neurons project to the pontomedullary junction via the acoustic nerve. After synapsing in the ventral (low-frequency tones) or dorsal (high-frequency tones) cochlear nuclei in the rostral, lateral medulla, second-order neurons project to ipsilateral and contralateral superior olivary nuclei. Note that acoustic information is bilaterally represented at this point onward throughout the auditory system. Neurons in the superior olive then project From: The Clinical Neurophysiology Primer Edited by: A. S. Blum and S. B. Rutkove © Humana Press Inc., Totowa, NJ 475 476 Berger and Blum Fig. 1. Normal BAEP waveforms. These waveforms are from a 30-yr-old woman undergoing a work-up for possible multiple sclerosis. She had no auditory complaints. The top two channels represent results after left ear stimulation and the bottom two channels after right ear stimulation. Recording montages are indicated. Each study was performed in duplicate. Note the replicable BAEP waveforms, numbered I to V, as described in the text. Waveform latencies are measured for each and interwave latencies are derived including I to III, III to V, and I to V intervals. These are then compared with normative values. These BAEPs are normal and symmetric, side-to-side. through the lateral lemniscus in the pontine tegmentum to the inferior colliculus. The inferior colliculus projects to the medial geniculate nucleus of thalamus, which projects forward to Heschl’s gyrus (superior temporal gyrus), the primary auditory cortex. BAEPs are made up of a sequence of stereotyped waveforms; five well-recognized waves are observed, numbered I to V (Fig. 1). Two later-appearing waves (VI and VII) are less reliable and of limited clinical value. These waveforms, elicited by auditory stimulation, are generated by specific structures in the auditory pathway described in the previous paragraph. All BAEP waveforms represent far-field potentials, caused by activity of deep gray and/or white matter structures, relatively far from the surface recording electrodes. Table 1 lists the known or likely generators for each of these waves. Brainstem Auditory Evoked Potentials 477 Table 1 Brainstem Auditory Evoked Potential Waveforms and Their Associated Physiological Generators Wave I II III IV V VI VII Generator Proximal acoustic nerve (segment near cochlea) Distal acoustic nerve (segment near brainstem) or cochlear nuclei Superior olive and projections to the lateral lemniscus; medial nucleus of trapezoid body might generate a part of wave III Most likely the lateral lemniscus, but data is not definitive High pontine or lower midbrain structures: probably the lateral lemniscus, inferior colliculus, or a combination thereof Most likely the medial geniculate nucleus or projections from the inferior colliculus Most likely the auditory radiations to primary auditory cortex 3. METHODOLOGY 3.1. Stimulation and Recording Technique Auditory evoked potentials (AEPs) are classified as short, middle, or long latency potentials depending on their latency from stimulus onset. The short latency AEPs, occurring within 10 to 15 ms of stimulus onset, consist of the electrocochleogram and BAEPs. The electrocochleogram, middle, and late-onset AEPs are of less clinical relevance and will not be included in this review. To elicit and record BAEPs, an aural stimulus is delivered to the patient via headphones or indwelling earphones. Surface electrodes placed at A1 (left ear or mastoid), and A2 (right ear or mastoid) positions record voltage differences generated by stimulation of auditory pathways, using Cz (vertex) as a common reference. Waveforms are recorded from ipsilateral and contralateral pathways simultaneously, allowing easier recognition of individual peaks. Lowand high-frequency filters are commonly set to frequencies of 10 to 3000 Hz, respectively. Low-frequency filters can be raised to 100 to 200 Hz if muscle or mechanical artifact proves problematic. However, as the bandpass narrows, distortion of waveform morphology, amplitude, and latency can occur because of exclusion of low-frequency elements. Although pure tones are routinely used to analyze the specific frequency spectra of hearing loss, they are generally not used to elicit BAEPs. The most common acoustic stimuli used in BAEP testing are broadband (wide frequency spectra) 2-ms-long clicks, which are generated by a 100 µs square-wave pulse delivered to the diaphragm of the speaker membrane. As one ear is stimulated with clicks, the other is masked with white noise, an equal mixture of all of the frequencies within the range of human hearing (typically 20 Hz–20 kHz). This method helps to prevent the undesired coactivation of the contralateral ear caused by bony conduction from the ipsilateral stimulated ear. As with visual and somatosensory evoked potentials (SSEPs), and owing to the relatively small amplitude of the evoked auditory potentials, it is essential to average the BAEP waveforms produced by multiple stimulations to increase the signal-to-noise ratio. In general, 1000 to 4000 stimuli are given and averaged in BAEP testing. Eight to ten stimuli are given 478 Berger and Blum per second in most laboratories. Higher rates of frequency cause a rate-dependent reduction of amplitude, dispersion of waveforms, and longer interpeak latencies. Thus, if stimulation rates exceed 10 Hz, a different set of normative values must be used. Click intensity can impact BAEP generation. With decreasing click intensity, absolute latencies are increased and amplitudes are diminished. However, interpeak latencies remain relatively constant. Click stimulus intensity is measured in units of decibel sensation level (dBSL), decibel hearing level (dBHL), or decibel peak equivalent sound pressure level (dBpeSPL) rather than the more familiar decibels. Units of dBSL are used when hearing thresholds are determined for the individual ear being examined. If hearing thresholds are established using a group of healthy people, dBHL units are used. To ensure maximal and consistent BAEP acquisition, the stimulus intensity is set to 65 dB above dBSL or dBHL. As an example, if a person or group studied had a mean perceptual threshold of 10 dB for pure tone audiometry in the testing environment, an appropriate click stimulus intensity for BAEP acquisition would be 75 dB. Both the dBSL and dBHL are subjective measurements. If more objective measures are required, the dBpeSPL can be used. To determine the dBpeSPL, the amplitude of the headphone speaker’s membrane response to a brief click is recorded. This amplitude is matched to a longer duration sine-wave stimulus of defined dB intensity. In general, the dBpeSPL is approx 30 dB greater than the dBSL or dBHL. Stimulus polarity can also affect BAEP waveforms. The movement of the speaker membrane towards the eardrum is called condensation; movement away from the eardrum is termed rarefaction. Most BAEPs are recorded during rarefaction, but it is often helpful to switch polarity (record during condensation) to distinguish artifact from true BAEP waveforms. Artifact should reverse in polarity whereas BAEPs should not be altered. Wave I is the BAEP most affected by changes in stimulus polarity, with rarefaction producing a shorter latency. It may be necessary to change stimulus polarity to adequately see individual waveforms in some patients. Wave V in particular may seem to be absent until stimulus polarity is reversed. 3.2. Patient-Related Variables Affecting BAEPs A number of patient-related factors may also impact the BAEP recording. These include the individual’s age, gender, level of arousal, body position, temperature, medications, and preexisting hearing loss. Of these, body position, level of arousal, medications, and patient temperature can be adjusted to optimize results. Muscle artifact can interfere with the facile recording of BAEPs in 30 to 50% of waking patients. Sleep, most anesthetics, and coma of metabolic origin reduce this artifact. In the outpatient arena, it is often helpful to encourage the patient to try to sleep. Proper body positioning can also reduce the degree of muscle artifact caused by the cervical musculature as well as providing a situation more conducive to sleep. Although minor differences in BAEP amplitudes and latencies occur as an individual matures to adulthood, the most pronounced changes occur in infancy and early childhood. Neonates and infants have thinner skulls and smaller head sizes than adults. As a result, their scalp recording electrodes are in closer proximity to the generators for these potentials. This results in higher amplitude BAEPs. Premature infants less than 30 wk of age may not have detectable BAEP waveforms. By age 3 to 6 mo, waveform morphology should approximate that observed in adulthood; by 1 to 2 yr, latencies shorten to adult values. Changes occur most rapidly in early infancy, reflecting the rate of myelination, nerve fiber growth, and development of synaptic efficiency occurring in the developing nervous system. Brainstem Auditory Evoked Potentials 479 Female patients typically have shorter peak and interpeak latencies than male patients. Higher amplitudes are also frequently observed in female patients. Although effects of temperature on BAEPs are well-established, they are rarely clinically relevant, except for cases of severe hypothermia. Decreasing temperature prolongs both absolute and interpeak latencies. Waveforms can be observed at 27°C and above. If necessary, correction factors can be used. Hyperthermia has unclear effects on BAEP waveforms. Numerous toxins and medications affect BAEPs. Ethanol intoxication prolongs both absolute and interpeak latencies without affecting amplitude; ethanol withdrawal has unclear effects. Barbiturates, benzodiazepines, chloral hydrate, and most anesthetics do not significantly alter BAEPs in all but extreme doses. Paralytic agents can reduce muscle artifact and facilitate waveform recognition. Aminoglycosides and salicylates cause prolonged wave I latency and reduced BAEP amplitudes; these changes are usually reversible with medication cessation. Platinum-containing chemotherapeutic medications prolong all BAEP latencies and raise the threshold needed to elicit BAEPs. Some anticonvulsants, including phenytoin, carbamazepine, and valproate, prolong absolute and interpeak latencies. Sensorineural or conductive hearing loss can significantly impact the recording of BAEP waveforms. Mild hearing loss prolongs absolute latencies but will not affect interpeak latencies, as long as the stimulus intensity is strong enough. Severe hearing loss results in dispersed waveforms, phase cancellation, and difficult-to-interpret BAEP peaks. This may appear as absence of all waveforms. The I to V interpeak latency may be shorter with hearing loss, because of relative prolongation of the absolute latency of wave I. Cochlear dysfunction, as observed in Ménière’s disease or in presbyacusis, is characterized by a hearing deficit, which is maximal at threshold. Increasing stimulus intensity can result in normalization of waveforms, presumably by augmenting recruitment of cochlear neurons. 4. INTERPRETATION It is important to note that, in many normal individuals, all BAEP waves are not always present. Waves III and V should be detectable in all healthy individuals; wave I should also be observed but will only be present ipsilaterally. Wave II is often absent and wave IV is frequently buried and, therefore, indistinguishable from wave V. Wave III often has decreased amplitude on the side contralateral to that being stimulated. Waves VI and VII appear variably after wave V. Amplitudes of BAEP waveforms are extremely variable and, therefore, generally not of clinical significance. In most laboratories, latencies are considered abnormal if they fall beyond three standard deviations of the mean. Laboratories usually establish their own normative database. However, published tables of normal absolute and interpeak latencies are available (e.g., Chiappa, 1997). BAEPs have been studied in humans since the 1950s, although routine clinical use did not occur for another 20 yr. Historically, BAEPs were largely used to diagnose suspected lesions of the brainstem or the VIIIth cranial nerve that were unable to be visualized by imaging techniques in the pre-MRI era. BAEPs have played a particularly important role in the diagnosis of multiple sclerosis and cerebellopontine angle (CPA) tumors and helped differentiate between metabolic and structural causes of coma. The advent of MRI and other advanced neuroimaging techniques have dramatically decreased the use of BAEPs because of the relative ease and sensitivity of these modern imaging modalities for posterior fossa processes. Despite its fall from favor as the initial test of choice in suspected brainstem or VIIIth cranial nerve disease, important clinical roles for BAEPs still exist. It should be remembered 480 Berger and Blum Table 2 Overall Patterns of Brainstem Auditory Evoked Potential Abnormalitiesa Brainstem auditory evoked potential finding Prolonged wave I latency Prolonged I–III interpeak latency Prolonged III–V interpeak latency Prolonged I–III and III–V latencies Absent wave I with normal III and V Absent wave III with normal I and V Absent wave V with normal I and III Absence of all waves Absence of all waves except I (and possibly II) Lesion Distal CN VIII Between proximal CN VIII and pons (CPA masses) Lesion between caudal pons and midbrain (stroke, tumor, MS, ICH, AVM, etc.) Both rostral pons or midbrain and acoustic nerve or caudal pons Mild to moderate peripheral hearing loss Normal variant Above the caudal pons Severe hearing loss Brain death aCN, cranial nerve; CPA, cerebellopontine angle; MS, multiple sclerosis; ICH, intracranial hemorrhage; AVM, arteriovenous malformation. that BAEPs assess function of auditory pathways whereas neuroimaging studies examine structure. BAEPs are still a test of choice if physical examination and imaging findings are unrevealing but suspicion remains high for a brainstem or VIIIth cranial nerve functional deficit. In individuals who cannot undergo MRI secondary to implanted pacemakers, defibrillators, claustrophobia, and other reasons, BAEPs may provide valuable information regarding brainstem integrity. Because BAEPs are sensitive to auditory pathway dysfunction, a suspicion for clinically silent disease can be supported via evoked potential abnormalities. In demyelinating conditions, such as multiple sclerosis, BAEP testing can detect subclinical lesions, helping to define the extent and distribution of disease. However, BAEPs are less sensitive than VEPs and SSEPs in detecting abnormalities in patients with multiple sclerosis. The sensitivity for BAEPs in all those with suspected or confirmed multiple sclerosis is approx 46%. Those without overt brainstem symptoms have an even lower yield. In addition, BAEPs have a fairly low specificity for multiple sclerosis because numerous brainstem processes may result in abnormal responses. Nonetheless, testing enables the clinician to establish a baseline for comparison with future studies. In this way, improvement or progression of disease can be monitored objectively with electrophysiological data. On the other hand, BAEPs exhibit much greater sensitivity for acoustic schwannomas and other tumors of the CPA. Sensitivities ranging from 75 to 100% have been reported in the detection of various tumors in this locale. BAEPs may even be higher in sensitivity than CT imaging, although inferior to MRI for tumors of the CPA. As in demyelinating diseases, the specificity of BAEPs for recognizing cerebellopontine tumors is less impressive than is its sensitivity. BAEPs are also routinely used to assess hearing function in populations who cannot reliably cooperate with standard audiological testing (e.g., neonates and infants, and individuals with cognitive impairment). In addition, BAEPs are occasionally monitored in patents receiving potentially ototoxic chemotherapeutic agents. 481 Fig. 2. Abnormal BAEPs. These waveforms are from a 59-yr-old man with bilateral intranuclear ophthalmoplegia. There were no reported auditory symptoms. These recordings were performed with left ear stimulation. Montages are listed. Wave I is poorly formed but evident and has a normal latency. All other latencies are delayed. Furthermore, the I to III, III to V, and I to V interwave latencies are delayed. Right-sided results are very similar (not shown). This suggests bilateral defects in the auditory pathways both between the medulla and the lower midbrain, and between the auditory nerves and medulla. 482 Berger and Blum Today, intraoperative monitoring has emerged as one of the most important uses of BAEPs. Often, BAEPs are requested during posterior fossa surgery to monitor brainstem and acoustic nerve integrity in “real time.” BAEPs are not affected by most anesthetic agents and remain reliable measures of brainstem function under general anesthesia. If BAEP waveforms become abnormally prolonged or lost during surgery, the procedure can be adjusted in an attempt to avoid long-lasting neurological injury. Examples of surgeries in which BAEPs are often used include resection of acoustic neuromas, microvascular cranial nerve decompression, and clipping/repair of posterior circulation aneurysms. Table 2 outlines the common patterns of BAEP abnormalities and identifies their most commonly associated pathological causes. The most useful and informative measures derived from BAEP testing are the following: 1. Absolute latency of wave I: prolongation implies a lesion of the VIIIth cranial nerve. This can be observed in sensorineural or conductive hearing loss. Most schwannomas spare wave I. 2. Wave I to III interpeak latency: prolongation implies a lesion between the proximal segment of the eighth cranial nerve and the superior olivary nucleus. Often this reflects damage to structures at the CPA. Meningiomas and schwannomas at the CPA are typical examples of neoplasms that can cause prolonged I to III interpeak latency. 3. Wave III to V interpeak latency: prolongation suggests a lesion in pathways traveling from the caudal pons to the midbrain. Demyelinating plaques, infarcts, and neoplasms in the brainstem are often associated with increased III to V latency. Figure 2 illustrates an example of an abnormal BAEP evaluation with accompanying interpretation. In addition to hearing loss, demyelinating lesions, CPA tumors, brainstem tumors, and infarcts affecting the auditory pathways, BAEP abnormalities have been described in numerous other disease states. Texts such as that of Chiappa (1997) have summarized these findings, which are beyond the scope of this review. SUGGESTED READING Celesia GG, Brigell M. Auditory evoked potentials. In: Electroencephalography, Basic Principles, Clinical Applications, and Related Fields, 3rd ed. (Neidermeyer E, Lopes Da Silva F, eds.). Williams & Wilkins, Baltimore, MD, 1993, pp. 937–956. Chiappa KH. Evoked potentials in clinical medicine, 3rd ed. Lippincott-Raven, Philadelphia, PA, 1997. Erwin CW, Husain AM. Brainstem auditory evoked potentials. In: Current practice of clinical electroencephalography (Ebersole JS, Pedley TA, eds.). Lippincott Williams & Wilkins, Philadelphia, PA, 2003, pp. 864–891. Huszar L. Clinical utility of evoked potentials. eMedicine [serial online] 2006. Available at www.emedicine.com/neuro/topic69.htm. Misulis KE. Spehlmann’s Evoked Potential Primer, 2nd ed. Butterworth-Heinemann, Boston, MA, 1994. Misulis KE, Head TC. Brainstem auditory-evoked potentials. In: Essentials of Clinical Neurophysiology, 3rd ed. Butterworth-Heinemann, Boston, MA, 2003, pp. 211–220. REVIEW QUESTIONS 1. A 66-yr-old man with bilateral watershed infarcts from complications of cardiac bypass surgery seems to have pure word deafness. BAEP testing would most likely reveal which of the following: A. Absence of all waveforms. B. Bilateral absence of wave V, VI, and VII. C. No abnormalities. D. Prolonged III to V interpeak latency. Brainstem Auditory Evoked Potentials 483 2. A 22-yr-old woman, deaf in both ears because of complications of meningitis in infancy, develops symptoms suggestive of multiple sclerosis. BAEPs will most likely reveal which of the following: A. Prolonged absolute latency of wave I. B. Prolonged III to V interpeak latency. C. Prolonged I to III interpeak latency. D. Absence of all waveforms. E. No abnormalities. 3. A prolonged I to III interwave latency would most likely be caused by which of the following: A. Coma. B. Meningioma. C. Demyelinating disease. D. Brainstem hemorrhage. 4. BAEPs in a patient meeting criteria for brain death would show which of the following: A. Absence of all waves. B. Intact waveforms I and II. C. No abnormalities. D. Absence of wave I. 5. When recording BAEPs, improving the signal-to-noise ratio is largely accomplished by which of the following: A. Increasing stimulus intensity. B. Increasing rate of repetitions. C. Increasing amplification of elicited waveforms. D. Giving multiple stimulus repetitions. 6. A patient with sensorineural hearing loss may have which of the following changes in BAEP waveforms: A. Global increase in waveform amplitude. B. Global increase in absolute latencies. C. Increased I to V interpeak latency. D. Rapid correction of prolonged latency with increased stimulus intensity. E. B and D. F. B and C. 7. Changes in stimulus polarity affect which BAEP waveform latency the most consistently: A. Wave I. B. Wave III. C. Wave IV. D. Wave V. 8. A BAEP study notable for a prolonged I to V interpeak latency might indicate the presence of which of the following: A. Pontine glioma. B. Neurofibromatosis type II. C. Multiple sclerosis. D. All of the above. 9. The inferior colliculus likely plays a role in generating which of the following waveforms: A. Wave I. B. Wave II. C. Wave III. D. Wave IV. E. Wave V. 10. The least-sensitive diagnostic assay for multiple sclerosis is which of the following: A. MRI of the brain with contrast enhancement. B. BAEPs. C. VEPs. D. SSEPs. 484 Berger and Blum REVIEW ANSWERS 1. The correct answer is C. Cortical lesions should not affect BAEP waveforms. It is possible that wave VII might be affected by a lesion involving the auditory radiations, but waves VI and VII are not used routinely in clinical evaluation. 2. The correct answer is D. Severe hearing loss can cause BAEP amplitudes to be reduced so much that they are not detectable. 3. The correct answer is B. Masses at the CPA often cause this pattern of abnormalities on BAEP testing. Common lesions include vestibular schwannomas and meningiomas. 4. The correct answer is B. Patients who meet criteria for brain death typically have intact wave I responses. In approx 10% of individuals, wave II may also be present. 5. The correct answer is D. Giving multiple stimulus repetitions is essential to achieving an adequate signal-to-noise ratio. Hundreds to thousands of stimuli are given to differentiate small AEPs from EEG potentials. 6. The correct answer is E. Mild-to-moderate hearing loss globally prolongs absolute latencies. Interpeak latencies are not appreciably changed. Increasing stimulus intensity can result in normalization of waveforms. 7. The correct answer is A. Rarefaction causes shorter absolute wave I latency than condensation. Although changing polarity can affect the amplitudes and latencies of other waveforms, there is more variation between individuals. Use of alternating polarity clicks is not routinely used because of the potential of phase cancellation. In most cases, rarefaction clicks produce the most reliable waveforms. If artifact is suspected or certain waveforms seem absent, a trial with condensation clicks is warranted. 8. The correct answer is D. All of the above are correct. A pontine glioma, depending on its location, could impact the I to III and/or III to V interpeak latencies. Neurofibromatosis type II is often characterized by bilateral acoustic schwannomas, resulting in prolonged I to III latencies. Demyelinating lesions in the brainstem can cause prolonged III to V latency. All of these would, in turn, cause I to V interpeak latency prolongation. 9. The correct answer is E. Wave V is probably, at least in part, generated by activity in the inferior colliculus. 10. The correct answer is B. BAEPs have the least sensitivity for detecting abnormalities in multiple sclerosis.